










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Curriculum ScienTI
Curriculum ScienTI Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkRevista Pan-Amazônica de Saúde
Print version ISSN 2176-6215On-line version ISSN 2176-6223
Rev Pan-Amaz Saude vol.11 Ananindeua 2020 Epub Aug 25, 2020
http://dx.doi.org/10.5123/s2176-6223202000229
ORIGINAL ARTICLE
Spatial distribution of leprosy cases in children under 15 years old, in Belém, Pará State, Brazil
1 Instituto Evandro Chagas, Programa de Pós-Graduação em Epidemiologia e Vigilância em Saúde, Ananindeua, Pará, Brasil
2 Instituto Evandro Chagas, Ananindeua, Pará, Brasil
OBJECTIVES:
To identify the leprosy spatial distribution cases in individuals under 15 years old, in Belém, Pará State, Brazil, from 2005 to 2014, correlating with socioeconomic indicators.
MATERIALS AND METHODS:
An ecological study was conducted with 356 new cases registered in Belém, whose data were collected in the Information System for Notifiable Diseases. The following clinical and epidemiological variables were evaluated: sex, age group, operational classification, clinical form, degree of physical disability in the diagnosis, detection mode, and detection coefficient in individuals under 15 years old. Georeferencing was carried out from the address registered in the notification form to produce maps with neighborhood divisions, and the incidence rate was correlated with the socioeconomic data of each neighborhood using linear regression.
RESULTS:
Belém was classified as hyperendemic for leprosy in individuals under 15 years old, and five districts with approximately 35% of cases. Of 71 neighborhoods, 22 were considered hyperendemic due to the detection rate, and georeferencing identified two cluster areas. The correlation of socioeconomic data showed significance for lack of income, absence of garbage and sewage collection.
CONCLUSION:
The leprosy distribution is not homogeneous in Belém, with the necessity to direct resources to the most vulnerable areas.
Keywords: Leprosy; Public Health Surveillance; Epidemiology; Geographic Mapping; Health Vulnerability; Minors
INTRODUCTION
Over the years, the epidemiological situation of leprosy in Brazil has shown several challenges to public health sectors for the disease eradication. Approximately 40% of leprosy cases registered in Brazil in 2016 were found in regions with about 15% of the population1. While the North and Midwest Regions registered, in the same year, a rate of 28.70 and 30.02 cases per 100,000 inhabitants, respectively, the South Region had a number 10 times lower1, demonstrating that the country has areas far from reaching the elimination target. In this scenario, the cities located in the Brazilian Amazon are considered places of high endemicity for the disease2 and low social infrastructure.
The unequal distribution of leprosy can also be observed when the analysis scale increases or decreases, such as by municipal sectors or neighborhoods3. Thus, the space component becomes crucial for the leprosy epidemiological understanding. Space is considered an analysis category that is not limited to physical and geometric conceptions, but it is understood from a relational and inseparable view of a social perspective4,5. When a place is observed, it is known that the people organization in a territory does not occur arbitrarily. The discussion about the spatial distribution of leprosy in the urban area also implies discussing the urbanization process, the existing urban poverty, and how the population is distributed across space in the face of unmet needs5.
As people take possession of certain areas and, in return, are deprived of others, the different accesses to urban infrastructure services and the risks of falling ill are delimited. Therefore, space becomes a determinant in the health-disease process5,6, especially regarding leprosy, in which the low quality of life has been identified as a significant factor in its endemicity by several authors3,5,7.
Faced with this interlocution between geography and health surveillance, in the 1990s, new geoprocessing techniques emerged to create maps for understanding spaces and their relationship with diseases6. By enabling better leprosy spatial distribution cases visualization and epidemiological indicators, in addition to coverage for the treatment of the disease, this technological resource became a recommendation of the World Health Organization8. Thus, the use of this technology began to be encouraged, especially for areas of high endemicity, with wide regional differences and the need to allocate additional investments7,9.
Even with the importance of space for leprosy incidence, it is essential to recognize what these areas have in common and what makes them a potential factor in the disease acquisition. Several socioeconomic factors have proven to be relevant, such as precarious housing conditions, low education, and income and migratory movements2,7. Several associations indicate a higher prevalence of leprosy among less favored social strata. By recognizing the possible correlations between leprosy and socioeconomic circumstances, which make it possible for the disease to become endemic in a location, they collaborate to develop more effective combat strategies, such as implementing active search measures and health surveillance in the territory.
Faced with this disease, which has such a critical socio-spatial component, the age group of children and young people deserves special attention. The presence of leprosy in individuals under 15 years old is usually linked to intra-household transmission, as the disease has a prolonged incubation period, so these contacts are an important means for maintaining the endemic disease. Therefore, the leprosy incidence in this age group is an epidemiological indicator of active disease transmission, revealing early transmission and persistence of untreated bacilliferous people. In addition, this indicator points to high endemicity and insufficient actions in terms of disease surveillance, control, and health education, making it a significant marker. Based on this perspective, the reduction of cases in individuals under 15 years old has become a priority of the National Leprosy Control Program in the Heath Surveillance Secretariat of the Brazilian Ministry of Health, a fact that should be prioritized in hyperendemic locations, such as Pará State, which registered a rate of 17.54 cases/100,000 inhabitants in this age group, in 201411.
This study aimed to identify the spatial distribution, based on georeferencing of leprosy cases in individuals under 15 years old in Belém City, Pará State, Brazil, between 2005 and 2014, and to correlate it with socioeconomic indicators. With this data, it will be possible to expand the knowledge about the leprosy endemic process, contribute to the city's health information system, and provide information for active search and disease control measures.
MATERIALS AND METHODS
This is an epidemiological, exploratory, analytical study performed in 2016. The research site was in Belém, the capital of Pará State, in Brazil's North Region. The city has 71 neighborhoods, 23 located on Mosqueiro island (in the far north) and Outeiro, comprising non-urban areas. In the present study, the municipality districts were used as the unit of analysis. In 2010, there were 1,393,399 residents, with a population density of 1,315.26 inhabitants/km², where 321,092 were under 15 years old12,13.
For the leprosy cases analysis in individuals under 15 years old in Belém, between 2005 and 2014, data from the Notifiable Diseases Information System (SINAN) made available by the Health State Department of Pará (SESPA) were used. These data were input into databases using Microsoft Excel and Epi Info™ v7.2 to be selected and processed according to clinical-epidemiological and georeferencing criteria. As for the clinical-epidemiological criteria, the following variables were analyzed: sex; age group (0-4, 5-9, and 10-14 years old); operational classification (multibacillary and paucibacillary); clinical form (undetermined, tuberculoid, borderline, and lepromatous); degree of physical disability at diagnosis (0.1 and 2); and detection mode (referral, spontaneous demand, collective examination, contact examination, and other modes), divided into active search (contact examination and collective examination) and passive search (referral and spontaneous demand). Leprosy monitoring indicators14 were also generated: the detection rate in individuals under 15 years old (per 100,000 inhabitants) in Belém, in 2010, and the leprosy proportion cases with grade 2 physical disability at the time of diagnosis. For georeferencing, data about the city, neighborhood, street address, house number, address complement, landmark, and year of notification were used.
Georeferencing was initially carried out through geocoding using Google Earth Pro software. The latitude and longitude data generated were then entered into the Epi Info™ v7.2 to produce thematic maps in the choropleth model. In maps design, the digital mesh outlining the districts of Belém from the Development and Administration Company of the Belém Metropolitan Area was used, made available by the Evandro Chagas Institute Georeferencing Laboratory.
The geocoding method started from the addresses registered in SINAN, which were input in Google Earth Pro for automatic search, prioritizing the street and, when possible, the house number. In cases of doubt regarding the residence position in relation to the neighborhood, the Street View feature of the same software was used. When locating the street address failed, or the record was incomplete, only the neighborhood registered at the time of notification was used. In order to compare the spatial distribution over the years, two thematic maps were generated to analyze leprosy spatial distribution in individuals under 15 years old, with five-year subperiods. Thus, observing the disease's progression in Belém and potential patterns and variations over the years was possible.
A correlation was performed using multivariate linear regression statistical analysis between the leprosy incidence rate in individuals under 15 years old and socioeconomic data in each neighborhood to verify possible risk factors for higher disease incidence in these territorial units. To this end, population data were obtained from the Belém city statistical yearbook13, and municipal sanitation data were provided by the General Coordination of Planning and Management Municipal Secretary (SEGEP), both from 2010.
The following socioeconomic variables were computed by city district: residents proportion per household; people percentage aged 10 or over, by nominal monthly income class; illiterate people percentage aged 10 or over; percentage of households without water supply from the general network; percentage of households not connected to the general sewage network or that did not have a septic tank; and percentage of households without garbage collection.
The present study was conducted following the bioethics basic principles, recommended in international standards and Resolution nº 466/12 of the National Health Council, guaranteeing the privacy of its contents and preventing the information use for other purposes.
RESULTS
From 384 cases of leprosy in individuals under 15 years old reported in the period, only new cases were included, totaling 356 records. As described in table 1, the epidemiological picture of leprosy in Belém in this age group for the analyzed period showed predominance among males (proportion of 1.2 cases) and the age group from 10 to 14 years old (64.9%). Most cases were classified as paucibacillary (59.6%) and tuberculoid clinical form (37.9%); two cases were not classified. As for the degree of disability, 10.1% (36 notifications) cases had some disability at the diagnosis time, 11 (3.1%) with disability level 2, and 43 (12.1%) were not classified. Referral was the most recurrent mode of detection (62.4%), followed by spontaneous demand (29.2%). The collective examination occurred in four (1.1%) cases, while the contact examination occurred in 24 (6.7%). Thus, the active search constituted 7.9% of the cases, while the passive search represented 91.6%.
Table 1 - Leprosy characteristics in new cases of individuals under 15 years old in Belém, Pará State, Brazil, between 2005 and 2014
| Variables | Registered cases | |
|---|---|---|
| N = 356 | % | |
| Sex | ||
| Male | 194 | 54.5 |
| Female | 162 | 45.5 |
| Age range (years) | ||
| 0-4 | 16 | 4.5 |
| 5-9 | 109 | 30.6 |
| 10-14 | 231 | 64.9 |
| Operational classification | ||
| Multibacillary | 144 | 40.4 |
| Paucibacillary | 212 | 59.6 |
| Clinical form | ||
| Undetermined | 74 | 20.8 |
| Tuberculoid | 135 | 37.9 |
| Borderline | 117 | 32.9 |
| Lepromatous | 28 | 7.9 |
| Not classified | 2 | 0.5 |
| Degree of physical disability | ||
| 0 | 277 | 77.8 |
| 1 | 25 | 7.0 |
| 2 | 11 | 3.1 |
| Not classified | 43 | 12.1 |
| Detection mode | ||
| Referral | 222 | 62.4 |
| Spontaneous demand | 104 | 29.2 |
| Collective examination | 4 | 1.1 |
| Contact examination | 24 | 6.7 |
| Other modes or ignored | 2 | 0.6 |
Source: SINAN/SESPA, 2016.
Considering the Belém population under 15 years old in 2010, the new cases annual detection rate indicator in this age group for that year was 10.28 cases/100,000 inhabitants. In addition, it was possible to establish an approximation of 11.09 cases/100,000 inhabitants, considering the average number of cases between 2005 and 2014 and the population of 2010. There was one leprosy case in every 9,017 individuals under 15 years old. The proportion of leprosy cases with grade 2 physical disability at diagnosis was 3.5% among new cases detected and evaluated in the year.
The leprosy georeferencing carried out from the neighborhoods excluded 27 of the 356 cases due to lack of necessary data, totaling 329 mapped cases. Three cases were detected outside the city limits, and 10 cases did not fit the neighborhood boundaries, being considered residents in rural areas of the municipality. In view of this, 316 cases were within the limits of Belém neighborhoods, and, of these, 49 were georeferenced only from the neighborhoods. From the address analysis, 53 cases of discrepancy between the self-declared neighborhood and the one found from the street georeferencing (street, house number, and perimeter) were observed.
Figure 1 shows the distribution of 316 leprosy cases in individuals under 15 years old in the 71 districts of Belém. Neighborhoods with more than 5% of mapped cases were considered clusters, representing more than 16 cases. The neighborhoods included in this category were Guamá (41 cases), Jurunas (24 cases), Tapanã (23 cases), Montese (20 cases), and Benguí (18 cases). These five neighborhoods represented approximately 35% of all cases registered. Thus, it was possible to observe two groups of neighborhoods by physical proximity, the Montese-Guamá-Jurunas region and the Tapanã-Benguí region.
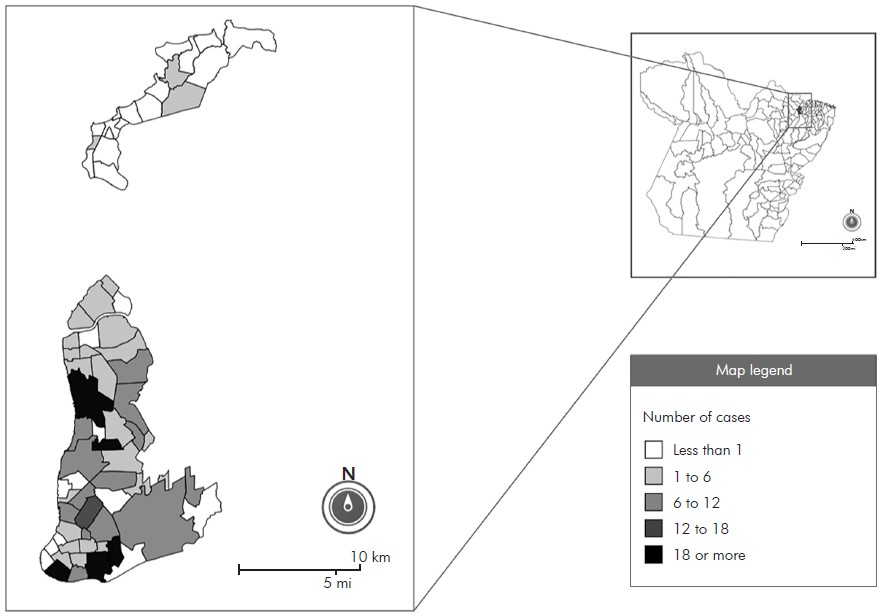
Figure 1 - Thematic map of Belém City, Pará State, Brazil, according to the number of leprosy cases in individuals under 15 years old between 2005 and 2014
Due to the districts' population difference, the map in figure 2 shows the leprosy detection rate by neighborhood. The categories were organized according to the detection endemic parameters rate indicator. It was observed that 22 of the 71 neighborhoods were considered hyperendemic. The neighborhoods Bonfim (119.92 cases/100,000 inhabitants) and Praia Grande (105.82 cases/100,000 inhabitants), both located on Mosqueiro Island (island at the extreme north of the map), presented the worst epidemiological scenarios, followed by the Val-de-Cães (82.22 cases/100,000 inhabitants), Fátima (46.12 cases/100,000 inhabitants), Guanabara (23.31 cases/100,000 inhabitants), and Carananduba (23.30 cases/100,000 inhabitants), the latter also located on Mosqueiro Island.
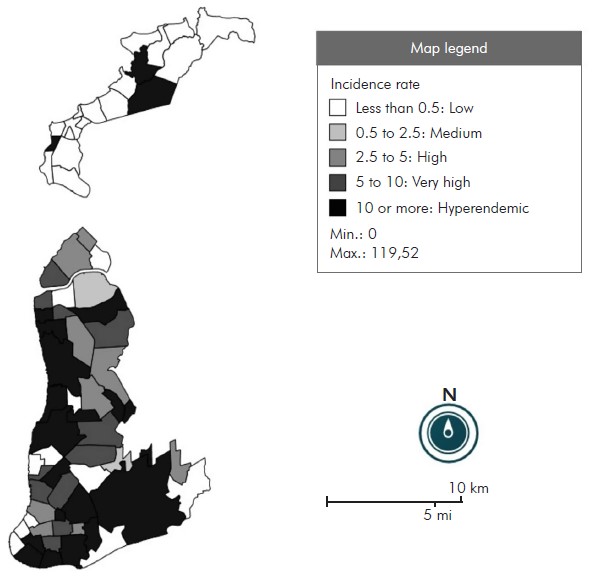
Figure 2 - Thematic map of Belém City, Pará State, Brazil, according to the leprosy incidence rate in individuals under 15 years old between 2005 and 2014
Figure 3 contains the georeferencing maps based on the number of cases divided into periods of five years, the first (on the left) from 2005 to 2009 and the second (on the right) from 2010 to 2014. There was a 32% decrease in the second period compared to the first, going from 188 cases to 128. The number of neighborhoods with nine or more cases went from six, in the first five years, to three in the second half of the analyzed decade. Half the number of cases in figure 1 was used as an extension of the values to obtain a proportional comparison to the analyzed period.
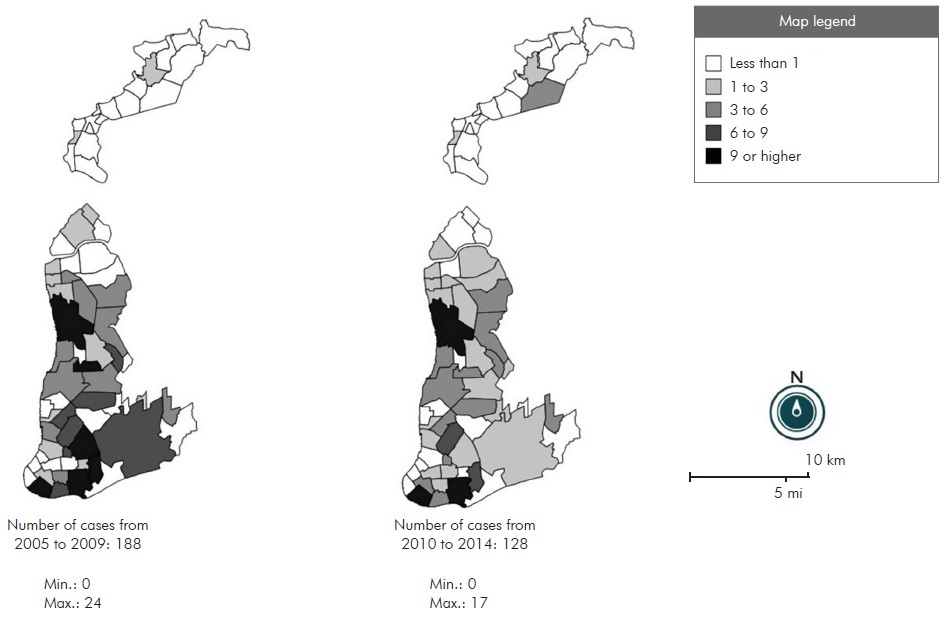
On the left, the map rate from 2005 to 2009 with 188 registered and georeferenced cases. On the right, the map rate from 2010 to 2014 with 128 registered and georeferenced cases.
Figure 3 - Thematic maps of Belém City, Pará State, Brazil, according to the number of leprosy cases in individuals under 15 years old, between 2005 and 2014
Regarding the socioeconomic characteristics, table 2 shows the neighborhoods with the highest frequency in the analyzed indicators. The Sucurijuquara neighborhood was recorded in five indicators; Bonfim and Caruara, in three; and Ariramba, Aurá, Natal do Murubira, and São Francisco, in two indicators each. Of these seven neighborhoods, six belong to Mosqueiro Island.
Table 2 - Classification of neighborhoods in Belém city, Pará state, Brazil, for 2010, according to socioeconomic indicators
| Variables | Amount |
|---|---|
| Neighborhoods with residents/household ratio > 4 | |
| Sucurijuquara | 4.18 |
| Barreiro | 4.13 |
| Fátima | 4.12 |
| Condor | 4.10 |
| Baía do Sol | 4.10 |
| Jurunas | 4.06 |
| Telégrafo | 4.06 |
| Guamá | 4.04 |
| Neighborhoods with more than 50% of people aged 10 years or older without income | |
| Bonfim | 65.57% |
| Ariramba | 61.37% |
| São Francisco | 57.85% |
| Sucurijuquara | 55.09% |
| Brasília | 53.34% |
| Natal do Murubira | 52.23% |
| Paracuri | 51.66% |
| Neighborhoods with more than 10% illiteracy | |
| São Francisco | 59.61% |
| Caruara | 38.77% |
| Benguí | 13.51% |
| Neighborhoods with more households without general water supply | |
| Marahú | 100.00% |
| Paraíso | 100.00% |
| Sucurijuquara | 98.83% |
| Bonfim | 98.57% |
| Caruara | 98.52% |
| Neighborhoods with more households without access to the general sewage system or septic tank | |
| Sucurijuquara | 99.61% |
| Natal do Murubira | 97.93% |
| Aurá | 96.12% |
| Porto Arthur | 87.84% |
| Ariramba | 86.90% |
| Neighborhoods with more households without garbage collection | |
| Bonfim | 62.38% |
| Mangueiras | 62.01% |
| Aurá | 34.11% |
| Caruara | 33.00% |
| Sucurijuquara | 31.52% |
Source: SEGEP, 2010.
Finally, linear regression was performed between the mentioned socioeconomic variables and the incidence rate of the neighborhoods (Table 3). Statistical analysis showed a significant correlation value (p < 0.05) for the variables income (0.0327), sewage (0.0144), and garbage collection (0.0369). As for the correlation coefficient of the significant variables, the income variable had the highest value (124.628).
Table 3 - Linear regression between the incidence rate (dependent variable) and socioeconomic data of the neighborhoods (independent variable) in Belém City, Pará State, Brazil, between 2005 and 2014
| Independent variable | Estimate (β) | Standard error | t-test | p-value |
|---|---|---|---|---|
| Proportion of residents per household | 5.411 | 12.356 | 0.438 | 0.6629 |
| Income: percentage of people aged 10 years or older without income | 124.628 | 57.096 | 2.183 | 0.0327 |
| Education: percentage of illiterate people aged 10 years or older | -50.621 | 34.094 | -1.485 | 0.1425 |
| Sewage: percentage of households without access to the general sewage system or septic tank | -27.718 | 11.017 | -2.516 | 0.0144 |
| Garbage collection: percentage of households without garbage | 54.943 | 25.780 | 2.131 | 0.0369 |
| Water: percentage of households without general water supply | -7.277 | 10.961 | -0.664 | 0.5092 |
Source: SINAN/SESPA, 2016 and SEGEP, 2010.
DISCUSSION
Leprosy in individuals under 15 years old was considered hyperendemic in Belém during the analyzed period, according to the parameters for the rate detection by the Brazilian Ministry of Health14. Nevertheless, the active search represented less than 1/10 forms of detection. There was a low proportion of leprosy cases with grade 2 physical disability at the time of diagnosis among the new cases detected and evaluated in the year; however, the proportion of new disease cases with a degree of physical disability assessed at diagnosis was classified as regular (assessed between ≥ 75 to 89.9%), also according to the criteria by the Ministry of Health14.
The leprosy distribution did not demonstrate homogeneity throughout the municipality's territory, which corroborates previous studies in other cities and regions of Brazil15,16,17. The leprosy spatial distribution cases in individuals under 15 years old in Belém had cluster areas, with the most relevant neighborhoods being Guamá, Jurunas, Montese, Benguí, and Tapanã. The cases distribution map showed a greater concentration in the city's southern region, forming an expansion corridor towards the north, and little expression of cases in the southwest. This fact coincided with the town's socioeconomic distribution, with greater concentration of income areas in the southwest and population clusters with less financial resources in the south18. In addition, a reorganization of urban space has been observed in recent decades, with a historical expansion of settlement to the northern area, a movement associated with real estate speculation, population relocations, and demographic increase18.
Furthermore, the lack of notification was registered in 27 (38%) neighborhoods. Among these, some neighborhoods border those considered clusters, such as Cidade Velha (border with Jurunas) and São Clemente (border with Benguí and Tapanã). Such data may suggest low coverage or fragility of primary care in these locations, highlighting leprosy as a neglected disease often undiagnosed. In this sense, cases underreporting can mask other cluster areas, especially in regions with higher people concentration and lower financial resources.
The detection rate map revealed that many neighborhoods (22 out of 71) were classified as hyperendemic, according to the Ministry of Health parameters14, demonstrating the city's vulnerability to leprosy in individuals under 15 years old. There are relevant places for leprosy other than areas classified as clusters, such as Mosqueiro Island, located in the extreme north. Mosqueiro has neighborhoods where the highest detection rate was found alongside those with a low or zero detection rate, which suggests the underreporting of several cases in the area and the fragility of health services. When the detection rate was analyzed with the socioeconomic indicators of the city's neighborhoods, the precarious conditions of the neighborhoods on Mosqueiro Island were revealed.
The clusters found and the regions with a high incidence rate demonstrate the need for greater attention by the health network and epidemiological surveillance. The degree of disability at the time of diagnosis and the method of detecting the clinical case are tools that reveal the quality of public health actions for the early search for cases, especially in individuals under 15 years old. Regarding these data, several cases were still reported with some degree of disability, even though the proportion of leprosy cases with grade 2 physical disability at the time of diagnosis was classified as low. In addition, the health service had an exceptionally low active leprosy search in individuals under 15 years old, a fact that may obscure the number of real cases among the population. These data align with the high endemic rate throughout the municipality and its fragility in containing the disease.
The comparison between the five years analyzed showed a decrease in the number of cases, more evident in the southern region. In contrast, in the neighborhoods located on Mosqueiro Island, in the northern region, there was an intensification. However, this general decrease may hide a decrease in notification actions in the last five years. Studies focused on the disability degree, the detection mode, and the primary care presence can clarify possible underreporting in this period. Furthermore, the maintenance of the cases corridor in the south-north direction in the two temporal maps indicates that the transmission chains are still present.
When analyzing the association between socioeconomic conditions and the leprosy incidence in individuals under 15 years old in Belém during the studied period, it was observed that not all socioeconomic variables had a significant influence. Significance was demonstrated for the variables income, sewage, and garbage collection, with income variation being the most impactful for the disease incidence in this age group. These data partially agree with previous studies, which analyze leprosy in the general population in other municipalities with similar socioeconomic assessments4,17,19,20,21,22. In a recent study in a hyperendemic city in Tocantins State, the authors concluded that populations with a high degree of vulnerability, such as low socioeconomic status and a higher proportion of immigrants, are associated with high detection rates of new leprosy cases and potentially the highest degree of disability21. Despite the lack of statistical correlation with all the variables, it was observed that the high incidence rate in some neighborhoods on Mosqueiro Island corroborates the precarious socioeconomic conditions analyzed.
In addition, the clusters of leprosy in Guamá, Montese, Jurunas, Benguí, and Tapanã neighborhoods are also considered areas of socioeconomic vulnerability in the city. Despite not being recurrently among the worst socioeconomic indexes (except for the residents/domicile indicator in which the Guamá and Jurunas appear, and for the illiteracy indicator in which the Benguí is found), such neighborhoods have low access conditions to basic sanitation and education23,24.
Therefore, even without statistical correlation with all socioeconomic variables analyzed, the combination of low living conditions and the leprosy occurrence in individuals under 15 years old cannot be excluded as an important criterion when identifying a priority area for intervention. Furthermore, the causes for this distribution still need to be clarified, given that several other factors, besides socioeconomic ones, may be correlated with the disease development, such as genetic factors and subclinical infections16,25, in addition to the absence or low quality of health services.
CONCLUSION
The non-homogeneous distribution of leprosy in individuals under 15 years old demonstrates the existence of more susceptible areas, indicating that children and young people from these locations, such as Mosqueiro Island or the neighborhoods located in the clusters, are more vulnerable to becoming ill with leprosy. The production of maps based on georeferencing with populations under the age of 15 contributes to health surveillance and makes it possible to direct resources to areas with the highest risk of transmission. Thus, it is suggested to train the health team for early diagnosis, especially through active search, and adequate notification, aiming to reduce transmission in the locality and the sequelae that leprosy not treated early can cause.
REFERENCES
1 Ministério da Saúde (BR). Registro ativo: número e percentual, casos novos de hanseníase: número, taxa e percentual, faixa etária, classificação operacional, sexo, grau de incapacidade, contatos examinados, por estados e regiões, Brasil, 2016. Brasília: Ministério da Saúde; 2017. [ Links ]
2 Monteiro LD, Martins-Melo FR, Brito AL, Alencar CH, Heukelbach J. Spatial patterns of leprosy in a hyperendemic state in Northern Brazil, 2001-2012. Rev Saude Publica. 2015;49:84. [ Links ]
3 Dias MCFS, Dias GH, Nobre ML. Distribuição espacial da hanseníase no município de Mossoró/RN, utilizando o Sistema de Informação Geográfica - SIG. An Bras Dermatol. 2005 nov-dez;80(supl 3):S289-94. [ Links ]
4 Faria RM, Bortolozzi A. Espaço, território e saúde: contribuições de Milton Santos para o tema da geografia da saúde no Brasil. RA'E GA. 2009;17:31-41. [ Links ]
5 Mencaroni DA, Pinto NetoJM, Villa TCS, Oliveira MHP. Análise espacial da endemia hansênica na área urbana do município de Fernandópolis/SP. Hansen Int. 2004;29(1):12-20. [ Links ]
6 Bonfim C, Medeiros Z. Epidemiologia e geografia: dos primórdios ao geoprocessamento. Espaç Saude. 2008 dez;10(1):53-62. [ Links ]
7 Amaral EP, Lana FCF. Análise espacial da hanseníase na microrregião de Almenara, MG, Brasil. Rev Bras Enferm. 2008 nov;61(no. esp):701-7. [ Links ]
8 World Health Organization. Estratégia global para Hanseníase 2016-2020: aceleração rumo a um mundo sem hanseníase. Genebra: World Health Organization; 2016. [ Links ]
9 Gauy JS, Hino P, Santos CB. Distribuição espacial dos casos de hanseníase no município de Ribeirão Preto no ano de 2004. Rev Latino-Am Enfermagem. 2007 jun;15(3):460-5. [ Links ]
10 Pires CAA, Malcher CMSR, Abreu Jr JMC, Albuquerque TG, Corrêa IRS, Daxbacher ELR. Hanseníase em menores de 15 anos: a importância do exame de contato. Rev Paul Pediatr. 2012 jun;30(2):292-5. [ Links ]
11 Ministério da Saúde (BR). Taxa de detecção de hanseníase em menores de 15 anos: estados e regiões, Brasil, 1994 a 2016. Brasília: Ministério da Saúde ; 2017. [ Links ]
12 Instituto Brasileiro de Geografia e Estatística. Cidades: população residente no município de Belém - 2010 [Internet]. Rio de Janeiro: IBGE; 2017 [citado 2017 out 10]. Disponível em: Disponível em: https://cidades.ibge.gov.br/brasil/pa/belem/panorama . [ Links ]
13 Prefeitura Municipal de Belém. Secretaria Municipal de Coordenação Geral do Planejamento e Gestão. Anuário estatístico do município de Belém, 2011. Vol. 16. Belém: Prefeitura Municipal de Belém; 2012. [ Links ]
14 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Diretrizes para vigilância, atenção e eliminação da hanseníase como problema de saúde pública: manual técnico-operacional. Brasília: Ministério da Saúde ; 2016. [ Links ]
15 Alencar CH, Ramos Jr AN, Santos ES, Richter J, Heukelbach J. Clusters of leprosy transmission and of late diagnosis in a highly endemic area in Brazil: focus on different spatial analysis approaches. Trop Med Int Health. 2012 Apr;17(4):518-25. [ Links ]
16 Duarte-Cunha M, Souza-Santos R, Matos HJ, Oliveira MLW. Aspectos epidemiológicos da hanseníase: uma abordagem espacial. Cad Saude Publica. 2012 jun;28(6):1143-55. [ Links ]
17 Imbiriba ENB, Silva Neto AL, Souza WV, Pedrosa V, Cunha MG, Garnelo L. Desigualdade social, crescimento urbano e hanseníase em Manaus: abordagem espacial. Rev Saude Publica. 2009 ago;43(4):656-65. [ Links ]
18 Cardoso ACD, Ventura Neto RS. A evolução urbana de Belém: trajetória de ambiguidades e conflitos socioambientais. Cad Metrop. 2013 jan-jun;15(29):55-75. [ Links ]
19 Cury MRCO, Paschoal VDA, Nardi SMT, Chierotti AP, Rodrigues Jr AL, Chiaravalloti-Neto F. Spatial analysis of leprosy incidence and associated socioeconomic factors. Rev Saude Publica. 2012 Feb;46(1):110-8. [ Links ]
20 Kerr-Pontes LRS, Montenegro ACD, Barreto ML, Werneck GL, Feldmeier H. Inequality and leprosy in Northeast Brazil: an ecological study. Int J Epidemiol. 2004 Apr;33(2):262-9. [ Links ]
21 Monteiro LD, Mota RMS, Martins-Melo RF, Alencar CH, Heukelbach J. Social determinants of leprosy in a hyperendemic State in North Brazil. Rev Saude Publica. 2017;51:70. [ Links ]
22 Silva CLM, Fonseca SC, Kawa H, Palmer DOQ. Spatial distribution of leprosy in Brazil: a literature review. Rev Soc Bras Med Trop. 2017 Jul-Aug;50(4):439-49. [ Links ]
23 Governo do Brasil. Metas para saneamento básico [Internet]. 2012 [citado 2017 out 10]. Disponível em: Disponível em: http://www.brasil.gov.br/old/copy_ of_imagens/noticias/imagens-2012/agosto/metas-para-saneamento-basico/view . [ Links ]
24 Ministério da Educação (BR). Planejando a próxima década: conhecendo as 20 metas do plano nacional de educação. Brasília: Ministério da Educação; 2014. [ Links ]
25 Bakker MI, May L, Hatta M, Kwenang A, Klatser PR, Oskam L, et al. Genetic, household and spatial clustering of leprosy on an island in Indonesia: a population-based study. BMC Med Genet. 2005 Nov;6:40. [ Links ]
14Article originally published in Portuguese (https://doi.org/10.5123/S2176-6223202000229)
Received: March 20, 2019; Accepted: February 04, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
