










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.3 Brasília jun. 2020 Epub 20-Mayo-2020
http://dx.doi.org/10.5123/s1679-49742020000300004
Original article
Sex differentials in avoidable mortality and potential life expectancy gains in São Paulo, SP, Brazil: a cross-sectional study of the period 2014-2016
1Universidade Federal de Alfenas, Instituto de Ciências Sociais Aplicadas, Varginha, MG, Brazil
Objective
to estimate potential life expectancy gains and differences between males and females, if avoidable deaths from circulatory system diseases, neoplasms and external causes had been eliminated in São Paulo, SP, Brazil, in the period 2014- 2016.
Methods
this was a cross-sectional study using data from the Mortality Information System (SIM), and the Brazilian Institute of Geography and Statistics (IBGE), using multiple decrement tables.
Results
of the 81,087 deaths from the diseases studied here, 75.1% were classified as avoidable; elimination of avoidable deaths due to circulatory system diseases was found to generate the greatest potential life expectancy gains, followed by neoplasms among females and external causes among males.
Conclusion
magnitude of lost life expectancy due to avoidable deaths differs between males and females; sex differentials in avoidable mortality therefore persist, producing a series of challenges.
Key words: Mortality; Life Expectancy; Life Tables; Cross-Sectional Studies
Introduction
Ever since the mid 19th century, mortality levels and patterns according to sex have been changing.1 Health-related technological progress, as well as improvements in quality of life, have led to a reduction in mortality and gains in lifespan.2 Standing out among the phenomena that accompany this process of transition is the production of mortality differentials among population subgroups3 and the predominance of deaths from chronic noncommunicable diseases (NCDs).4
The non-uniform trend in mortality reduction over time has produced differentials between the sexes. Practically all the world’s countries report higher male mortality than female mortality, while life expectancy at all ages is usually greater among females.1,5 Value has been placed on social, behavioral and biological aspects in the attempt to explain why female indicators are better.1,3,5
Even in view of these differences, the continuing fall in mortality has contributed to males and females surviving for longer and living to a ripe old age, both in high income countries and in middle and low income countries.2 In 2010, noncommunicable diseases accounted for 73.9% of deaths registered in Brazil;7 in particular cardiovascular diseases, neoplasms and external causes have led the way in the country’s overall mortality profile.7
As levels of life expectancy in Brazil have come closer to those experienced by high income countries, a reduction in the rhythm of this process of convergence have begun to be seen.2 This phenomenon has arisen firstly because reduction in deaths from communicable and parasitic diseases does not leave much room for life expectancy gains and, secondly, it has arisen as a consequence of a rise in NCDs, due to behaviors associated with alcoholism and tobacco smoking, among other factors.2
In high income countries, reduction in mortality in older age groups, a result of prevention campaigns and availability of new forms of treatment, has contributed to life expectancy gains reaching higher levels.5 With regard to the Brazilian case, it is also possible to envisage a scenario of potential gains in life expectancy, given that part of causes of death are considered avoidable, i.e. preventable, partially or totally, through adequate health care.9
The objective of this study was to estimate potential life expectancy gains and differences between males and females, if avoidable deaths from circulatory system diseases, neoplasms and external causes had been eliminated in São Paulo, SP, Brazil, in the period 2014- 2016.
Methods
This was a cross-sectional study of avoidable deaths from external causes, neoplasms and circulatory system diseases, in the population aged between 5 and 74 years old, in the municipality of São Paulo between 2014 and 2016.
Information about deaths was provided by the National Health System Information Technology Department (DATASUS) via its Mortality Information System (SIM).10 The population of São Paulo at the middle of the reference year, stratified by age groups and sex, was based on estimates made by the Brazilian Institute of Geography and Statistics (IBGE), retrieved from the DATASUS website.11 Death registry coverage in the municipality of São Paulo has been considered to be complete since 1940,12 thus justifying the choice of that municipality for this study.
The data used in this study consisted of the total number of deaths from avoidable causes and the total number of death from all causes, as described in three chapters of the International Statistical Classification of Diseases and Related Health Problems - 10th revision (ICD-10)13 as follows:
II – neoplasms;
IX – circulatory system diseases; and
XX – external causes of morbidity and mortality.
Figure 1 presents the composition of the selected groups of causes of death, according to the classification given by the ‘Brazilian National Health System List of Deaths Avoidable by Intervention’, for individuals aged 5 to 74 years old.9
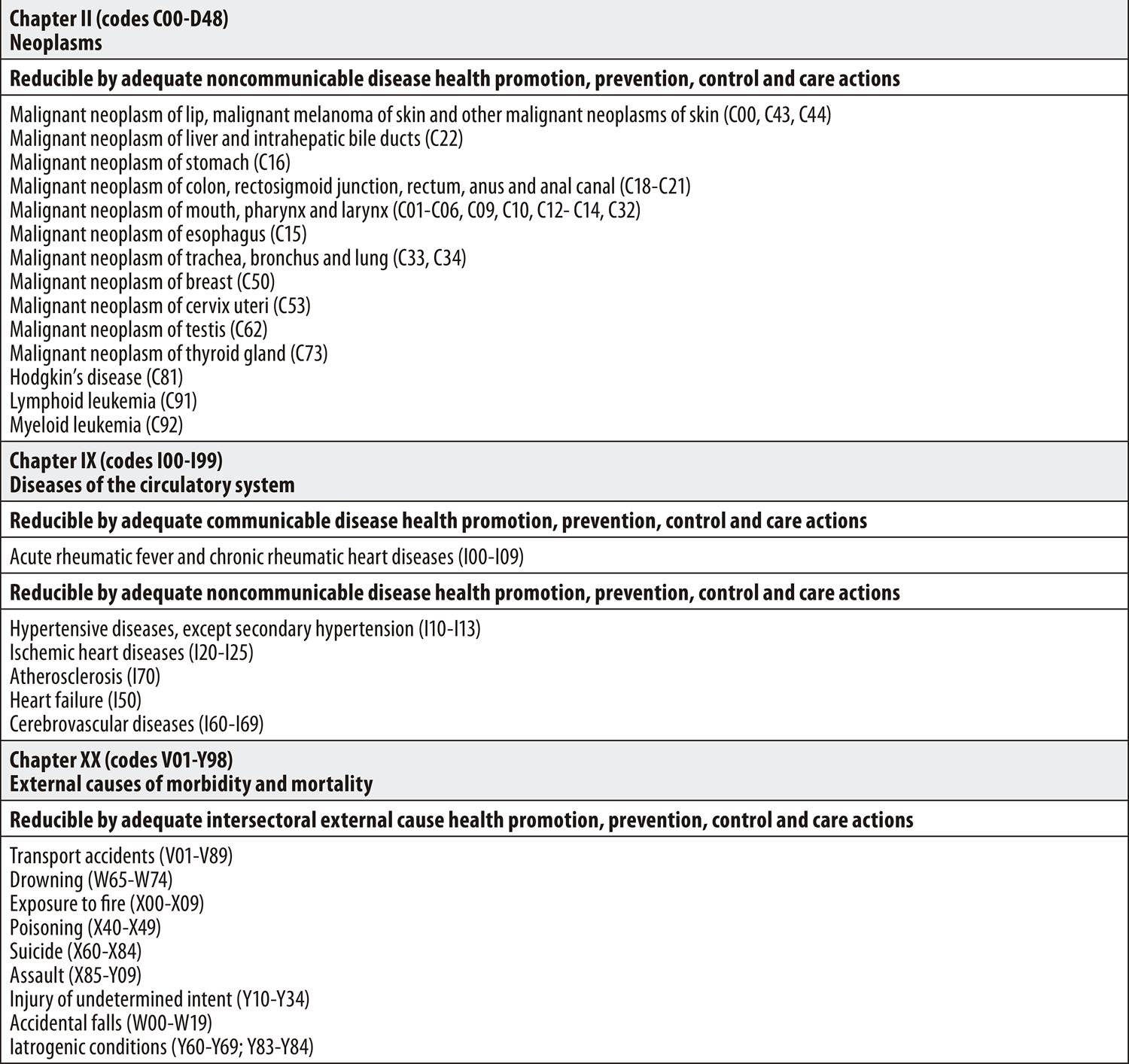
Source: ‘Brazilian National Health System List of Causes of Death Avoidable by Interventions’.(9)
Figure 1 – Brazilian National Health System List of Causes of Death Avoidable by Interventions, organized as per chapters of the International Statistical Classification of Diseases and Related Health Problems - 10th revision (ICD-10), for individuals between 5 and 74 years old
The ratio between specific male and female mortality rates was calculated in order to verify the age pattern of the mortality differential between the sexes, by cause of death. This measurement compares mortality between males and females:1 a ratio greater than 1 indicates that males are experiencing higher risk of mortality than females in the same age group; a ratio less than 1 suggests that females are at a disadvantage in terms of mortality; and a ratio equal to 1 suggests that both sexes have the same risk of death.
Following this, multiple decrement tables for males and females were calculated in order to analyze the impact of avoidable deaths on the likelihood of death and on life expectancy.14This analysis was performed excluding one cause of death group at a time, only taking into consideration avoidable deaths among individuals aged 5 to 74 years old. The mean number of deaths that occurred between 2014 and 2016 was used as the numerator of the specific mortality rates, with the aim of reducing the impact of random fluctuations.
The approach used in the table associated with a single decrement presumes that the function of the force of mortality from cause i is proportional to the function of the force of decrement for all causes together in the age interval x to x+n.14 The difference between total life expectancy, exact age x, and life expectancy and exact age x, when excluding a group of causes of death i, enables assessment of the indicator’s potential gain after eliminating each cause.14
Finally, the relative differences between the crude and adjusted probabilities of death were obtained. The former refers to probability of death in the age group, taking into consideration all causes of death; the latter refers to the age group’s new probability of death, after eliminating the selected group of cause of death.14
The analysis was performed using Microsoft Excel 2016. This study was conducted based on the ethical principals defined in National Health Council Resolution No. 466, dated December 12th 2012. Public domain secondary data was used with no nominal data capable of enabling people to be identified. As such, the study project did not need to be registered and assessed by the Research Ethics Committee/National Research Ethics Commission (CEP/CONEP) system.
Results
Between 2014 and 2016, 75% (60,919) of the 81,087 deaths from neoplasms, circulatory system diseases and external causes that occurred in the municipality of São Paulo were classified as avoidable. Out of the total of 29,573 deaths registered as being due to neoplasms in São Paulo in the period studied, 61% (18,168) were classified as avoidable, approximately 50% of which were female and 50% male. With regard to the 37,377 deaths from circulatory system diseases, 77% (28,663) were deaths that were on the SUS list of deaths avoidable through interventions, 62% of which were male deaths and 38% were female. In relation to deaths from external causes, the differences were however even more pronounced: 99.7% of the 14,137 deaths from these causes were considered to be avoidable, 84% of which were male (Table 1). Avoidable mortality was clearly significantly greater among males in comparison to females for all causes of death studied.
Table 1 – Distribution of neoplasm, circulatory system diseases and external cause avoidable and unavoidable deaths, São Paulo, SP, 2014-2016
| Causes of death | Deaths | Proportion (%) | ||||
|---|---|---|---|---|---|---|
| Male | Female | Total | Male | Female | ||
| Neoplasms (N) | Avoidable | 9,177 | 8,991 | 18,168 | 50.51 | 49.49 |
| Unavoidable | 5,849 | 5,556 | 11,405 | 51.28 | 48.72 | |
| Total | 15,026 | 14,547 | 29,573 | 50.81 | 49.19 | |
| Circulatory System (CS) Diseases | Avoidable | 17,744 | 10,919 | 28,663 | 61.91 | 38.09 |
| Unavoidable | 5,202 | 3,512 | 8,714 | 59.70 | 40.30 | |
| Total | 22,946 | 14,431 | 37,377 | 61.39 | 38.61 | |
| External causes (EC) | Avoidable | 11,798 | 2,290 | 14,088 | 83.75 | 16.25 |
| Unavoidable | 39 | 10 | 49 | 79.59 | 20.41 | |
| Total | 11,837 | 2,300 | 14,137 | 83.73 | 16.27 | |
| (N) + (CS) + (EC) | Avoidable | 38,719 | 22,200 | 60,919 | 63.56 | 36.44 |
| Unavoidable | 11,090 | 9,078 | 20,168 | 54.99 | 45.01 | |
| Total | 49,809 | 31,278 | 81,087 | 61.43 | 38.57 | |
Better results for the female sex were found not only with regard to death distribution but also in relation to risk of death, represented by the ratio between the mortality coefficients (Table 2). Risk of death was greater among males than among females in practically all age ranges and avoidable cause groups. The only exception was the 25-49 age group in which risk of death from avoidable neoplasms was greater among females than among males.
Table 2 – Sex ratio between specific mortality rates, São Paulo, SP, 2014-2016
| Age range (in years) | Sex ratio between specific mortality rates | ||
|---|---|---|---|
| Neoplasms | Circulatory system diseases | External causes | |
| 5-9 | 1.61 | 1.28 | 1.09 |
| 10-14 | 1.12 | 1.12 | 2.45 |
| 15-19 | 1.81 | 3.22 | 9.75 |
| 20-24 | 1.18 | 3.10 | 8.12 |
| 25-29 | 0.80 | 2.61 | 7.09 |
| 30-34 | 0.53 | 2.23 | 7.23 |
| 35-39 | 0.54 | 2.06 | 5.67 |
| 40-44 | 0.52 | 1.82 | 6.82 |
| 45-49 | 0.74 | 2.02 | 6.61 |
| 50-54 | 1.01 | 2.14 | 5.67 |
| 55-59 | 1.28 | 2.10 | 4.63 |
| 60-64 | 1.56 | 2.31 | 4.15 |
| 65-69 | 1.65 | 2.04 | 2.85 |
| 70-74 | 1.81 | 1.86 | 2.26 |
The external causes group had the highest ratios. The indicator had a rising trend among the younger age groups, and fell with effect from the 40 year-olds. The highest ratio was found in the 15-19 age group, in which risk of male deaths from avoidable external causes was almost twice that of females. A similar pattern was found for avoidable diseases of the circulatory system, albeit at lower levels: the main disadvantage was also found in the 15-19 age group, although risk of death from these causes was 3.22 times higher for males than for females.
Table 3 shows life expectancy when selected avoidable causes were excluded. Greatest life expectancy at birth for males (76.33 years) and for females (83.26 years), was obtained after excluding deaths from avoidable circulatory system diseases. At birth, male life expectancy would have increased by 2.44 years (3.3%), while for females it would have increased by 1.69 years (2.1%). This increase reached 7.9% (1.65 year) at age 60 for males and 4.5% (1.15 year) for females.
Table 3 – Life expectancy gain when the avoidable cause group is eliminated, São Paulo, SP, 2014-2016
| Males | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Age (in years) | ex | Neoplasms | Circulatory system diseases | External causes | ||||||
| ex- i | ex-i - ex | (%) | ex- i | ex-i - ex | (%) | ex- i | ex-i - ex | (%) | ||
| 0 | 73.89 | 75.21 | 1.32 | 1.8 | 76.33 | 2.44 | 3.3 | 75.84 | 1.95 | 2.6 |
| 5 | 70.05 | 71.34 | 1.29 | 1.8 | 72.48 | 2.43 | 3.5 | 72.03 | 1.98 | 2.8 |
| 10 | 65.11 | 66.39 | 1.28 | 2.0 | 67.54 | 2.43 | 3.7 | 67.08 | 1.97 | 3.0 |
| 15 | 60.19 | 61.47 | 1.28 | 2.1 | 62.62 | 2.43 | 4.0 | 62.12 | 1.94 | 3.2 |
| 20 | 55.68 | 56.96 | 1.28 | 2.3 | 58.10 | 2.42 | 4.3 | 57.28 | 1.60 | 2.9 |
| 25 | 51.19 | 52.47 | 1.28 | 2.5 | 53.59 | 2.41 | 4.7 | 52.48 | 1.29 | 2.5 |
| 30 | 46.59 | 47.87 | 1.28 | 2.7 | 48.98 | 2.40 | 5.1 | 47.66 | 1.08 | 2.3 |
| 35 | 41.98 | 43.26 | 1.28 | 3.0 | 44.36 | 2.37 | 5.7 | 42.89 | 0.90 | 2.2 |
| 40 | 37.43 | 38.70 | 1.27 | 3.4 | 39.77 | 2.34 | 6.2 | 38.18 | 0.75 | 2.0 |
| 45 | 32.98 | 34.23 | 1.25 | 3.8 | 35.25 | 2.26 | 6.9 | 33.60 | 0.62 | 1.9 |
| 50 | 28.72 | 29.93 | 1.20 | 4.2 | 30.85 | 2.13 | 7.4 | 29.23 | 0.51 | 1.8 |
| 55 | 24.71 | 25.83 | 1.12 | 4.5 | 26.64 | 1.92 | 7.8 | 25.12 | 0.41 | 1.7 |
| 60 | 20.97 | 21.93 | 0.96 | 4.6 | 22.63 | 1.65 | 7.9 | 21.31 | 0.34 | 1.6 |
| 65 | 17.53 | 18.27 | 0.74 | 4.2 | 18.80 | 1.27 | 7.3 | 17.81 | 0.27 | 1.6 |
| ≥70 | 14.41 | 14.89 | 0.49 | 3.4 | 15.21 | 0.81 | 5.6 | 14.62 | 0.22 | 1.5 |
|
| ||||||||||
| Female | ||||||||||
| Age (in years) | ex | Neoplasms | Circulatory system diseases | External causes | ||||||
| ex- i | ex-i - ex | (%) | ex- i | ex-i - ex | (%) | ex- i | ex-i - ex | (%) | ||
|
| ||||||||||
| 0 | 81.57 | 83.00 | 1.42 | 1.7 | 83.26 | 1.69 | 2.1 | 82.11 | 0.54 | 0.7 |
| 5 | 77.67 | 79.07 | 1.40 | 1.8 | 79.33 | 1.67 | 2.1 | 78.21 | 0.54 | 0.7 |
| 10 | 72.72 | 74.12 | 1.40 | 1.9 | 74.39 | 1.67 | 2.3 | 73.25 | 0.53 | 0.7 |
| 15 | 67.78 | 69.18 | 1.40 | 2.1 | 69.45 | 1.67 | 2.5 | 68.30 | 0.52 | 0.8 |
| 20 | 62.92 | 64.31 | 1.39 | 2.2 | 64.58 | 1.66 | 2.6 | 63.40 | 0.48 | 0.8 |
| 25 | 58.08 | 59.47 | 1.39 | 2.4 | 59.73 | 1.65 | 2.8 | 58.52 | 0.44 | 0.8 |
| 30 | 53.24 | 54.61 | 1.37 | 2.6 | 54.88 | 1.64 | 3.1 | 53.64 | 0.40 | 0.8 |
| 35 | 48.42 | 49.77 | 1.35 | 2.8 | 50.04 | 1.62 | 3.4 | 48.79 | 0.37 | 0.8 |
| 40 | 43.68 | 44.98 | 1.30 | 3.0 | 45.27 | 1.60 | 3.7 | 44.02 | 0.34 | 0.8 |
| 45 | 39.01 | 40.24 | 1.23 | 3.2 | 40.55 | 1.54 | 4.0 | 39.33 | 0.32 | 0.8 |
| 50 | 34.47 | 35.60 | 1.13 | 3.3 | 35.93 | 1.45 | 4.2 | 34.77 | 0.30 | 0.9 |
| 55 | 30.08 | 31.08 | 1.00 | 3.3 | 31.41 | 1.33 | 4.4 | 30.36 | 0.28 | 0.9 |
| 60 | 25.88 | 26.70 | 0.82 | 3.2 | 27.03 | 1.15 | 4.5 | 26.14 | 0.26 | 1.0 |
| 65 | 21.87 | 22.50 | 0.63 | 2.9 | 22.81 | 0.94 | 4.3 | 22.12 | 0.24 | 1.1 |
| ≥70 | 18.14 | 18.56 | 0.42 | 2.3 | 18.77 | 0.63 | 3.5 | 18.35 | 0.21 | 1.2 |
Subtitle:
ex: life expectancy at exact age x.
ex-i: life expectancy at exact age x with elimination of deaths from avoidable causes i.
ex-i - ex: absolute gain.
% : relative gain.
Following this, the ICD chapters responsible for the biggest increases were external causes for males and neoplasms for females. When deaths from external causes were eliminated, the male sex had a potential gain of 1.95 year in life expectancy at birth (2.6%), while for females this gain would have been 0.54 year (0.7%). Males would have had a rising trend up until 20 years of age, reaching a gain of 2.9%, falling after this age until reaching 1.5% at 70 years old. In turn, excluding deaths from avoidable neoplasms would have led to a gain of 1.8% (1.32 year) in life expectancy at birth for males, and 1.7% (1.42 year) for females.
In relative terms, excluding deaths from neoplasms and diseases of the circulatory system resulted in a similar behavior, characterized by a rising percentage share up until the older age groups, after which a falling trend in these increases can be seen. The same applies to neoplasms, which reach a potential increase of life expectancy at 60 of approximately 4% for males and 3% for females.
Figure 2 shows the relative differences between crude probabilities of death (considering all causes of death selected) and adjusted probabilities of death (following the elimination of a group of causes). For males, the impact was greater when deaths from avoidable external causes were eliminated, hence why we opted to present the results of this cause separately in Figure 2a. Crude probability of death from external causes among males aged 15-20 was 220% higher than adjusted probability of death. Among females, the result of excluding this cause on probability was much lower than among males in all age groups.
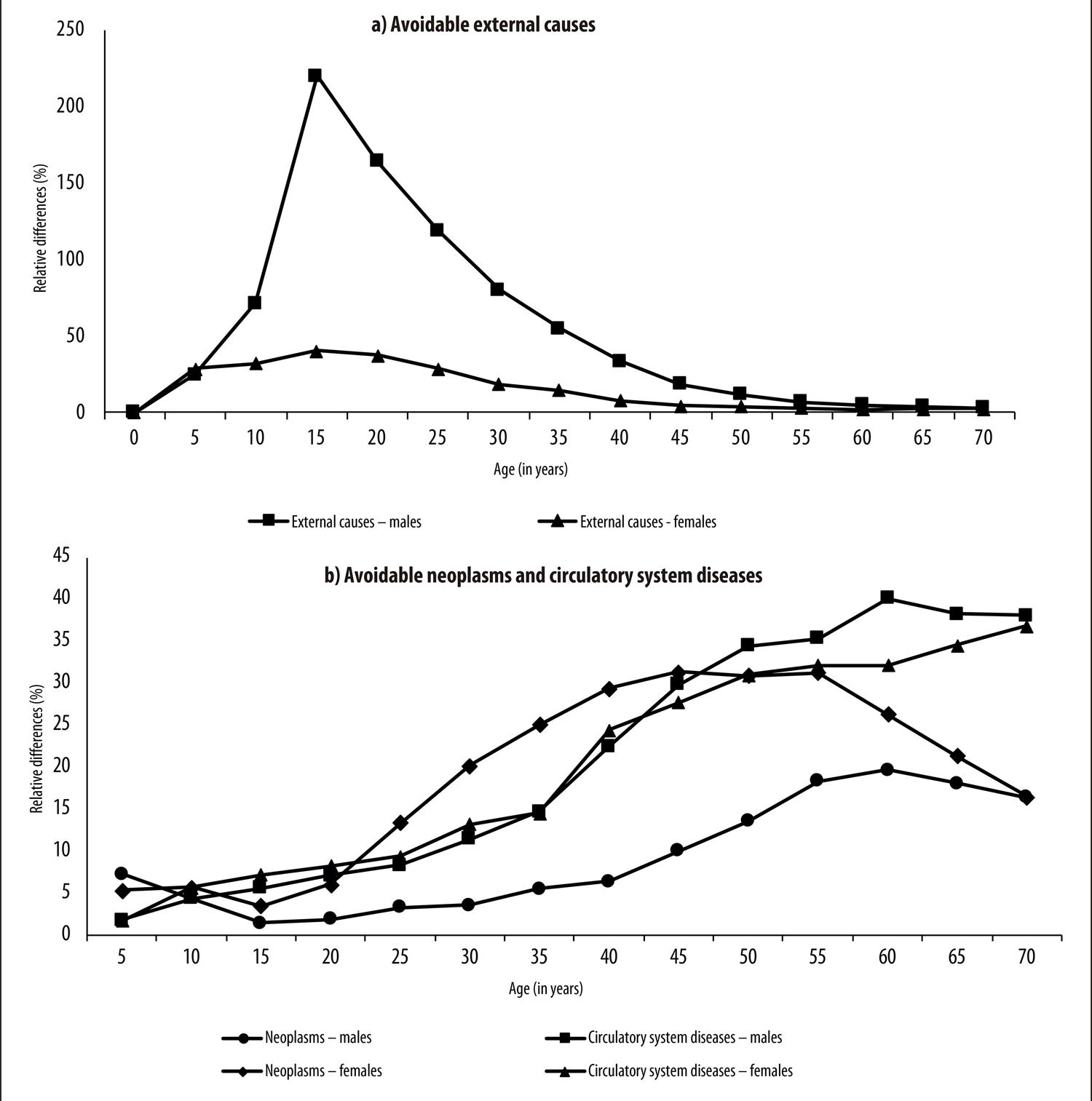
Figure 2 – Relative differences between crude and adjusted probabilities of death, by avoidable cause group and sex, São Paulo, SP, 2014-2016
The differentials in probability of death from the other causes are shown in Figure 2b. In the case of avoidable diseases of the circulatory system, reductions in probability of death were similar for males and females. However, up to 45 years of age, the difference was slightly greater among females, but after this age it became greater among males as age advanced. Elimination of this cause would account for the second largest impact on male probability differences in practically all age groups.
In the case of females, excluding avoidable neoplasms led to the biggest reductions in probability of death in practically all age ranges. The importance of eliminating this cause was found above all between 25 and 45 years of age, as this was where the biggest differences in probability of death were found.
Discussion
Avoidable mortality accounted for a considerable proportion of deaths in the municipality of São Paulo between 2014 and 2016. In this period, more than half of deaths from diseases of the circulatory system, neoplasms and external causes were classified as avoidable according to the ‘Brazilian National Health System List of Deaths Avoidable by Intervention’.9 Males in particular had a higher percentage of avoidable deaths than females, as well as greater risk of death, in practically ages and groups of avoidable causes. With regard to gains in life expectancy at birth, exclusion of death from avoidable diseases of the circulatory system resulted in gains in this indicator for both sexes.
In general, women’s behavior is more preventive than men’s, due to their using health services more and avoiding risk.15 In addition, it is important to highlight that differently to the reduction in communicable diseases that has occurred through efficacious treatment, such as antibiotics and vaccines and access to treated water, treatment of noncommunicable diseases has also taken place through individual prevention actions. As such, one of the reasons for the lower female mortality found could be female perception of the need to change lifestyle habits and adopt prevention behaviors.5 It is therefore reasonable to suppose that the higher proportion of deaths from avoidable causes among males is associated with these factors.
With regard to the age pattern of mortality between the sexes, males were found to be at a disadvantage in practically all age ages and groups of causes. The municipality of São Paulo appears to follow the trend of excess male mortality,16 found not only in terms of overall mortality but also in relation to specific causes of death.17 The only exception occurred in the 25-49 age range, in which females had higher risk of death from avoidable neoplasms than males. This result may be related to breast and cervical neoplasms which significantly affect young women.17
The highest sex ratios between mortality rates were found in the external causes group, specifically in younger males. This result can be explained by deaths from external causes, especially homicides and violence, principally among young and adult males.18 It must be stressed, however, that measurement of relative risk does not provide evidence about the magnitude of mortality rates experienced by each group.
In relation to potential life expectancy gains, when deaths from specific causes are excluded two distinct trends between the sexes become evident: by age; and by group of avoidable deaths. In relation to age, the analysis shows that in percentage terms the exclusion of any cause of death group would lead to a gain in life expectancy for males. With regard to cause of death group, however, the importance of each ICD chapter varies according to sex.
Generally speaking, avoidable circulatory system diseases produce considerable life expectancy gains for both sexes. The importance of reducing these deaths was also found by a national study conducted in Brazil, especially when excluding avoidable ischemic heart diseases, which resulted in gains of 1.3 year for males and 1.7 year for females.17
Due to advanced medical technology and changes in individual behavior, East European countries have made progress with treating cardiovascular diseases, thus increasing life expectancy to even higher levels. Not all societies are ready to make the most of the benefits of technological and medical innovations simultaneously: initially because there is divergence in life expectancy gains, followed by a process of convergence between countries.5 Given the trajectory of the developed countries, it is reasonable to imagine that diffusion of technology in developing countries can contribute to life expectancy gains through reduction in the cardiovascular disease mortality rate, given that more than half the deaths from circulatory system diseases were classified as avoidable in the period studied.
Among the female population, the potential gain in life expectancy when deaths from neoplasms were eliminated was greater than the gain from eliminating external causes. It is possible that this may be associated with higher risk of female deaths from avoidable neoplasms. In the case of males, the situation is reversed, as follows: as males are subject to higher mortality rates due to external causes, in terms of life expectancy, removing these deaths benefits males more than females. Ever since 1980, external causes have had a negative impact on mortality rate age structure in Brazil, contributing to life expectancy years being lost.2
Excess male mortality, both from circulatory system diseases and from external causes, was reflected in the analysis of the differentials between crude and adjusted probabilities of death. Excluding these groups of causes resulted in the biggest reductions in probability of male deaths. On the other hand, excess mortality in females was found in relation to neoplasms in adult age groups, and a greater fall in probability of death occurred when this cause group was excluded.
Early mortality and disabilities, principally due to noncommunicable causes, have given rise to economic and social costs for society, including increased use of resources for health treatment, loss or reduction in production capacity, early granting of retirement pensions and other benefits and, above all, reduction in the quality of life of affected people and their family members.8
Predominance of NCDs, as a result of the process of epidemiological transition, leads to increased health expenditure, given the need to incorporate new technologies in treatments which are generally long and from which patients are slow to recover.8 When someone becomes ill or dies, the expected flow of income during their lifespan is reduced and, consequently, there is a loss of economic resources due to reduced hours/years of productive life.20 Loss of production attributed to deaths from homicides is the most significant among all external causes, precisely because of their greater incidence among young males, whose income is relatively higher and who also have a greater economically active life expectancy than young females.20
Disabilities caused by a disease can also result in high costs, principally due to long periods of time off work and retirement pensions and other benefit payments.19 It is therefore important to remember that fact that these health conditions and deaths are classified as avoidable and, therefore, totally or partially preventable, as well as reflecting access to health services and quality of service delivery.9Adopting health promotion and prevention actions, in addition to being a way towards new life expectancy gains, can represent a strategy for reducing overall health system costs, as well as the economic and social costs of deaths and disabilities.
Investigation of the main causes of avoidable morbidity and mortality, their distribution in different geographic spaces and populations, can contribute to making health policy decisions aimed at service quality and reducing inequalities between specific social classes and segments.
A limitation of this study is related to the short period of time analyzed and the causes of death selected. Comparative analysis over time, along with more specific studies of avoidable deaths (ICD-10 categories) could provide relevant information for health service evaluation and designing more efficient public policies.
The results of this study point to a high proportion of avoidable deaths when examining the main causes of death among the population of the municipality of São Paulo. Generally speaking, these deaths generate a loss in life expectancy at birth and an impact of different magnitudes on the probability of male and female deaths. The conclusion is reached that sex differentials in avoidable mortality persist, producing a series of challenges not only for health care policies but also for policies intended to reduce inequalities faced by specific population groups.
REFERENCES
1. Wisser O, Vaupel JW. The sex differential in mortality: a historical comparison of the adult-age pattern of the ratio and the difference. MPIDR Working Paper [Internet]. 2014 Jun [cited 2020 Apr 20];005:1-17. Available from: https://doi.org/10.4054/MPIDR-WP-2014-005 [ Links ]
2. Albuquerque FRPC, Silva LGC. Tendências dos níveis e padrões de mortalidade e seus diferenciais regionais no período 2000-2030: Brasil, Grandes Regiões e Unidades da Federação. In: Ervatti LR, Borges GM, Jardim AP (Ed.). Mudança demográfica no Brasil no início do século XXI subsídios para as projeções da população. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2015. [ Links ]
3. Sundberg L, Agahi N, Fritzell J, Fors S. Why is the gender gap in life expectancy decreasing? The impact of age and cause-specific mortality in Sweden, 1997-2014. Int J Public Health [Internet]. 2018 Jul [cited 2020 Apr 20];63(6):673-81. Available from: https://doi.org/10.1007/s00038-018-1097-3 [ Links ]
4. Omran AR. The epidemiologic transition: a theory of the epidemiology of population change. Milbank Mem Q [Internet]. 1971 Oct [cited 2020 Apr 20];49(4):509-38. Available from: https://doi.org/10.1111/j.1468-0009.2005.00398.x [ Links ]
5. Vallin J, Meslé F. Convergences and divergences in mortality: a new approach to health transition. Demographic Research. Dem Res [Internet]. 2004 Apr [cited 2020 Apr 20];Special Collection 2(2):11-44. Available from: https://doi.org/10.4054/DemRes.2004.S2.2 [ Links ]
6. Yokota, RT, Nusselder WJ, Robine JM, Tafforeau J, Renard F, Deboosere P, et al. Contribution of chronic conditions to gender disparities in health expectancies in Belgium, 2001, 2004 and 2008. Eur J Public Health [Internet]. 2018 Feb [cited 2020 Apr 20];29(1):82-7. Available from: https://doi.org/10.1093/eurpub/cky105 [ Links ]
7. Guimarães RM, Andrade SSCA, Machado EL, Bahia CA, Oliveira MM, Jacques FVL. Diferenças regionais na transição da mortalidade por doenças cardiovasculares no Brasil, 1980 a 2012. Rev Panam Salud Pública [Internet]. 2015 [citado 2020 abr 20];37(2):83-9. Disponível em: https://scielosp.org/article/rpsp/2015.v37n2/83-89/ [ Links ]
8. Schramm JMA, Oliveira AF, Leite IC, Valente JG, Gadelha AMJ, Portela MCP, et al. Transição epidemiológica e o estudo de carga de doença no Brasil. Ciênc Saúde Coletiva [Internet]. 2004 out-dez [citado 2020 abr 20];9(4):897-908. Disponível em: https://doi.org/10.1590/S1413-81232004000400011 [ Links ]
9. Malta DC, Duarte EC, Almeida MF, Dias MAS, Morais Neto OL, Moura L, et al. Lista de causas de mortes evitáveis por intervenções do Sistema Único de Saúde do Brasil. Epidemiol Serv Saúde [Internet]. 2007 out-dez [citado 2020 abr 20];16(4):233-44. Disponível em: http://dx.doi.org/10.5123/S1679-49742007000400002 [ Links ]
10. Ministério da Saúde (BR). Departamento de Informática do Sistema Único de Saúde – Datasus. Óbitos por causas evitáveis – 5 a 74 anos [Internet]. Brasília: Ministério da Saúde; 2019 [citado 2020 abr 20]. Disponível em: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sim/cnv/evitb10sp.def [ Links ]
11. Ministério da Saúde (BR). Departamento de Informática do Sistema Único de Saúde – Datasus. População residente [Internet]. Brasília: Ministério da Saúde; 201- [citado 2020 abr 20]. Disponível em: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?novapop/cnv/popbr.def [ Links ]
12. Paes NA, Albuquerque MEE. Avaliação da qualidade dos dados populacionais e cobertura dos registros de óbitos para as regiões brasileiras. Rev Saúde Pública [Internet]. 1999 fev [citado 2020 abr 20];33(1):33-43. Disponível em: https://doi.org/10.1590/S0034-89101999000100006 [ Links ]
13. World Health Organization. International statistical classification of diseases and related health problems [Internet]. 10th rev, 7th ed. Geneva: World Health Organization; 2016 [cited 2020 Apr 20]. 195 p. Available from: https://www.who.int/classifications/icd/ICD10Volume2_en_2010.pdf [ Links ]
14. Preston SH, Heuveline P, Guillot M. Demography: measuring and modeling population process. Massachusets: Blackweil Publishers; 2001. [ Links ]
15. Kanso S. Causas de morte evitáveis para a população idosa [tese]. Rio de Janeiro (RJ): Fundação Instituto Oswaldo Cruz; 2011. Disponível em: https://pesquisa.bvsalud.org/enfermeria/resource/pt/lil-616666 [ Links ]
16. Abreu DMX, César CC, França EB. Relação entre as causas de morte evitáveis por atenção à saúde e a implementação do Sistema Único de Saúde no Brasil. Rev Panam Salud Pública [Internet]. 2007 abr [citado 2020 abr 20];21(5):282-91. Disponível em: https://www.scielosp.org/pdf/rpsp/2007.v21n5/282-291 [ Links ]
17. Abreu DMX, César CC, França EB. Diferenciais entre homens e mulheres na mortalidade evitável no Brasil (1983-2005). Cad Saúde Pública [Internet]. 2009 dez [citado 2020 abr 20];25(12):2672-82. Disponível em: https://doi.org/10.1590/S0102-311X2009001200014 [ Links ]
18. Moura EC, Gomes R, Falcão MTC, Schwarz E, Neves ACM, Santos W. Desigualdades de gênero na mortalidade por causas externas no Brasil, 2010. Ciênc Saúde Coletiva [Internet]. 2015 mar [citado 2020 abr 20];20(3):779-88. Disponível em: https://doi.org/10.1590/1413-81232015203.11172014 [ Links ]
19. Carter HE, Schofield D, Rupendra S. The long-term productivity impacts of all cause premature mortality in Australia. Aust N Z J Public Health [Internet]. 2016 Apr [cited 2020 Apr 20];41(2):137-43. Available from: https://doi.org/10.1111/1753-6405.12604 [ Links ]
20. Carvalho AX, Cerqueira DRC, Rodrigues RI, Lobão WJA. Custos das mortes por causas externas no Brasil [Internet]. Brasília: Instituto de Pesquisa Econômica Aplicada; 2007 [citado 2020 abr 20]. 45 p. (Texto para Discussão, 1268). Disponível em: https://www.ipea.gov.br/portal/index.php?option=com_content&view=article&id=4497 [ Links ]
21. Cervantes CAD, Montaño AMP. Análisis de la tendencia e impacto de la mortalidad por causas externas: México; 2000-2013. Salud Colect. 2016;12(2):251-64. [ Links ]
22. Siqueira ASE, Siqueira-Filho AGS, Land MGP. Analysis of the economic impact of cardiovascular diseases in the last five years in Brazil. Arq Bras Cardiol [Internet]. 2017 Jul [cited 2020 Apr 20];109(1):39-46. Available from: https://doi.org/10.5935/abc.20170068 [ Links ]
23. Carter HE, Schofield DJ, Shrestha R. The productivity costs of premature mortality due to cancer in Australia: evidence from a microsimulation model. PLoS One [Internet]. 2016 Dec [cited 2020 Abr 20];11(12). Available from: https://doi.org/10.1371/journal.pone.0167521 [ Links ]
24. Carter HE, Schofield D, Shrestha R. Productivity costs of cardiovascular disease mortality across disease types and socioeconomic groups. Open Heart [Internet]. 2019 Feb [cited 2020 Apr 20];6(1): e000939. Available from: https://doi.org/10.1136/openhrt-2018-000939 [ Links ]
Associate editor: Lucia Rolim Santana de Freitas - orcid.org/0000-0003-0080-2858 Vivian Siqueira Santos Gonçalves - orcid.org/0000-0001-6893-8263
Received: February 02, 2019; Accepted: March 30, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
