










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.31 no.1 Brasília 2022 Epub 22-Abr-2022
http://dx.doi.org/10.1590/s1679-49742022000100015
Original Article
Factors associated with the reduction of dental care in Primary Health Care in Brazil after the emergence of COVID-19: a cross-sectional study, 2020
1 Universidade Federal de Pelotas, Faculdade de Medicina, Pelotas, RS, Brazil
2 Universidade Federal de Pelotas, Faculdade de Odontologia, Pelotas, RS, Brazil
Objective:
To analyze factors associated with the reduction of dental care in Primary Health Care, during the COVID-19 pandemic in Brazil.
Methods:
This was a cross-sectional study conducted with dentists in primary healthcare centers (PHCCs). The reduction of dental care was the outcome, and the exposure variables were sociodemographic data, availability of personal protective equipment (PPE) and measures adopted by PHCCs during the pandemic. Poisson regression was performed to determine the prevalence ratio and 95% confidence interval (95%CI).
Results:
Of the total of 958 participants, 62.6% reported a reduction of over 50% in dental visits after the beginning of the pandemic. Adoption of biosafety protocols (PR = 1.04; 95%CI 1.01;1.07), availability of PPE recommended by new protocols (PR = 0.94; 95%CI 0.89;0.99) and adoption of tele-screening (PR = 0.90; 95%CI 0.85;0.96) were associated with the reduction.
Conclusion:
The availability of new types of PPE and implementation of tele-screening in PHCCs seem to have minimized the reduction of dental care after the beginning of the pandemic.
Keywords: Oral Health Care Services; Primary Health Care; COVID-19; Personal Protective Equipment; Cross-Sectional Studies
Study Contributions
Main results
Adoption of biosafety protocols may have contributed to the reduction of dental care after the emergence of COVID-19. However, the availability of PPE and the implementation of tele-screening in PHCCs may have minimized this reduction.
Introduction
In March 2020, the World Health Organization (WHO) declared COVID-19 a pandemic.1 According to data made available by Johns Hopkins University, as of early February 2022, the COVID-19 pandemic had affected 386,891,974 people and caused 5,707,157 deaths worldwide. Brazil has been one of the hardest hit countries by the pandemic. It holds the third highest number of cases and the second highest death toll, in the world.2
The spread of SARS-CoV-2 virus during aerosol generating procedures makes dentistry one of the professions at highest risk of COVID-19 transmission, with the risk of contagion for both the professional and users of dental services, through cross infection.3 Therefore, the American Dental Association recommended dentists postponed elective dental procedures, concentrating only on dental emergencies.4
In Brazil, the Ministry of Health, Agência Nacional de Vigilância Sanitária (Anvisa), Conselho Federal de Odontologia (CFO) and dental organizations also recommended that elective dental procedures should be limited during the pandemic.5,6 Some of these reductions have already been documented in the literature. A survey conducted at the beginning of the pandemic, involving Brazilian dentists who work in the public and private sectors, showed a 95% reduction in dental procedures, with a greater activity restriction in the hardest hit regions by the pandemic.6 Studies that assessed the number of dental procedures performed in the Brazilian National Health System (SUS), based on data available on the Brazilian National Health System Information Technology Department (DATASUS), showed a reduction of almost 90% in pediatric dental care,7 66.7% in the fabrication for dentures8 and 68.8% in oral biopsies9 during the pandemic, compared to the period prior to COVID-19.
In addition to the measures to limit elective dental care, the use of additional personal protective equipment (PPE), which were not part of the routine care prior to the pandemic, was also recommended in order to control COVID-19 transmission in the dental office environment. According to biosafety manuals, in the scenario of the COVID-19 pandemic, professionals should perform dental procedures wearing a waterproof cross back apron, cap, gloves, facial respirator (N95 or similar), surgical mask, goggles and face shields.5,10 However, the high demand and increase in PPE prices, in addition to the priority allocation of the use of this equipment by health professionals providing care to people with COVID-19, caused scarcity of this equipment, which may have affected dental procedures globally.11
In order to reduce the impact on the population oral health, given the reduction of dental care during the COVID-19 pandemic, especially among the most vulnerable individuals, a situational diagnosis is necessary to develop strategies to cope with the problem. Despite the large number of publications on COVID-19 in 2020, no studies were found to evaluate the factors associated with the reduction in the number of dental procedures performed in primary health care (PHC) in Brazil. The objective of this work was to analyze the factors associated with the reduction in the number of dental procedures performed in PHC, in Brazil during the COVID-19 pandemic.
Methods
This study was reported according to the recommendations of the Checklist for Reporting Results of Internet E-Surveys (CHERRIES).12 This was a cross-sectional study conducted with dentists working in PHC, in Brazil, that is, those who are linked to some PHCCs in the public health service and answered an online questionnaire.
Recent data show that Brazil has more than 360,000 dentists, of whom approximately 26.0% (95,000) work in the public health sector,13 at different levels of care, notwithstanding unevenly distributed among the national macro-regions: most of them in the states of São Paulo (28.0%), Minas Gerais (12.0%) and Rio de Janeiro (9.4%), and the lowest percentage in Roraima (0.3%).13 The sample size was calculated using the OpenEPI©, a web-based software. Considering a 50% prevalence, 5.0% alpha and 30.0% of losses, it would be necessary the participation of 635 dentists from different regions of Brazil to estimate the prevalence that was proposed for the study, whose target population was comprised of dentists linked to PHCCs. The criteria for participation in the study were: being a dentist, working in a PHCC in Brazil and working in person at the time of data collection.
We used social media for the recruitment of dentists. In order to disseminate the study, the researchers shared the link to access the questionnaire on the study Instagram® account (@saude.bucal_covid19) and on Facebook groups®, more specifically, 'Odontologia do Brasil' and 'Odontologia e o SUS'. In addition, outreach emails were sent to a total of 21,404 dentists working in the public sector.
Data collection included the development of an online self-administered questionnaire on dental care conditions at PHCCs, after the emergence of COVID-19. The instrument was stored on Google® Forms between July 28 and August 17, 2020. Strategies were carried out to check the consistency of the data obtained in this study. Initially, a self-administered questionnaire was developed, in which the participants answered all questions related to their PHCC. In addition, the selection of a single answer option was applied to all questions, and the items provided a non-applicable answer option, as 'not applicable'. Thus, there were no questions left unanswered. Finally, the verification of duplicate questionnaires was performed by checking the e-mails provided by the participants during the study. When there were two or more questionnaires that had been registered using the same e-mail address, the last one was the questionnaire that we took into consideration.
The items of the questionnaire were pre-tested by ten dentists working in the public sector, although linked to medium complexity services. Each participant evaluated the clarity of the survey questions. The evaluators answered the questionnaire and recorded the time of completion, and pointed out the questions to be reviewed by the researchers. The mean time of completion of the questionnaire was 12 minutes.
The questionnaire was developed in five blocks, separated according to the themes listed below.
Region of Brazil where he/she works: North; Northeast; Midwest; Southeast; South.
-
Monitoring measures and biosafety protocols adopted by the PHCC after the emergence of COVID-19:
- Implementation of the tele-screening service (yes; no); and
- adoption of new biosafety protocols (yes; no).
-
Information related to the PPE used by dental professionals:
- availability of all types of mandatory PPE for dental care, recommended by biosafety protocols after the emergence of COVID-19, which were not previously part of dental practice (N955/PFF2 mask, disposable apron and face shield), being considered as 'yes' when the three types of PPE were available and 'no' when at least one type of PPE was not available); and
- a sufficient number of surgical masks, gloves and goggles (mandatory PPE), frequently used, that is, they were used in dental practice before the emergence of COVID-19; for each type of PPE, the participant answered the question: Was the amount of 'equipment named PPE' sufficient for all dental visits in the last month? (yes; no), being considered sufficient when the participant answered 'yes' to all types of PPE, and insufficient when the participant answered 'no' to at least one type of PPE.
-
Information related to the dentist:
- observes risk of COVID-19 infection during dental care (yes; no);
- has already been diagnosed with COVID-19 (yes; no); and
- has already taken the COVID-19 test (yes; no).
The outcome analyzed in this study was the proportional reduction in the number of dental procedures during the COVID-19 pandemic, compared to the period prior to its emergence. The information of the outcome was obtained through the following questions: On average, how many people, per shift, used to be seen at your PHCC before the emergence of COVID-19? and On average, how many people, per shift, have been seen at your PHCC after the emergence of COVID-19? The answers were collected in a discrete numerical way, and subsequently, organized into two categories for analysis purposes: reduction below 50.0%; reduction above 50.0%.
Statistical data analysis was performed using Stata 15.0 software (StataCorp LP; College Station, TX, USA). Initially, descriptive analyses were performed using absolute and relative frequencies, mean and standard deviation (SD). The association of the outcome (reduction of dental care after the emergence of the COVID-19 pandemic) with the exposure variables studied was analyzed using Pearson's chi-square test. Then, the prevalence ratios (PR) and their respective 95% confidence intervals (95%CI) were estimated by means of Poisson regression analysis, with robust variance adjustment. The model was adjusted applying the backward stepwise method, and the variables with level of association presenting p-value ≤0.20 were maintained. The selection of variables was carried out based on the hierarchical theoretical model presented in Figure 1A. For all statistical tests, a significance level of 5% was considered.
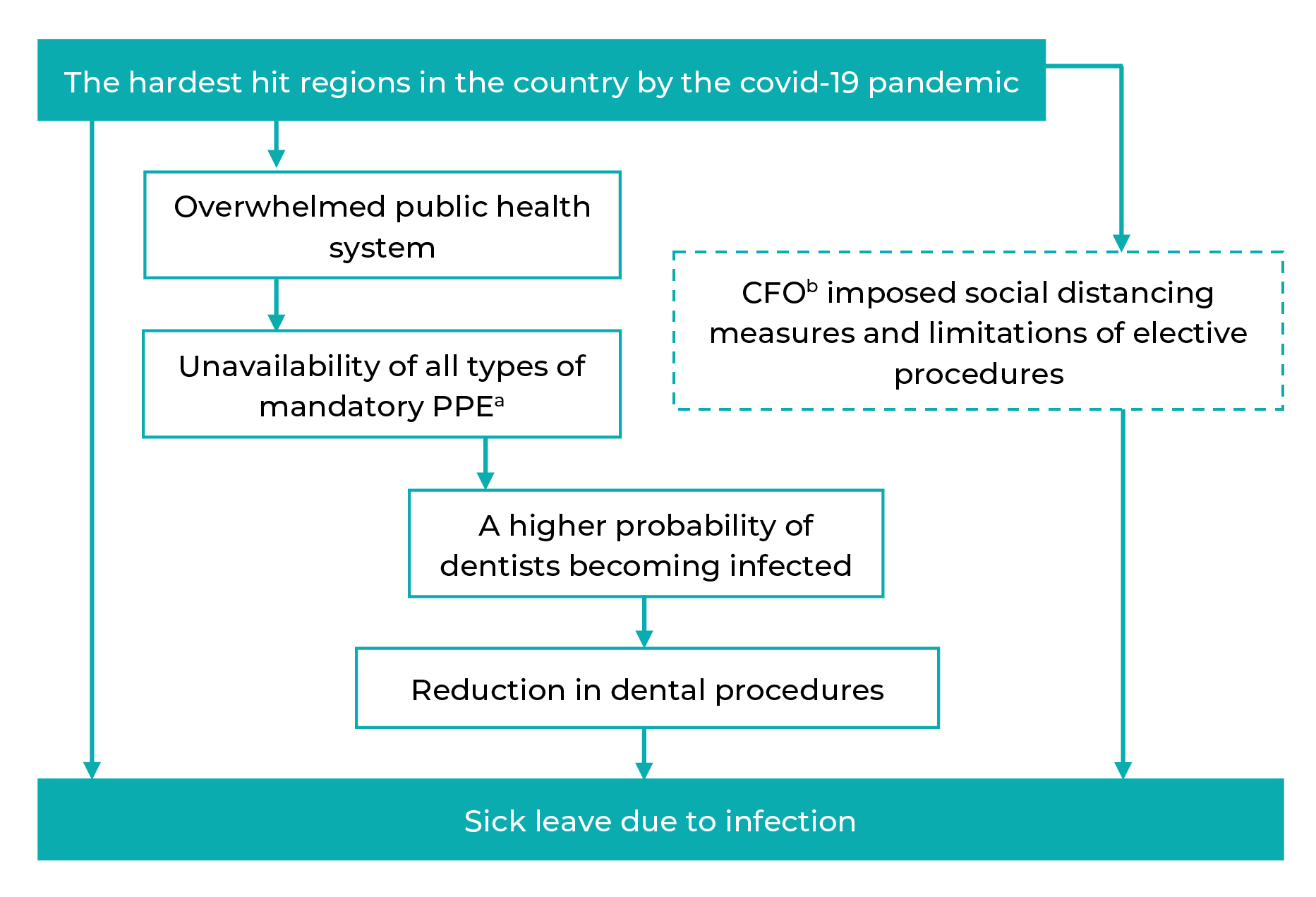
a) PPE: Personal protective equipment; b) CFO: Conselho Federal de Odontologia (Federal Board of Dentistry).
Figure 1A Conceptual theoretical model of reduction in dental procedures after the emergence of the COVID-19 pandemic and its associated factors, Brazil, 2020
The study received a favorable opinion from the Research Ethics Committee of the Faculty of Medicine of the Universidade Federal de Pelotas (CEP/FAMED/UFPel) on June 29, 2020. Certificate of Submission for Ethical Appraisal (CAAE) No. 33837220.4.00005317. All participants were informed about the objectives of the study and were assured about the confidentiality of the information provided. Those who agreed to participate had access to the electronic Free and Informed Consent Form and the questionnaire itself, which could only be read and answered after their 'acceptance' to participate.
RESULTS
958 dentists answered the questionnaire between July 28 and August 17, 2020. Table 1 shows the characteristics of dentists who performed dental treatments in the PHCCs in Brazil, during that period.
Table 1 Frequency distribution of demographic information and characteristics of Primary Health Care dentists linked to primary health centers, Brazil, 2020
| Variables | n | % |
|---|---|---|
| Regions of Brazil | 958 | |
| North | 29 | 3.0 |
| Northeast | 180 | 18.8 |
| Midwest | 53 | 5.5 |
| Southeast | 194 | 20.3 |
| South | 502 | 52.4 |
| All types of PPEa recommended by the new protocols have been made availableb | 951 | |
| No | 219 | 23.0 |
| Yes | 732 | 77.0 |
| PPEa for clinical routine prior to the pandemic has been sufficientc | 830 | |
| No | 210 | 25.3 |
| Yes | 620 | 74.7 |
| Risk for SARS-Cov-2 infection in professionals | 958 | |
| Yes | 897 | 93.6 |
| No | 61 | 6.4 |
| The PHCCd has tele-screening for COVID-19 | 958 | |
| Yes | 229 | 23.9 |
| No | 729 | 76.1 |
| The PHCCd has adopted COVID-19 protocols | 880 | |
| Yes | 607 | 69.0 |
| No | 273 | 31.0 |
| The professional has already been diagnosed with COVID-19 | 925 | |
| Yes | 47 | 5.1 |
| No | 878 | 94.9 |
| The professional has already taken the COVID-19 test | 955 | |
| Yes | 630 | 66.0 |
| No | 325 | 34.0 |
| Reduction in dental visits in PHCe during the COVID-19 pandemic >50.0% | 958 | |
| No | 358 | 37.4 |
| Yes | 600 | 62.6 |
a) PPE: Individual protective equipment; b) PPE recommended by the new protocols: PFF2/N95 mask, disposable apron and face shield; c) PPE for clinical routine prior to the pandemic: surgical mask, goggles and gloves; d) PHCC: Primary Healthcare Center; e) PHC: Primary Health Care.
Among the respondents, 502 (52.4%) were from the South region. With regard to PPE, 219 (23.0%) professionals reported that the mandatory PPE recommended by the new biosafety protocols related to COVID-19 (N95/PFF2 mask, disposable apron and face shield) was not made available, while 210 (25.3%) reported that the PPE used in routine dental care, prior to the COVID-19 pandemic, was not sufficient to provide dental care. Regarding the risk of infection caused by the SARS-Cov-2 virus, 897 (93.6%) reported that dental professionals were at risk of infection during dental care. At the time of the interview, 878 (94.9%) reported that they had not been diagnosed with COVID-19 and 630 (66.0%) reported having taken SARS-Cov-2 test at least once. Regarding the adoption of monitoring measures and biosafety protocols related to COVID-19 by the PHCC, 729 (76.1%) reported absence of tele-screening and 607 (69.0%) reported the adoption of new biosafety protocols. A total of 600 (62.6%) dentists reported a reduction of more than 50.0% in dental visits per shift at the PHCC, compared to the period before the beginning of the pandemic (Table 1).
Table 2 shows the average number of people receiving care per shift and by region of Brazil, before and during the COVID-19 pandemic. The highest average number of individuals receiving care per shift before the pandemic was 10.6 (SD = 5.9), in the North region, and the lowest, 7.9 (SD = 3.8) individuals in the South region. During the pandemic, the highest average number of individuals receiving care per shift was 4.5 (SD = 4.6), in the Northeast region, and the lowest average was 2.9 (SD = 1.9) in the Midwest region.
Table 2 Average number of dental visits per shift in Primary Health Care, before and during the COVID-19 pandemic, by region of Brazil, 2020 (n = 958)
| Regions of Brazil | Average number of dental visits per shift in PHCa | ||||
|---|---|---|---|---|---|
| Before the COVID-19 pandemic | During the COVID-19 pandemic | ||||
| Average (SDb) | p-valuec | Average (SDb) | p-valuec | ||
| North | 10.6 (5.9) | <0.001 | 3.9 (3.3) | <0.001 | |
| Northeast | 10.4 (5.9) | 4.5 (4.6) | |||
| Midwest | 9.8 (7.6) | 2.9 (1.9) | |||
| Southeast | 9.9 (6.5) | 3.6 (2.5) | |||
| South | 7.9 (3.8) | 3.2 (2.2) | |||
a) PHC: Primary Health Care; b) SD: Standard deviation; c) Analysis of variance (ANOVA).
Table 3 shows the results of the bivariate analysis of the association between exposure variables and the reduction in the number of dental visits after the beginning of the COVID-19 pandemic. It could be seen statistically significant difference in the region of Brazil (p = 0.040), availability of all types of mandatory PPE recommended by the new biosafety protocols after the emergence of COVID-19 (p = 0.035), availability of PPE in the routine prior to COVID-19 (p = 0.043) and adoption of new biosafety protocols by the PHCC (p = 0.027). The analysis of dental care in PHC, by region of Brazil, showed that 66.7% (95%CI 46.9;81.9) of the respondents in the North region, 59.3% (95%CI 51.9;66.3) in the Northeast, 82.3% (95%CI 69.3;90.6) in the Midwest, 64.2% (95%CI 56.9;70.6) in the Southeast and 64.8% (95%CI 60.5;69.0) in the South region reported a reduction of more than 50% in the number of visits after the emergence of the pandemic (Table 3).
Table 3 Distribution of variables of interest related to the reduction of dental care in Primary Health Care during the COVID-19 pandemic, Brazil, 2020
| Variables | Reduction of dental care in PHC during the COVID-19 pandemic >50.0% (%) | 95%CIb | p-valuec |
|---|---|---|---|
| Region of Brazil (n = 958) | |||
| North | 66.7 | 46.9;81.9 | 0.040 |
| Northeast | 59.3 | 51.9;66.3 | |
| Midwest | 82.3 | 69.3;90.6 | |
| Southeast | 64.2 | 56.9;70.6 | |
| South | 64.8 | 60.5;69.0 | |
| All types of PPEd recommended by the new protocols have been made availablee (n = 951) | |||
| No | 55.7 | 49.0;62.2 | 0.035 |
| Yes | 47.1 | 43.9;51.2 | |
| PPEd for clinical routine prior to the pandemic has been sufficientf (n = 830) | |||
| No | 55.2 | 48.4;61.8 | 0.043 |
| Yes | 47.1 | 43.9;51.1 | |
| Risk for SARS-Cov-2 infection in professionals (n = 958) | |||
| Yes | 66.7 | 61.3;67.6 | 0.736 |
| No | 64.5 | 53.8;77.4 | |
| The PHCC has tele-screening for COVID-19 (n = 958) | |||
| Yes | 64.9 | 57.2;69.9 | 0.761 |
| No | 63.8 | 61.3;69.9 | |
| The PHCC has adopted COVID-19 protocols (n = 880) | |||
| Yes | 67.0 | 63.2;70.7 | 0.027 |
| No | 59.3 | 53.4;65.0 | |
| The professional has already been diagnosed with COVID-19 (n = 925) | |||
| Yes | 63.8 | 49.1;76.3 | 0.891 |
| No | 64.8 | 61.6;67.9 | |
| The professional has already taken the COVID-19 test (n = 955) | |||
| Yes | 65.8 | 61.9;69.4 | 0.352 |
| No | 62.7 | 57.1;67.9 | |
a) PHC: Primary Health Care; b) 95%CI: 95% confidence interval; c) Pearson’ chi-square test; d) PPE: Personal protective equipment; e) PPE recommended by the new protocols: PFF2/N95 mask, disposable apron and face shield; f) PPE for the clinical routine prior to the pandemic: surgical mask, goggles and gloves.
Table 4 shows the prevalence ratios and their respective crude and adjusted confidence intervals, estimated using Poisson regression, of the association between the reduction in dental procedures in PHC during the COVID-19 pandemic and the study variables. In the adjusted regression analysis, the availability of all types of mandatory PPE recommended by new biosafety protocols (PR = 0.94; 95%CI 0.89;0.99) and the implementation of tele-screening service (RP = 0.90; 95%CI 0.85;0.96), could be seen as protective factors for the reduction above 50% in the number of dental visits during the pandemic. The adoption of biosafety protocols in dental care by the PHCC proved to be a risk factor for the reduction in the number of dental visits (above 50%) (PR = 1.04; 95%CI 1.01;1.07), although the strength of this association was weak.
Table 4 Crude and adjusted analysis of the association between reduction in dental procedures in Primary Health Care during the COVID-19 pandemic and variables of interest, Brazil, 2020
| Variables | Crude analysis | p-value | Adjusted analysisa | p-value | ||
|---|---|---|---|---|---|---|
| PRb | 95%CIc | PRb | 95%CIc | |||
| Region of Brazil (n = 928) | ||||||
| Northeast | 1.00 | 0.670 | 1.00 | 0.670 | ||
| North | 1.06 | 0.93;1.20 | 1.06 | 0.93;1.20 | ||
| Midwest | 1.06 | 0.96;1.18 | 1.06 | 0.96;1.18 | ||
| Southeast | 1.02 | 0.95;1.09 | 1.02 | 0.95;1.09 | ||
| South | 1.01 | 0.95;1.07 | 1.01 | 0.95;1.07 | ||
| All types of PPEd recommended by the new protocols have been made availablee (n = 951) | ||||||
| No | 1.00 | 0.020 | 1.00 | 0.042 | ||
| Yes | 0.94 | 0.90;0.99 | 0.94 | 0.89;0.99 | ||
| PPEd for clinical routine prior to the pandemic has been sufficientf (n = 830) | ||||||
| No | 1.00 | 0.026 | 1.00 | 0.050 | ||
| Yes | 0.94 | 0.89;0.90 | 0.95 | 0.90;1.00 | ||
| Risk for SARS-Cov-2 infection in professionals (n = 958) | ||||||
| No | 1.00 | 1.00 | 0.995 | 1.00 | 0.383 | |
| Yes | 1.00 | 0.91;1.09 | 0.94 | 0.84;1.06 | ||
| PHCCg has tele-screening for COVID-19 (n = 958) | ||||||
| No | 1.00 | 0.012 | 1.00 | <0.001 | ||
| Yes | 0.94 | 0.90;0.98 | 0.90 | 0.85;0.96 | ||
| PHCCg has adopted protocols (n = 907) | ||||||
| No | 1.00 | 0.007 | 1.00 | <0.001 | ||
| Yes | 1.03 | 1.01;1.05 | 1.04 | 1.01;1.07 | ||
| The professional has already been diagnosed with COVID-19 (n = 925) | ||||||
| No | 1.00 | 0.363 | 1.00 | 0.435 | ||
| Yes | 0.95 | 0.86;1.05 | 0.95 | 0.85;1.06 | ||
| The professional has already taken the COVID-19 test (n = 955) | ||||||
| No | 1.00 | 0.575 | 1.00 | 0.604 | ||
| Yes | 1.01 | 0.96;1.05 | 0.98 | 0.93;1.03 | ||
a) Analysis adjusted using stepwise backward method, keeping in the model all variables with p-value less than or equal to 0.2. The choice of variables included was based on the hierarchical analysis model described in Figure 1A; b) PR: Prevalence ratio; c) 95%CI: 95% confidence interval; d) PPE: Personal protective equipment; e) PPE available: PFF2/N95 mask, disposable apron and face shield; f) Previous PPE: Surgical mask, goggles and gloves; g) PHCC: Primary Healthcare Center.
Figure 1B shows the percentage of dentists who reported availability of PPE recommended by new biosafety protocols at PHCCs, in addition to the percentage of dentists who reported a sufficient amount of PPE used in the routine dental care at the PHCC before the COVID-19 pandemic. It can be seen that all types of PPE used in routine dental care before the pandemic were considered sufficient by most dentists, although 200 (22.9%) of these professionals reported insufficient availability of surgical masks after the emergence of the pandemic. Regarding the PPE recommended by the new biosafety protocols for clinical dental care, most dentists reported that the PPE was made available, but 77 (8.0%) affirmed that face shields were not made available.
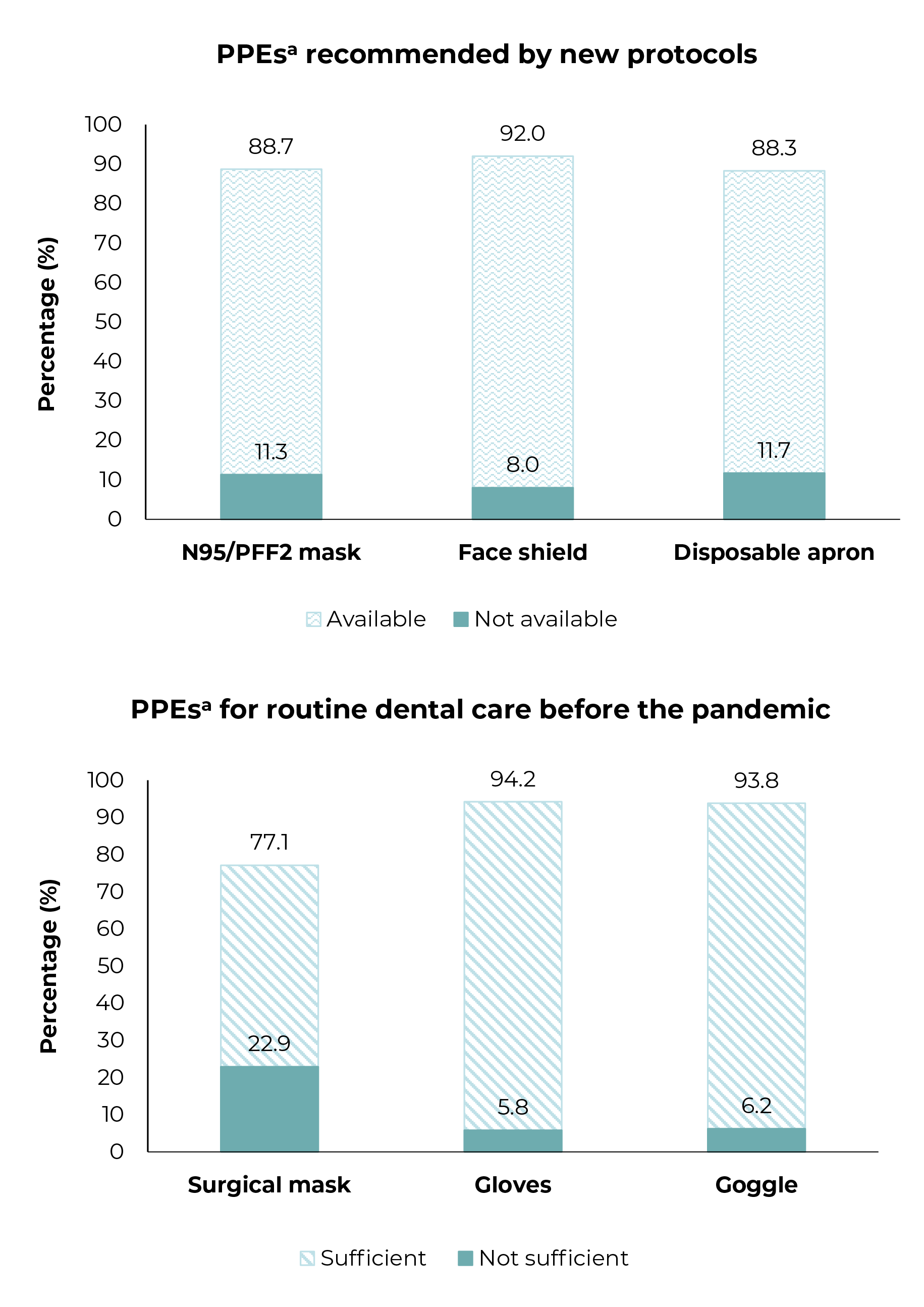
a) PPE: Personal protective equipment; b) CFO: Conselho Federal de Odontologia (Federal Board of Dentistry).
Figure 1B Percentage of availability of personal protective equipment (PPE) recommended by the new protocols and percentage of sufficiency of PPE used in dental routine in Primary Health Care, before the COVID-19 pandemic, Brazil, 2020
Discussion
This is possibly the first study to evaluate the reduction in the number of dental visits in PHC during the COVID-19 pandemic. The results of the study demonstrated that i) the availability of the recommended PPE according to the new biosafety protocols, for dentists working in PHC, and ii) the implementation of the tele-screening service at PHCCs, carried out by Health Departments, may have contributed to minimize the reduction of dental care after the beginning of the pandemic.
The largest epidemiological study on the evolution of the prevalence of COVID-19 in Brazil (EPICOVID-19), showed that there were several epidemics occurring at the same time in Brazil: if some regions presented a high number of cases, in other regions the cases would increase to a lesser extent and at different times.14 However, in this study, no association was identified between the reduction of dental care in PHC and the regions of Brazil, where the dentists worked. These differences can be explained by the fact that most participants are from the South region, and by the period when data collection occurred, between July and August 2020, when this region reported a lower number of COVID-19 cases, compared to the number of cases in the other regions of the country.15 A study conducted with dentists working in public and private sectors in Brazil in May 2020 found a greater reduction in dental activities in the hardest hit regions by the pandemic.6
The reduction of dental care (above 50%) in PHC, after the beginning of the pandemic, was associated with the unavailability of all new types of PPE and the insufficient amount of PPE in the routine dental care at PHCCs, reported by the dentists. It is worth highlighting that, if the number of dental visits had not been reduced, the scarcity of PPE would have represented an even more serious problem. Before the COVID-19 pandemic, developing countries had already been facing difficulties of access, unavailability and scarcity of personal protective equipment, leading to a low adherence to biosafety guidelines.16 However, in Brazil, it is worth emphasizing the importance of implementing policies capable of promoting the manufacturing of strategic essential inputs, such as PPE, especially in the most significant health emergencies, such as a pandemic.
The COVID-19 pandemic caused an increase in global demand for PPE and, consequently, an increase in prices, scarcity and inadequate use of these items.17-21 In addition, the supply of PPE, such as N95/PFF2 respirators and surgical masks, was prioritized for professionals responsible for providing health care to those with COVID-19.22 This problem has required national and international health authorities to publish guidance on the use, reuse and prolonged use of N95/PFF2 respirators.23,24 Prolonged use of PPE seems to be an effective and low-cost strategy to overcome the global shortage of respirators.25 This scenario of difficulty in the purchase and supply of PPE may have been one of the reasons for the reduction in the number of dental visits observed in this study.
The availability of all new types of PPE showed a protective effect in relation to the outcome studied. According to Simms et al. (2020),21 professionals' perception of the inadequate use of protective equipment was significantly associated with symptoms of mental disorder, probable posttraumatic stress disorders, worse overall health and greater reporting of emotional problems. These problems can generate negative impacts on performing work safely. A review of the guidelines for prevention and control of respiratory infections revealed that the lack of PPE represented a serious problem for professionals and managers, and it was necessary to adjust the volume of supplies as infection outbreaks continued.26 Probably, the availability of new types of PPE has contributed to a greater confidence and safety of PHC dentists in the continuity of dental care, in order to explain the protective effect on the reduction of dental care at PHCCs observed in this study.
The adoption of biosafety protocols by PHCCs was associated with a reduction in daily dental care, above 50.0%, in relation to the number of dental procedures performed before the pandemic. International and national protocols recommend measures aimed at reducing user demand for these health services,4,5,27 such as the prevention of droplet or aerosol-generating procedures, especially routine dental care procedures such as tartarectomy, endodontic access and cavity cleaning. In addition, dentists were recommended to try to perform the treatment in as few visits as possible, also limiting the number of professionals during the procedures, which may have led to a decrease in dental procedures that needed to be performed using four-handed technique.28,29 At the beginning of the pandemic, in March 2020, the Ministry of Health recommended that dentists from all over Brazil postponed elective treatments, limiting practice to urgent and emergency care, another fact that may have influenced the reduction in the number of visits found in this study, although data collection was performed between the fifth and sixth months after the beginning of the pandemic.4,28
Based on the experience gained from the previous outbreak of SARS-CoV and the available data on this virus and its associated disease, COVID-19, some specific measures have been suggested for the treatment of dental patients during this epidemic period.23,24,27 Before the individual is given an appointment, protocols recommend that a tele-screening should be done via the internet or telephone, including questions about medical history and the presence of flu-like symptoms such as fever, dry cough, sore throat, breathing difficulties, headache or muscle pain.4,10 If any of these symptoms are identified, the individual with suspected COVID-19 should be instructed to stay home, in isolation, and contact the health service as soon as possible, as recommended by the Centers for Disease Control and Prevention (CDC/USA).10 The tele-screening service, which represented a contributing factor for the reduction of dental care, ensures that it is possible to maintain the number of dental visits at the same level as that one in the period prior to the pandemic. The tele-screening allows us to identify clearly the nature of dental care: emergency or routine care.
The main limitation of this study was the impossibility of obtaining a representative sample of Brazilian dentists working in PHC in Brazil, evidenced by the high proportion - about 50% - of participants working in the South region. However, it is worth mentioning that efforts were made by the researchers to contact the entire population of interest, having sent e-mails to all PHC dentists and disseminated the project to municipal managers, universities and dentistry groups on social media. Nevertheless, many dentists may not have answered the survey due to lack of internet access in the most remote areas, or because they were not aware that the research was ongoing.
Despite the limitations, this study collected data via an online questionnaire, at a time when there was no possibility of conducting face-to-face surveys. Thus, it was possible to provide information on the effects of COVID-19 on dental care in PHC during the first wave of the pandemic in Brazil, and identify the difficulties encountered by dentists and the actions implemented by managers of Health Departments in the country in the face of insecurity about the modes of transmission of the disease, lack of personal protective equipment - PPE - and the need to maintain oral health care services for the population.
The results presented suggest that the COVID-19 pandemic caused a reduction of more than 50% in dental procedures performed by most dentists working in PHC in Brazil. Due to this problem, it is possible that there may be pent-up demand of users with different oral health needs and the change in the profile of those who seek the service due to the delay or non-performance of dental procedures. It is worth highlighting that the guidelines and recommendations disseminated by health authorities, after the emergence of COVID-19, guided the necessary adaptations in health services and thus enabled the maintenance of dental care, even with restrictions, contributing to the reduction of the impact of COVID-19 pandemic on oral health indicators of the Brazilian population.
Referências
1. World Health Organization. Coronavirus disease (COVID-19) dashboard [Internet]. Geneva: World Health Organization, 2020 [cited 2021 mar 26]. Available from: https://covid19.who.int/ [ Links ]
2. Johns Hopkins University. COVID-19: dashboard by the Center for Systems Science and Engineering at Johns Hopkins University (JHU) [Internet]. [Baltimore]: Johns Hopkins University; 2021 [cited 2021 mar 26]. Available from: https://coronavirus.jhu.edu/map.html [ Links ]
3. Van Doremalen N, Bushmaker T, Morris DH, Holbrook MG, Gamble A, Williamson BN, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med 2020;382(16):1564-7. doi: 10.1056/NEJMc2004973 [ Links ]
4. American Dental Association. ADA recommending dentists postpone elective procedures [Internet]. Illinois: American Dental Association; 2020 [update 2020 mar 16; cited 2021 apr 11]. Avaliable from: https://www.ada.org/publications/ada-news/2020/march/ada-recommending-dentists-postpone-elective-procedures [ Links ]
5. Conselho Federal de Odontologia. Manual de boas práticas em biossegurança para ambientes odontológicos [Internet]. Brasília: Conselho Federal de Odontologia; 2020 [citado 2021 jan 12]. Disponível em: http://website.cfo.org.br/covid19-manual-de-boas-praticas-em-biosseguranca-para-ambientes-odontologicos-e-lancado-com-apoio-institucional-do-cfo/ [ Links ]
6. Moraes RR, Correa MB, Queiroz AB, Daneris Â, Lopes JP, Pereira-Cenci T, et al. COVID-19 challenges to dentistry in the new pandemic epicenter: Brazil. PLoS One. 2020;15(11):e0242251. doi: 10.1371/journal.pone.0242251 [ Links ]
7. Chisini LA, Costa FS, Demarco GT, Silveira ER, Demarco FF. COVID-19 pandemic impact on paediatric dentistry treatments in the Brazilian Public Health System. Int J Paediatr Dent. 2021;31(1):31-4. doi: 10.1111/ipd.12741 [ Links ]
8. Chisini LA, Sartori LRM, Costa FDS, Salvi LC, Demarco FF. COVID-19 pandemic impact on prosthetic treatments in the Brazilian Public Health System. Oral Dis. 2020;00:1-3. doi: 10.1111/odi.13668 [ Links ]
9. Cunha AR, Antunes JLF, Martins MD, Petti S, Hugo FN. The impact of the COVID-19 pandemic on oral biopsies in the Brazilian National Health System. Oral Dis. 2020;00:1-4. doi: 10.1111/odi.13620. [ Links ]
10. Centers of Disease Control and Prevention. Interim infection prevention and control guidance for dental settings during the COVID-19 [Internet]. [Atlanta]: Centers of Disease Control and Prevention; 2020 [update 2020 dec 14; cited 2021 jan 12]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/hcp/dental-settings.html [ Links ]
11. Mhango M, Dzobo M, Chitungo I, Dzinamarira T. COVID-19 risk factors among health workers: a rapid review. Saf Health Work. 2020;11(3):262-5. doi: 10.1016/j.shaw.2020.06.001 [ Links ]
12. Eysenbach G. Improving the quality of web surveys: the Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J Med Internet Res 2004;6(3)e34. doi: 10.2196/jmir.6.3.e34 [ Links ]
13. Conselho Federal de Odontologia. Quantidade geral de profissionais e entidades ativas [Internet]. Brasília: Conselho Federal de Odontologia; 2021 [update 2021 jun 24; citado 2021 nov 16]. Disponível em: https://website.cfo.org.br/estatisticas/quantidade-geral-de-entidades-e-profissionais-ativos/ [ Links ]
14. Hallal PC, Hartwig FP, Horta BL, Silveira MF, Struchiner CJ, Vidaletti LP, et al. SARS-CoV-2 antibody prevalence in Brazil: results from two successive nationwide serological household surveys. Lancet Glob Health. 2020;8(11):1390-8. doi: 10.1016/S2214-109X(20)30387-9 [ Links ]
15. Ministério da Saúde (BR). Painel Coronavírus [Internet]. Brasília: Ministério da Saúde; 2021 [citado 2021 mar 2]. Disponível em: https://covid.saude.gov.br [ Links ]
16. Oosthuysen J, Potgieter E, Fossey A. Compliance with infection prevention and control in oral health-care facilities: a global perspective. Int Dent J. 2014;64(6):297-311. doi: 10.1111/idj.12134 [ Links ]
17. Cadnum JL, Li DF, Redmond SN, John AR, Pearlmutter B, Donskey CJ. Effectiveness of ultraviolet-c light and a high-level disinfection cabinet for decontamination of N95 respirators. Pathog Immun. 2020;5(1):52-67. doi: 10.20411/pai.v5i1.372 [ Links ]
18. Cheng VCC, Wong SC, Kwan GSW, Hui WT, Yuen KY. Disinfection of N95 respirators by ionized hydrogen peroxide during pandemic coronavirus disease 2019 (COVID-19) due to SARS-CoV-2. J Hosp Infect. 2020;105(2):358-9. doi: 10.1016/j.jhin.2020.04.003 [ Links ]
19. Li DF, Cadnum JL, Redmond SN, Jones LD, Pearlmutter B, Haq MF, et al. Steam treatment for rapid decontamination of N95 respirators and medical face masks. Am J Infect Control. 2020;48(7):855-7. doi: 10.1016/j.ajic.2020.05.009 [ Links ]
20. Vedovato TG, Andrade CB, Santos DL, Bitencourt SM, Almeida LP, Sampaio JFS. Trabalhadores(as) da saúde e a COVID-19: condições de trabalho à deriva?. Rev Bras Saúde Ocup. 2021;46:e1. doi: 10.1590/2317-6369000028520 [ Links ]
21. Simms A, Fear NT, Greenberg N. The impact of having inadequate safety equipment on mental health. Occup Med. 2020;70(4):278-81. doi: 10.1093/occmed/kqaa101 [ Links ]
22. World Health Organization. Mask use in the context of COVID-19: interim guidance [Internet]. Geneva: World Health Organization; 2020 [update 2020 dec 1; cited 2021 mar 08]. Available from: https://apps.who.int/iris/handle/10665/337199 [ Links ]
23. Agência Nacional de Vigilância Sanitária. Nota Técnica GVIMS/GGTES/ ANVISA No 04/2020 - Orientações para serviços de saúde: medidas de prevenção e controle que devem ser adotadas durante a assistência aos casos suspeitos ou confirmados de infecção pelo novo coronavírus (SARS-CoV-2) [Internet]. Brasília: Agência Nacional de Vigilância Sanitária; 2020 [update 2020 out 29; citado 2021 mar 12]. Disponível em: https://www.gov.br/anvisa/pt-br/centraisdeconteudo/publicacoes/servicosdesaude/notas-tecnicas/nota-tecnica-n-04-2020-gvims-ggtes-anvisa-atualizada.pdf/view [ Links ]
24. Centers of Disease Control and Prevention. Recommended guidance for extended use and limited reuse of N95 filtering facepiece respirators in healthcare settings [Internet]. [Atlanta]: Centers of Disease Control and Prevention; 2020 [cited 2021 mar 12]. Available from: https://www.cdc.gov/niosh/topics/hcwcontrols/recommendedguidanceextuse.html [ Links ]
25. Sarkis-Onofre R, Borges RDC, Demarco G, Dotto L, Schwendicke F, Demarco FF. Decontamination of N95 respirators against SARS-CoV-2: a scoping review. J Dent. 2021;104:103534. doi: 10.1016/j.jdent.2020.103534 [ Links ]
26. Houghton C, Meskell P, Delaney H, Smalle M, Glenton C, Booth A, et al. Barriers and facilitators to healthcare workers' adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: a rapid qualitative evidence synthesis. Cochrane Database Syst Rev. 2020;4(4):CD013582. doi: 10.1002/14651858.CD013582 [ Links ]
27. Conselho Federal de Odontologia. Recomendações AMIB/CFO para enfrentamento da COVID-19 na Odontologia [Internet]. 3. ed. [Brasília]: Conselho Federal de Odontologia; 2020 [citado 2021 abr 11]. Disponível em: https://website.cfo.org.br/wp-content/uploads/2020/07/Recomendac%cc%a7o%cc%83es-AMIB-CFO-Covid-19-atualizada-.pdf [ Links ]
28. Dadlani S. SARS-CoV-2 transmission in a dental practice in Spain: after the outbreak. Int J Dent. 2020; 2020:8828616. doi: 10.1155/2020/8828616 [ Links ]
29. Ather A, Patel B, Ruparel NB, Diogenes A, Hargreaves KM. Coronavirus disease 19 (COVID-19): implications for clinical dental care. J Endod. 2020;46(5):584-95. doi: 10.1016/j.joen.2020.03.008 [ Links ]
Received: July 30, 2021; Accepted: December 15, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
