










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
Print version ISSN 1679-4974On-line version ISSN 2337-9622
Epidemiol. Serv. Saúde vol.25 no.3 Brasília July/Sept. 2016
http://dx.doi.org/10.5123/S1679-49742016000300004
ORIGINAL ARTICLE
Aids mortality trends according to sociodemographic characteristics in Rio Grande do Sul State and Porto Alegre City, Brazil: 2000-2011*
1Fundação Oswaldo Cruz, Escola Nacional de Saúde Pública Sérgio Arouca, Rio de Janeiro-RJ, Brasil
OBJECTIVE:
to analyze AIDS mortality trends in Rio Grande do Sul State (RS) and Porto Alegre City (POA) according to sociodemographic characteristics in the period 2000-2011.
METHODS:
this was an ecological time series study of AIDS mortality rates; Prais-Winsten regression model was used.
RESULTS:
the standardized mortality AIDS rate showed a stationary trend in RS (1.3%; 95%CI: -0..;6.7) and in POA (-0.3%; 95%CI: -5.1;3.9); there was an increasing trend in the following categories: women in RS (4.1%; 95%CI: 3.0; 5.3) and in POA (2.7%; 95%CI: 1.8; 3.5), people with brown skin color in RS (4.5%; 95%CI: 1.9; 7.2) and in POA (4.6%; 95%CI: 1.5; 7.9), the 40-49 age group in RS (4.0%; 95%CI: 1.3; 6.7), the 50-59 age group in RS (5.8%; 95%CI: 1.9; 9.9) and in POA (6.0%; 95%CI: 2.1; 9.9), and the >60 age group in RS (4.0%; 95%CI: 1.1; 6.9).
CONCLUSION:
AIDS mortality increased among women, individuals with brown skin color and older age groups in RS and POA.
Key words: Mortality; AIDS; Epidemiological Surveillance; Sociodemographic Factors; Time Series Studies
Introduction
It is estimated that, in 2014, 36.9 million people throughout the world were infected with the human immunodeficiency virus (HIV), an infectious agent that causes the acquired immunodeficiency syndrome (AIDS). This result is quite influenced by the large number of antiretroviral therapy (ART) users, which contributes to increasing survival of individuals with HIV/AIDS. Nevertheless, it is important to highlight that this epidemic is still high in some regions, resulting in substantial health expenditures in health. 80% of the individuals living with HIV are concentrated in only 20 countries, and Brazil is one of them. The global incidence of AIDS, showed a 35% reduction between 2000 and 2014; notwithstanding, Brazil has registered an increase in new cases in this period.1
Since the beginning of HIV/AIDS epidemic in the country, there were 238,306 deaths due to this disease. When comparing AIDS mortality rates in Brazil between 2004 and 2013, we can observe a 6.6% reduction in mortality risk: in 2004, the mortality coefficient was of 6.1 deaths/100 thousand inhabitants, and in 2013, 5.7/100 thousand inhabitants.2
It is important to emphasize that Brazil was a pioneer in free and universal distribution of antiretroviral therapy, through the Brazilian National Health System (SUS), in 1996.3 This treatment has contributed for mortality reduction, increase in survival, reduction in viral burden and prevention of mother-to-child transmission.4
In spite of the reduction in AIDS mortality rates in Brazil, some regions presented a high number of deaths due to this disease. Rio Grande do Sul State (RS) has presented, since 2001, the highest mortality rates from the disease, and its capital, Porto Alegre City (POA), shows a coefficient higher than its own state and four times higher than the country's coefficient.2
The objective of this study was to analyze AIDS mortality trends in Rio Grande do Sul State (RS) and Porto Alegre City (POA) according to sociodemographic characteristics between 2000 and 2011.
Methods
This was an ecological time series study of AIDS mortality rates, performed with data from the Ministry of Health's Mortality Information System (SIM). The units of analysis were Rio Grande do Sul State (RS) and its capital, Porto Alegre City (POA). All the AIDS deaths occurred in the state and its capital from 2000 to 2011 were included.
Rio Grande do Sul State (RS) is located in the Southern region of Brazil; it has 281,730.223 km2 and 497 municipalities. In 2010, RS had a population of 10,693,929 inhabitants and a population density of 39.8 inhabitants/km2.5 Concerning education level, 55% of the population of the state older than 15 years old had, at least, complete Elementary School, and their average per capita income was BRL 729.40. With regard to ethnicity/skin color, 86.5% of the RS population self-declared white.5
The capital of the state, Porto Alegre City (POA), presented an area of 496.682 km2, a population density of 2,837.52 inhabitants/km2 and a population of 1,409,351 inhabitants in 2010, corresponding, in that year, to 13.2% of RS population.6 In POA, 72.9% of the population older than 15 years old had, at least, complete Elementary School. The average per capita income in POA was BRL 1,722.37. Concerning ethnicity/skin color, 79.2% of the population self-declared white.6
To calculate the mortality rates per 100 thousand inhabitants, we considered all the deaths recorded with the codes from the International Statistical Classification of Diseases and Related Health Problems - 10th revision (ICD-10) related to AIDS: B20 to B24. We calculated crude mortality rates according to sex, age group and ethnicity/skin color. The calculation of the standardized mortality rates was performed by age, for all the years of the studied period, using the direct method and considering as a standard the 2010 Brazilian population.
The information on resident population used to calculate mortality rates according to sex and age group are the data estimated by the Brazilian Institute of Geography and Statistics (IBGE), available at the SUS IT Department website (Datasus). However, the population for mortality rates according to ethnicity/skin color was estimated through the geometric model for the years for which the IBGE did not provide the information on ethnicity/skin color, since that institution only published these data for the years 2000 and 2010. Thus, to estimate the population for the remaining years (2001 to 2009; and 2011), it was conducted the calculation of the population growth rate from two identified points: the years 2000 and 2010.7
By using this model, we assume that the growth rate is constant, and identified through the formulation below:7
Where:
r is the population growth rate;
P(t) is the final population to identify the growth rate, i.e., it corresponds to the population of the year 2010;
P(0) is the initial population to identify the growth rate, i.e., it corresponds to the year 2000; and
t is the time elapsed between the measurement of the initial and final population, i.e., 2010-2000, a ten-year period.
The data was analyzed according to the following sociodemographic variables: sex (male; female), age group (in years: 0-19; 20-29; 30-39; 40-49; 50-59; and >60); and ethnicity/skin color (white; black; brown; dark skinned [in this study, it refers to the sum of black plus brown]). The categories of ethnicity/skin color yellow and indigenous were excluded, due to the low number of deaths.
For the trend analysis, the general linear model by Prais-Winsten was used. The independent variables (X) were the years when the deaths occurred; the mortality rates were considered the dependent variables (Y). The Prais-Winsten model is recommended to correct the serial correlation in temporal series. To identify the existence of serial autocorrelation, Durbin-Watson test was applied. The test value is measured in a scale that varies from 0 to 4. Values approaching zero, indicate positive autocorrelation, whereas values close to 4, indicate negative autocorrelation. On the other hand, when the test value is close to 2, there is no serial autocorrelation.8
For applying the model, we used the method suggested by Antunes and Cardoso.8
At first, we conducted the log transformation of Y values, followed by the application of Prais-Winsten regressive model, so that the b1 values of crude and standardized mortality rates were estimated, such as mortality rates according to sex, age group and ethnicity/skin color. Subsequently, the b1 values for each of the rates were included into the following formulation, to identify the annual percent changes:

From the APC analysis, we can affirm that a trend is (i) increasing, when the APC is positive, (ii) decreasing, when the APC is negative, and (iii) stationary, when there is no significant difference between its value and zero.
The final stage of modeling consisted of calculating the confidence intervals (CI) of study measurements, by using the following formulation:

The values of b minimum and b maximum are obtained from the confidence interval (CI), derived from the statistical analysis program, and are applied to the formulation, being the value of b minimum the minimum point of the CI and the value of b maximum the maximum point of the CI.
In this study, the significance level considered was 5% and the data analysis and processing was conducted with the Statistical Package for the Social Sciences 20.0 program (SPSS).
The research project was submitted to the Ethics and Research Committee of the National School of Public Health Sérgio Arouca (ESNP)/Oswaldo Cruz Foundation (Fiocruz) and approved - Report No. 15/2012.
Results
In the period from 2000 to 2011, the Mortality Information System (SIM) registered 16,804 deaths due to AIDS in RS; 35.8% of these deaths occurred in POA, what corresponds to 5,765 deaths in this city.
In tables 1 and 2, we can observe that the crude and standardized AIDS mortality rates for RS had increasing trend, with a variation rate of 1.8% (95%CI 0.7;3.0) for crude rates and 1.3 for standardized rates (95%CI -0.6;6.7). With regard to POA, the crude and standardized AIDS mortality rates were higher than the RS rates for all the years of the time series and presented stationary trend, with a variation rate of 0.4% (95%CI -1.3; 2.1) and -0.3% (95%CI -5.1;3.9) for crude and standardized rates, respectively.
Table 1 - Crude and standardizeda AIDS mortality rates (per 100 thousand inhabitants) in Rio Grande do Sul State and Porto Alegre City, 2000-2011
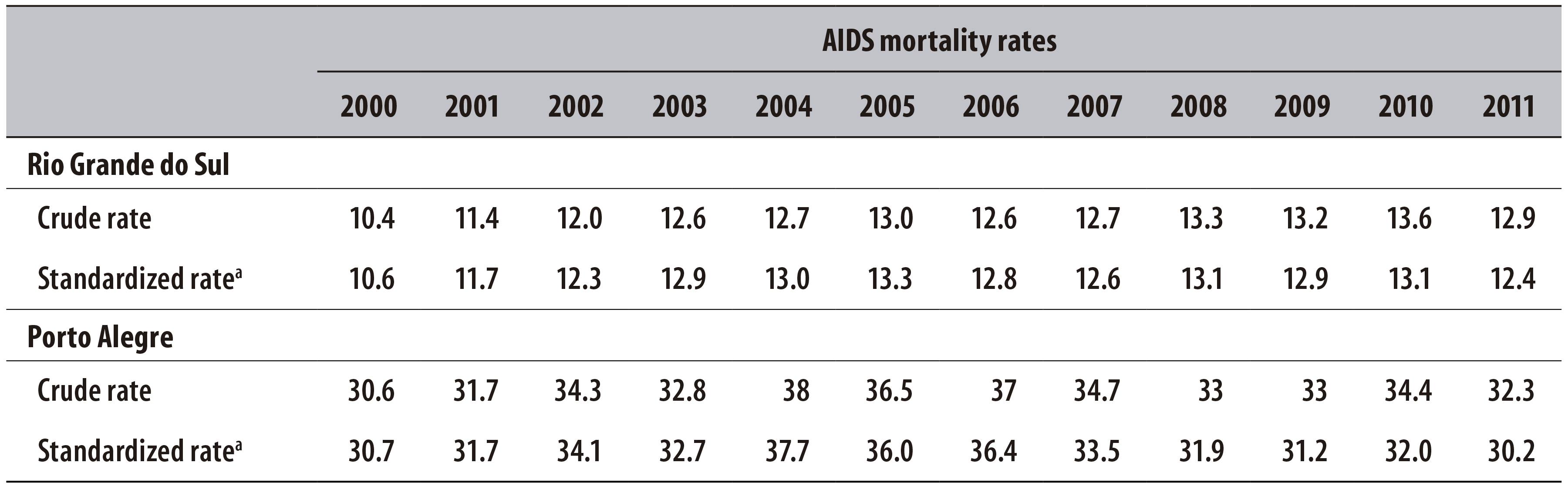
a) Rates standardized by age, through the direct method.
Table 2 - Variation and trends of AIDS mortality rates (per 100 thousand inhabitants) in Rio Grande do Sul State and Porto Alegre City, 2000-2011
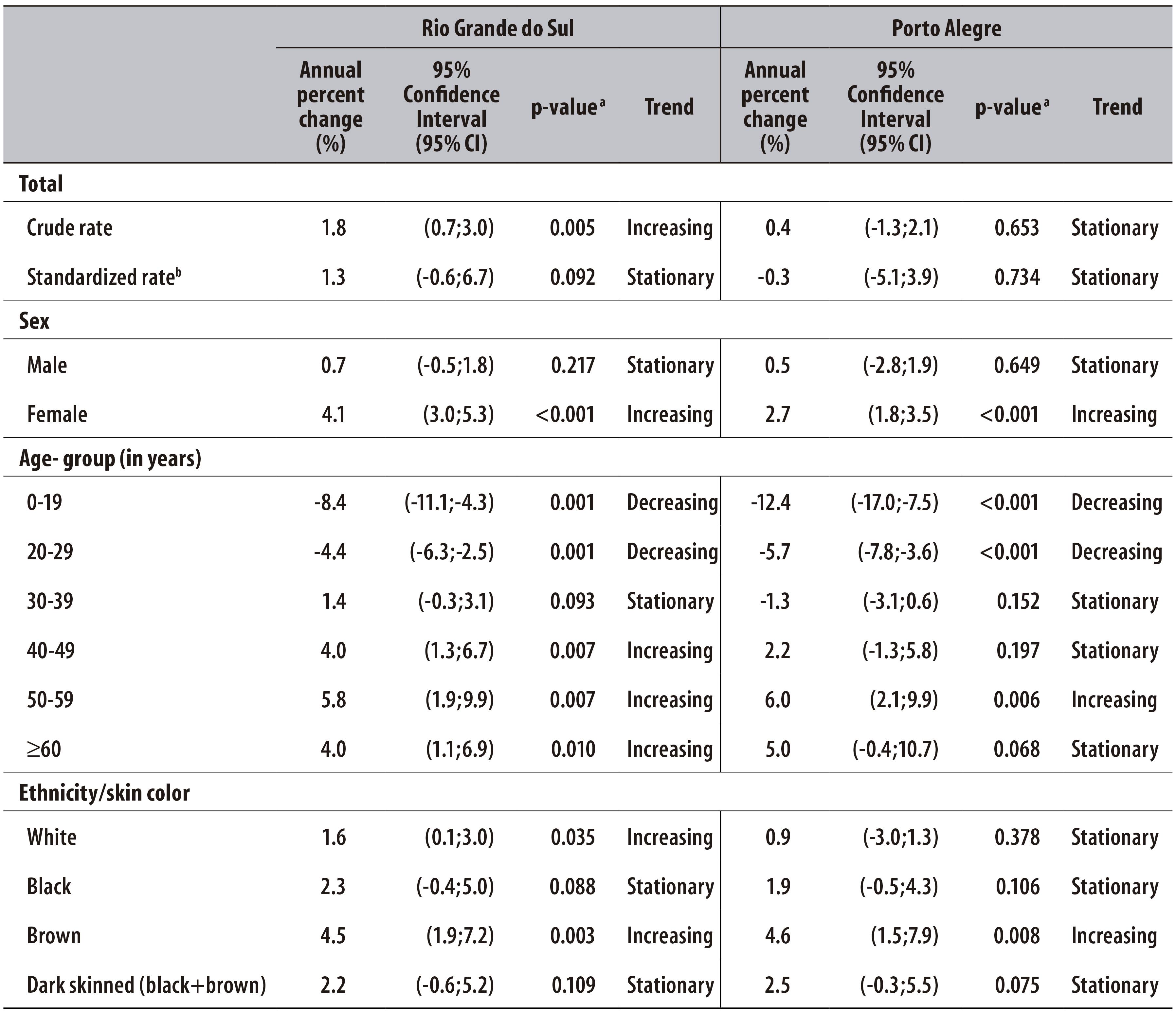
a) Prais-Winsten regression model
b) Rates standardized by age, through the direct method
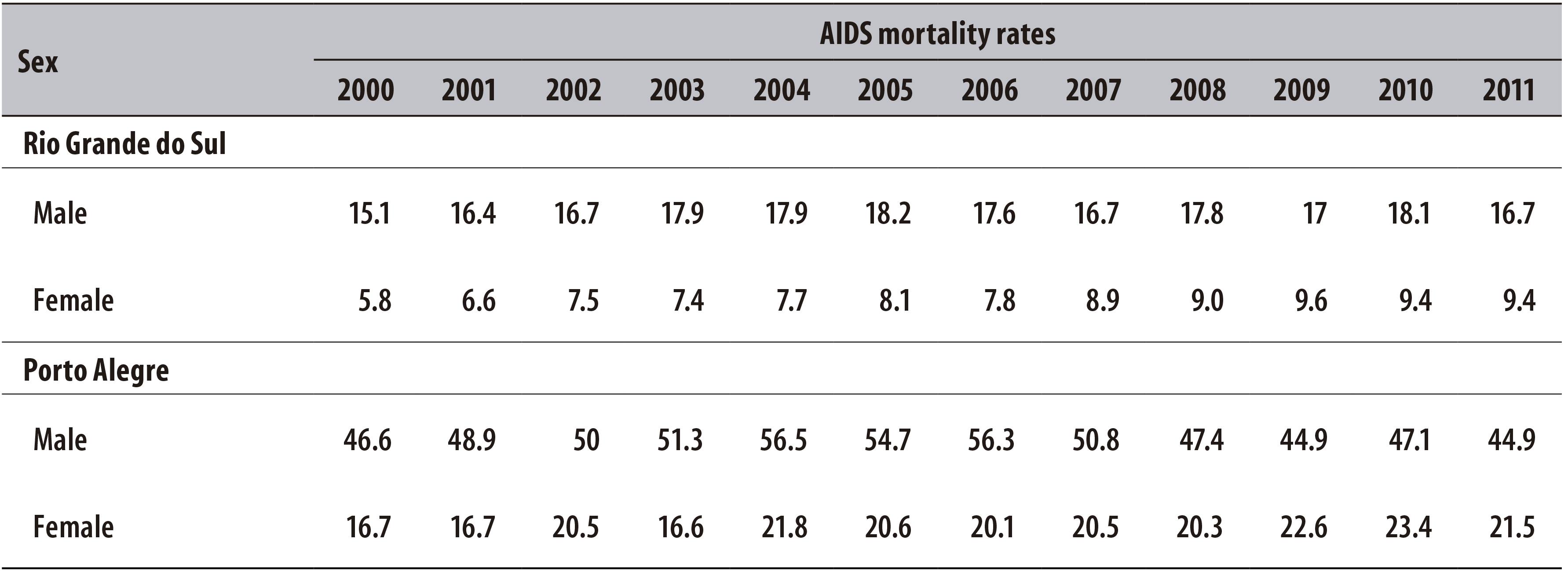
The time series of AIDS mortality in RS and in POA showed stationary trends among men, with a variation of 0.7% (95%CI -0.5;1.8) in the state and of 0.5% in the capital (95%CI -2.8;1.9). In the female population, there was a significant increase in AIDS mortality rates between 2000 and 2011, with increasing trend both in RS, and in POA, with a change of 4.1% in the state (95%CI 3.0;5.3) and of 2.7% in the capital (95%CI 1.8;3.5) (Tables 2 and 3).
Table 3 - AIDS mortality rates per 100 thousand inhabitants according to sex in Rio Grande do Sul State and Porto Alegre City, 2000-2011
With regard to age groups, we can observe a decreasing trend in RS for the following groups: 0-19, with a variation rate of -8.4% (95%CI -11.1;-4.3), and 20-29, with a variation of -4.4% (95%CI -6.3;-2.5). There was stationary trend in AIDS mortality rate for the group aged 30-39, with a variation rate of 1.4% (95%CI -0.3;3.1). However, an increasing trend was found in older age groups, for which the following variation rates were observed: 4.0% in the 40-49 group (95%CI 1.3;6.7), 5.8% in the 50-59 group (95%CI 1.9;9.9) and 4.0% in the >60 group (95%CI 1.1;6.9) (Tables 2 and 4).
Table 4 - AIDS mortality rates (per 100 thousand inhabitants) according to age group in Rio Grande do Sul State and Porto Alegre City, 2000-2011

In POA, the age groups 0-19 and 20-29 also presented a decreasing trend in AIDS mortality, with an APC of -12.4% (95%CI -17.0;-7.5) and -5.7% (95%CI -7.8;-3.6), respectively. There was stationary trend in of the following age groups: 30-39 (APC -1.3%; 95%CI -3.1;0.6), 40-49 (APC 2.2%; 95%CI -1.3; 5.8) and >60 (APC 5.0%; 95%CI -0.4;10.7). Only for the 50-59 age group, there was increasing trend, with an APC of 6.0% (95%CI 2.1;9.9) (Tables 2 and 4).
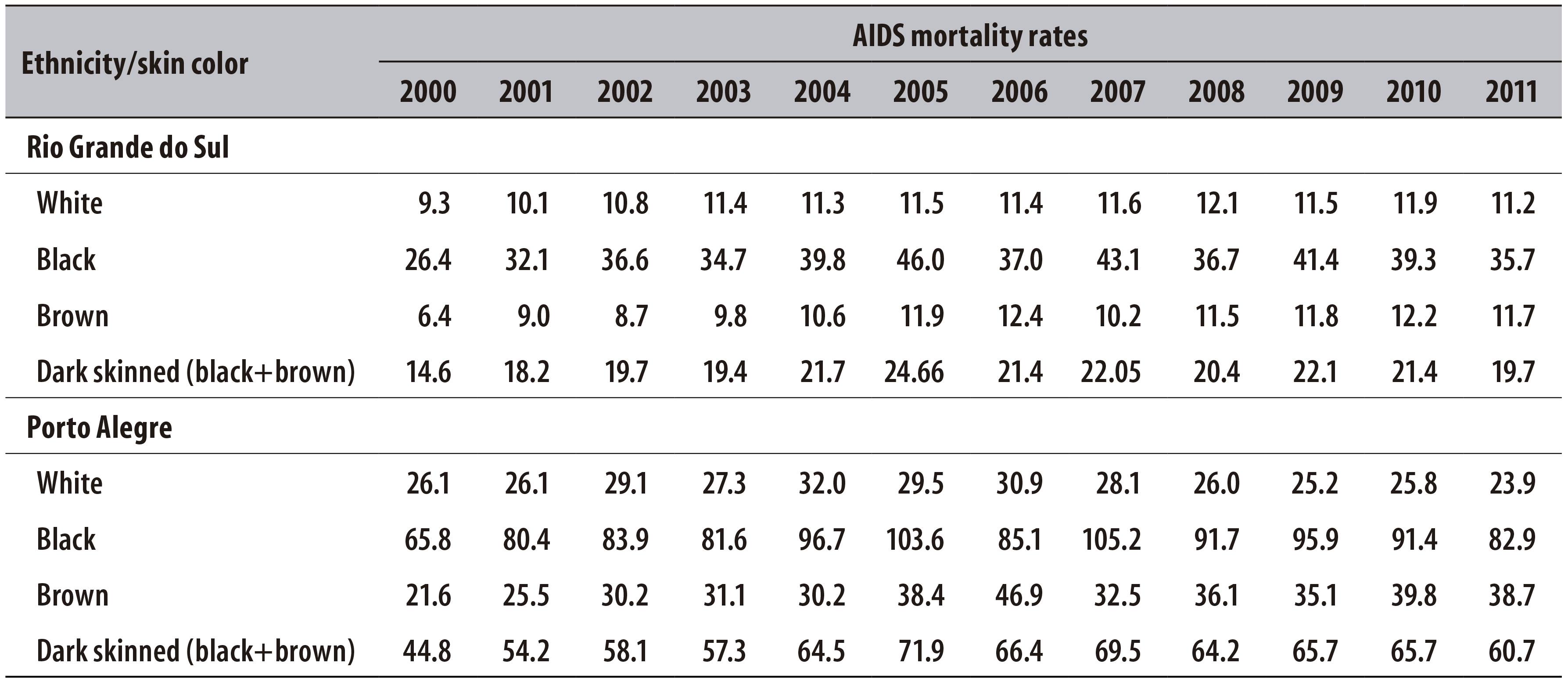
In RS, there was an increase of AIDS mortality in white and brown skinned population, with an APC of 1.6% (95%CI 0.1;3.0) and 4.5% (95%CI 1,9;7.2), respectively. The skin colors black and dark (black+brown) presented stationary trend, with an APC of 2.3% (95%CI -0.4;5.0) and 2.2% (95%CI -0.6;5.2), respectively. In POA, trends were stationary for white, black and dark (black+brown) skin colors. However, brown skin color presented increasing trend and APC of 4.6% (95%CI 1.5;7.9) (Tables 2 and 5).
Discussion
In the period from 2000 to 2011, AIDS mortality in RS and POA presented stationary trend. When considering that AIDS rates in POA were higher than the RS rates, this stationary trend reveals that AIDS mortality rates in the city remained high during a considerable time.
A research that assessed the death risk due to this disease, as well as its incidence from 1990 to 2002, pointed that, after the beginning of antiretroviral therapy in Brazil, there was a reduction in mortality rates.9 According to data of the HIV/AIDS Epidemiological Report, between 2004 and 2013, the mortality rates declined in Brazil.2 However, a study that investigated mortality due to HIV/AIDS in the period from 1999 to 2007 showed that the rates were stable in the country, but, when observing this indicator regionally, it was possible to identify disparities in AIDS mortality rates.10
It is important to emphasize that the high mortality rates in RS and POA can be associated to the uneven distribution of health care services. An investigation that assessed the magnitude and trend of HIV/AIDS epidemic from 2000 to 2006 showed that the inequality of access to health care services for HIV/AIDS response was high in the Brazilian South and Southeast urban centers, where the epidemic is under a more strict control, when compared to other medium sized regions which have increasing profile epidemic and reduced response capacity.11
In a scenario of universal and free availability, of a therapy that contributes to the mortality reduction and the increase in life expectancy of individuals infected with HIV/AIDS, since 1996, it is worrisome to observe that AIDS mortality rates still present high levels, and with increasing and stationary trend in RS and POA, respectively. According to Veras et al.,12 AIDS mortality in Brazil remains high, and there is inequality in the access to public health services. Furthermore, the late start of antiretroviral therapy influences the treatment success, because, when there is early diagnosis, the possibilities of a satisfactory treatment increase.
A study developed in the United Kingdom analyzed the effect of late diagnosis in the life expectancy of a population of men who have sex with men (MSM), diagnosed in 2010, identified that the life expectancy increased in places where there was wide access to health services and retroviral drugs and that the late diagnosis is the main factor for death in individuals infected with HIV/AIDS.4
The current guidelines of the Brazilian Ministry of Health to control HIV/AIDS are based on preventing the disease among individuals who have not been infected, as well as the diagnosis and early start of ART in individuals infected with HIV/AIDS.2
The present study showed that, among men from RS and POA, AIDS mortality rates were higher than among women. However, AIDS mortality trend among men was stationary in both RS and POA. Concerning female sex, both in RS and in POA, AIDS mortality trend was increasing. These results are similar to the national pattern of AIDS mortality increasing among women and stable among men.2
The increase of aids mortality among women is known as feminization of the epidemic, and has been observed since the 1990s.13
Some studies have been discussing the elements that contribute to women's vulnerability towards AIDS. Some authors suggest that this situation can be associated to socioeconomic and low risk perception issues.14 It is worth mentioning that a research that analyzed the differences between the sexes in practices associated to HIV infection in Brazil emphasized the difficulty to negotiate the use of condom with the male partner, reducing its use among women.15
With regard to age, in RS, 0-19 and 20-29 age groups showed reduction trend, whereas 30-39 age groups presented stationary trends, and the older groups - 40-49, 50-59 and >60 - presented increasing trend. In POA, the trends were decreasing for the 0-19 and 20-29 age groups. Stationary trends were observed in the 30-39, 40-49 and >60 age groups. Only the 50-59 age group presented increasing trend. The aforementioned profile is similar to the national pattern of mortality according to age,2,13 and also corresponds to the global profile, according to which AIDS is the fifth leading cause of death among adults.16 Nevertheless, it is important to highlight that, for 50-59 and>60 age groups, there was significant increase. The current AIDS situation in older individuals is a reality that was also observed in a research which assessed AIDS in Ceará in the period from 2001 to 2011.17 Furthermore, an investigation that analyzed the AIDS epidemic among eldery individuals in the Federal District, pointed that this disease growth among the population over the age of 60 was oscillating, with stability trend, over the years from 1999 to 2009, thereby attributing a new pattern to the epidemic.18
Regarding the reduction in AIDS mortality in the population included in the 0-19 age group, this can be a consequence of the implementation of HIV/AIDS prevention of mother-to-child transmission, which is characterized by the availability of HIV test during prenatal care, as well as the rapid test in childbirth and antiretroviral therapy for the newborn.19,20
With regard to skin color or ethnicity, this survey data showed that, in RS, there was increasing trend of AIDS mortality rate for both white and brown skin color, and stationary trend for black and dark (black+brown) skinned. In POA, AIDS mortality according to ethnicity/skin color had increasing trend in brown and dark (black+brown) skinned individuals, and stationary trend in white and black skinned individuals. It is important to highlight that AIDS mortality rates were higher in black and dark (black+brown) skinned individuals, both in RS and in POA. Another important point to be addressed about ethnicity/skin color, is related to the great difference between the numerator and denominator for calculating mortality rates according to ethnicity/skin color, which can be understood as a limitation in the calculation of mortality rate according to ethnicity/race color, because the numerator is composed by SIM data, and the register of ethnicity/skin color is established by the personnel who fill the Death Certificate (DO). The denominator is taken from projections related to census years, which may generate an overestimation or underestimation of rates, because, when considering that the population growth is constant, it can generate a non-identification of increase or decrease rates. This factor may influence on trends analysis - when the population is overestimated, the rates decrease, and when it is underestimated, the rates increase-, in other words, it can point to a mistaken trend.
It is important to highlight that the high AIDS mortality rate in the black, brown and dark skinned population in RS and POA can be related to the exclusion suffered by this population throughout the Brazilian history.21
For Barata,22 belonging to a population of certain ethnicity/skin color says a lot about having or not having access to public health services, and also impacts on health conditions. The black skinned population is characterized by being concentrate in places with lack of resources, featured by the lack of adequate sanitation, education and work, which contributes to the vulnerability of this group.
A limitation of this study is the use of secondary data from the Mortality Information System (SIM), because, in spite of the improvements occurred over the years in this system, there is a variation in its quality and coverage, depending on the region.23 The improvement on quality of SIM data can also be assigned to the reduction of register of death due to ill-defined causes, which results in the increase of specific mortality rates in regions that present a high register of death due to ill-defined causes, such as the North and Northeast regions.
A different pattern is identified in the Southeast and South regions, where there is a lower number of registers of death due to ill-defined causes.24 From this information, it is important to highlight that there is a possibility of underestimation of the rates in the beginning of this study period, which may lead to the conclusion that the increasing trends could be attributed, partially or totally, to the quality improvement and coverage of data on death.
Finally, it is important to emphasize that, according to this study, Porto Alegre City showed, during the entire analyzed period, higher mortality rates than the ones presented by its own state, pointing to the need of attention by the municipal health managers in order to strengthen practices of promotion, prevention and assistance to HIV/AIDS.
Furthermore, for a greater understanding of mortality in the units of analysis presented here, it is also essential to develop studies to investigate certain features, such as the population's living conditions and the access to HIV/AIDS testing and treatment. Indeed, it is not enough to understand only the profile of the individuals infected by the disease, although it contributes to health care management practices and strategies to change incidence indicators and mortality due to AIDS.
REFERENCES
1. Joint United Nations Programme on HIV/AIDS. How Aids changed everything: MDG 6: 15 years, 15 lessons of hope from the Aids response. Geneva: United Nations Programme on HIV/AIDS; 2015. [ Links ]
2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de DST, Aids e Hepatites Virais. Boletim epidemiológico: HIV/Aids. 2014;3(1):19-21. [ Links ]
3. Fazito E, Vasconcelos AMN, Pereira MG, Rezende DF. Trends in non-Aids-related causes of death among adults with HIV/Aids, Brazil, 1999 to 2010. Cad Saude Publica. 2013 Aug;29(8):1644-53. [ Links ]
4. Nakagawa F, Lodwick RK, Smith CJ, Smith R, Cambiano V, Lundgren JD, et al. Projected life expectancy of people with HIV according to timing of diagnosis. AIDS. 2012 Jan;26(3):335-43. [ Links ]
5. Instituto Brasileiro de Geografia e Estatística. Estados: Rio Grande do Sul [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; [2010] [citado 2013 jan 27]. Disponível em: Disponível em: http://www.ibge.gov.br/estadosat/perfil.php?sigla=rs . [ Links ]
6. Instituto Brasileiro de Geografia e Estatística. Estados: Porto Alegre [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2016 [citado 2013 jan 27]. Disponível em: Disponível em: http://cidades.ibge.gov.br/xtras/perfil.php?lang=&codmun=431490&search=rio-grande-do-sul|porto-alegre [ Links ]
7. Rede Interagencial de Informação para a Saúde. Indicadores básicos para a saúde no Brasil: conceitos e aplicações [Internet]. Brasília: Organização Pan-Americana da Saúde; 2008 [citado 2012 fev 5]. 349 p. Disponível em: Disponível em: http://tabnet.datasus.gov.br/tabdata/livroidb/2ed/indicadores.pdf [ Links ]
8. Antunes JLF, Cardoso MRA. Uso da análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saude. 2015 jul-set;24(3):565-76. [ Links ]
9. Dourado I, Veras MASM, Barreira D, de Brito AM. Tendências da epidemia de Aids no Brasil após a terapia anti-retroviral. Rev Saude Publica. 2006 abr;40 supl:9-17. [ Links ]
10. Teixeira TRA, Gracie R, Malta MS, Bastos FI. Social geography of Aids in Brazil: identifying patterns of regional inequalities. Cad Saude Publica. 2014 Feb;30(2):259-71. [ Links ]
11. Grangeiro A, Escuder MML, Castilho EA. A epidemia de Aids no Brasil e as desigualdades regionais e de oferta de serviço. Cad Saude Publica. 2010 dez;26(12):2355-67. [ Links ]
12. Veras MASM, Ribeiro MCA, Jamal LF, McFarland W, Bastos FI, Ribeiro KB, et al. The "AMA-Brazil" cooperative project: a nation-wide assessment of the clinical and epidemiological profile of Aids-related deaths in Brazil in the antiretroviral treatment era. Cad Saude Publica. 2011; 27 Suppl 1:s104-s13. [ Links ]
13. Reis AC, Santos EM, Cruz MM. A mortalidade por Aids no Brasil: um estudo exploratório de sua evolução temporal. Epidemiol Serv Saude. 2007 jul-set; 16(3):195-205. [ Links ]
14. Santos NJS, Barbosa RM, Pinho AA, Villela WV, Aidar T, Filipe EMV. Contextos de vulnerabilidade para o HIV entre mulheres brasileiras. Cad Saude Publica. 2009;25 supl 2:s321-s33. [ Links ]
15. Pascom ARP, Szwarcwald CL. Sex inequalities in HIV-related practices in the Brazilian population aged 15 to 64 years old, 2008. Cad Saude Publica. 2011;27Suppl 1:s27-s35. [ Links ]
16. Organização das Nações Unidas; Joint United Nations Programme on HIV/Aids. A ONU e a resposta à Aids no Brasil. Brasília: Organização das Nações Unidas; 2013. [ Links ]
17. Pedrosa NL, Paiva SS, Almeida RL, Holanda ER, Kerr LR, Galvão MT. The historic data series on Aids in the state of Ceará, Brazil. Cienc Saude Coletiva. 2015 Apr;20(4):1177-84. [ Links ]
18. Oliveira MLC, Paz LC, Melo GF. Dez anos de epidemia do HIV-Aids em maiores de 60 anos no Distrito Federal - Brasil. Rev Bras Epidemiol. 2013 mar;16(1):30-9. [ Links ]
19. Santos EM, Reis AC, Westman S, Alves RG. Avaliação do grau de implantação do programa de controle da transmissão vertical do HIV em maternidades do 'Projeto Nascer'. Epidemiol Serv Saude. 2010 jul-set;19(3):257-69. [ Links ]
20. Barreto ML, Teixeira MG, Bastos FI, Ximenes RAA, Barata RB, Rodrigues LC. Successes and failures in the control of infectious diseases in Brazil: social and environmental context, policies, interventions, and research needs. Lancet. 2011 May;377(9780):1877-89. [ Links ]
21. Joint United Nations Programme on HIV/Aids; World Health Organization. Aids epidemic update. Geneva: Jointed United Nations Programme on HIV/Aids; 2002. [ Links ]
22. Barata RB. Como e por que as desigualdades sociais fazem mal à saúde. Rio de Janeiro: Editora Fiocruz; 2009. [ Links ]
23. Szwarcwald CL, Morais Neto OL, Frias PG, Souza Júnior PRB, Escalante JJC, Lima RB, et al. Busca ativa de óbitos e nascimentos no Nordeste e na Amazônia Legal: estimação das coberturas do SIM e do SINASC nos municípios brasileiros. In: Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Saúde Brasil 2010: uma análise da situação de saúde e de evidências selecionadas de impacto de ações de vigilância em saúde. Brasília: Ministério da Saúde; 2011. p. 79-98. (Série G. Estatística e Informação em Saúde). [ Links ]
24. Cavalini LT, Ponce de Leon ACM. Correção de sub-registros de óbitos e proporção de internações por causas mal definidas. Rev Saude Publica. 2007 fev;41(1):85-93. [ Links ]
*This study was carried out with the support of the Scientific Initiation Program (PIBIC) of the National Council for Scientific and Technological Development (CNPq), of the Ministry of Science, Technology and Innovation (MCTI), at the National School of Public Health Sérgio Arouca (ENSP)/ Oswaldo Cruz Foundation (Fiocruz): Process No. 129212/2012-1.
Received: September 03, 2015; Accepted: March 28, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
