










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.25 n.4 Brasília oct./dic. 2016
http://dx.doi.org/10.5123/S1679-49742016000400002
Articles
Description of the first cases of Zika virus fever investigated in municipalities of the Brazilian Northeastern Region, 2015
1Ministério da Saúde, Secretaria de Vigilância em Saúde, Brasília-DF, Brasil
2Secretaria de Estado da Saúde Pública do Rio Grande do Norte, Secretaria de Vigilância em Saúde, Natal-RN, Brasil
3Secretaria de Estado da Saúde do Maranhão, Centro de Informações Estratégicas em Vigilância em Saúde, São Luís-MA, Brasil
4Secretaria Municipal de Saúde de Barra do Corda, Vigilância Epidemiológica, Barra do Corda-MA, Brasil
5Secretaria Municipal de Saúde de São Luís, Coordenação de Vigilância Epidemiológica da Dengue e Chikungunya, São Luís-MA, Brasil
6Secretaria de Estado da Saúde da Paraíba, Coordenação-Geral de Vigilância em Saúde, João Pessoa-PB, Brasil
7Secretaria Municipal de Saúde de João Pessoa, Coordenação de Vigilância Epidemiológica, João Pessoa-PB, Brasil
OBJECTIVE:
to confirm Zika virus circulation and discard other etiological agents in an outbreak occurred in the states of Rio Grande do Norte, Maranhão and Paraíba, in May, 2015.
METHODS:
this is a case series descriptive study with residents in Natal-RN, Barra do Corda-MA, São Luis-MA and João Pessoa-PB, with 20 cases in each state, presenting rash, absent or mild fever and one of the following signs/symptoms: conjunctival hyperemia, arthralgia or limb edema; RT-PCR/isolation tests for Zika, enterovirus and respiratory viruses, and serology tests (dengue, rubella and parvovirus B19) were performed.
RESULTS:
the main symptoms were rash (n=60), pruritus (n=54), and arthralgia (n=47); 51 individuals did not present fever; Zika virus was identified in 18 cases (12 in Paraíba, four in Maranhão and two in Rio Grande do Norte), and antibodies to dengue, in 14 cases.
CONCLUSION:
the symptoms were consistent with Zika virus fever; there was laboratory confirmation for Zika and dengue.
Keywords: Exanthema; Arboviruses; Zika Virus; Zika Virus Infection; Epidemiology, Descriptive
Introduction
In October 2014, some individuals resident in municipalities of Rio Grande do Norte State (RN) reported the occurrence of rash, in addition to pruritus, mild fever and joint pain, which did not fit the definitions of suspect cases for measles, rubella and dengue. Thus, the health services suspected of chikungunya, a disease recently introduced in Brazil, with autochthonous cases since 2014;1 however, serology tests for IgM detection of the disease were conducted, and the results were negative.
Rash is a lesion on the skin, composed by macules or papules, associated or not with pruritus, blisters and crusts, striking a specific region or the whole body.2-4 The rash may be related to a range of diseases and conditions, although the infectious causes (virus, bacteria, fungus and protozoans) are responsible for more than 70% of the cases,2 and may be present in many diseases, such as measles, rubella, parvovirus, dengue, chikungunya fever, and Zika virus fever.5,6-8
In February 2015, Paraíba State recorded cases of individuals who presented the same medical conditions observed in Rio Grande do Norte. In March of the same year, the Center for Strategic Information for Health Surveillance of Maranhão State (CIEVS/MA) began, in the municipality of Barra do Corda, Maranhão, an investigation of the cases of exanthematous syndromes of uncertain origin.
Besides Rio Grande do Norte, Maranhão and Paraíba, other six states of the Northeast region notified the occurrence of exanthematous syndrome to the national CIEVS, from October 2014 to March 2015. In April 2015, six months after the first records of this syndrome of unknown etiology in the Brazilian Northeast, it was necessary to clarify the possible etiological agents involved. On May 15, 2015, the Zika virus was confirmed by the Ministry of Health to be autochthonous in Brazil.9
In this context, the conduction of an investigation was proposed, with the objective of confirming Zika virus circulation and discarding other etiological agents in an outbreak occurred in the states of Rio Grande do Norte, Maranhão and Paraíba, in May, 2015.
Methods
A case series descriptive study was conducted, with active search for suspect cases of infection due to Zika virus in the municipalities of Natal-RN, Barra do Corda-MA, São Luís-MA, and João Pessoa-PB.
We selected 20 individuals from each state, assisted in the health services suggested by the State and Municipal Health Departments. The number of individuals was limited due to the capacity of the laboratories to process the samples collected during the investigation. The individuals were selected the moment they went to the health care facilities.
The following definition of suspect case of Zika virus was used: individuals resident in one of the municipalities of the study who, in the period from May 11 to 22, 2015 were assisted in the health facilities suggested by the Health Departments and presented, in the five days previous to the health care (recent infection) rash and absent or mild fever (up to 37.7ºC) with at least one of the following signals/symptoms:
- conjunctival hyperemia or arthralgia or limb edema; and
- did not fit into any of the case definitions from the Guide of Health Surveillance, of the Secretariat of Health Surveillance of the Ministry of Health (SVS/MS) for dengue, chikungunya fever, measles and rubella.7
Data collection was performed with a standard questionnaire, semi-structured, developed specially for that investigation, containing sociodemographic variables, date of initial symptoms, signs and symptoms, use of drugs, nonspecific and specific tests, allergies and vaccination history, contact with other person who presented similar symptoms, hospitalization, travels in the previous 15 days and comorbidities. The interviews were conducted by the SVS/MS's rapid response team, during the individuals' health care or by telephone.
Two blood samples were collected (serum and whole blood) from each individual, in order to perform (i) IgM serology for dengue, measles, rubella and parvovirus, with the objective of discarding these etiological agents, and (ii) reverse transcription polymerase chain reaction (RT-PCR) to detect Zika virus. The laboratory test used to diagnose the aforementioned viruses - through detection of specific IgM - was the Elisa - IgM.
The first sample was collected by the fifth day after the initial signs and symptoms. The second sample was collected 10 days after the first sample.
The programs Epi Info TM 7.1.5.0 and Microsoft Office Excel 2010 were used for data analysis.
Before the interview, the informed consent was read and the participants orally accepted it. The researchers ensured the individuals' anonymity and confidentiality, in accordance to the resolution of the National Health Council (CNS) No. 466, dated December 12, 2012. The data analyzed was obtained in the context of the action on epidemiological surveillance, which exempts from the appreciation by an Ethics Research Committee.
Results
From the 60 individuals included in the study, 20 were from Natal-RN, 20 from João Pessoa-PB, four were from Barra do Corda-MA and 16 were from São Luís-MA. Among the selected individuals, most of them were adults. The most frequent age group was 20-39 years old in Natal-RN and 40-59 in Maranhão (Barra do Corda-MA and São Luís-MA) and João Pessoa-PB (Table 1).
Table 1 - Distribution of exanthematous syndrome cases, according to age group, in the municipalities of Natal-RNa, Barra do Corda-MAb, São Luís-MAb, and João Pessoa-PBc, May, 2015
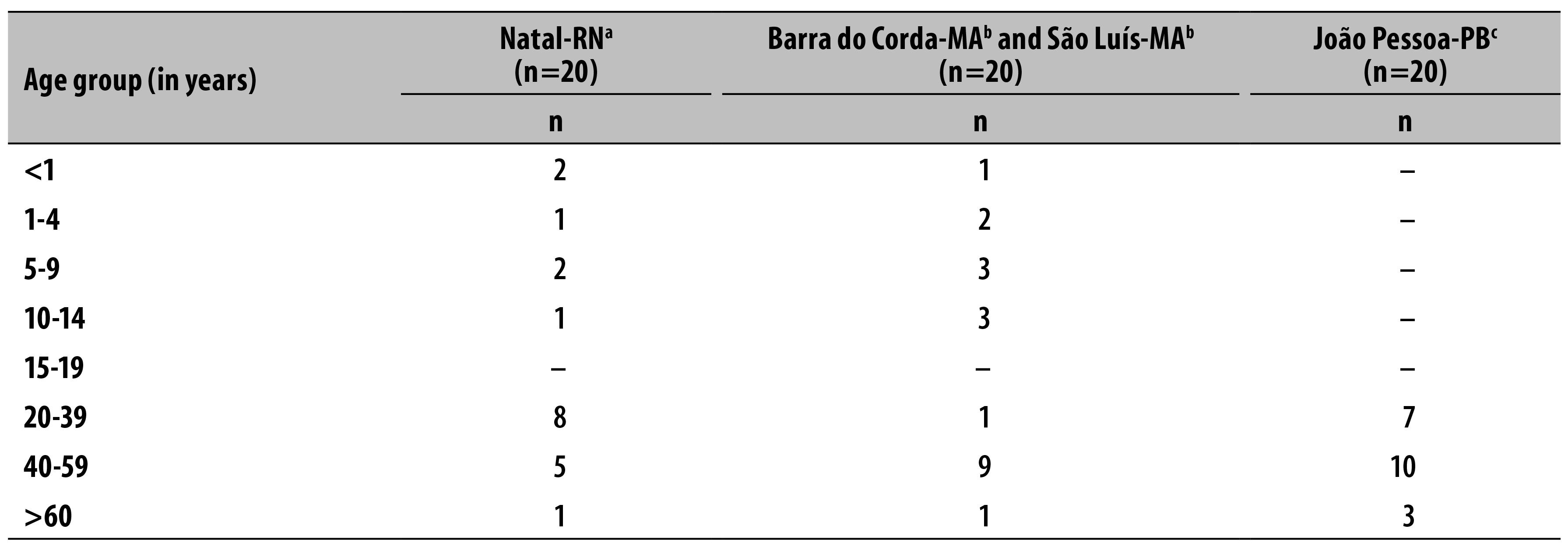
a) Rio Grande do Norte State
b) Maranhão State
c) Paraíba State
The presence of rash was observed at the same day of the initial symptoms or after it; there was no case where the rash started before the other symptoms. In 10/20 cases in Rio Grande do Norte State, the rash appeared at the same day of the other symptoms, and in Maranhão and Paraíba States, this occurred in 13/20 and 18/20 of the cases, respectively.
With regard to the part of the body where the rash first appeared, for most cases in Natal-RN (14/20) and João Pessoa-PB (12/20), it was the upper body; for the two municipalities of Maranhão, it was face/neck in 10/20 cases. The rash observed was the maculopapular type, in all the individuals interviewed in the four municipalities (Table 2).
Table 2 - Distribution of exanthematous syndrome cases, according to its appearance in comparison to the other symptoms, part of the body where it began and type, in the municipalities of Natal-RNa, Barra do Corda-MAb, São Luís-MAb, and João Pessoa-PBc, May, 2015
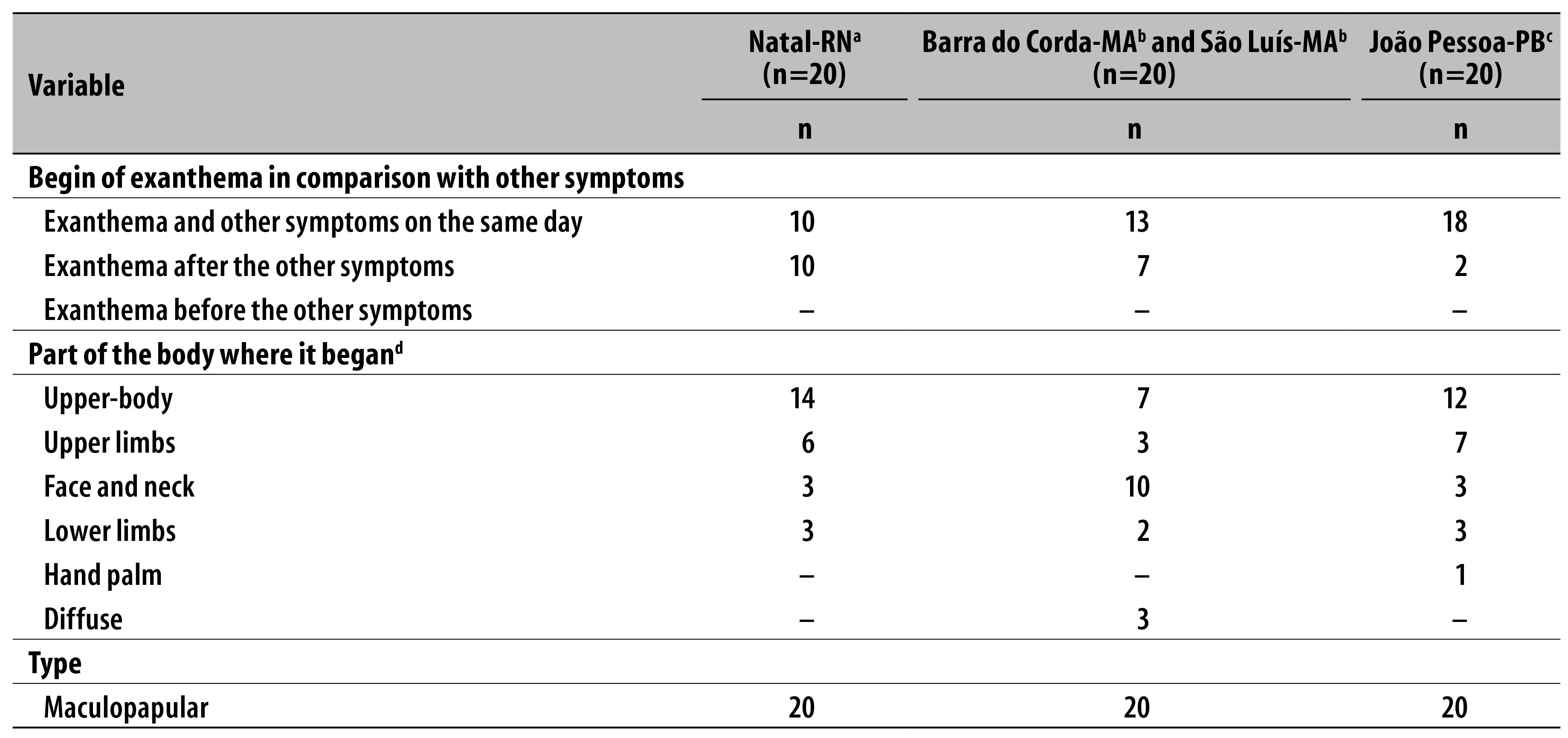
a) Rio Grande do Norte State
b) Maranhão State
c) Paraíba State
d) The exanthema may have begun in more than one part of the body
In Natal-RN, the mild fever occurred in two individuals; from the 18 individuals who did not report fever, 12 used analgesic/antipyretic (Table 3). In Maranhão (Barra do Corda-MA and São Luís-MA), from the 15 individuals who did not report fever, 8 used analgesic and antipyretic. The residents in João Pessoa-PB did not report fever.
Table 3 - Characterization of exanthematous syndrome cases, according to signs and symptoms, in the municipalities of Natal-RNa, Barra do Corda-MAb, São Luís-MAb, and João Pessoa-PBc, May, 2015
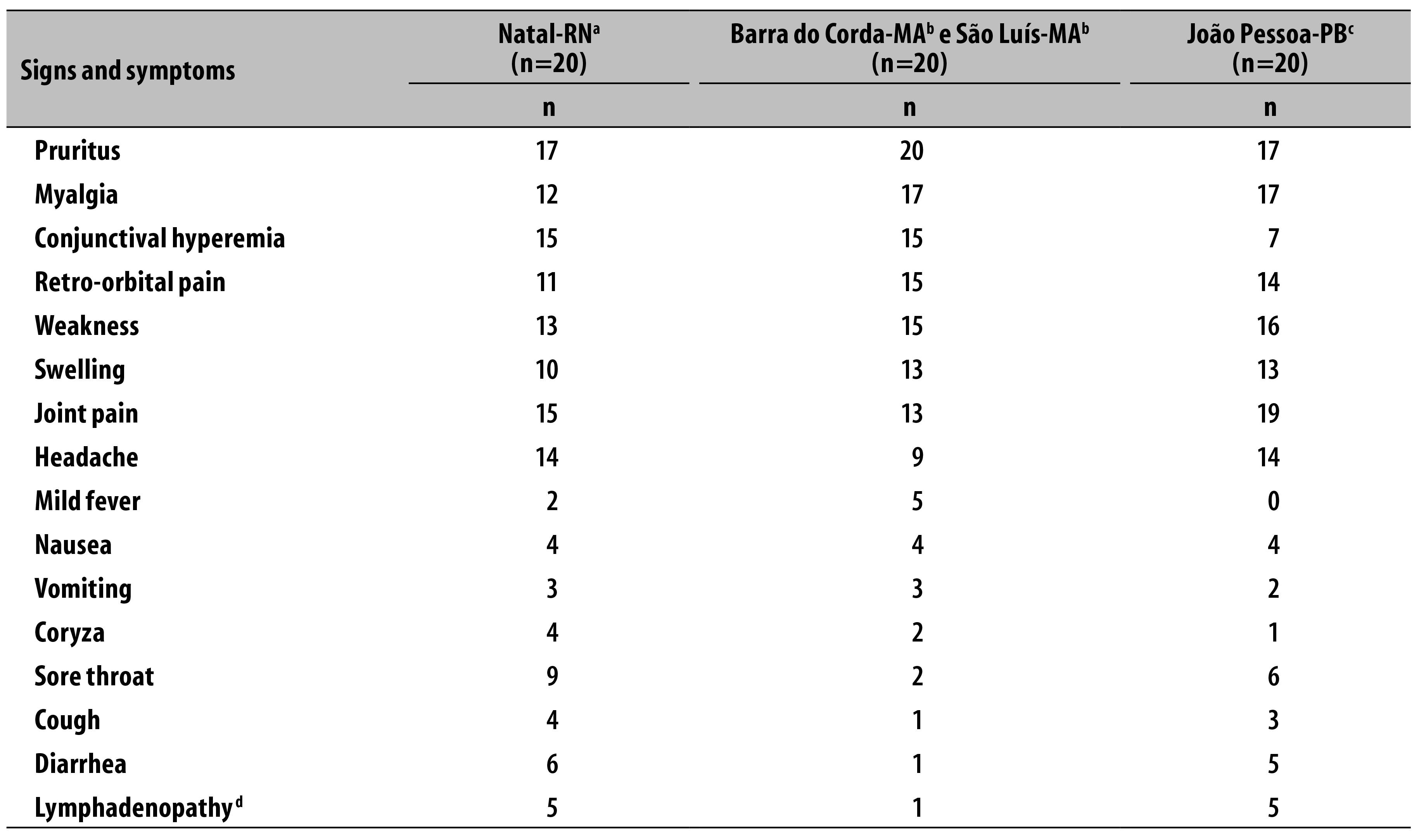
a) Rio Grande do Norte State
b) Maranhão State
c) Paraíba State
d) Auricular, occipital and cervical lymphadenopathy
The rash was present in 100% of the individuals interviewed in the states. In addition to this, among the residents of Rio Grande do Norte, the most frequently reported symptom was pruritus in 17/20 and 20/20 of the interviewed individuals, respectively. The residents in Paraíba, although having reported pruritus in 17/20 complained more frequently of joint pain (19/20) (Table 3). One individual was hospitalized in Natal-RN.
In João Pessoa-PB and Natal-RN, the individuals reported, most frequently, problems in the hands and ankles joints. In the municipalities of Maranhão, ankles, knees and wrists were reported to be the most painful joints. Concerning symmetry, in all the municipalities, 55 individuals suffered from joint pain on both the right and left sides (Table 4).
Table 4 - Distribution of exanthematous syndrome cases, according to part of the body of joint pain, in the municipalities Natal-RNa, Barra do Corda-MAb, São Luís-MAb, and João Pessoa-PBc, May, 2015

Note: the individual may had pain in more than one joint
a) Rio Grande do Norte State
b) Maranhão State
c) Paraíba State
In Natal-RN, a complete blood count (CBC) was conducted with the blood samples of 14 individuals: the platelet count was inferior to 100 thousand in one of the individuals; the average hematocrit value among the individuals who underwent the CBC was of 35.8 (range from 28.2 to 40.0).
In João Pessoa-PB, a CBC was conducted with blood samples of nine individuals and the average hematocrit was of 41.7 (range from 34.8 to 46.2) (Table 5).
Table 5 - Distribution of exanthematous syndrome cases, according to platelets and white blood cells count, in the municipalities of Natal-RNa and João Pessoa-PBb, May, 2015
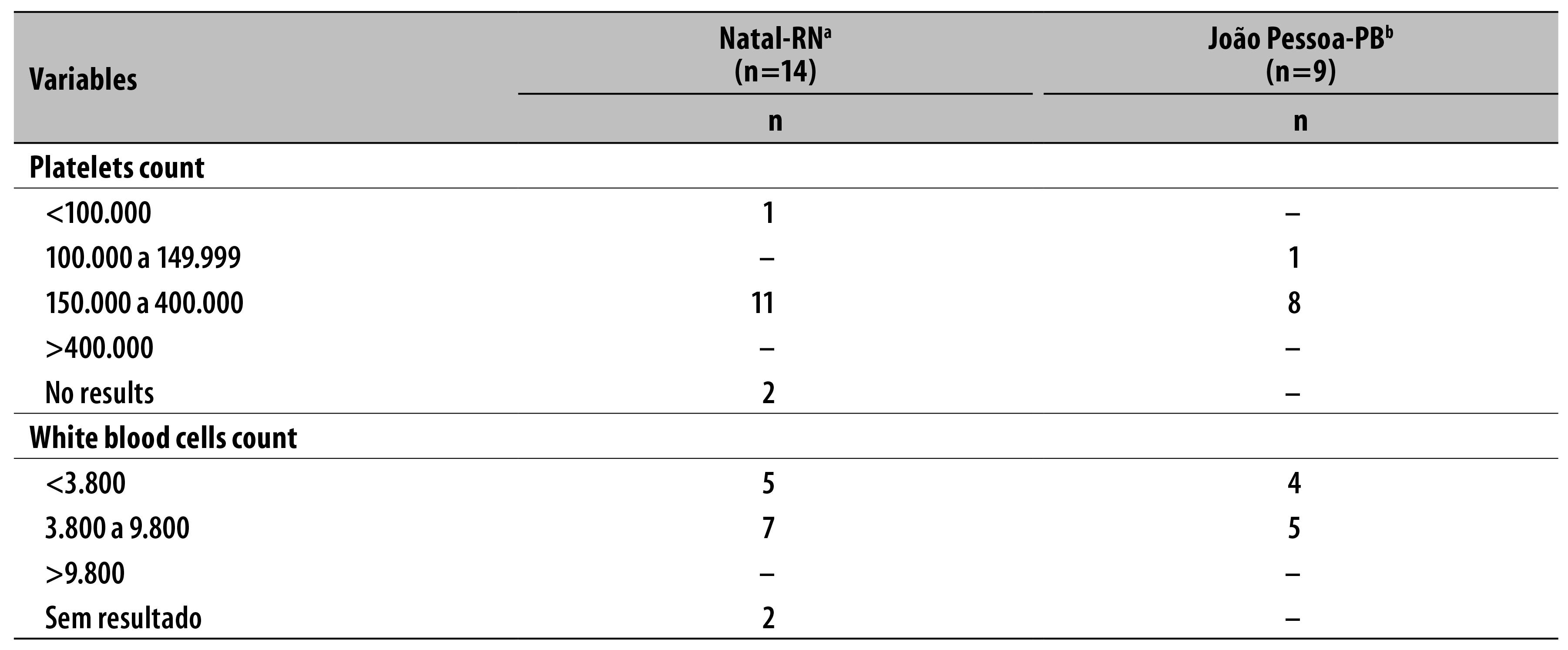
Note: the complete blood count was not performed in Barra do Corda-MA and São Luís-MA.
a) Rio Grande do Norte State
b) Paraíba State
The presence of food allergies - diagnosed by a doctor - was informed by five individuals in Natal-RN, two in Maranhão (Barra do Corda-MA and São Luís-MA) and three in João Pessoa-PB. Concerning immunization, 15 individuals from RN, 10 from MA and 12 from PB had received measles and rubella (MR) or measles, mumps and rubella (MMR) vaccines.
Of the first samples of IgM serology tested for dengue, measles, rubella and parvovirus B19, 11 resulted positive for dengue: seven in Natal-RN, three in Maranhão (Barra do Corda-MA and São Luís-MA), and one in João Pessoa-PB. For measles, rubella and parvovirus, the results were all negative. Of the second set of samples, six were positive for dengue in Maranhão (Barra do Corda-MA and São Luís-MA), and three of them had already resulted positive in the first sample.
The RT-PCR detected Zika virus in 18 cases: 12 in João Pessoa, four in Maranhão (Barra do Corda-MA and São Luís-MA) and two in Natal-RN. Five of these 18 cases had IgM positive for dengue.
Discussion
The present study described the first cases of Zika virus fever confirmed in the municipalities of Barra do Corda-MA, SãoLuís-MA, João Pessoa-PB and Natal-RN. The occurrence of dengue cases was also observed.
Zika virus is a RNA virus, of the genus Flavivirus, family Flaviviridae,10,11 with two lineages described so far: the Africam and the Asian.12 The virus was first isolated in non-human primates at the Zika forest, in Uganda, in 1947.13-15 Nowadays, there is record of sporadic circulation in Africa, Asia and Oceania.5,14 Zika virus was first identified in the Americas in 2014, in Easter Island, a Chilean territory located in the Pacific Ocean, 3,500 km far from the continent.16
The symptoms observed in the cases described in the present study were typical of Zika virus fever. The symptoms that appear due to the disease are: arthralgia, swelling in the limbs, mild fever, headache, retro-orbital pain, conjunctival hyperemia and maculopapular rash, frequently with pruritus.5
The rash may be present in a range of infectious diseases, such as measles, rubella, parvovirus, dengue, chikungunya fever, and Zika virus fever;5,6-8 in most of the definitions for these diseases, fever is one of the typical symptoms - except for rubella, which presents mild fever associated with rash and auricular, occipital and cervical lymphadenopathy; the latter being present in few cases identifyied with Zika virus fever.
In the present study, no samples were tested positive for measles and rubella, which confirms the vaccination history of the interviewed individuals who reported to have received MR or MMR vaccines. In the national immunization calendar, MMR vaccine is indicated for infants over 12 months old.17 There were no samples positive for parvovirus B19, either.
Among the individuals who reported mild fever, most of them had taken painkillers and antipyretics, which may have contributed to the absent or mild fever at the moment of measurement of body temperature. In turn, the fever, in some diseases such as dengue, roseola, measles or parvovirus lasts more than one day and reappears after the use of painkillers,18 which reinforces the negative results for measles and parvovirus.
The disease appeared to be benign, and there was only one record of hospitalization from the total of individuals interviewed. In cases of Zika virus fever, hospitalization has a low frequency.19
A high number of joint pain, mainly in hands and ankles, was observed. Viral agents are known to involve accute or chronic joint problems, and the most frequently affected joints are the proximal interphalangeal, the metacarpophalangeal, knees, ankles and elbow.20
The rash was maculopapular in all the cases, presenting the initial symptoms on the upper body, upper limbs and face/neck, with diffuse evolution and early start, usually on the same day of the other symptoms.
Diseases such as measles, rubella, parvovirus, dengue, roseola and Zika virus fever present maculopapular rash.5,7,21 In the case of dengue, the lesions are more common on the face, upper body and limbs, with or wihtout pruritus, and frequently appear after the disappearance of the fever, around the fifth day. In the case of Zika virus fever, the lesions usually spread over the upper body and limbs, come with pruritus, and appear on the first or second day.5,21
In most of the CBC tests, changes related to platelet, white blood cells and haematocrit count were not observed. Dengue, for example, may cause haematological changes which can be detected by CBC tests.22
The fact that more women were included in the study in Rio Grande do Norte and Maranhão (Barra do Corda-MA and São Luís-MA) may be related to a higher search of these individuals for health care, because they usually report diseases more easily than men and because they have better perception of their own signs and symptoms.23
The laboratory tests identified the presence of the Zika virus and IgM positive for dengue, which suggests a cross reaction. The results presented in this study highlight the importance on implementing differential diagnosis for exanthematous diseases. We recommend the implementation of a sentinel surveillance protocol for Zika virus fever in order to monitor the cases timely, contributing to the early and accurate adoption of control measures; and also to follow the laboratory flow recommended in the sentinel surveillance protocol to diagnose the disease, with the objective of identifying viral circulation in other Brazilian states. Likewise, we highlight the need of developing adequate diagnosis tests for Zika virus, in order to minimize the cross reaction with serology for dengue.
Referências
1. Ministério da Saúde (BR). Nota informativa: Ministério da Saúde intensifica medidas de controle da febre Chikungunya. Brasília: Ministério da Saúde; 2014 [citado 2016 jul 19]. Disponível em: Disponível em: http://portalsaude.saude.gov.br/index.php/cidadao/principal/agencia-saude/14666-ministerio-da-saude-intensifica-medidas-de-controle-da-febre-chikungunya [ Links ]
2. Silva JA, Ferreira R, Hamidah AM, Pinto Junior VL. Abordagem diagnóstica das doenças exantemáticas na infância. Rev Med Saude Brasilia. 2012 jan-abr;1(1):10-9. [ Links ]
3. Silva NVA. Doenças exantemáticas da infância com manifestações orais. [dissertação]. Porto: Universidade do Porto; 2010. [ Links ]
4. Lopes N, Nozawa C, Linhares REC. Características gerais e epidemiologia dos arbovírus emergentes no Brasil. Rev Pan-Amaz Saude. 2014 set;5(3):55-64. [ Links ]
5. Ioos S, Mallet HP, Goffart IL, Gauthier V, Cardoso T, Herida M. Current Zika virus epidemiology and recent epidemics. Med Mal Infect. 2014 Jul;4(7):302-7. [ Links ]
6. Santos APT, Russo DH, Machado BC, Luchs A, Timenetsky MCST, Carmona RCC. Echovírus 6 associado à doença exantemática. Rev Soc Bras Med Trop. 2008 nov-dez;41(6):672-5. [ Links ]
7. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Guia de vigilância em saúde. Brasília: Ministério da Saúde; 2014. [ Links ]
8. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Preparação e resposta à introdução do Vírus Chikungunya no Brasil: baseado no livro Preparación y respuesta ante la eventual introducción del virus chikungunya en las Américas. Brasília: Ministério da Saúde ; 2014. [ Links ]
9. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Nota Informativa nº6/2015 CIEVS/DEVIT/SVS/MS [Internet]. Brasília:Ministério da Saúde; 2015 [citado 2016 jul 19]. Disponível em: Disponível em: http://www.aeciherj.org.br/publicacoes/Informativos-CCIH/Nota-informativa-6-2015.pdf [ Links ]
10. Diallo D, Sall AA, Diagne CT, Faye O, Ba Y, Hanley KA, et al. Zika virus emergence in mosquitoes in southeastern Senegal, 2011. Plos One. 2014 Oct;9(10):e109442. [ Links ]
11. Hamel R, Dejarnac O, Wichit S, Ekchariyawat P, Neyret A, Luplertlop N, et al. Biology of Zika virus infection in human skin cells. J Virol. 2015 Sep;89(17):8880-96. [ Links ]
12. European Centre for Disease Prevention and Control. Rapid risk assessment: Zika virus infection outbreak, French Polynesia: 14 february 2014 [Internet]. Stockholm: European Centre for Disease Prevention and Control; 2014 [cited 2016 Jul 19]. Available from: Available from: http://ecdc.europa.eu/en/publications/Publications/Zika-virus-French-Polynesia-rapid-risk-assessment.pdf [ Links ]
13. Faye O, Freire CCM, Iamarino A, Faye O, Oliveira JVC, Diallo M, et al. Molecular evolution of Zika virus during its emergence in the 20th century. PloS Negl Trop Dis. 2014 Jan;8(1):e2636. [ Links ]
14. Balm MN, Lee CK, Lee HK, Chiu L, Koay ES, Tang JW. A diagnostic polymerase chain reaction assay for Zika virus. J Med Virol. 2012 Sep;84(9):1501-5. [ Links ]
15. Hayes EB. Zika virus outside Africa. Emerg Infect Dis. 2009 Sep;15(9):1347-50. [ Links ]
16. Ministerio de Salud (CL). Departamento de Epidemiología. División de Planificación Sanitaria. Virus Zika: informe de situación: información disponible al 20 de marzo del 2014 [Internet]. Santiago: Ministerio de Salud; 2014 [citado 2016 Jul 19]. Disponible en: Disponible en: http://www.sochinf.cl/sitio/templates/sochinf2008/documentos/2014/Informe_situacion_Zika_Isla_de_Pascua.pdf [ Links ]
17. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Manual de normas e procedimentos para vacinação. Brasília: Ministério da Saúde; 2014. [ Links ]
18. Ministério da Saúde (BR). Informações técnicas [Internet]. Brasília: Ministério da Saúde; 2015 [citado 2016 Jul 19]. Disponível em: Disponível em: http://portalsaude.saude.gov.br/index.php/informacoes-tecnicas-sarampo [ Links ]
19. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Febre pelo vírus Zika: uma revisão narrativa sobre a doença. Bol Epidemiol. 2015;46(26):1-7. [ Links ]
20. Oliveira SA, Camacho LAB, Bettini LR, Fernandes DG, Gouvea NAC, Barros RAQ, et al. Manifestações articulares nas viroses exantemáticas. Rev Soc Bras Med Trop. 1999 mar-abr;32(2):125-30. [ Links ]
21. Ranie Ralph. Pediatria: doenças exantemáticas [Internet]. Vitória: Ranie Ralph, 2016 [citado 2016 jul 19]. Disponível em: Disponível em: http://ranieralph.com/ [ Links ]
22. Barros LPS, Igawa SES, Jocundo SY, Brito Júnior LC. Análise crítica dos achados hematológicos e sorológicos de pacientes com suspeita de Dengue. Rev Bras Hematol Hemoter. 2008 set-out;30(5):363-6. [ Links ]
23. Barros MBA, César CLG, Carandina L, Torre GD. Desigualdades sociais na prevalência de doenças crônicas no Brasil, PNAD-2003. Cienc Saude Coletiva. 2006 out-dez;11(4):911-26. [ Links ]
Received: June 15, 2016; Accepted: July 20, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
