










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.25 n.4 Brasília out./dez. 2016
http://dx.doi.org/10.5123/S1679-49742016000400011
ORIGINAL ARTICLE
Time trend of lack of access to health services in Brazil, 1998-2013
1Universidade Federal de Pelotas, Departamento de Enfermagem, Pelotas-RS, Brasil
2Universidade Federal de Pelotas, Programa de Pós-Graduação em Epidemiologia, Pelotas-RS, Brasil
3Instituto de Pesquisa Econômica Aplicada, Diretoria de Estudos e Políticas Sociais, Brasília-DF, Brasil
4Universidade de São Paulo, Departamento de Epidemiologia, São Paulo-SP, Brasil
5Universidade Federal de Pelotas, Programa de Pós-Graduação em Enfermagem, Pelotas-RS, Brasil
OBJECTIVE:
to analyze the time trend on the demand and lack of access to public health services in Brazil.
METHODS:
this is a panel of cross-sectional studies with data of the National Household Sample Survey (1998, 2003, 2008) and the National Health Survey (2013); the prevalence of demand and lack of access within the fifteen days prior to the survey was estimated; Poisson regression was used for trend analysis.
RESULTS:
the demand for health services increased from 13.0% (95%CI 12.3;13.7), in 1998, to 15.0% (95%CI 14.5;15.4), in 2013; the lack of access remained stable, being of 3.7% (95%CI 3.2;4.2) in 1998 and 4.5% (95%CI 4.0;5.0) in 2013.
CONCLUSIONS:
the increase in demand for health services and the stability in the lack of access indicate improvements in the Brazilian public health system performance; additional efforts are required to ensure universal access to public health services in Brazil.
Key words: Health Services Accessibility; Equity in Access; Brazilian National Health System; Time Series Studies; Brazil
Introduction
Access to health services is a constitutional right of the population, guaranteed with the creation of the Brazilian National Health System (SUS), in 1990.1,2 Since then, several improvements in the health system have been noticed, especially those related to the expansion of the Family Health Strategy (FHS), implemented in 1994.1-5
The use of health services has increased in Brazil, especially medical appointments, mainly because of the expansion of primary health care services.6 However, the use of health care services does not depend only on the offer, but also on the perception of need and the demand for health services by the population.7
Although utilization is a good proxy of access to health care service, its definition excludes individuals who sought health care but were not assisted, which also indicates lack of access.8,13 Despite the deficient information about the lack of access to health care services in Brazil, population-based surveys showed prevalence lower than 7% of the total of individuals who sought health care.8,9,14 When these findings are scaled-up to the Brazilian population, using the National Household Sample Survey (PNAD), it is estimated that, in 2003, approximately one million people could not access public health services within the fifteen days prior to the survey.14 Another national study, conducted in 2009, found that 1.1% of adults did not have access to medical appointments within three months prior to the survey and 3% did not have access to hospitalization within twelve months prior to the survey.9 Findings from a study conducted in 2012 in the south of Brazil showed a lack of access in the month prior to the interview of 6.5%, which represents approximately 4,500 of the 220 thousand adults living in the urban area of Pelotas, Rio Grande do Sul.8
The identification of trends of lack of access to Health Care in the country may help with the recognition of SUS remaining challenges, as well as contributing to support necessary policies and actions to ensure, for real, the universal access to health services established in the 1988 Federal Constitution. The objective of this study was to analyze the time trend on the demand and lack of access to public health services in Brazil, from 1998 to 2013.
Methods
This is a panel of cross-sectional studies of national basis that used data from the National Household Sample Survey (PNAD) and the National Health Survey (PNS), both initiatives of the Brazilian Institute of Geography and Statistics (IBGE) in partnership with the Ministry of Health. We used data from the PNAD conducted in 1998, 2003 and 2008, which included a supplement on health, and the PNS held in 2013.
The sampling procedure of PNAD and PNS was conducted per clusters, in three stages. The four samples are representative of the country, regions, states and some metropolitan areas, except for the 1998 and 2003 PNAD, whose samples did not include households located in the rural area of the North region. During the three years of PNAD, approximately one million people were interviewed (1998 = 344,975; 2003 = 384,844; 2008 = 391,868). The final sample of PNS was composed of 64,348 household surveys. Information on the use of health services was provided by 205,546 residents of those households, and on self-reported morbidity by 60,202 residents. A total of 1,327,233 individuals of all ages participated in the surveys. More information can be obtained in other papers.15-18
The study outcomes were the demand and lack of access to health care services, self-reported by the surveyed individuals. The demand for health care was identified through the following question: "In the last two weeks, did you seek any place, a health care service or a health professional for assistance related to your own health?". Lack of access was measured using the following question: "In this first time you sought health care in the last two weeks, did you get assistance?". The questions used were the same throughout the whole research.
The prevalence of demand and lack of access and their respective 95% confidence intervals (95%CI) were obtained according to the following variables:
- sex (male; female);
- age (in years: children, from 0 to 9; adolescents, from 10 to 19; adults, from 20 to 59; elderly, 60 or older);
- skin color (white; black; brown);
- education level (no schooling; elementary school; high school; higher education);
- area of residence (urban; rural);
- country's region (North; Northeast; South; Southeast; Midwest);
- self-reported diagnosis of hypertension (no; yes) and diabetes mellitus (yes; no);
- number of diseases (self-reported diagnosis of hypertension, diabetes mellitus, heart condition, asthma, arthritis, back problem and depression, quantified as: zero; one; two; three or more diagnosed diseases);
- coverage of FHS (yes; no, only for 2008 and 2013); and
- private health insurance (yes; no)
The time trend of lack of access was also assessed according to the reasons for seeking health care (routine or prevention; disease; dental problem), reasons for not getting assistance (lack of vacancy, lack of doctors, lack of service or specialized professional, service or equipment not working, not able to pay for it, long time waiting) and type of service sought (primary health care units [UBS]; emergency rooms and hospitals, clinics, other health professionals' offices, private medical offices).
The descriptive analysis included the calculation of proportions (%) and 95%CI. Annual variation of demand and lack of access to health services was calculated using the values observed in 1998 and 2013, and obtained by the following formula:
Where p1998 and P2013 are the prevalences in those years. The trend was classified as increasing, decreasing or stable, according to the annual variation value (positive, negative or zero, respectively) and p-value. Trends with p-value <0.05 in the Wald test for linear trends were considered statistically significant. Crude and adjusted analyses were estimated by Poisson regression.19 For adjusted trends all the independent variables were included in the regression. The variables related to self-reported morbidities were not included in the adjustment, because this information was gathered from a smaller number of respondents in 2013, according to PNAD methods.17,18
The databases were obtained from IBGE website (www.ibge.gov.br/home). Analyses were performed using the statistical program Stata(r) 12.1. All analyses were performed with the survey module, considering the sampling process used in the surveys.
PNAD and PNS projects were submitted and approved by the National Research Ethics Committee (CONEP).15,16,18 All participants signed the Term of Free Informed Consent.
Results
The description of the four research samples are presented in Table 1 and shows the demographic and epidemiological changes in the Brazilian population. From 2008 to 2013, the elderly population increased from 8.8 to 13.0%; the proportion of individuals who self-reported white-skinned decreased from 54.0 to 45.6%; and the percentage of individuals with no schooling decreased from 27.7 to 16.2%. An increase in the prevalence of chronic diseases was observed. FHS coverage increased 12.3 percentage points between 2008 and 2013 (from 50.9 to 63.2%). Health insurance coverage remained stable with slight increase in 2013, reaching 27.9% of the Brazilian population (Table 1).
Table 1 - Description of demographic and socioeconomic characteristics, morbidities and health care services coverage, according to the year of study. Brazil, 1998-2013
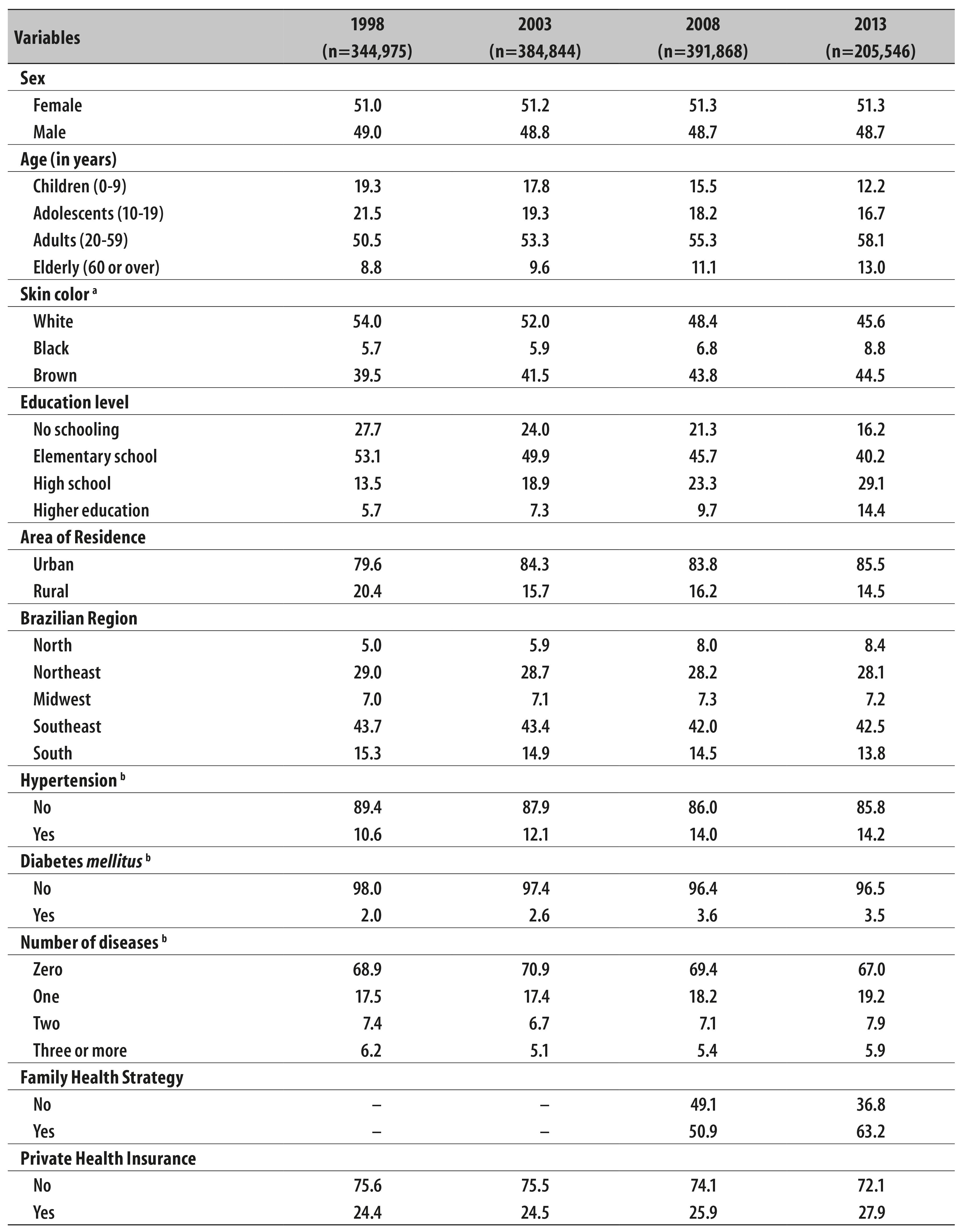
a) Skin color: yellow and indigenous represented less than 1% of the population, for all the years.
b) Only for individuals aged 18 or older in 2013.
The demand for health services within the fifteen days prior to the survey was of 13.0% (95%CI 12.3;13.7) in 1998 and 15.0% (95%CI 14.5;15.4) in 2013. There was an increasing time trend in the demand for health services in the total population (annual variation of 1.0%; p <0.001) and for most of the analyzed variables. The highest annual increase was observed for individuals who reported not having diabetes (+ 2.0%) (Table 2).
Table 2 - Time trends in demand for health care services according to demographic, socioeconomic, morbidity and coverage of health services variables. Brazil, 1998-2013
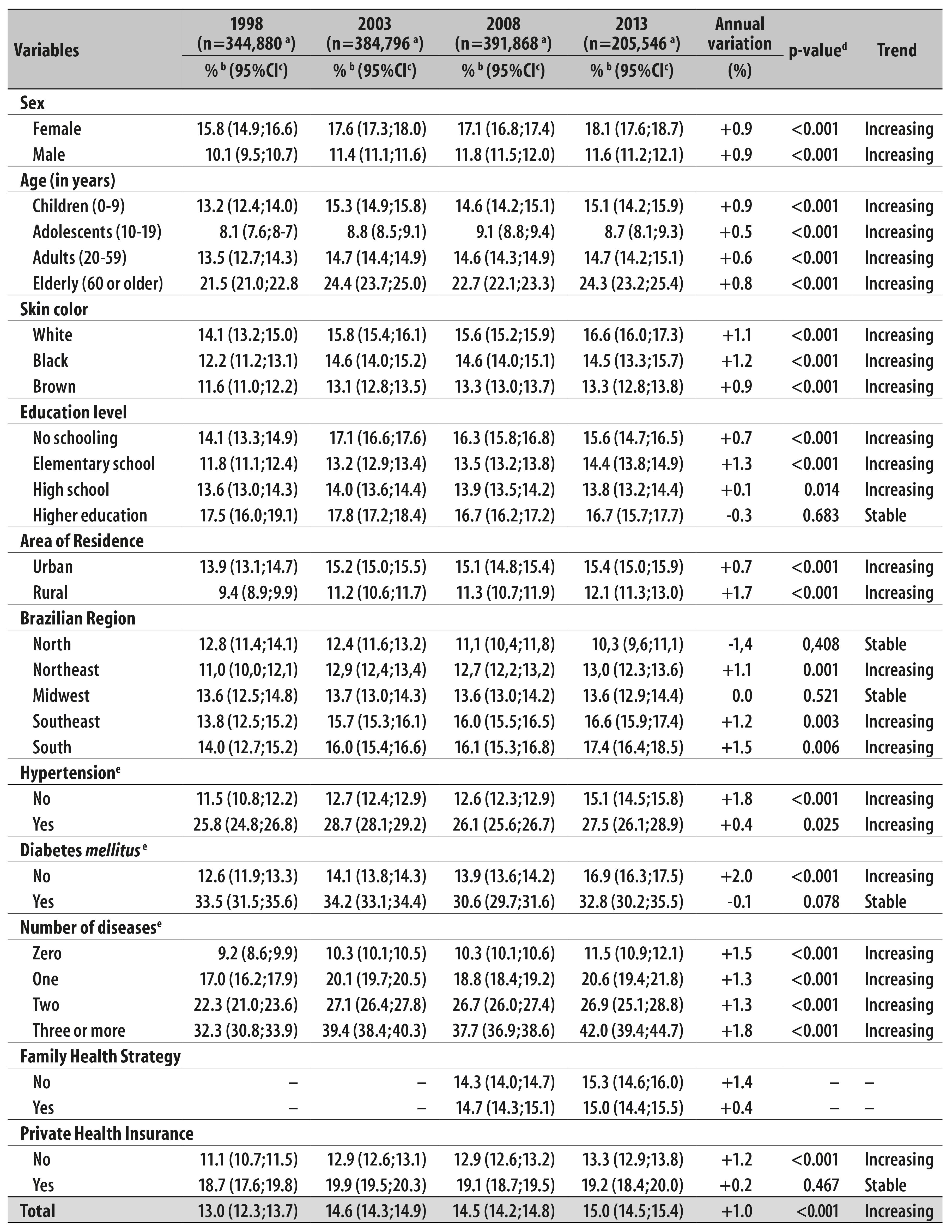
a) Number of people who sought health care within the fifteen days prior to the survey.
b) %: prevalence.
c) 95%CI: 95% confidence level.
d) p-value: Wald test of linear trends, obtained by Poisson regression adjusted for other variables in the table - except for morbidities.
e) Only for individuals aged 18 or older in 2013.
The lack of access was stable in the period (annual growth of 1.3%; p = 0.565), ranging from 3.7% (95%CI 3.2;4.2) in 1998 to 4.5% (95%CI 4.0;5.0) in 2013. The trends remained stable in almost all categories of the analyzed variables; the exception was for residents in the south of Brazil, who had decreasing trend of lack of access to health services: annual variation of -0.4%; p = 0.006 (Table 3).
Table 3 - Time trends of lack of access (in the first health care facility searched) according to demographic, socioeconomic, morbidity and coverage of health services variables. Brazil, 1998-2013

a) Number of people who sought health care within the fifteen days prior to the survey.
b) %: prevalence.
c) 95%CI: 95% confidence level.
d) p-value: Wald test of linear trends, obtained by Poisson regression adjusted for other variables in the table - except for morbidities.
e) Only for individuals aged 18 or older in 2013.
The trend for lack of access was decreasing for the variable search for health care driven by routine or prevention (annual decrease of 7.1%; p <0.001), and increasing for disease (annual growth of 3.2%; p <0.001). The reasons for the lack of access presented stability and the most mentioned were: lack of vacancy and lack of doctors (80.0% of the reasons of lack of access). Not being able to pay for health care was a virtually non-existent reason in the period (Table 4).
Table 4 - Time trend of lack of access according to reasons for seeking care and reasons for lack of health care. Brazil, 1998-2013
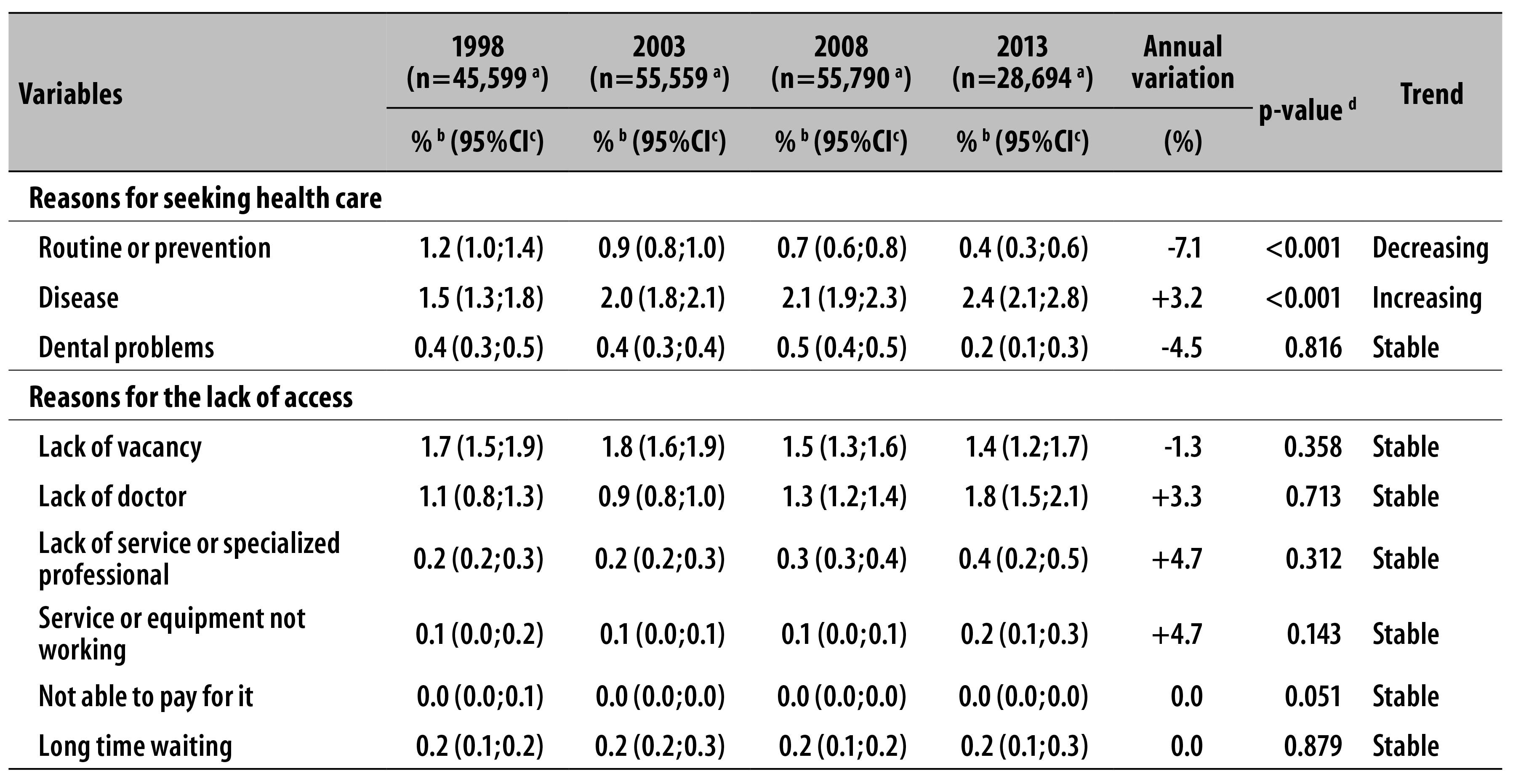
a) Number of people who sought health care within the fifteen days prior to the survey.
b) %: prevalence.
c) 95%CI: 95% confidence level.
d) p-value: Wald test of linear trends, obtained by adjusted Poisson regression.
Figure 1 shows the time trend of lack of access related to the type of service sought. No statistically significant differences were observed. However, it was possible to identify that the health services with the highest percentage of lack of access, for all the periods, were those provided by the primary health care units (between 6.0 and 8.0%).

Discussion
From 2008 to 2013, the demand for health care services by the Brazilian population has increased significantly, especially among individuals without health insurance, less schooling and residents of rural areas. On the other hand, the prevalence of lack of access was low and stable. In 2013, for every 20 individuals who sought care in the fifteen days prior to the survey, one did not receive care in the first health care facility they went. Most of the reasons for lack of access were related to the lack of professionals for health care, especially doctors.
We should consider some limitations in this present study. One limitation relates to the question used to measure the lack of access. Despite of being used in the literature,8,9,20 the way the question was posed may not have taken into account the organization of primary health care services, which, in some cases, host the individual and schedule appointment for a later date. Also, the inadequate search for secondary and tertiary health care services for problems related to primary health care would also result in reports of lack of access, as measured. A significant proportion of the demand for emergency services, for example, could be assisted in primary health care units, but for different reasons, mainly cultural, first the population seeks services considered more specialized, rather than going directly to the UBS.21 These situations may result in an overestimation of the prevalence of lack of access. However, this potential bias in the study is minimized exactly by the high number of people who had lack of access searching for UBS. Another limitation refers to methodological differences between the PNAD and PNS, for example, the non-inclusion of rural households in the 1998 and 2003 PNAD, and differences in the geographic distribution of the survey, given that there was difference in the municipalities included. However, as comparisons were performed between specific municipalities, these methodological differences in time trends estimates may have low influence. Furthermore, by restricting the results to the Brazilian state capitals, which are the same municipalities in both studies (data not shown), the findings are very similar to those described in this article.
The results of this study show advances in the Brazilian health system. By ensuring health care without direct payment by the citizen, SUS contributes to a low and stable percentage of lack of access in the period studied, despite the growing demand. Moreover, the decreasing lack of access in the southern region of Brazil may result from the rapid and recent expansion of the Family Health Strategy and primary health care services, especially in Rio Grande do Sul. The southern states have always presented population services coverage indicators lower than those of states in the Northeast, for example, where the FHS was initially implemented.4 However, universal access depends on overcoming barriers still observed, especially for users of the primary health care services, which assists the largest number of Brazilians. By scaling-up the prevalence found in 2013 for the Brazilian population, it is estimated that 874,496 people had no access to primary health care services when seeking care.
Among those people who sought care at UBS, there was stability in the lack of access more often than with those who sought care elsewhere. In 2013, for every 13 individuals who sought care at a UBS within the fifteen days prior to the survey, only one was not assisted in the first place he/she went. However, it is important to notice that the demand for care in the UBS has increased significantly during the period studied, concomitantly with the expansion of primary health care, especially of the FHS.
Despite the low percentage significance, the magnitude of the lack of access observed in Brazil is a major problem. It is important to highlight that the outcome assessed refers to the lack of assistance in the first unit sought, and not to the obstacles in the access. That is, those individuals who did not seek health services due to different difficulties of access, related to their behavior in the search for care, personal issues,1 prejudice22 and organizational problems.
Organizational problems of health care services4,5 seems to explain better the lack of access to services. Without disregarding the importance of barriers related to the individuals, those imposed by the health services can be more easily resolved by managers and health workers. It is noteworthy that the first contact with the health service is usually due to the personal behavior of those looking for that service,11,12 but success in finding and persistence in care depend mainly on the characteristics of the services and the work of the professional involved.5,7,23,24
Moreover, the growing demand for health services in Brazil may have contributed to the maintenance of the lack of access problem. The increasing number of people seeking for health care, in almost all groups, although higher among the poor and those without chronic diseases, suggests a more comprehensive and varied demand. This finding indicates a more equal and fair access to services, regardless of economic and health conditions. The change in how much care is necessary for the proper confrontation of the increase of noncommunicable diseases should not be restricted only to the treatment of individuals of high risk. It requires an increase in primary and secondary prevention actions to avoid the preventive paradox highlighted by Rose,25 when focusing on actions for individuals is minimized by the negative influence of social determinants of health.
These study findings are consistent with results from other national baseline study and a population-based study in southern Brazil.8,9 These studies also point out that the main reasons for lack of access are related to human resources issues and the way of organizing the demand. The low number of health professionals, a historical problem for the Brazilian health system, significantly impacts on access to care. In addition, a large part of the country access to UBS is done through attendance forms, which are precarious and obsolete, making it difficult to guarantee universality, equity and integrity in SUS.26 Usually, people have to wait hours for the UBS to open and to get the attendance form, which perpetuates inequalities in health as the most vulnerable individuals and with lower socioeconomic conditions represent most part of users of the services which are organized this way.5
Restructuring the assistance in primary health care units, ensuring assistance to spontaneous demand and humanization in access to services are priority tasks to improve the Brazilian health system performance.26-28 In this sense, one of the initiatives already implemented is the Programa Mais Médicos (More Doctors Program), which has increased the availability of doctors in the poorest regions of Brazil and will ensure greater public access to health services.29 In addition, the More Doctors intends to increase the number of places in medical schools in the country. 29 However, with the data here presented, it is not possible to evaluate any effect of the program since its implementation only began in 2013, the last research year included in this present study.
Despite the achievements, the findings confirm the relevance of the analysis of the lack of access to health care services, especially to guide decisions of managers and health workers in order to achieve universality and comprehensiveness in SUS. The increasing demand and stability in the lack of access indicates advances in the performance of the public health system. There are still challenges. Improvements are necessary in the management and supply of services, including the provision of human resources, to improve the performance of the Brazilian National Health System and to ensure universal and equal access to health services in Brazil.
Referências
1. Paim J, Travassos C, Almeida C, Bahia L, Macinko J. The Brazilian health system: history, advances, and challenges. Lancet. 2011 May;377(9779):1778-97. [ Links ]
2. Barreto ML, Rasella D, Machado DB, Aquino R, Lima D, Garcia LP, et al. Monitoring and evaluating progress towards universal health coverage in Brazil. PLoS Med. 2014 Sep;11(9):e1001692. [ Links ]
3. Rasella D, Harhay MO, Pamponet ML, Aquino R, Barreto ML. Impact of primary health care on mortality from heart and cerebrovascular diseases in Brazil: a nationwide analysis of longitudinal data. BMJ. 2014 Jul;349:g4014 [ Links ]
4. Facchini LA, Piccini RX, Tomasi E, Thumé E, Silveira DS, Siqueira FV, et al. Desempenho do PSF no Sul e no Nordeste do Brasil: avaliação institucional e epidemiológica da Atenção Básica à Saúde. Cienc Saude Coletiva. 2006 jul-set;11(3):669-81. [ Links ]
5. Facchini LA, Thumé E, Nunes BP, Silva SM, Fassa AG, Garcia LP, et al. Governance and health system performance: national and municipal challenges to the Brazilian Family Health Strategy. In: Reich MR, Takemi K, editors. Governing health systems: for nations and communities around the world. Brookline: Lamprey & Lee; 2015. p. 203. [ Links ]
6. Macinko J, Lima-Costa MF. Horizontal equity in health care utilization in Brazil, 1998-2008. Int J Equity Health. 2012 Jun;11:33. [ Links ]
7. Andersen RM. Revisiting the behavioral model and access to medical care: does it matter? J Health Soc Behav. 1995 Mar;36(1):1-10. [ Links ]
8. Nunes BP, Thumé E, Tomasi E, Duro SMS, Facchini LA. Socioeconomic inequalities in the access to and quality of health care services. Rev Saude Publica. 2014 Dec;48(6):968-76. [ Links ]
9. Dilélio AS, Tomasi E, Thumé E, Silveira DS, Siqueira FCV, Piccini RX, et al. Lack of access and continuity of adult health care: a national population-based survey. Rev Saude Publica . 2015 Jun;49:1-15. [ Links ]
10. Barker D, Rose G. Epidemiology in medical practice. Edinburgh: Churchill Livingstone; 1990. [ Links ]
11. Travassos C, Castro MSM. Determinantes e desigualdades sociais no acesso e na utilização de serviços de saúde. In: Giovanella L, Escorel S, Lobato LVC, Noronha JC, Carvalho AI, organizadores. Políticas e sistema de saúde no Brasil. Rio de Janeiro: Fiocruz; 2008. p. 215-43. [ Links ]
12. Travassos C, Martins M. Uma revisão sobre os conceitos de acesso e utilização de serviços de saúde. Cad Saude Publica. 2004;20 supl 2:S190-8. [ Links ]
13. Oliver A, Mossialos E. Equity of access to health care: outlining the foundations for action. J Epidemiol Community Health. 2004 Aug,2004;58(8):655-8. [ Links ]
14. Ribeiro MCSA, Barata RB, Almeida MF, Silva ZP. Perfil sociodemográfico e padrão de utilização de serviços de saúde para usuários e não-usuários do SUS - PNAD 2003. Cienc Saude Coletiva . 2006 out-dez;11(4):1011-22. [ Links ]
15. Instituto Brasileiro de Geografia e Estatística. Diretoria de Pesquisas. Coordenação de Trabalho e Rendimento. Pesquisa Nacional de Saúde 2013: percepção do estado de saúde, estilos de vida e doenças crônicas: Brasil, Grandes Regiões e Unidades da Federação. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2014. [ Links ]
16. Travassos C, Viacava F, Laguardia J. Os suplementos saúde na Pesquisa Nacional por Amostra de Domicílios (PNAD) no Brasil. Rev Bras Epidemiol. 2008;11 supl 1:98-112. [ Links ]
17. Souza-Júnior PRB, Freitas MPS, Antonaci GA, Szwarcwald CL. Desenho da amostra da Pesquisa Nacional de Saúde 2013. Epidemiol Serv Saude. 2015 abr-jun;24(2):207-16. [ Links ]
18. Damacena GN, Szwarcwald CL, Malta DC, Souza Júnior PRB, Vieira MLFP, Pereira CA, et al. O processo de desenvolvimento da Pesquisa Nacional de Saúde no Brasil, 2013. Epidemiol Serv Saude . 2015 abr-jun;24(2):197-206. [ Links ]
19. Barros AJ, Hirakata VN. Alternatives for logistic regression in cross-sectional studies: an empirical comparison of models that directly estimate the prevalence ratio. BMC Med Res Methodol 2003 Oct;3:21 [ Links ]
20. Arrivillaga M, Borrero YE. Visión comprensiva y crítica de los modelos conceptuales sobre acceso a servicios de salud, 1970-2013. Cad Saude Publica . 2016 maio;32(5):e00111415. [ Links ]
21. Carret ML, Fassa AC, Domingues MR. Inappropriate use of emergency services: a systematic review of prevalence and associated factors. Cad Saude Publica . 2009 Jan;25(1):7-28. [ Links ]
22. Baumgarten A, Peron TB, Bastos JL, Toassi RFC, Hilgert JB, Hugo FN, et al. Experiências de discriminação relacionadas aos serviços de saúde: análise exploratória em duas capitais do Sul do Brasil. Epidemiol Serv Saude . 2015 jul-set;24(3):353-62 [ Links ]
23. Facchini LA, Nunes BP, Duro SMS, Thumé E, Siqueira F, Fripp JC, et al. Iniquidades socioeconômicas no acesso e na qualidade da atenção ao diabetes entre idosos brasileiros. In: Conselho Nacional de Secretários de Saúde (BR). CONASS Debate: a crise contemporânea dos modelos de atenção à saúde. Brasília: Conselho Nacional de Secretários de Saúde; 2014. [ Links ]
24. Starfield B. Atenção primária: equilíbrio entre necessidades de saúde, serviços e tecnologia. Brasília: UNESCO. Ministério da Saúde; 2002. [ Links ]
25. Rose G. Sick individuals and sick populations. Int J Epidemiol. 2001 Jun;30(3):427-32. [ Links ]
26. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Atenção Básica. Brasília: Ministério da Saúde; 2012. p. 110. (Série E. Legislação em Saúde) [ Links ]
27. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Acolhimento à demanda espontânea. Brasília: Ministério da Saúde; 2011. p. 56. (Cadernos de Atenção Básica, n. 28, v. 1) [ Links ]
28. Vieira-da-Silva LM, Chaves SC, Esperidião MA, Lopes-Martinho RM. Accessibility to primary healthcare in the capital city of a northeastern state of Brazil: an evaluation of the results of a programme. J Epidemiol Community Health . 2010 Dec;64(12):1100-5. [ Links ]
29. Ministério da Saúde (BR). Secretaria de Gestão do Trabalho e da Educação na Saúde. Programa mais médicos - dois anos: mais saúde para os brasileiros. Brasília: Ministério da Saúde ; 2015. p. 129. [ Links ]
Received: April 28, 2016; Accepted: June 06, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
