










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.1 Brasília jan./mar. 2017
http://dx.doi.org/10.5123/s1679-49742017000100003
ORIGINAL ARTICLE
Assessment of the investigation of ill-defined causes of death in Brazil in 2010
1Universidade Federal de Minas Gerais, Grupo de Pesquisas em Epidemiologia e Avaliação em Saúde-GPEAS, Belo Horizonte-MG, Brasil
2Universidade Federal de Minas Gerais, Programa de Pós-Graduação em Saúde Pública, Belo Horizonte-MG, Brasil
Objective:
to assess the results of the investigation of ill-defined causes of death (IDCD) to improve the quality of cause-of-death data in Brazil.
Methods:
this is a descriptive study using data from the Mortality Information System; all IDCD which occurred in 2010 were selected; deaths were analyzed according to macroregions, states, state capitals and characteristics of how the investigations were carried out.
Results:
the proportion of IDCD was 8.6% in Brazil in 2010 and decreased to 7.0% after investigation and fell from 4.7% to 3.4% in state capitals after investigation; approximately 65% of the investigated cases were reclassified to a defined cause in states and state capitals.
Conclusion:
there was an improvement in data quality on cause of death resulting from these investigations which have led to an important decrease in the proportion of IDCD in the states and state capitals, although there are still some regional inequalities.
Key words: Causes of Death; Mortality Registries; Information Systems; Health Evaluation; Vital Statistics
Introduction
Mortality indicators are essential to understand the epidemiologic profile and assess the populations’ health situation, and for planning, monitoring and evaluating health services. In this sense, data on death causes are the most used.1 However, mortality analysis can be compromised in cases where there is a high number of ill-defined causes of death (IDCD), especially in time series studies and in the distribution of causes by sex and age.2
According to the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10), underlying cause of death is
"(a) the disease or injury which initiated the train of morbid events leading directly to death or (b) the circumstances of the accident or violence which produced the fatal injury”.
IDCD are those whose underlying cause is classified in Chapter XVIII of the ICD-10 and contain only the description of symptoms and signs of diseases. The occurrence of these deaths indicates problems in the access to health services and reflects the quality of medical assistance offered to the population.1)-(3
In Brazil, despite the improvement and consolidation of the Mortality Information System (SIM) since the 2000's, the high number of IDCD is still a concern.4 In 2003, these deaths corresponded to 13.3% of the country's total deaths, presenting a great variety among municipalities, states and macroregions, with proportions varying from 25.9% in the Northeast region to 6.7% in the South region.3),(4 In 2000, developed countries such as Hungary, New Zealand, Finland, Cuba and Romania already presented IDCD proportion of less than 1%,5 which highlights Brazil's high proportion of IDCD.
North and Northeast regions, which are responsible for the occurrence of most IDCDs, presented a sharp decrease in this proportion, resulting mostly from specific investment made by the Ministry of Health to improve essential information,6)-(7 especially in regulation of data collection, flow and regularity for providing information on deaths,8 discontinuation of automatic and regular transference of resources, in the case of problems in providing this information,9 besides the release of data, technical publications and human resources training, especially on codes of underlying cause of death.10 We can also highlight the promotion and distribution of a new instructions manual in the filling in of Death Certificates (DC) since 2011, aiming to raise the healthcare professional's awareness on the importance of this document.4),(11
Regarding the quality improvement of statistics on causes of death, the Ministry of Health established a proposal for investigation of IDCD, especially in the country's North and Northeast regions.6)-(7 In 2006, the National Network of Death Verification Service (SVO) was created, highlighting the need for implementing the SVO in every state capital and in the Federal District, which will total up to 74 services distributed among the 27 Federation Unities (UF).12 In 2008, a pilot project to introduce verbal autopsy (VA) as a method of investigation of IDCD home deaths was initiated, using World Health Organization's (WHO) standard forms for VA adapted to the most prevailing causes in Brazil. Supposedly, the VA analysis allows the physician to identify the sequence of events which led to death.2),(13),(14 Good results were described regarding the decrease of IDCD in the North and Northeast regions with the implementation of the program 'Percentage Reduction of Ill-Defined Causes of Death'.4),(15
Considering the importance of IDCD and its investigation, together with the availability of mortality data from the national health information systems, the aim of this study was to describe the results of the investigation of ill-defined causes of death (IDCD) to improve the quality of cause-of-death data in Brazil.
Methods
This is a descriptive study about ill-defined causes of death and its investigation in Brazilian states, state capitals and macroregions.
In 2010, the country had a total population of approximately 200 million people, in the 26 states and the Federal District (DF), living in 5,540 municipalities distributed among five macroregions: North, Northeast, Midwest, Southeast and South. In economy, as well as in the population characteristics, there are significant differences among regions and states.16
We used data from SIM, available at the website of the IT Department of the Brazilian National Health System (Datasus): www.datasus.gov.br.
We selected all deaths occurred in 2010 whose underlying cause of death was covered in Chapter XVIII of ICD-10 (categories: R00 to R99). The place of residence was considered here in order to stratify deaths by macroregions, UF and capitals.
In SIM's database, investigated IDCDs are informed in a variable field named 'TTPOS', and the underlying causes of death are presented in two ways: the original (variable field 'CAUSABAS_O'), referring to the underlying cause registered at the time of death, in the field 40/Bloco V of the original DC; and the final underlying cause (variable field 'CAUSABAS'), referring to the cause determined after investigating the death. In case there is no investigation or it does not enable the clarification of the underlying cause, the original underlying cause will be the same as the final. In case there is a substitution of IDCD for an underlying cause not covered in Chapter XVIII of the ICD-10, that will be the final cause, and these deaths will be presented as reclassified.4
With regard to the database variables 'Place of Death Occurrence' (variable field "LOCOCOR") and 'Death Attested by a physician' (variable field " ATESTANTE "), these data come from the field 20/Bloco III and field 43/Bloco VI of the DC, respectively. The first variable refers to the place where the death occurred, and the second refers to the condition of the attesting physician - responsible for confirming the death and filling in the DC.11
The following variables were analyzed: original IDCD (all deaths whose original underlying cause belonged to chapter XVIII of ICD-10); deaths investigated as IDCD (all deaths with original IDCD and declared as investigated at SIM the following way: yes, no, or blank); reclassified IDCD (deaths with original IDCD that had the underlying cause reclassified); investigated deaths with reclassification (deaths with original IDCD investigated that had the underlying cause reclassified); final IDCD (deaths investigated or not, which remained IDCD, that is, they had a final underlying cause included in chapter XVIII of ICD-10, presented in the format of code for cause of death with one letter and up to three digits); place of occurrence of investigated deaths (hospital and other health facilities, household, public road/other places or ignored); person responsible for attesting (signee) the underlying cause of deaths investigated (assistant physician, substitute physician, SVO physician, physician from the Institute of Forensic Medicine (IFM), other or ignored).
According to procedures standardized by the Ministry of Health,13 the investigations of IDCD, that is, the search for information about the terminal disease for clarification of the underlying cause of death can be performed at primary health care units (PHU), clinics and hospitals, at committees for prevention of infant or maternal death, or comparing with other databases. Information on the underlying cause of death can also be collected on the SVO, responsible for clarifying the causes of death by natural cause without diagnosis, and at the IFM, legally responsible for clarifying deaths by external causes. Deaths in which the information obtained in the investigation sources aforementioned do not allow for the clarification of the cause of death, must be investigated through household interviews, using the verbal autopsy (VA) form.
The following indexes were calculated: (i) IDCD percentage, in relation to the total of deaths; (ii) percentage of investigated IDCD, in relation to the total of deaths due to these causes; (iii) percentage of IDCD that were reclassified to defined cause after investigation, in relation to the total of IDCD; (iv) percentage of IDCD that were reclassified to defined cause after investigation, in relation to the total of investigated deaths; (v) percentage of deaths that remained IDCD after investigation (remaining IDCD), in relation to the total of deaths; and (vi) variation of IDCD in relation to the total of deaths, calculated as the difference between the number of deaths observed by original IDCD and the number of deaths by remaining IDCD, divided by the total number of deaths. The variation of IDCD will be considered negative when, after investigation of defined cause deaths, there was reclassification to chapter XVIII, i.e., there was an increase in the percentage of ill-defined causes. If the variation is considered positive, it mean that there was a decrease in the percentage of ill-defined causes.
Data were processed with the software Tabwin version 3.2 and Microsoft Office Excel 2013 (Microsoft Corporation, United State of America) to produce the spreadsheets.
The study project was developed according to the Resolution of the National Health Council (CNS) No. 466, dated December 12th, 2012. The study was dismissed from appreciation by an ethics in research committee, for being based exclusively on secondary data from SIM, of public domain, without nominal identification.
Results
In 2010, 1,136,947 deaths in the country were notified to SIM, 8.6% of them being originally attributed to an IDCD. This percentage ranged from 5.7% in the South region to 13.5% in the North region. Among the Federation Units (UF), the percentage of IDCD ranged from 1.5% in the Federal District (DF) to 19.9% in the state of Acre. In the South region, all states presented a similar percentage of approximately 5.7%. However, in the North region, most states presented a percentage of IDCD higher than 10%, except from Tocantins and Roraima. The low percentage of IDCD in the states of Roraima (4.0%), Rio Grande do Norte (3.3%), Espírito Santo (2.8%) and Mato Grosso do Sul (2.1%), and in DF (1.5%) stands out in this study (Table 1).
Table 1 - Total of deaths and original, investigated and reclassified ill-defined causes of death, according to, macroregions and Federation Units (UF), Brazil, 2010
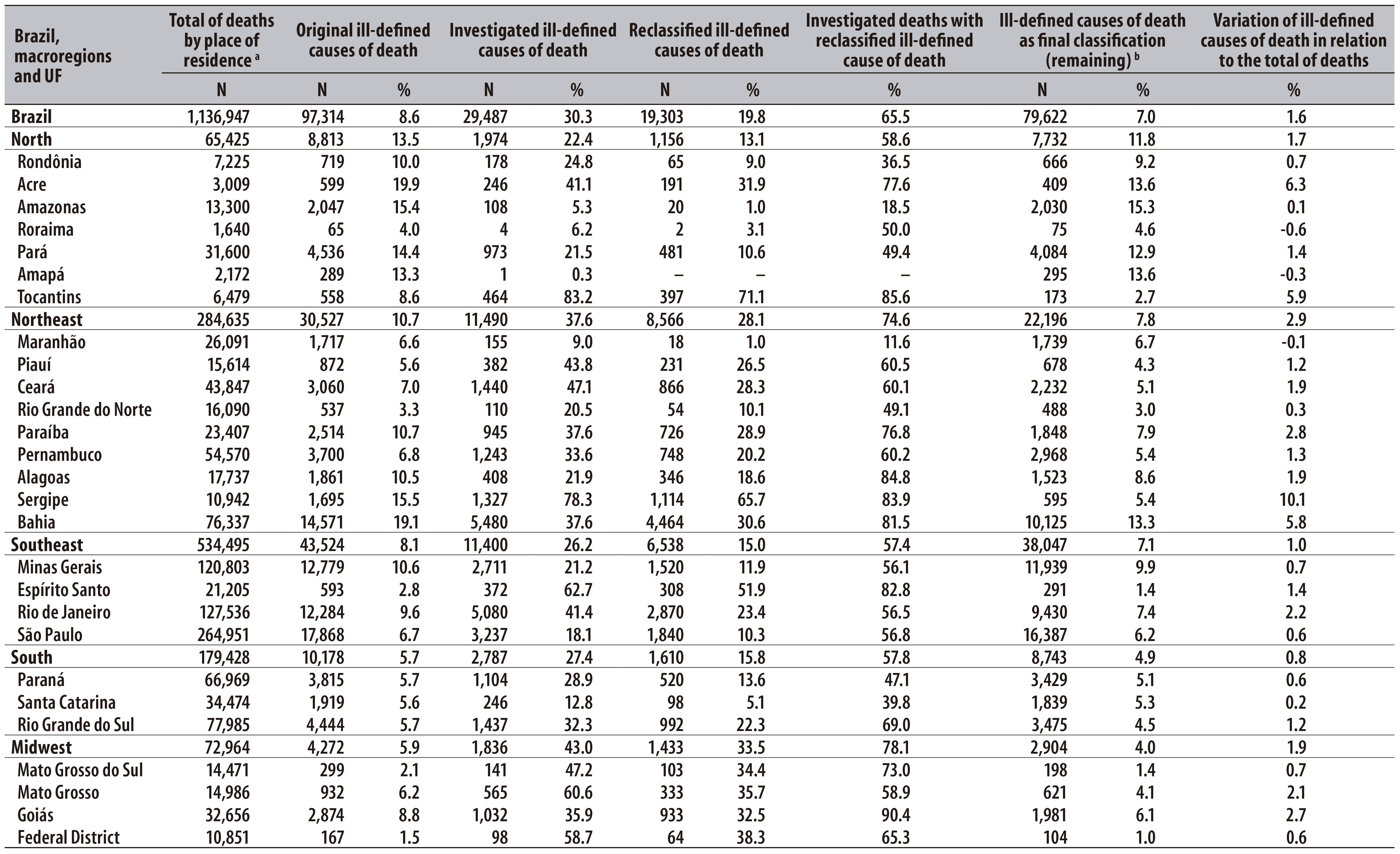
a) Includes ill-defined causes of death
b) Some deaths were classified as ill-defined causes after investigation of defined causes
Among deaths by IDCD, 30.3% were registered at SIM as investigated, ranging from 22.4% in the North region to 43.0% in the Midwest region. The states that investigated the highest percentage of IDCD were Tocantins (83.2%), Sergipe (78.3%) and Espírito Santo (62.7%), whereas Amapá (0.3%), Amazonas (5.3%) and Roraima (6.2%) presented the lowest percentage of investigation (Table 1).
After the investigations were carried out, 19.8% of IDCD had the underlying cause of death reclassified. In 14 Federation Units, the percentage of investigated deaths with reclassification of IDCD was of at least 60%, reaching 85.6% in Tocantins and 82.8% in Espírito Santo. However, in the states of Amazonas, Amapá, and Maranhão, besides the low percentage of investigations, the percentage of reclassification among investigated deaths was lower than 20%. In turn, we observed a significant decrease in the percentage of original IDCD in relation to the total of deaths in Acre (6.3%), Tocantins (5.9%), Sergipe (10.1%) and Bahia (5.8%).
In the state capitals, 278,952 deaths were notified to SIM, of which 4.7% were by IDCD, ranging from 2.1% in South region capitals to 9.4% in North region capitals. The lowest percentage was found in Teresina-PI (0.6%) and the highest in Rio Branco-AC (17.9%), and only three capitals of the North region presented percentage of IDCD higher than 10% (Table 2).
Table 2 - Total of deaths and original, investigated and reclassified ill-defined causes of death, according to capitals of Federation Units (UF), Brazil, 2010
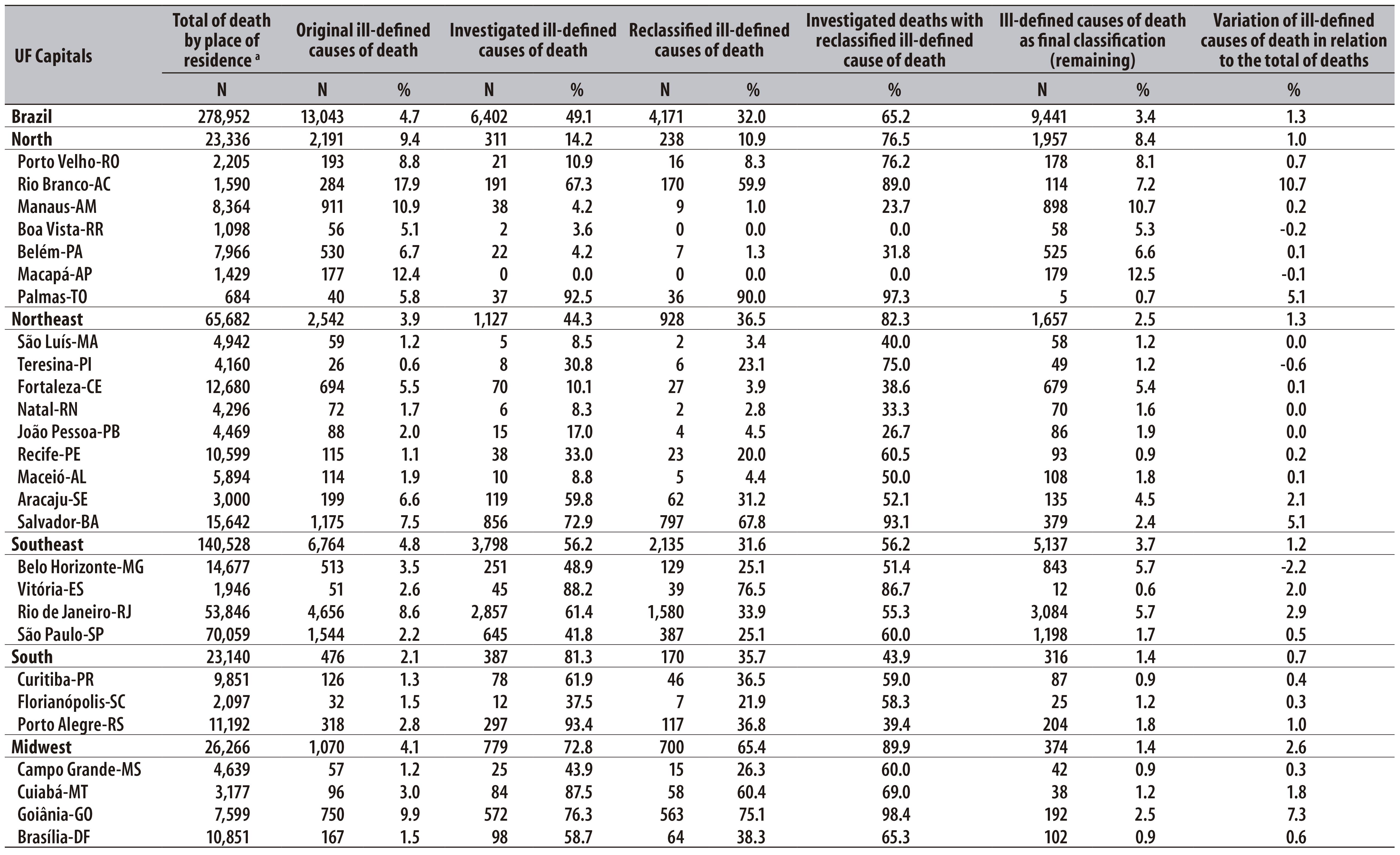
a) Includes ill-defined causes of death
b) Some deaths were classified as ill-defined causes after investigation of defined causes
In general, the percentage of investigated deaths was higher in the state capitals than in the states. For the total of state capitals, the percentage of investigation was of almost 50%, ranging from 81.3% in the South region to 14.2% in the North region. In Palmas-TO, more than 90% of IDCD were investigated. The percentage of reclassification was of 32.0% in the total of capitals. Palmas-TO, Rio Branco-AC, Goiânia-GO and Salvador-BA were the capitals that presented the highest percentage of reclassification and reduction of IDCD in relation to the total number of deaths. In turn, some capitals in North and Northeast regions had the lowest percentage of reclassification (Table 2).
Figure 1 presents indexes related to IDCD in the Federation Units (UF) and capitals, grouped according to macroregions, and to the country as a whole. There was a lower percentage of original IDCD in the capitals when compared to the UF, especially in states from the South and Northeast regions (Figure 1 A). In turn, we observed a higher percentage of investigation in capitals of the South and Midwest regions (Figure 1 B). The North region stood out with the highest percentage of IDCD and the lowest percentage of investigations. With regard to the investigated IDCD, the Midwest region had the highest percentage, followed by the Northeast region (Figure 1 C). This percentage presented important differences between states and capitals only in the South region (Figure 1 D). The percentage of remaining IDCD after investigation was lower than 10% in almost every region, except for the North region (Figure 1 E). The highest percentage decrease of IDCD in relation to the total of deaths was observed in the Midwest region, UF and capital, and in the UF of North and Northeast regions (Figure 1 F).
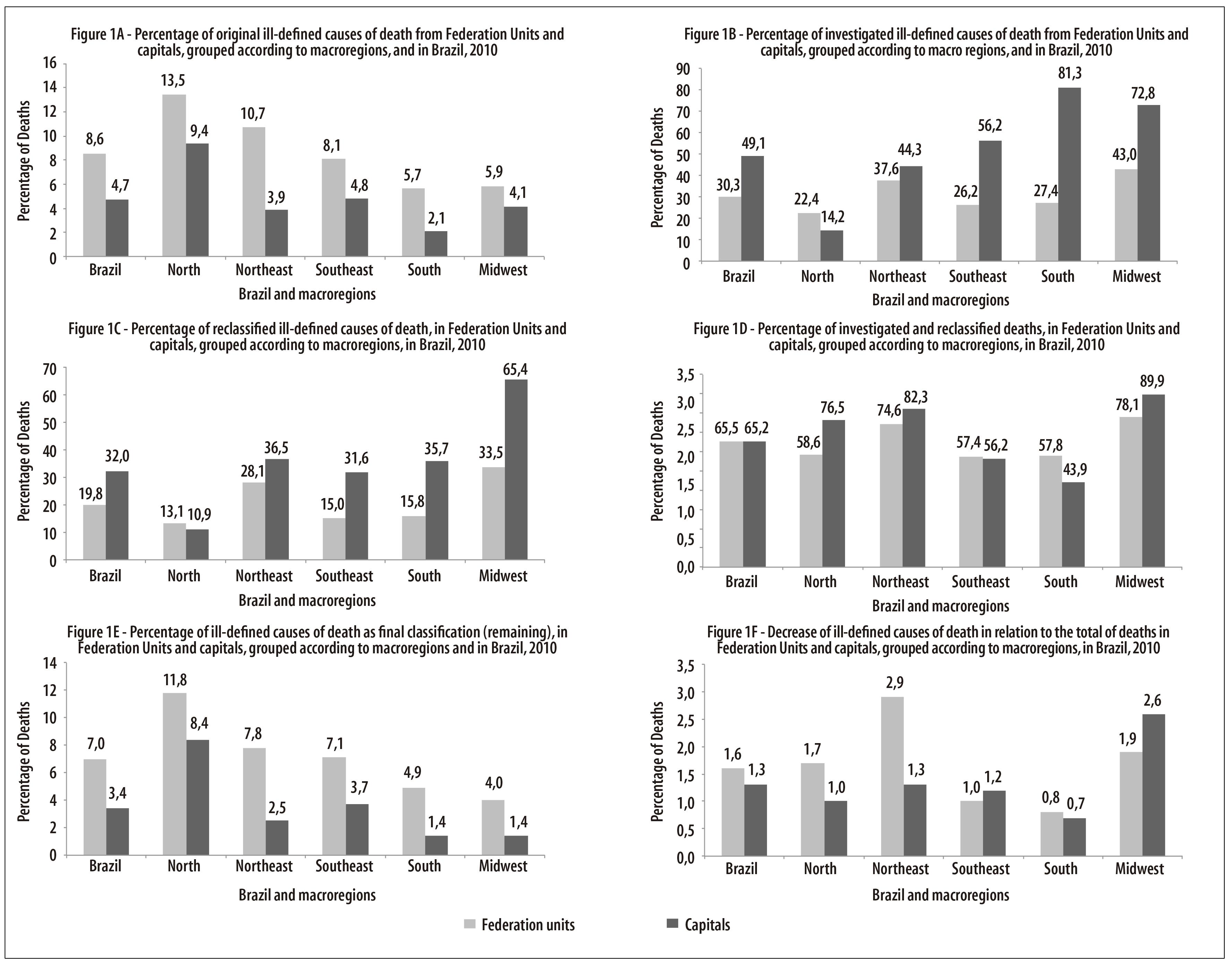
Figure 1 - Indicators related to original, investigated and reclassified ill-defined causes of death, in Federation Units and capitals, grouped according to macroregions, and in Brazil, 2010
We observed that, from the total of investigated deaths, more than 50% occurred in households, with a highest percentage in the North (67.4%)and Northeast (74.5%) regions. In turn, in the states of Rio de Janeiro (82.7%) and Goiás (67,9%), and the Federal District (77.6%), most investigated IDCD occurred in hospitals. The percentage of investigated deaths which occurred in public ways/other places was of 8% in the country, and equal or lower than 10% in the macroregions (Table 3). It is important to highlight that in the North and Northeast regions approximately 70% of IDCD occurred in households, whereas in the Southeast and Midwest regions, this percentage was 45%, and in the South region, it was approximately 60% (data not presented).
Table 3 - Place of occurrence of the investigated ill-defined causes of death according to macroregions and Federation Units (UF), Brazil, 2010
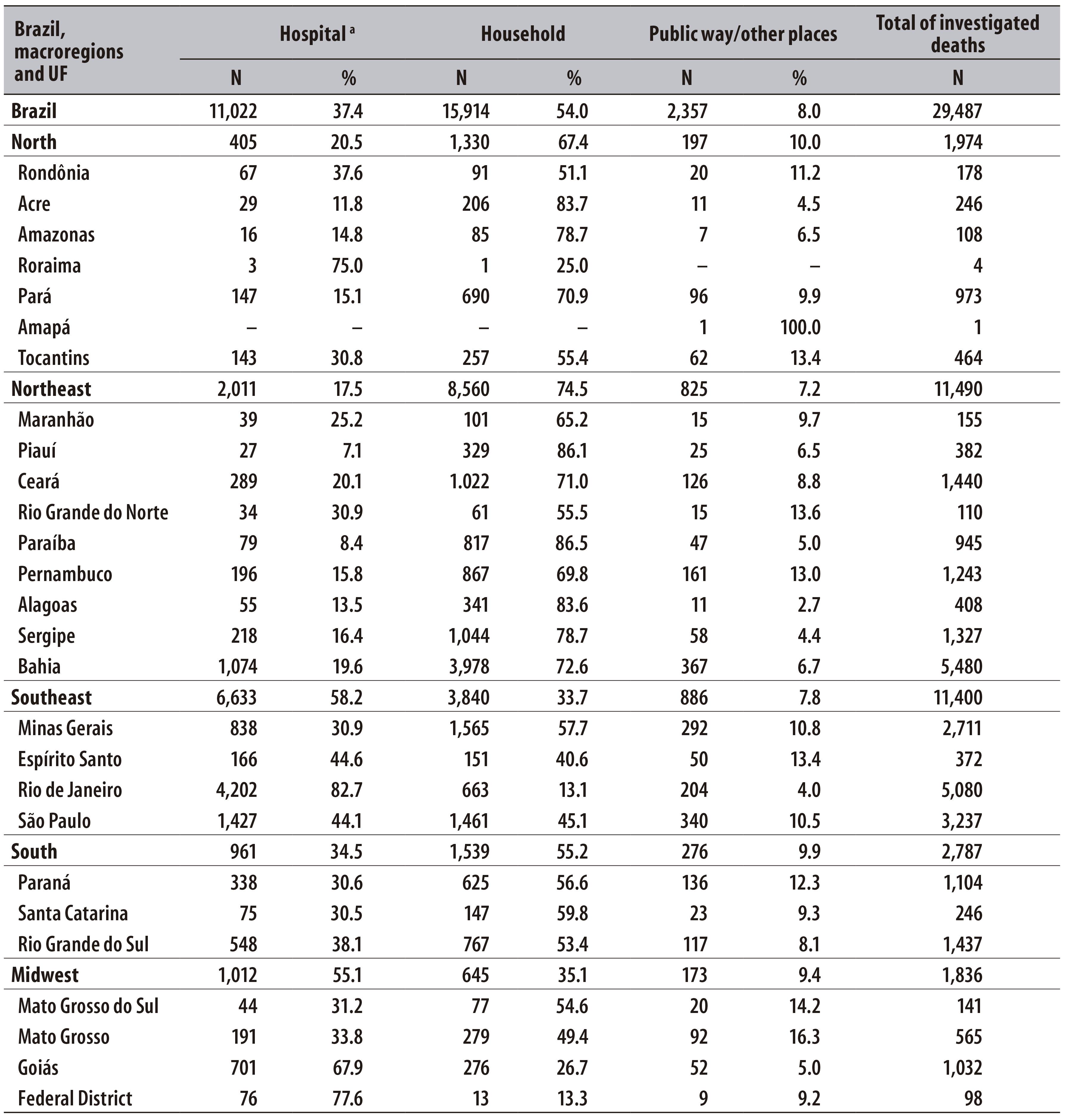
a) Refers to the sum of the categories 'hospital' and 'health facilities’
Note: Deaths which the place of occurrence was registered in the Death Certificate as ignored were not significant. For Brazil, they summed up 0.7% of the total, ranging from 0.3% to 0.8% among the macroregions.
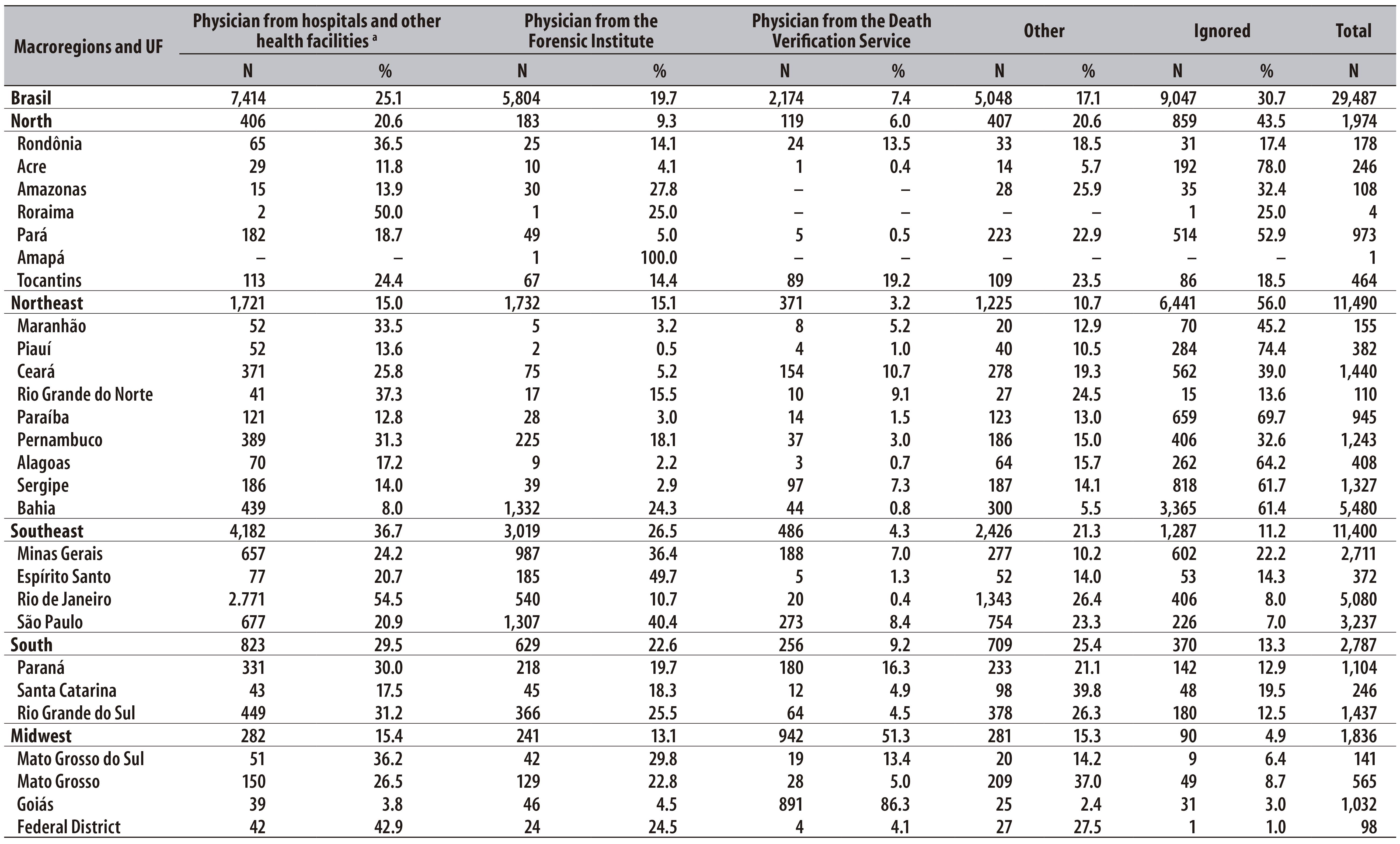
Physicians from hospitals and other health facilities were responsible for attesting 25.1% of the investigated IDCD; in the Federal District, specifically, this percentage was 42.9%. In the country, physicians from the Forensic Institute attested 19.7% of the investigated IDCD, being 26.5% in the Southeast region, and reaching 49.7% in the state of Espírito Santo. The services of death verification - SVO - were responsible for attesting 7.4% of the investigated IDCD in the country, with the highest percentage in the Midwest region (51.3%), especially in the state of Goiás (86.3%). However, about a third of the investigated deaths (30.7%) did not inform the death signee, especially the Northeast region, where more than half of deaths (56.0%) did not mention this information (Table 4).
Discussion
In this study, we observed an improvement in the quality cause-of-death data registered at SIM due to investigative activities, with a decrease in the percentage of IDCD in country's states and state capitals. After investigation, the percentage of reclassification was approximately 65% for states and capitals, which resulted in a 20% decrease of IDCD in official statistics. However, regional differences remained: North and Northeast regions still presented a percentage of IDCD above the target established by the Ministry of Health - which must be inferior to 10% of the total of notified deaths.13),(17
An analytic study of IDCD spatial pattern in Brazil and its relation with death register, when comparing 1980-1991 and 2000-2010 periods, concluded that there has been an improvement in mortality data in Brazil, with a decrease of 53% in IDCD from the total of the country; in the North and Northeast regions, the percentage of IDCD decreased from 72% in 1991 to about 25% in 2010.18 This reduction was a result of several initiatives of the Ministry of Health, whose efforts were concentrated in these regions’ states.18),(19) However, more investments are necessary in states such as Amazonas and Acre, in the North region, and Bahia, in the Northeast region, for they still presented, in 2010, percentages of IDCD above 15% before investigations and above 10% after investigations, which may imply issues on access to health services. The study aforementioned also revealed that a rise of 1% in death coverage corresponds to a decrease of 0.24% of IDCD, showing the need to improve register in order to create more trustworthy data related to the number of IDCD in the states.18 For instance, the low percentage of original IDCD in states such as Tocantins, Roraima, Rio Grande do Norte, Espírito Santo and Mato Grosso do Sul, observed in this paper, points to potential issues of under-registration of deaths, mainly in the North and Northeast regions, where the coverage of deaths in states is 85.4% and 88.9%, respectively.20
In this study, a lower percentage of IDCD was expected to have been found in the state capitals. Nevertheless, we found a percentage of original IDCD higher than 10% in three capitals in the North region, whereas in Rio de Janeiro-RJ and in Goiânia-GO, these numbers were close to 10%. These findings are worrisome, because the capitals are expected to have a better quality of assistance and information on death causes and, consequently, a decrease of IDCD.21 In Rio de Janeiro-RJ, a study on the evolution of registers of deaths due to violence, based on the period from 2000 to 2009, showed that the rise in undetermined causes corresponded mostly to unrecognized homicides, which brought to light issues on the quality of data.22
Moreover, in this study, we observed that, in the state capitals, the percentage of investigations conducted was higher than in the states as a whole. However, it was exactly outside of the capitals where there were the highest percentages of IDCD and, therefore, a greater need for investigation.
The result of investigations can be verified when analyzing the percentage of investigated deaths which were reclassified in their underlying cause: higher than 80% of deaths in five states and higher than 50% in fifteen states. Studies showed that the use of the verbal autopsy form for investigating IDCD enabled the clarification of underlying cause in approximately 80% of the investigated deaths.2),(23 The investigation of IDCD with subsequent reclassification of underlying cause in states of the North and Northeast regions, with a significant decrease in the percentage of IDCD, reassures the importance of these investigations.13 However, in some states from the North region, such as Roraima and Amapá, there was an unexpected rise in this percentage, which suggests the existence of issues on the quality of data registered at SIM.
With regard to the place of occurrence of death, there was a higher percentage of investigated IDCD that occurred in households (54%); in the North and Northeast regions, this information was compatible with the high occurrence of household IDCD in these regions. On the other hand, the fact that more than 50% of investigated IDCD in the Southeast and Midwest regions have occurred in hospitals or health establishments is worrisome. In these places, patients are expected to have access to medical care and, therefore, have a lower percentage of IDCD in death certificates. These data can indicate issues on stating the cause of death in these institutions.
Studies conducted in Brazilian municipalities showed that the IDCD certificate could be avoided in many deaths if physicians sought complementary information in medical records, indicating that available information was not completely used to clarify the death causes.3),(24 Therefore, it is extremely important for the physician to raise awareness on the relevance of the death certificate, through actions of continued training which allow a complete and correct filling in of the document, in a way that these professionals are able to specify in the DC the conditions and causes that led to death, placing the underlying cause and its complications in the correct fields.3),(11
A possible explanation for the high percentage of IDCD attested in the IFM and SVO can be found in flowcharts and procedures to issue the DC and notification of underlying cause in these services. In some places, it is possible that the issuing of the DC and the underlying cause were determined through necropsy exams. Therefore, the underlying cause of death registered in the DC will be the IDCD. Later, when the underlying cause is clarified after results of examination, this new underlying cause should be uploaded at SIM as the result of investigation, and then the underlying cause will be changed in the system, which may not happen every time. This way, it is essential that the health departments search for results of necropsies for improving data on causes of death. These findings reinforce the importance of establishing flows and procedures related to information on deaths declared by these services.
The fact that roughly one third of investigated deaths did not have the information regarding the section signee filled in in the DC and, consequently, not informed at SIM, shows one more possible contribution of IDCD investigation. If there was death investigation and a later reclassification of the underlying cause by a physician, it is important that the new signee is registered in the system, as it is already done for the underlying cause of death.
Possible limitations of this study refer to the fact that it is based on SIM's data and, therefore, it depends on the quality of DC filling in and death coverage, matters that present significant regional differences. The quality of investigations and the validity of reclassified causes were not evaluated, besides being possible that some investigations that were really carried out have not been reported to SIM. Also, we should consider that the criteria of considering a case as investigated is not standardized among the Brazilian states.
All in all, the findings of this study indicate that IDCD investigations contributed to improve data on death causes in Brazilian states and capitals in 2010. Investigations of these deaths must be conducted and stimulated by the health managers, until the Mortality Information System - SIM - reaches satisfactory levels of data quality on death causes, resulting from a complete and correct filling in of the Death Certificate, enabling actions from health services to be in harmony with the population’s needs, at every level. A gradual decrease in the need for investigation is expected as the population gains more access to adequate and quality medical care.
integrity.
Referências
1. Teixeira CLS, Klein CH, Bloch KV, Coeli CM. Reclassificação dos grupos de causas prováveis dos óbitos de causa mal definida, com base nas Autorizações de Internação Hospitalar no Sistema Único de Saúde, Estado do Rio de Janeiro, Brasil. Cad Saude Publica. 2006 jun;22(6):1315-24. [ Links ]
2. Campos D, França E, Loschi RH, Souza MFM. Uso da autópsia verbal na investigação de óbitos com causa mal definida em Minas Gerais, Brasil. Cad Saude Publica. 2010 jun; 26(6):1221-33. [ Links ]
3. Jorge MHPM, Laurenti R, Gotlieb SLD. O Sistema de Informações sobre Mortalidade - SIM: concepção, implantação e avaliação. In.: Ministério da Saúde; Organização Pan-Americana de Saúde; Fundação Oswaldo Cruz. A experiência brasileira em sistemas de informação em saúde. Brasília: Ministério da Saúde; 2009. (Série B. Textos Básicos de Saúde). v. 1. p. 71-107. [ Links ]
4. França E, Teixeira R, Ishitani L, Duncan BB, Cortez-Escalante JJ, Morais Neto OL, et al. Ill-defined causes of death in Brazil: a redistribution method based on the investigation of such causes. Rev Saude Publica. 2014 Aug; 48(4):671-81. [ Links ]
5. Mathers CD, Vos T, Lopez AD, Salomon J, Ezzati M, editors. National burden of disease studies: a practical guide. Geneva: World Health Organization; 2001. [cited 2016 Aug 04 ]. Avaliable from: Avaliable from: http://www.who.int/healthinfo/nationalburdenofdiseasemanual.pdf [ Links ]
6. Ministério da Saúde (BR). Sistemas de Informações sobre Mortalidade (SIM) e Nascidos Vivos (SINASC) para os profissionais do Programa de Saúde da Família. 2. ed. rev. atual. Brasília: Ministério da Saúde ; 2004. (Série F. Comunicação e Educação em Saúde). [ Links ]
7. Ministério da Saúde (BR). Monitoramento da acurácia dos sistemas de informações sobre mortalidade e nascidos vivos. In: Anais da 3ª Expoepi: Mostra Nacional de Experiências Bem-sucedidas em Epidemiologia, Prevenção e Controle de Doenças [Internet]; 2003 nov 18-21; Salvador. Brasília: Ministério da Saúde, 2004 [citado 2016 ago 04]. 216 p. (Série D. Reuniões e Conferências). 2004. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/anais_3expoepi.pdf [ Links ]
8. Brasil. Ministério da Saúde. Portaria nº 116, de 11 de fevereiro de 2009. Regulamenta a coleta de dados, fluxo e periodicidade de envio das informações sobre óbitos e nascidos vivos para os Sistemas de Informações em Saúde sob gestão da Secretaria de Vigilância em Saúde. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2009 fev 12;Seção 1:37. [ Links ]
9. Brasil. Ministério da Saúde. Portaria nº 3252, de 22 de dezembro de 2009. Aprova as diretrizes para execução e financiamento das ações de Vigilância em Saúde pela União, Estados, Distrito Federal e Municípios e dá outras providências. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2009 dez 23;Seção 1:65. [ Links ]
10. Frias PG, Pereira PMH, Andrade CLT, Lira PIC, Szwarcwald CL. Avaliação da adequação das informações de mortalidade e nascidos vivos no Estado de Pernambuco, Brasil. Cad Saude Publica. 2010 abr;26(4):671-81. [ Links ]
11. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Manual de instruções para o preenchimento da declaração de óbito. Brasília: Ministério da Saúde; 2011.(Série A. Normas e Manuais Técnicos). [ Links ]
12. Brasil. Ministério da Saúde. Portaria nº 1.405 de 29 de junho de 2006. Institui a Rede Nacional de Serviços de Verificação de Óbito e Esclarecimento da Causa Mortis (SVO). Diário Oficial da República Federativa do Brasil , Brasília (DF), 2006 jun 30;Seção 1:242. [ Links ]
13. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Manual para investigação do óbito com causa mal definida. Brasília: Ministério da Saúde; 2009. 48 p. (Série A. Normas e Manuais Técnicos). [ Links ]
14. World Health Organization. Verbal autopsy standards: ascertaining and attributing cause of death. Geneva: World Health Organization; 2007 [cited 2016 Aug 4]. Available from: Available from: http://apps.who.int/iris/bitstream/10665/43764/1/9789241547215_eng.pdf [ Links ]
15. Souza MFM, Barea V, Williams D. Improving the mortality information in poor areas: the Brazilian experience. Proceedings of the WHO Family of International Classifications - WHO-FIC; 2007 Oct 28- Nov 3; Trieste, Italy. [ Links ]
16. Instituto Brasileiro de Geografia e Estatística. Censo demográfico 2010 [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2011 [citado 2016 ago 04]. Disponível em: Disponível em: http://www.ibge.gov.br/home/estatistica/populacao/censo2010/default.shtm [ Links ]
17. Ministério da Saúde (BR). Secretaria de Gestão Estratégica e Participativa. Departamento de Articulação Interfederativa. Caderno de diretrizes, objetivos, metas e indicadores: 2013 - 2015. 2. ed. 156 p.: il. - (Série Articulação Interfederativa; v. 1) [ Links ]
18. Lima EEC, Queiroz BL. Evolution of the deaths registry system in Brazil: associations with changes in the mortality profile, under-registration of death counts, and ill-defined causes of death. Cad Saude Publica. 2014 ago;30(8):1721-30. [ Links ]
19. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Saúde Brasil 2011: uma análise da situação de saúde e a vigilância da saúde da mulher. Brasília: Ministério da Saúde; 2012. 444 p.: il. [ Links ]
20. Szwarcwald CL, Frias PG, Souza Júnior PRB, Almeida WS, Morais Neto OL. Correction of vital statistics based on a proactive search of deaths and live births: evidence from a study of the North and Northeast regions of Brazil. Population Health Metrics. 2014 Jun;12:16. [ Links ]
21. Abreu DMX, Sakurai E, Campos LN. A evolução da mortalidade por causas mal definidas na população idosa em quatro capitais brasileiras, 1996-2007. Rev Bras Estud Popul. 2010 jan-jun;27(1):75-88. [ Links ]
22. Cerqueira D. Mortes violentas não esclarecidas e impunidade no Rio de Janeiro. Econ Apl. 2012 abr-jun;16(2):201-35. [ Links ]
23. França EB, Cunha CC, Vasconcelos AMN, Escalante JJC, Abreu DX, Lima RB, et al. Avaliação da implantação do programa "Redução do percentual de óbitos por causas mal definidas" em um estado do Nordeste do Brasil. Rev Bras Epidemiol. 2014 jan-mar;17(1):119-34. [ Links ]
24. Jorge MHPM, Gotlieb SLD, Laurenti R. O sistema de informações sobre mortalidade: problemas e propostas para o seu enfrentamento I: mortes por causas naturais. Rev Bras Epidemiol. 2002 ago;5(2):197-211. [ Links ]
Received: July 13, 2015; Accepted: July 10, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
