










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.1 Brasília ene./mar. 2017
http://dx.doi.org/10.5123/s1679-49742017000100018
RESEARCH NOTE
Hospitalizations of Brazilian children under fiver years old: a systematic review
1Universidade Estadual da Paraíba, Programa de Pós-Graduação em Saúde Pública, Campina Grande-PB, Brasil
2Universidade Estadual da Paraíba, Mestranda do Programa de Pós-Graduação em Saúde Pública, Campina Grande-PB, Brasil
Methods:
this is a systematic review of articles published from 2008 to 2015, searched in the databases Medline and LILACS; selected studies were critically analyzed through a validated instrument.
Results:
eleven articles were included, four of them are ecological and seven are cross-sectional studies; respiratory diseases (n=5), parasitic infections (n=4) and perinatal diseases (n=2) were the main causes for hospitalizations in the reviwed articles; in the studies that analyzed the sensitive conditions, pneumonia (n=6), gastroenteritis (n=5), and asthma (n=5) were the mais causes pointed out.
Conclusion:
respiratory, parasitic and perinatal diseases revealed to be the main causes for hospitalizations in Brazilian children; pneumonia, gastroenteritis, and asthma constitute the most important of hospitalizations, treatable in the ambulatory health care.
Key words: Children’s Health Care; Hospitalization; Ambulatory Health Care; Literature Review as Topic
Introduction
The importance of Primary Healthcare (PHC) in the healthcare system implies the need of continuous evaluations of its performance.1 In order to accomplish this purpose, mortality and morbidity indicators may be employed, such as the list of hospitalizations for Ambulatory Care Sensitive Conditions (ACSC), which takes into consideration health problems for which the PHC can decrease the risk of hospitalization.1,3 This indicator was proposed to evaluate the PHC, and it considers that the rates of hospitalization can highlight the conditions of access to and the operation of health services.2,4
The term ACSC-related hospitalization originated in the United States of America in the 1990s. Later, other countries also have shown concern in evaluating the quality of ambulatory health care based on avoidable hospitalizations.5,6
In Brazil, considering the need for establishing a list that reflects the diversity of health conditions, and of illness in the national territory, in 2008, it was published the official list of ACSC-related hospitalization7. This list was built based on the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10).8 The Brazilian list contains 19 groups of causes of hospitalization, and diagnostics which gather preventable diseases by immunizations. It also gathers infectious and chronicles diseases. Its objective is to contribute to the evaluation of the health system performance and of the PHC impact on the health conditions of the population.7,9
Considering the health care provided to the population in general, children’s health care represents a priority field, due to their susceptibility to illness and worsening of illnesses as a consequence of their fragility proper of their age.10,11 In child population, unlike adults population, there is a predominance of acute illnesses, which compound part of the Brazilian list of ACSC-related hospitalization.7,9 Therefore, these pathologies are avoidable with the timely assistance of the PHC services. Especially the perinatal diseases - and the fact they could be avoided - makes them responsible for a large portion of the hospitalizations of children under a year and the main cause of infant death in Brazil.12,13 This literature review pointed out high rates of ACSC-related hospitalization in Brazilian children, although studies on the subject are still incipient.14
The research was conducted with the purpose of obtaining answers to the following question: what is known about the causes of hospitalization (general causes and Ambulatory Care Sensitive Conditions) of Brazilian children under five years old? This article proposes the following hypothesis: the leading causes of hospitalizations amongst Brazilian children under the age of five are respiratory diseases and perinatal, not sensitive to ambulatory health care. Thus, the present study aimed to describe the causes of Brazilian children's hospitalizations under five years old reported in the literature.
Methods
The study is a systematic review of scientific articles concerning the causes of general admissions, and of ACSC-related hospitalization in children under five years old in Brazil. The article fulfilled the PRISMA recommendation for reporting systematic reviews and meta-analyses.15 Two reviewers worked independently. The definition of conditions considered sensitive to ambulatory health care was based on the official list of the Ministry of Health.7
Eligibility criteria
We considered eligible the studies about hospitalizations published between 2008 and 2015. The choice of this period is justified because it the publication of the list of ACSC-related hospitalization occurred in 2008.7 Publications in English, Spanish and Portuguese were considered; scientific documents published in the format of original articles and studies with Brazilian populations which included in theirs analyses children under five years were considered likewise.
Sources of information
The studies were identified in the databases Medline (National Library of Medicine, Bethesda, MD) and LILACS (Latin American and Caribbean Center on Health Sciences Information - Bireme). The search was held on January, 11th 2016.
Search strategy
All the documents containing the combination of descriptors Hospitalization AND Ambulatory Health Care AND Child Health were considered. In Medline, the search added the descriptor Brazil. For the calculation of the total amount of studies identified, it was verified if any duplication of these studies between the two databases occurred. Each article was counted only once.
Selection of Studies
We screened the studies by reading the titles and abstracts. This process eliminated (i) publications in languages other than English, Spanish or Portuguese, (ii) monographs, dissertations and theses, (iii) review articles, (iv) studies conducted concerning other countries other than Brazil and (v) publications that did not include in its analysis children under the age of five. After the screening process, of inclusion and exclusion were applied, which involved reading the full text, and a careful analysis of it.
In order to include publications in this review, studies that addressed the theme of hospitalizations in children under five years old were taken into account. Studies that favored different age groups have been included since there was a categorization for children under five years, thus allowing to identify the profile of hospitalizations for the age group of interest. Studies that presented the following characteristics were excluded: (i) analyzed a group of specific causes (such as asthma and respiratory infection), without conforming an aggregate of different types of causes, (ii) analyzed institutionalized patients (childcare, for example), (iii) analyzed only the admissions in specific hospital units (intensive care unit), (iv) their analyses were solely on economic evaluation, (v) their analyses were solely on the effect of the improvement in access to PHC on hospitalizations for sensitive conditions without quoting the causes, and (vi) dealt with the impact of programs or techniques, independent of the PHC, on the sensitive conditions related hospitalization.
The references lists of the included articles were analyzed in order to identify other possible studies of interest. The selected articles, through the consultation of bibliographical references, underwent the same eligibility criteria, previously described. However, this procedure did not result in the addition of articles for the systematic review.
Data extraction
To ensure accuracy and reliability to the results of the review, the articles identified in the databases were grouped in folders that responded to the selection criteria. The discrepancies of rank between the two reviewers were resolved by consensus.
The selected information in the articles for their characterization was the following: author and year of publication, place, design, age group, type of data used in the analysis, method of definition of the sensitive disorders, hospitalizations of analysis (general and/or primary care sensitive conditions), performance indicators used in the analysis and main results. In case of studies that considered several age groups, only the results pertaining to children under the age of five were included.
Evaluation of the quality of the included articles
The quality of studies was assessed by one of the reviewers using the instrument of critical evaluation for studies of prevalence developed and tested by Munn et al.16 This instrument consists of ten questions about the adequacy and accuracy of the study in relation to the validity of the methods, interpretation and applicability of the results. Each item was evaluated with one point when the answer was positive or 'not applicable', half a point when the answer was uncertain, and zero when the answer was negative, generating a maximum score of 10 points. The score of each article was used for their classification into three categories: high quality (8 to 10 points), medium (5 to 7 points) and low (0 to 4 points).
Data analysis
The articles were grouped according to the hospitalizations of analysis (general and/or primary care-sensitive conditions). For each category, the causes of hospitalizations listed by the authors were described, considering the first up to the sixth cause. In the case of studies in which researchers discriminated age groups, these categories were respected. In these cases, the data on ambulatory care sensitive conditions were analyzed for children under one year, from 1 up to 4 years old and/or under the age of 5 years old. The results were synthesized considering the leading causes for hospitalizations and ACSC-related hospitalization.
Results
The flowchart which presents the process of identification and selection of the studies can be found in Figure 1. Eleven articles were included,1,2,3,11,12,17-22, four of them ecological2,12,17,22, and seven cross-sectionals.1,3,11,18-21. All the included articles were systematized, because only one of them presented an evaluation of the average quality and none of them was classified as low quality.
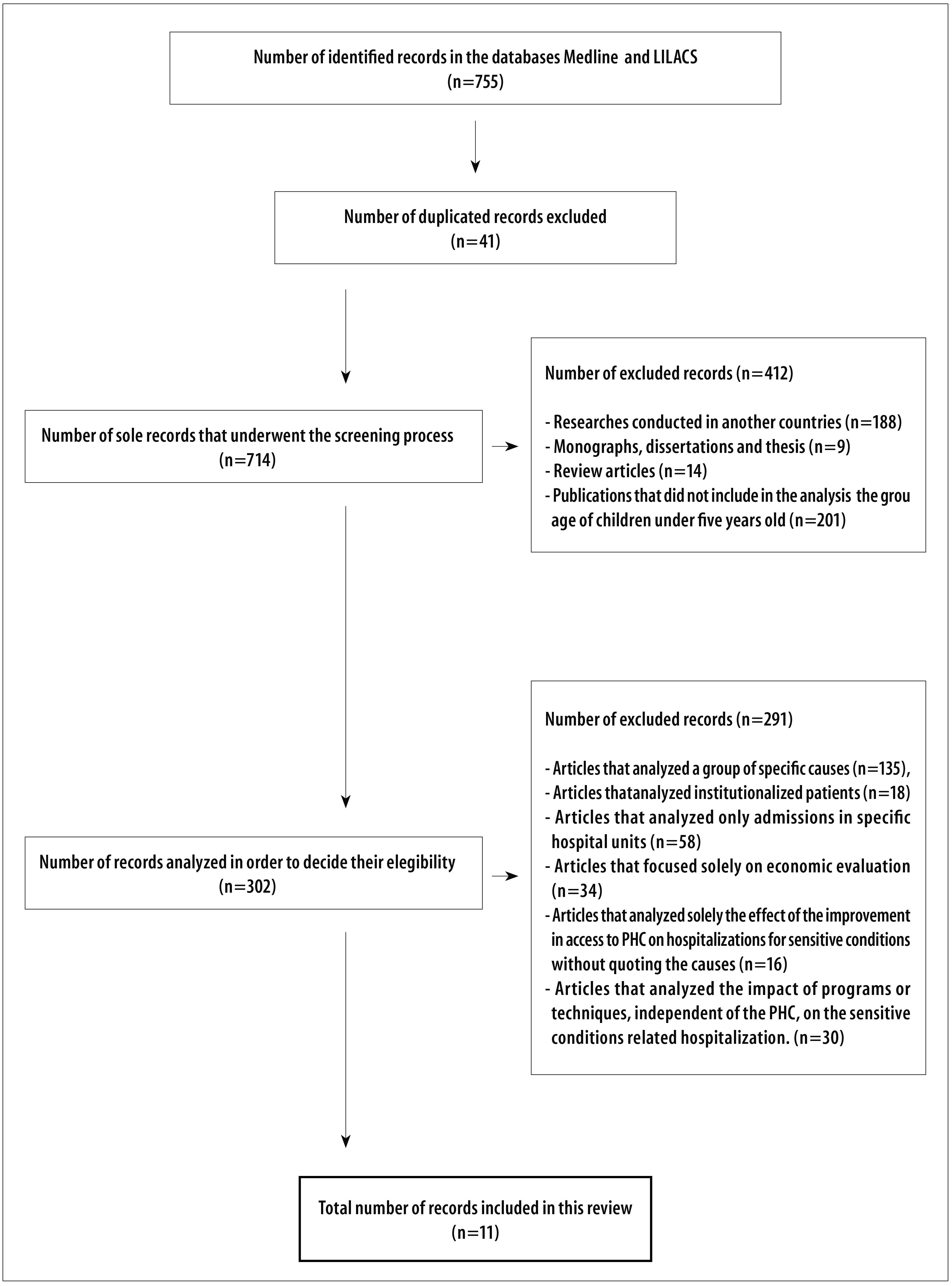
Figure 1 - Flowchart of the phases of identification, screening process, and selection of the articles about the causes of admissions in general and ambulatory care sensitive conditions related hospitalization of Brazilian children under five years old, published from 2008 to 2015
The general characterization of the studies is set in Table 1. Virtually all studies used secondary data for the survey of the information related to the causes of ACSC-related hospitalization, with the exception of one.3 Concerning the place where the studies were conducted, two of them have a nationwide scope17,18, four of them focused on the Southeastern region, 1,3,19,21, three of them refer to the Southern11,12,20 region, and two of them were held in the Northeastern region of the country. 2,22 All studies found high rates and general admissions and/or for sensitive conditions, especially for preventable causes.
Table 1 - Distribution of the included studies in the systematic review concerning the causes for general hospitalizations ambulatory care sensitive conditions related hospitalization of Brazilian children under five years old, published from 2008 to 2015
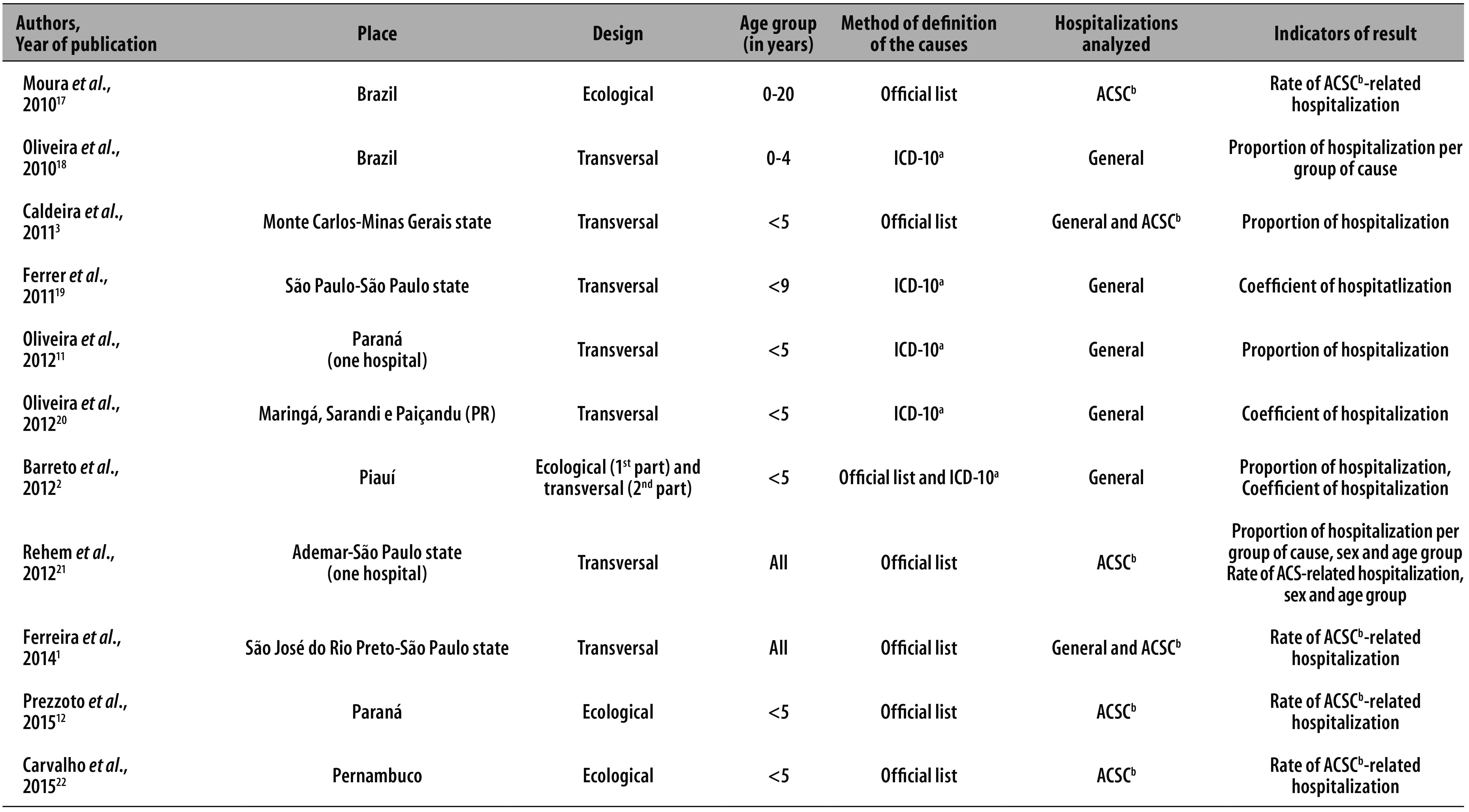
a) ICD-10: International Statistical Classification of Diseases and Related Health Problems - Tenth Revision
b) ACSC-related hospitalization: hospitalizations for Ambulatory Care Sensitive Conditions
While six studies included children’s age group which is the focus of the present review,2,3,11,12,20,22 two of them worked with all age groups1,21 and one includes children younger than 4 years old.18 The categorization of the ages was considered by four studies.1,17,19,21
The methods of definition of PHC sensitive conditions used by the studies were the following: the official list of the Brazilian Ministry of Health,7 used in six studies;1,3,12,17,21,22 ICD-10,8 used in four studies;11,18-20 and both the official list7 and the definition of the ICD-108 were used in one study.2 Regarding the hospitalizations under analysis, three studies12,17,22 referred only to ACSC-related hospitalization, five of them referred to hospitalizations in general,2,11,18-20 and three of them addressed both the ACSC-related hospitalization and hospitalizations in general.1,3,21
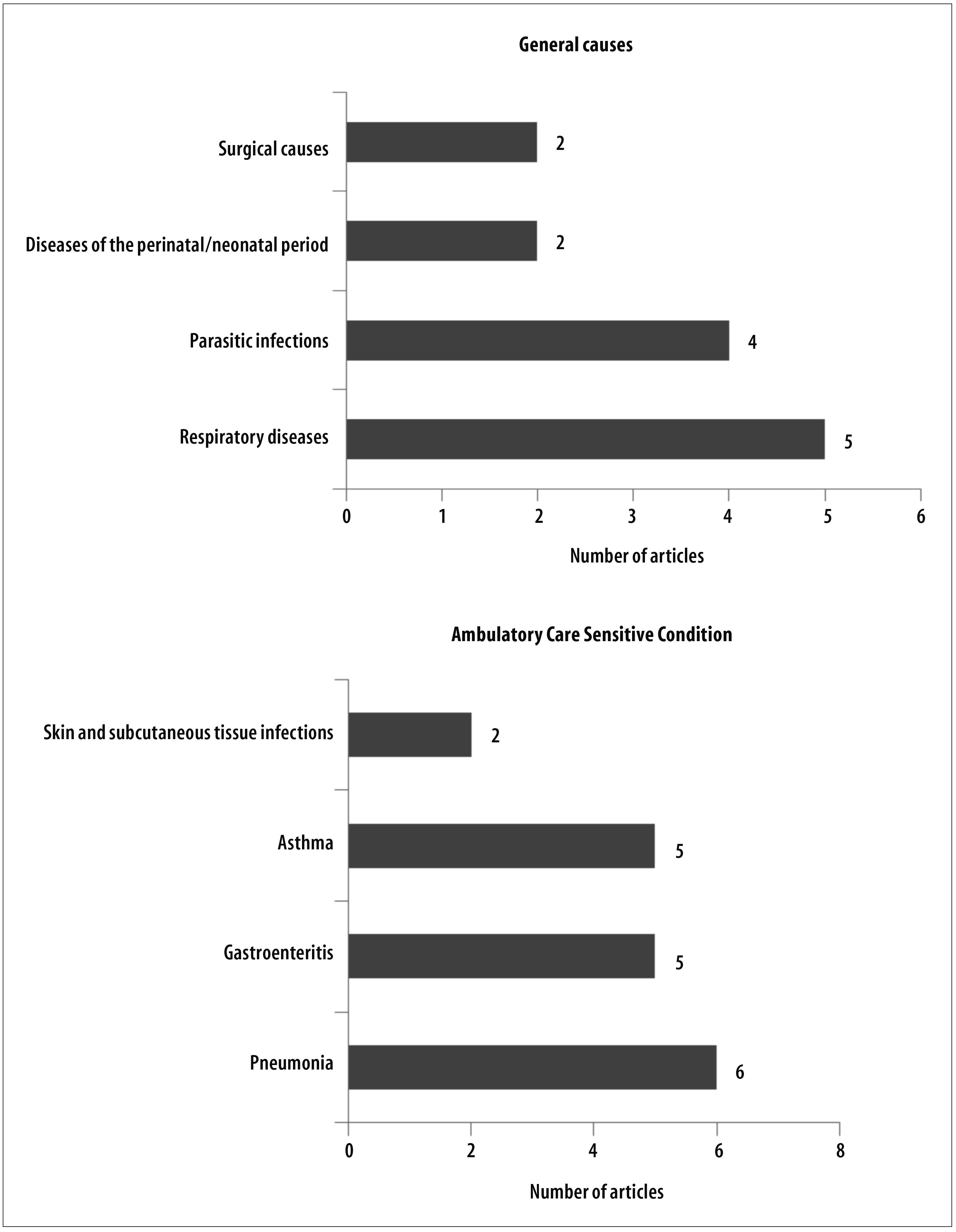
In the seven studies that addressed the admissions in general,1,2,3,11,18-20 their results reported the parasitic infections in children from 0 to 4 years old or under5, 2,3,18,20 respiratory diseases,2,11,18-20 diseases of the perinatal/neonatal period2,20 and surgical causes3,19 as causes of the most frequent hospitalizations (Table 2).
Table 2 - Main causes for hospitalizations of Brazilian children under five years old, according to the articles included in the systematic review and published from 2008 to 2015a
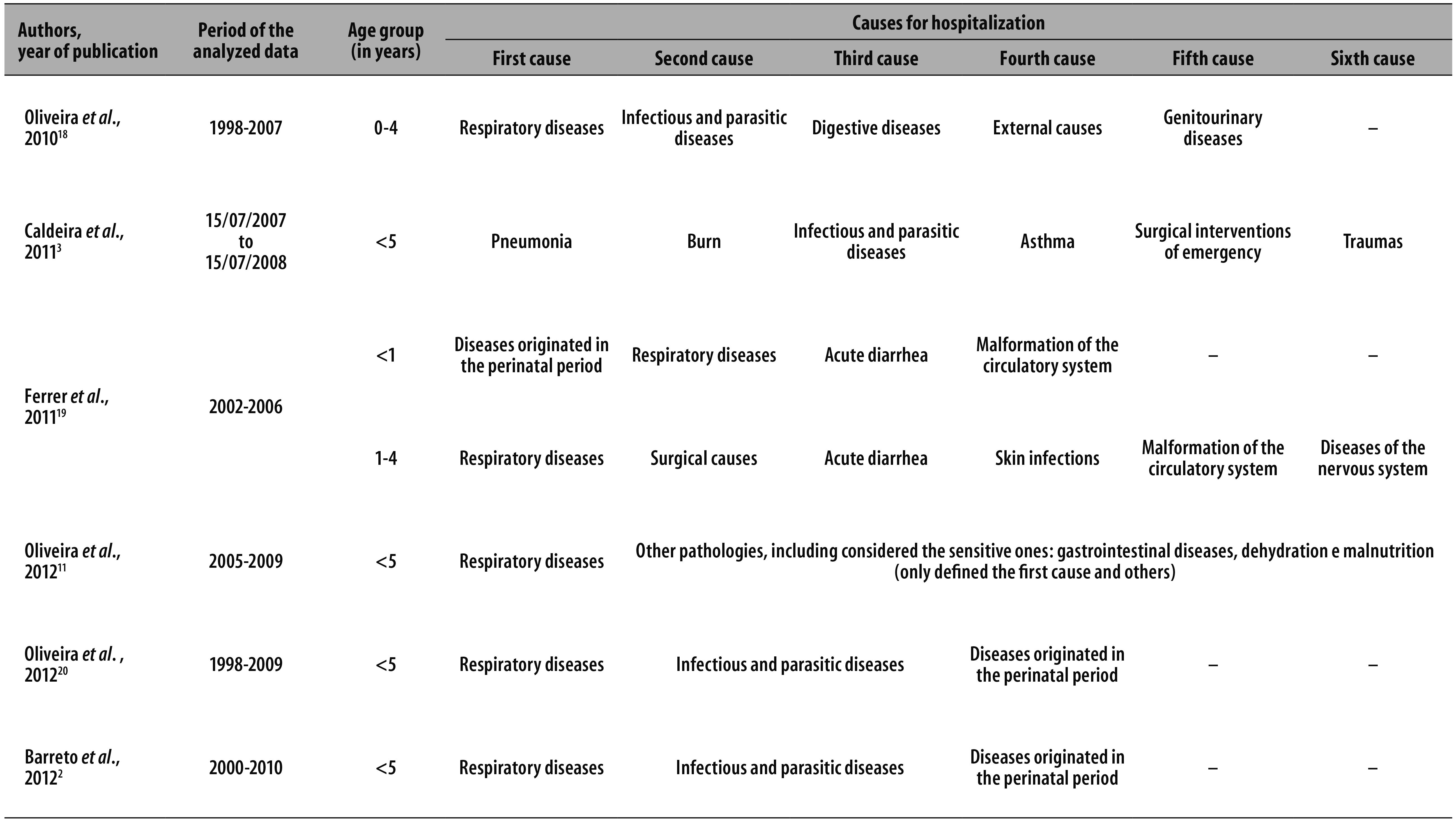
a) Ferreira et al., 2014,1 did not define the causes.
Considering the six studies that dealt with ACSC-related hospitalization,1,3,12,17,21,22 results for children from 1 to 4 years old and/or under 5 years old reported pneumonia,1,3,12,17,21,22 gastroenteritis,1,12,17,21,22 asthma3,12,17,21,22 and infections of skin and subcutaneous tissue3,21 as the causes of hospitalizations cited more frequently. Three studies of them1,17,21 discriminated the results for children under one year old, reporting pneumonia,1,17,21 asthma,17,21 gastroenteritis1,17 and kidney infections and urinary tract1,21 as leading causes for admissions (Table 3).
Table 3 - Main causes for Ambulatory Care Sensitive Conditions-related hospitalization of Brazilian children under five years old, according to the articles included in the systematic review and published from 2008 to 2015
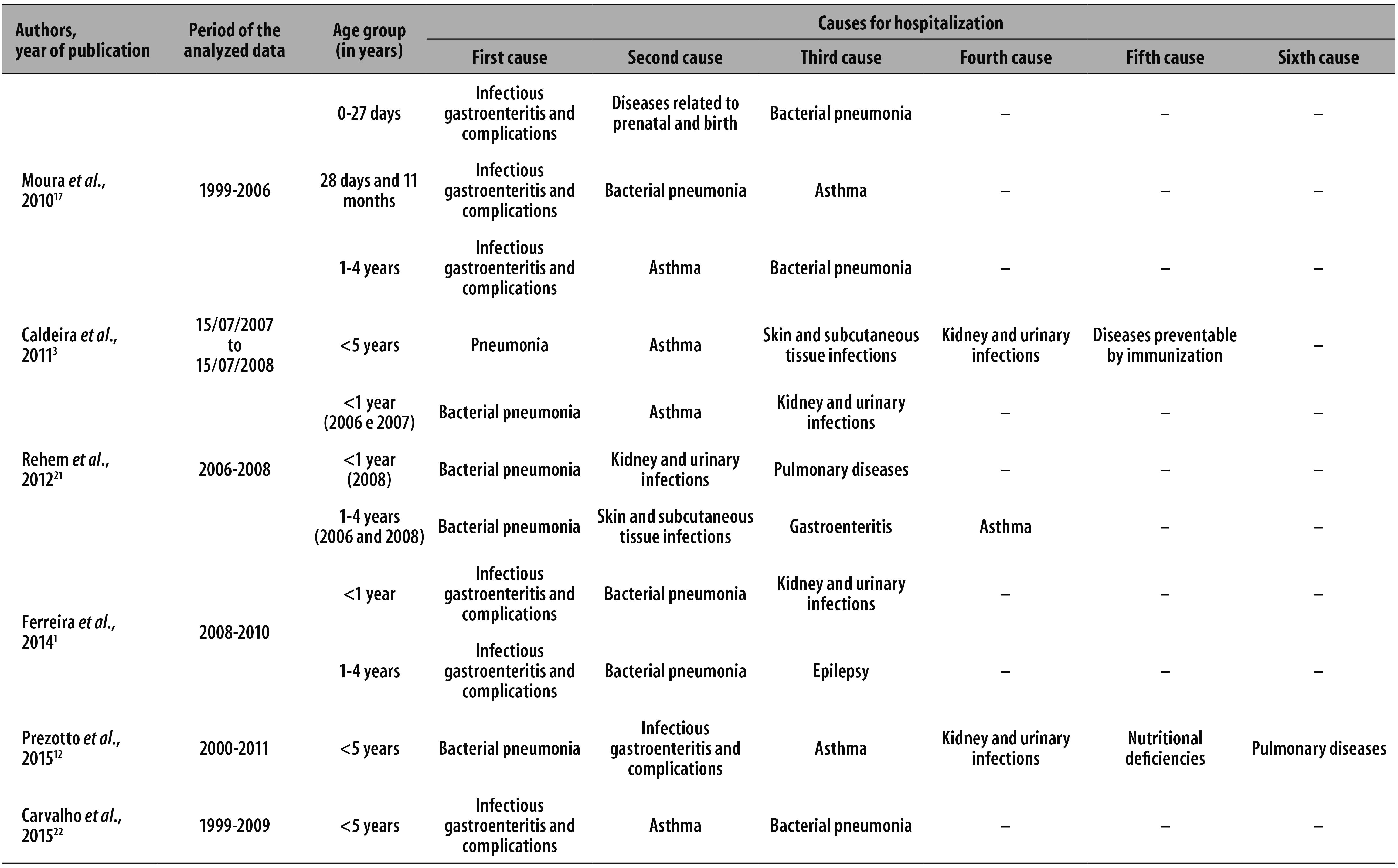
Figure 2 synthesizes the main causes of admissions. It is noticeable that pneumonia and asthma appear amongst the most frequently reported sensitive causes. These are the respiratory diseases which represent the leading causes amongst the general admissions. The gastroenteritis, parasitic type diseases, were also reported as avoidable causes of hospitalization with expressive frequency.
Discussion
According to the systematized results, pneumonia, gastroenteritis, and asthma were the main causes of ACSC-related hospitalization, resembling to the results of a previous study that pointed out higher frequencies for the first two diseases.14 These diseases are in sharp decline in the country, a fact that,12,17 added to the finding of frequencies and/or expressive rates of ACSC-related hospitalization in the reviewed articles, suggests commitment to the effectiveness of PHC. This thesis is in accordance with the results of the studies of evaluation of the Family Health Strategy (FHS) with other approaches, including perception of the users, especially related to deficiencies in the assistance for children's healthcare, to professional training, to the structure, to the process of work and to the attributes of the PHC.23-30
The results presented in this review showed respiratory diseases, especially pneumonia, as common morbidities amongst children in Brazil, including in the context of ACSC-related hospitalization, converging with the estimate of - held for the period of 1998 to 2007 — respiratory diseases representing 40% of all hospitalizations in children under five.31 Although children under five years old present greater susceptibility to hospitalization for such illnesses as a result of their biological vulnerability,31 the possibility of the timely identification of signs and symptoms of these diseases in the context of the PHC makes that outcome unjustifiable. Additionally, ambulatory care has resources of low density technology to prevent disease, which is done through immunization and antibiotics,32-34 avoiding hospitalization.
Despite the observed changes in morbidity and mortality profiles of the Brazilian population in recent decades, especially in the child’s age group,35 the intestinal parasitosis still constitute a public health problem, with more than half of Brazilian children affected, mostly in the Northeastern region of the country36,37, and in places with deficient conditions of sanitation and health education.38 This profile is also observed through the results of this research, since parasitic infections occupied a prominent position amongst the general admissions, and gastroenteritis amongst the ACSC-related hospitalizations.
It is worth to reaffirm that the PHC uses technologies of low complexity and high effectiveness, such as oral rehydration therapy and oral vaccine against human rotavirus, which are able to prevent gastroenteritis and its complications.34,35 Therefore, the indicated situation should be analyzed by considering the context of the structure and access of health units, as well as the predominance of the medical model of assistance in the daily life of health services through specific practices and healing actions, actions that go against the prospect of health promotion and prevention.23,25-27 In addition to the use of antiparasitic for the treatment of the parasitosis/enteritis in PHC, sanitation and environmental education measures are necessary, and reflects on the determinants of these conditions.6,18,39
The inclusion of asthma in the framework of the leading causes for children’s admissions, according to the results of this study, is reflected in the national statistics of the disease as a cause of large number of hospitalizations, especially of children in the age group up to the 6 years old (77.1 thousand hospitalizations in 2011), besides, it is of utmost importance to remember that asthma is responsible for the deaths of 2.5 thousand people each year.40 This reality may be conditioned by children’s health care, as shown in a study that highlighted the impact of simple practices in ambulatory care on asthma.41 It is pointed out that the management of this disease is carried out, for the most part, by punctual actions and approaches restricted to the symptomatic treatment of exacerbations, without early identification of the signs and symptoms that are essential in the prevention and resolution of the grievance.32 In the context of national policies, it is important that the professionals know and inform the citizen about the availability of free medications for asthma through the Popular Pharmacy Program.40
Kidney infections and urinary tract also represented important causes of admissions amongst children under one year old, according to the results. Children’s health care affected by these infections, through an early diagnosis, appropriate treatment and, in cases of recurrence, appropriate prophylaxis, can encourage the reduction of hospitalization and adverse effects resulting from the disease, such as pyelonephritis, with less likely therapeutic treatment in the ambulatory level.6 Concerning these infections and diagnosis, it is necessary to emphasize the importance of urinalysis, considered routine for its simplicity, low cost and ease of obtaining the sample; as for treatment, the use of drugs with antibiotics; and in case of recurrence, prolonged prophylaxis with antiseptic drugs.6,42 In children under one year old, breastfeeding may reduce the risk of urinary infections ambulatory care sensitive.42,43
In the context of general admissions, the perinatal causes revealed their relevance. The implementation of clinical protocol for the management of the prenatal care in PHC stands out amongst the priority measures to address adverse perinatal outcomes. It is suggested the impact of the following actions during the prenatal: supplementation with folic acid, vitamin A and iron; tetanus immunization; conducting examinations and treatment of infectious diseases; early diagnosis and treatment of hypertension and gestational diabetes; and calcium supplementation to prevent preeclampsia. Other relevant actions are increasing the amount of time between pregnancies and the presence of companion during labour.
It is appropriate to remember that the genesis of main diseases identified in this study as leading causes of ACSC-related hospitalizations is related to multiple circumstances to consider.12,17 One of them are the factors related to demographic and health profile of the population, to the network of health services available and to the specific context of the PHC/FHS (composition, qualification of human resources, employment bond, process of work and developed actions).12,17,44 Hence, FHS must face some challenges not only related to its structure and process of work, the due quality of PHC depends on the capacity to overcome some issues from these areas, but also the development of intersectoral actions in the confrontation of issues related to the social determinants of health-disease process.25
The results of this research should be analyzed with caution. First, the geographical concentration of the studies in the Southeast region limits the analysis of socio-spatial inequalities that characterize Brazil, and makes it impossible to extrapolate the results to the other regions or the whole country. The Southeast region is the largest one, and the concentration of production of scientific studies on it concerning ACSC-related hospitalization was also demonstrated in another review study,14 signaling the importance of developing greater amount of work in less developed regions of the country.
The methodological constraint imposed by the use of secondary sources in the Brazilian studies here organized matches the reality of the scientific production worldwide.45 In spite of the recognized inaccuracies resulting from secondary data and the possibility of fraud by financial issues, the national literature points out, too, that the hospital information system of the Brazilian National Health System (SUS) is characterized by its broadness and capacity to analyse the admissions in Brazil.12,14,46 Furthermore, important advances have occurred in the country in recent decades, in the process of implementation of health information systems, with the expansion of coverage, access to and use of national databases.47
Other limitations of this review can derive from the use of different lists of admissions by the different researches, and the consequent restraint for comparison of the results. In addition to this, there is not a specific descriptor about the ACSC-related hospitalization, which makes more complex the bibliographic search about the topic. The critical evaluation of the ecological studies, through an instrument that is not specific to this type of delineation, should also be mentioned. Nevertheless, it is important to emphasize that there is no similar proposal to those studies, studies included in this review resemble the cross design ones, for its characteristics of temporality, calculations of ACSC-related hospitalization rates and definition of the causes of admissions.
Despite the aforementioned limitations, the findings of this study represent a warning signal in order to trigger mechanisms for analysis and search for explanations for the occurrence of admissions, especially those related to the ambulatory care sensitive conditions (ASCS). The presented results allow an overview of the causes of hospitalizations, the general ones and the ambulatory care sensitive conditions in Brazilian children younger than five years old.
We concluded that pneumonia, gastroenteritis and asthma still are important causes of hospitalization amongst children, albeit they are preventable and treatable with the use of lower cost technologies currently available. When analyzed the hospitalizations in general, the reality is similar. In addition to the perinatal diseases, respiratory diseases and parasitic infections stand out, these two include, respectively, pneumonia and gastroenteritis. This is a worrisome panorama, considering the existence of the Family Health Strategy for more than two decades. The understanding of the importance of health promotion and disease prevention, as a practice directed toward children under the age of five, is essential to minimize the complications and hospitalization derived from morbidity in this segment of the population.
Referências
1. Ferreira JBB, Borges MJG, Santos LL, Forster AC. Internações por condições sensíveis à atenção primária à saúde em uma região de saúde paulista, 2008 a 2010. Epidemiol Serv Saude. 2014 mar;23(1):45-56. [ Links ]
2. Barreto JOM, Nery IS, Costa MSC. Estratégia Saúde da Família e internações hospitalares em menores de 5 anos no Piauí, Brasil. Cad Saude Publica. 2012 mar;28(3):515-26. [ Links ]
3. Pazó RG, Frauches DO, Galvêas DP, Stefenoni AV, Cavalcante ELB, Pereira-Silva FH. Internações por condições sensíveis à atenção primária no Espírito Santo: estudo ecológico descritivo no período 2005-2009. Epidemiol Serv Saude. 2012 jun;21(2):275-82. [ Links ]
4. Caldeira AP, Fernandes VBL, Fonseca WP, Faria AA. Internações pediátricas por condições sensíveis à atenção primária em Montes Claros, Minas Gerais, Brasil. Rev Bras Saude Matern Infant. 2011 jan-mar;11(1):61-71. [ Links ]
5. Rehem TCMSB, Egry EY. Internações por condições sensíveis à atenção primária no estado de São Paulo. Cien Saude Colet. 2011 dez;16(12):4755-66. [ Links ]
6. Rodrigues-Bastos RM, Campos EMS, Ribeiro LC, Firmino RUR, Bustamante-Teixeira MT. Internações por condições sensíveis à atenção primária em município do sudeste do Brasil. Rev Assoc Med Bras. 2013 mar-abr;59(2):120-7. [ Links ]
7. Brasil. Ministério da Saúde. Portaria nº 221, de 17 de abril de 2008. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2008 abr 18;Seção 1:70. [ Links ]
8. World Health Organization. International statistical Classification of Diseases and Related Health Problems. 10th ed. Geneva: World Health Organization; 2010. [ Links ]
9. Alfradique ME, Bonolo PF, Dourado I, Lima-Costa MF, Macinko J, Mendonça CS, et al. Internações por condições sensíveis à atenção primária: a construção da lista brasileira como ferramenta para medir o desempenho do sistema de saúde (Projeto ICSAP - Brasil). Cad Saude Publica. 2009 jun;25(6):1337-49. [ Links ]
10. Dias-da-Costa JS, Büttenbender DC, Hoefel AL, Souza LL. Hospitalizações por condições sensíveis à atenção primária nos municípios em gestão plena do sistema no estado do Rio Grande do Sul, Brasil. Cad Saude Publica. 2010 fev;26(2):358-64. [ Links ]
11. Oliveira BRG, Viera CS, Furtado MCC, Mello DF, Lima RAG. Perfil de morbidade de crianças hospitalizadas em um hospital público: implicações para a Enfermagem. Rev Bras Enferm. 2012 jul-ago;65(4):586-93. [ Links ]
12. Prezotto KH, Chaves MMN, Mathias TAF. Hospitalizações sensíveis à atenção primária em crianças, segundo grupos etários e regionais de saúde. Rev Esc Enferm USP. 2015 fev;49(1):44-53. [ Links ]
13. Ministério da Saúde (BR). Mortalidade perinatal: síntese de evidências para políticas de saúde. Brasília: Ministério da Saúde; 2012. (Série B. Textos Básicos de Saúde). [ Links ]
14. Pereira FJR, Silva CC, Lima Neto EA. Condições sensíveis à Atenção Primária: uma revisão descritiva dos resultados da produção acadêmica brasileira. Saude Debate. 2014 out;38(n. esp.):331-42. [ Links ]
15. Galvão TF, Pansani TSA, Harrad D, tradutores. Principais itens para relatar Revisões sistemáticas e Meta-análises: A recomendação PRISMA. Epidemiol Serv Saude. 2015 abr-jun;24(2):335-42. [ Links ]
16. Munn Z, Moola S, Riitano D, Lisy K. The development of a critical appraisal tool for use in systematic reviews addressing questions of prevalence. Int J Health Policy Manag. 2014 Aug;3(3):123-8. [ Links ]
17. Moura BLA, Cunha RC, Aquino R, Medina MG, Mota ELA, Macinko J, et al. Principais causas de internação por condições sensíveis à atenção primária no Brasil: uma análise por faixa etária e região. Rev Bras Saude Mater Infant. 2012 nov;10(supl 1):S83-91. [ Links ]
18. Oliveira BRG, Vieira CS, Collet N, Lima RAG. Causas de hospitalização no SUS de crianças de zero a quatro anos no Brasil. Rev Bras Epidemiol. 2010 jun;13(2):268-77. [ Links ]
19. Ferrer APS, Sucupira ACSL, Grisi SJFE. Causes of hospitalization among children ages zero to nine years old in the city of São Paulo, Brazil. Clinics. 2010 Jan;65(1):35-44. [ Links ]
20. Oliveira RR, Costa JR, Mathias TAF. Hospitalizações em menores de cinco anos por causas evitáveis. Rev Latino-Am Enfermagem. 2012 jan-fev;20(1):135-42. [ Links ]
21. Rehem TCMSB, Ciosak SI, Egry EY. Internações por condições sensíveis à atenção primária no hospital geral de uma microrregião de saúde do município de São Paulo, Brasil. Texto Contexto - Enferm. 2012 jul-set;21(3):535-42. [ Links ]
22. Carvalho SC, Mota E, Dourado I, Aquino R, Teles C, Medina MG. Hospitalizations of children due to primary health care sensitive conditions in Pernambuco State, Northeast Brazil. Cad Saude Publica. 2015 abr;31(4):744-54. [ Links ]
23. Souza RS, Ferrari RAP, Santos TFM, Tacla MTGM. Atenção à saúde da criança: prática de enfermeiros da Saúde da Família. Rev Min Enferm. 2013 abr-jun; 17(2):331-9. [ Links ]
24. Sarti TD, Campos CEA, Zandonade E, Ruschi GEC, Maciel ELN. Avaliação das ações de planejamento em saúde empreendidas por equipes de saúde da família. Cad Saude Publica. 2012 mar;28(3):537-48. [ Links ]
25. Arantes LJ, Shimizu HE, Merchán-Hamann E. Contribuições e desafios da Estratégia Saúde da Família na Atenção Primária à Saúde no Brasil: revisão da literatura. Cienc Saude Colet. 2016 mai;21(5):1499-510. [ Links ]
26. Silva LA, Casotti CA, Chaves SCL. A produção científica brasileira sobre a Estratégia Saúde da Família e a mudança no modelo de atenção. Cienc Saude Colet. 2013 jan;18(1):221-32. [ Links ]
27. Sampaio LFR. The Brazilian health system: highlighting the primary health care reform. Ital J Public Health. 2010;7(2):359-68. [ Links ]
28. Leão CDA, Caldeira AP, Oliveira MMC. Atributos da atenção primária na assistência à saúde da criança: avaliação dos cuidadores. Rev Bras Saude Mater Infant. 2011 jul-set;11(3):323-34. [ Links ]
29. Leão CDA, Caldeira AP. Avaliação da associação entre qualificação de médicos e enfermeiros em atenção primária em saúde e qualidade da atenção. Cienc Saude Colet. 2011 nov;16(11):4415-23. [ Links ]
30. Mesquita Filho M, Luz BSR, Araújo CS. A Atenção Primária à Saúde e seus atributos: a situação das crianças menores de dois anos segundo suas cuidadoras. Cienc Saude Colet. 2014 jul;19(7):2033-46. [ Links ]
31. Natali RMT, Santos DSPS, Fonseca AMC, Filomeno GCM, Figueiredo AHA, Terrivel PM, et al. Perfil de internações hospitalares por doenças respiratórias em crianças e adolescentes da cidade de São Paulo, 2000-2004. Rev Paul Enferm. 2011 dez;29(4):584-90. [ Links ]
32. Ministério da Saúde (BR). Secretaria de Políticas de Saúde. Departamento de Atenção Básica. Doenças Respiratórias Crônicas. Brasília (DF): MS; 2010. (Cadernos de Atenção Básica, n. 25) (Série A. Normas e Manuais Técnicos). [ Links ]
33. Avelino CCV, Goyatá SLT, Nogueira DA, Rodrigues LBB, Siqueira SMS. Qualidade da atenção primária à saúde: uma análise segundo as internações evitáveis em um município de Minas Gerais, Brasil. Cienc Saude Colet. 2015 abr;20(4):1285-93. [ Links ]
34. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Programa Nacional de Imunizações: aspectos históricos dos calendários de vacinação e avanços dos indicadores de coberturas vacinais, no período de 1980 a 2013. Bol Epidemiol. 2015;46(30):1-13. [ Links ]
35. Victora CG, Aquino EML, Leal MC, Monteiro CA, Barros FC, Szwarcwald CL. Saúde de mães e crianças no Brasil: progressos e desafios. Lancet. 2011 mai; 32-46. [ Links ]
36. Vasconcelos IAB, Oliveira JW, Cabral FRF, Coutinho HDM, Menezes IRA. Prevalência de parasitoses intestinais entre crianças de 4-12 anos no Crato, Estado do Ceará: um problema recorrente de saúde pública. Acta Sci Health Sci. 2011 jan-jun;33(1):35-41. [ Links ]
37. Junqueira RMP, Duarte EC. Internações hospitalares por causas sensíveis à atenção primária no Distrito Federal, 2008. Rev Saude Publica. 2012 out;46(5):761-8. [ Links ]
38. Valadares MB, Fonseca HM, Welter A. Parasitos intestinais em sanitários públicos da cidade de Palmas - TO. Cereus. 2014 jan-abr;9(1):19-34. [ Links ]
39. Andrade EC, Leite ICG, Rodrigues VO, Cesca MG. Parasitoses intestinais: uma revisão sobre seus aspectos sociais, epidemiológicos, clínicos e terapêuticos. Rev APS. 2010 abr-jun;13(2):231-40. [ Links ]
40. Damasceno E, Costa-Carvalho BT, Solé D, Wandalsen GF. Custos diretos e indiretos da asma: revisão de literatura. Rev. Bras. Alerg. Imunopatol. 2012 nov-dez;35(6):234-40. [ Links ]
41. Fontes MJF, Affonso AGA, Calazans GMC, Andrade CR, Lasmar LMLBF, Nader CMFF, et al. Impacto de um programa de manejo da asma sobre as hospitalizações e os atendimentos de urgência. J Pediatr (Rio J). 2011 set-out;87(5):412-8. [ Links ]
42. Rangel M, Tressa Y, Zago SS. Infecção urinária: do diagnóstico ao tratamento. Colloquium Vitae. 2013 jan-jun;5(1):59-67. [ Links ]
43. Damasio CP, Fingerhut DJP, Lima MZ, Reis MGS, Ehrenfreund R, Oliveira RRFC, et al. Revisão sistemática com metanálise relacionando as taxas de aleitamento materno com a prevalência de infecções urinárias em crianças. Rev UNILUS Ensino Pesqui. 2016 jan-mar;13(30):99-104. [ Links ]
44. Melo MD, Egry EY. Determinantes sociais das Internações por Condições Sensíveis à Atenção Primária em Guarulhos, São Paulo. Rev Esc Enferm USP. 2014 ago;48(n. esp.):133-40. [ Links ]
45. Nedel FB, Facchini LA, Martín M, Navarro A. Características da atenção básica associadas ao risco de internar por condições sensíveis à atenção primária: revisão sistemática da literatura. Epidemiol Serv Saude. 2010 jan-mar;19(1):61-75. [ Links ]
46. Rehem TCMSB, Oliveira MRF, Ciosak SI, Egry EY. Registro das internações por condições sensíveis à atenção primária: validação do sistema de informação hospitalar. Rev Latino-Am Enfermagem. 2013 set-out;21(5):06 telas. [ Links ]
47. Mello Jorge MHP, Laurenti R, Gotlieb SLD. Avaliação dos Sistemas de Informação em Saúde no Brasil. Cad Saude Colet. 2010 jan-mar;18(1):7-18. [ Links ]
Received: June 15, 2016; Accepted: July 29, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
