










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.1 Brasília jan./mar. 2017
http://dx.doi.org/10.5123/s1679-49742017000100019
PROFILE OF NATIONAL HEALTH DATABASES
Characteristics of the Violence and Accidents Survey Conducted in Brazilian Sentinel Emergency Departments
1Universidade Federal de Goiás, Hospital das Clínicas, Goiânia- GO, Brasil
2Universidade Federal do Piauí, Programa de Pós-Graduação em Saúde e Comunidade, Teresina-PI, Brasil
3Ministério da Saúde, Secretaria de Vigilância em Saúde, Brasília-DF, Brasil
4Universidade Federal de Minas Gerais, Escola de Enfermagem, Belo Horizonte-MG, Brasil
5Universidade de São Paulo, Departamento de Medicina Social, Ribeirão Preto-SP, Brasil
6Universidade de Brasília, Programa de Pós-Graduação em Saúde Coletiva, Brasília-DF, Brasil
7Fundação Oswaldo Cruz, Escola Nacional de Saúde Pública, Rio de Janeiro-RJ, Brasil
8Universidade São Paulo, Núcleo de Pesquisas Epidemiológicas em Nutrição e Saúde, São Paulo-SP, Brasil
The Violence and Accidents Survey Conducted in Sentinel Emergency Departments (VIVA Survey) is the sentinel surveillance component of the Violence and Accidents Surveillance System (VIVA). It was conducted for the first time in 2006 and again in 2007, 2009, 2011 and 2014. The sample is comprised of victims of accidents and violence treated in Emergency Departments linked to the Brazilian National Health System (SUS). The services are selected intentionally. This isfollowed by probability sampling of 12-hour shifts by conglomerates in single-stage selection. Data is collected by trained interviewers using a standard form. The variables include data about the service site, the victim, the event, injury and case development. The VIVA Survey provides key information for the implementation of policies for addressing violence and accidents as well as for health and peace promotion policies.
Key words: Health Surveys; Epidemiological Surveillance; Violence; Accidents; External Causes
Introduction
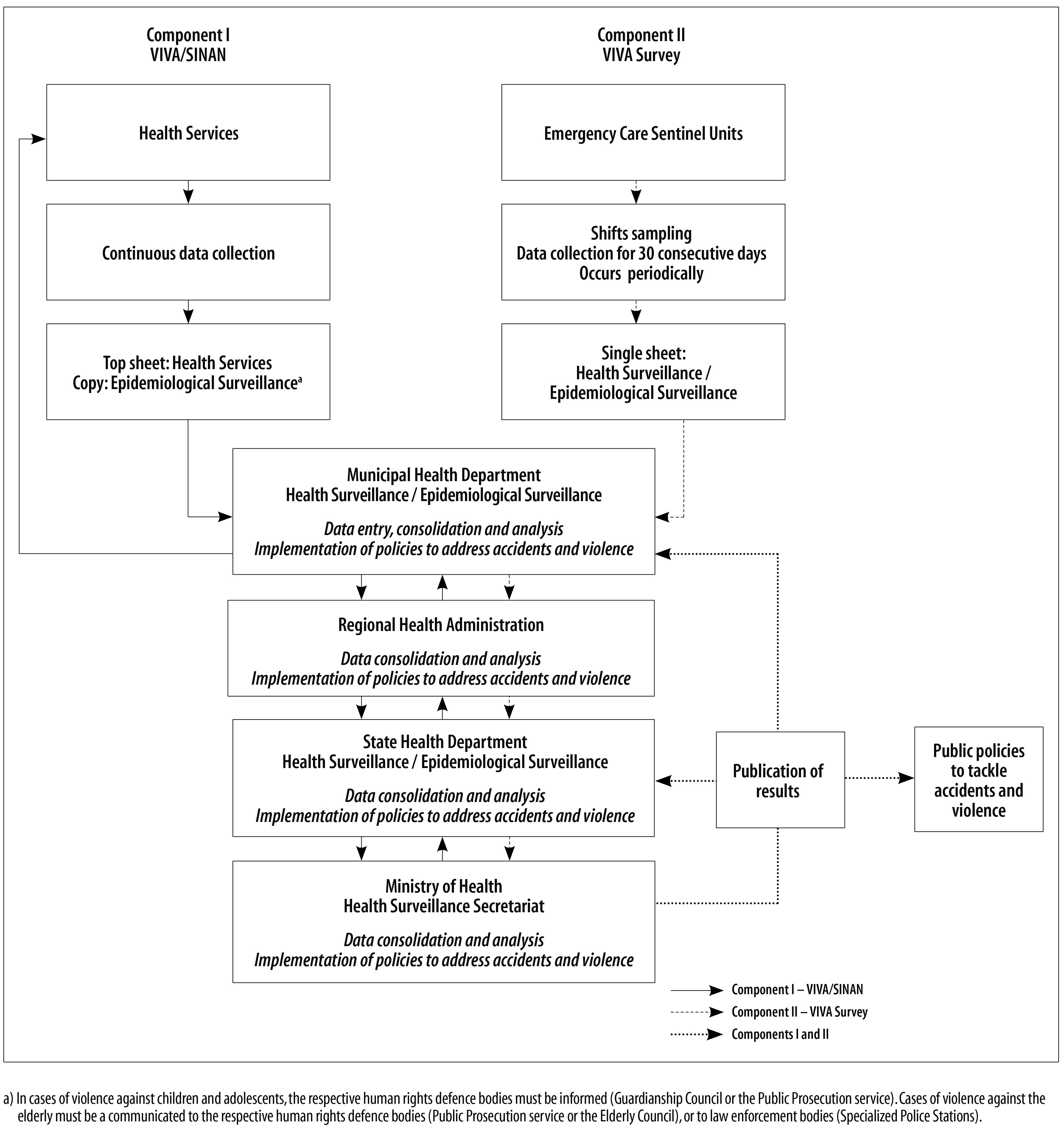
The Violence and Accidents Survey Conducted in Sentinel Emergency Departments (VIVA Survey) is the sentinel surveillance component of the Violence and Accidents Surveillance System (VIVA). The VIVA System also has a component providing continuous surveillance of domestic violence, sexual violence and/or other interpersonal and self-inflicted violence (VIVA Sinan) (Figure 1). The main focus of the VIVA System is to provide knowledge on the magnitude and severity of accidents and violence injuries in order to subsidize policies to address these conditions which are classified as external causes of morbidity and mortality.1-6
The VIVA System was launched in 2006, during the Thematic Seminar on the Surveillance of Accident and Violence Attendances in Sentinel Services as part of the Violence and Accidents Surveillance Project within the Violence and Accidents Sentinel Service Network (VIVA Network).1-6 . It is an initiative lead by the General Coordination of Noncommunicable Diseases Surveillance and Health Promotion (CGDANT), under the Department of Noncommunicable Diseases Surveillance and Health Promotion (DANTPS) within the Health Surveillance Secretariat (SVS/MS), of the Brazilian Ministry of Health. The system is in line with the National Policy on the Reduction of Accident and Violence Morbidity and Mortality (2001),7 the National Network of Violence Prevention and Health Promotion Centres (2004),8 and the National Health Promotion Policy (2006).9 The financial incentive for the implantation of the VIVA initiative was brought into being by Ordinance No. 1356/2006.10
The monitoring of external causes has been traditionally done by analyzing data from the Mortality Information System (SIM) and the National Hospital Information System (SIH-SUS), both of which are managed by the Ministry of Health (MS).1-6 However, these systems only record more serious cases, the outcome of which is death or hospitalization, in addition to only capturing information about victims. Few countries have systems providing information on inpatient and outpatient morbidity due to external causes.11-13
The VIVA System is a useful strategy for detailing less serious cases and has the potential to provide data on domestic and sexual violence, self-inflicted violence, child labour, psychological/moral violence and neglect/abandonment, as will as information on the perpetrations of violence.1-6
The VIVA Survey was conducted for the first time in 2006 following a period of planning which lasted around two years, based on local experiences, such as those of São Paulo/SP, Campinas/SP, Belo Horizonte/MG, Curitiba/PR, Goiânia/GO and Ribeirão Preto/SP; as well as international experiences such as that of the United States Center for Disease Control and Prevention (CDC).3 All the state-level Health Departments, the Federal District Health Department, the state capital city Health Departments and the Health Departments of some municipalities selected to develop external cause surveillance actions were invited to adhere to the proposal.1-3
Summary of the profile of the VIVA survey
When 2007edition of the VIVA Survey was evaluated during the 2nd National Seminar on Violence and Accident Surveillance, taking into account the logistics and the cost of the survey and the focus on trend analyses, it was decided to conduct the surveys periodically instead of annually. Five VIVA Surveys have been conducted so far, in 2006, 2007, 2009, 2011 and 2014.2,4,5,14 The current proposal is that the survey be conducted every three years and the next survey is due to take place in 2017.
Sample
The VIVA Survey sample is comprised of victims of accidents and violence cared for in the Brazilian National Health System (SUS) Emergency Departments. The services are selected from the National Health Establishment Register (CNES) based on the following inclusion criteria: (i) being a provider of emergency care services; and (ii) being a referral service for external causes in the municipality. Local health services managers are asked to validate the services selected, which must be entry points for caring for trauma arising from violence and accidents. This defines them as sentinel services for these conditions.
The services are then classified as to the volume of the demand for care for external causes, according to SIH-SIS hospitalization data and VIVA Survey data (for services taking part in the survey in 2006, 2007, 2009 and 2011).2,4,5,14
Following the intentional selection of the health establishments, probability sampling is then performed on 12-hour shifts, by conglomerates in single-stage selection stratified by establishment, whereby the shift is the Primary Sampling Unit (PSU) and the strata are comprised of the establishments.15-18 For the purpose of drawing lots, two shifts are taken into consideration (day shift and night shift) during the 30-day data collection period. This involves a total of 60 shifts, i.e. 30 day shifts (7 a.m. to 6.59 p.m.) and 30 night shifts (7 p.m. to 6.59 a.m.). All attendances due to external causes during the shift are included in the sample.
The precision criterion for prevalence estimates set for cross-sectional studies is taken into consideration when defining the sample size. In order to meet this criterion, the coefficient of variation must be less than 30% and standard error must be less than 3. Table 1 shows the sample sizes that include correction of design effect (deff=2) to ensure the precision of estimates obtained in surveys involving complex sampling plans. For VIVA Survey, the sample size calculated is, at least, 1,500 attendances in inner state municipalities and 2,000 attendances in state capitals. The number of shifts to be drawn by lot in each establishment is obtained using the ratio between minimum sample size of external cause attendances (n(total)= 1,500 or 2,000) and average attendances due to these causes in the same establishment in previous years Ni(total).
Table 1- Standard errors and variation coefficients (vc) by sample size (n) for cross-sectional studies
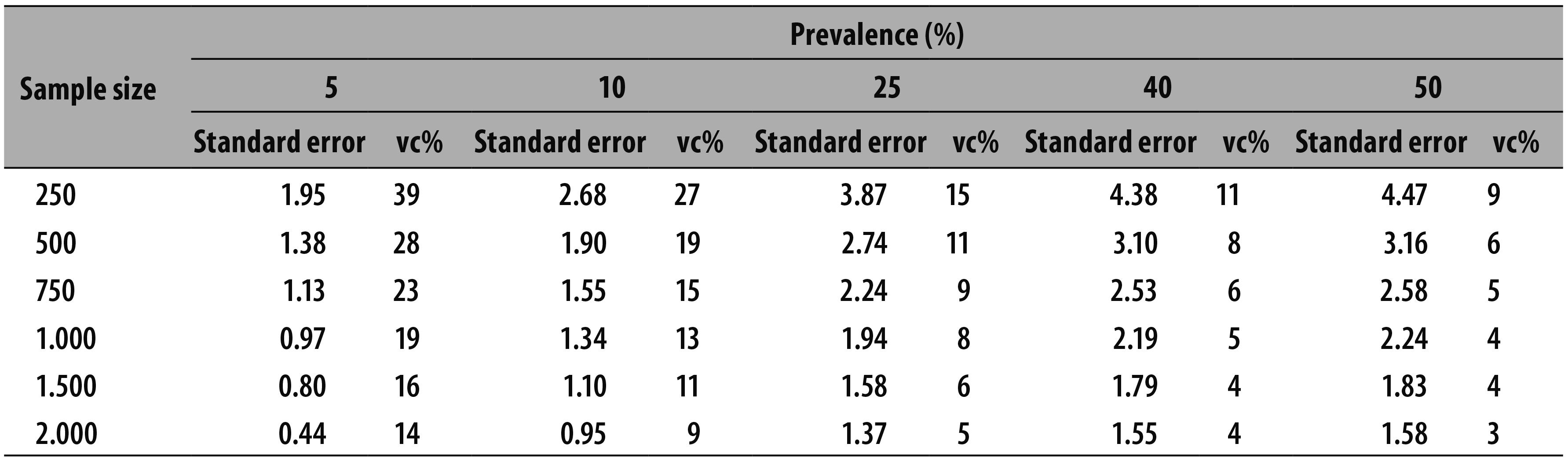
Source: United Nations. Department of Economic and Social Affairs, Statistics Division. Household Sample Surveys in Developing and Transition Countries (ST/ESA/STAT/SER.F/96), New York, 2005. p. 27-28.18
f = n(total) / Ni (total)
After that, the number of shifts to be drawn by establishment obtained by multiplying the sample fraction for each municipality per 60 (total number of shifts in a 30-day period).
t = f * 60
As an example, the procedure is shown below for drawing shifts in the municipality of Curitiba/PR (Table 2). Eleven shifts were drawn in this state capital city. In the 2009 and 2011 surveys two reserve shifts were drawn in order to ensure the achievement of minimum sample size; this did not occur in 2014. Once the number of shifts to be drawn for each municipality has been identified, the shift sample is obtained using ordered systematic selection, whereby the shifts are numbered from 1 to 60; the odd-numbered shifts indicate daytime data collection whilst the even-numbered shifts indicate night-time data collection. The selection interval is calculated by dividing the total number of shifts by the number of shifts to be drawn. A random number between 1 and the interval is then selected in order to identify the random starting point or the first element (shift). Following this, the number of the first element is added to the interval value in order to identify the second element and so on successively.
Table 2 - Example of the calculation of the number of shifts to be drawn in the services taking part in the Violence and Accidents Survey Conducted in Brazilian Sentinel Emergency Services (VIVA Survey), in Curitiba, Paraná, 2011
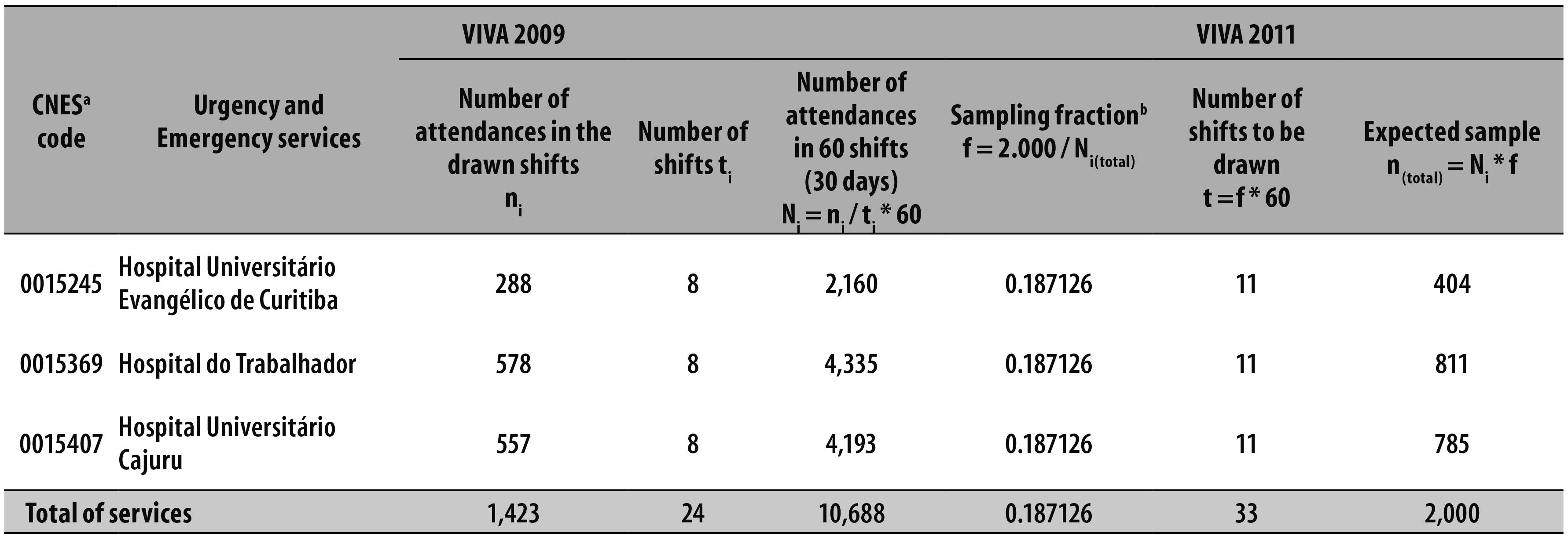
a) CNES code - Code at the National Registry of Health Facilities.
b) Sampling fraction (f) calculated considering the number of attendances for the total of establishments in the municipality and replicated to each establishment.
It was defined that data collection should take place during a 30-day period in the months of September and October, in order to avoid months when holidays are taken or months with a lot of public holidays, as these might increase the demand for care for external cause patients.2,4,5,14
Table 3 shows the number of services, municipalities and Federative Units (UFs) taking part in all the VIVA Surveys, as well as the number of attendances in each survey. The progression of the surveys can be seen with regard to complexity and increased number of services taking part.
Table 3 - Number of participating services, municipalities and Federative Units (UFs) and number of attendances recorded, by year of the Violence and Accidents Survey Conducted in Brazilian Sentinel Emergency Departments (VIVA Survey)

a) 21 state capitals, Federal District and 13 selected municipalities.
b) 23 state capitals, Federal District and 14 selected municipalities.
c) 23 state capitals, Federal District and 12 selected municipalities.
d) 24 state capitals, Federal District and 11 selected municipalities.
e) 24 state capitals, Federal District and 11 selected municipalities.
f) Number of attendances in the state capitals.
Following the first survey, services located in the state capitals and Federal District took part in the VIVA Survey, as well as some municipalities that had adhered to the 2006 survey.2 However, not all capitals or municipalities took part in all the surveys owing to issues relating to local management, whether these were political, administrative or technical/operational. It is noteworthy that the municipality of São Paulo, the country’s largest, only joined the VIVA Survey in 2011. Even so, owing to aspects relating to local management and the complexity of the hospital network, it only carried out a pilot survey in some services.
In 2009 a parallel survey was conducted involving other municipalities, over and above the state capitals, in the states of Espírito Santo, Mato Grosso, Rio Grande do Sul and Santa Catarina, with the aim of performing a pilot study to enable comparison between services in the state capitals and those in inner state cities. The same year two other specific studies also took place, one in Teresina/PI, where data collection occurred at 100% of the entry points of the municipality’s emergency care services, with the aim of verifying differences in the frequency of attendances for violence and accidents, by comparing data collected in selected services or in all services. The other study took place in Campinas/SP to compare external cause attendances between public and private health services.
In 2014 the state capital cities Florianópolis/SC and Cuiabá/MT were unable to conduct the survey owing to issues relating to local management. The remaining places that had taken part in the previous surveys were kept the same, except for Ananindeua/PA, which only joined the survey in 2011 as it is an important entry point for care for external cause cases in the Metropolitan Region of Belém/PA. The list of state capital cities taking part in each VIVA Survey is provided in the supplementary material available in the electronic version of this article (Appendix A).
Participants
The atudy population comprises people who sought emergency care owing to accidents or violence and who agreed to take part in the survey by giving their verbal consent.
An Accident is defined here as an “unintentional and avoidable event, causing physical and emotional injury, at home or in social situations such as work, school, sport and leisure”2,4,5,14,19 The definition of violence used is that given by the World Health Organization (WHO), which characterizes it as “the use of physical force against a group or community, that either results in or has a high likelihood of resulting in injury, death, psychological harm, maldevelopment or deprivation”11 These two definitions are in agreement with the 10th revision of the International Statistical Classification of Diseases and Health Related Problems (ICD-10)19 with regard to chapter XX thereof - External causes of morbidity and mortality. Events involving accidental causes include: transport accidents, falls, burns and other accidental events, such as cuts caused by sharp objects, being hit by falling objects, poisoning, suffocation, drowning and so forth. Violent events have been classified here as self-inflicted injury/suicide attempt, assault, maltreatment and legal intervention.
All victims of accidents and violence cared for during the shift selected in the survey period in each selected establishment are considered eligible to be interviewed. People are excluded if they have gone to the same service two or more times to get care for the same cause, as are people with follow-up appointments and complications occurring during health care.
Data collection
Data are collected using the standard “Violence and Accident Form” prepared by members of the CGDANT/DANTPS/SVS/MS team, researchers, consultants, technical staff as well as staff from other Ministry of Health departments and universities. The version of the form used in the 2014 VIVA Survey is provided in the supplementary material available in the electronic version of this article (Appendix B).2,4,5,14
The interviews are administered by duly trained Nursing and Medicine undergraduate students and health professionals supervised by managers and technical staff of the Health Departments of the municipalities included in the survey and also in partnership with the State Health Departments.2,4,5,14 Whenever a person was admitted to the emergency care service as a result of an accident or violence, the interviewers approached the victim, or the person accompanying them in the case of people under 18 years of age or the victim being unable to answer, to request permission and to begin the interview.
Quality control
CGDANT holds training sessions on the survey procedures for managers and technical staff of the municipal and state Health Departments involved. In turn, the course participants take on the commitment to coordinate the survey at local level and to train the local team together with the interviewers and the field supervisors.
The “Interviewer’s Manual” is provided during the training sessions. It provides information about the survey; the attributions of the local coordinator, supervisor and interviewer; general guidelines on the interview; as well as instructions for filling in the data collection form.
In order to minimize losses and refusals, the supervisors keep a “Field Diary”, which is a spreadsheet for monitoring the work done and checking whether all individuals cared for were in fact approached by the interviewers, by comparing the “Field Diary” data with the completed data collection forms. If a loss is identified, the interviewers check why the patient has not been interviewed and, if the reason is that they refused, the team approaches the patient again using a different interviewer to the one who made the first attempt, or the supervisor in charge, in order to try to reverse refusals. The total number of individuals external causes per shift, the total number of interviews, as well as refusals and losses, are recorded in the “Field Diary”.
The team of each municipality taking part in the survey records the data using Epi Info 3.5.1 software. The data are then transferred to the Ministry of Health via e-mail. The CGDANT team checks each file for consistency and double counting, using Rec Link III, version 3.1.6 (Figure 2 ).2,4,5,14
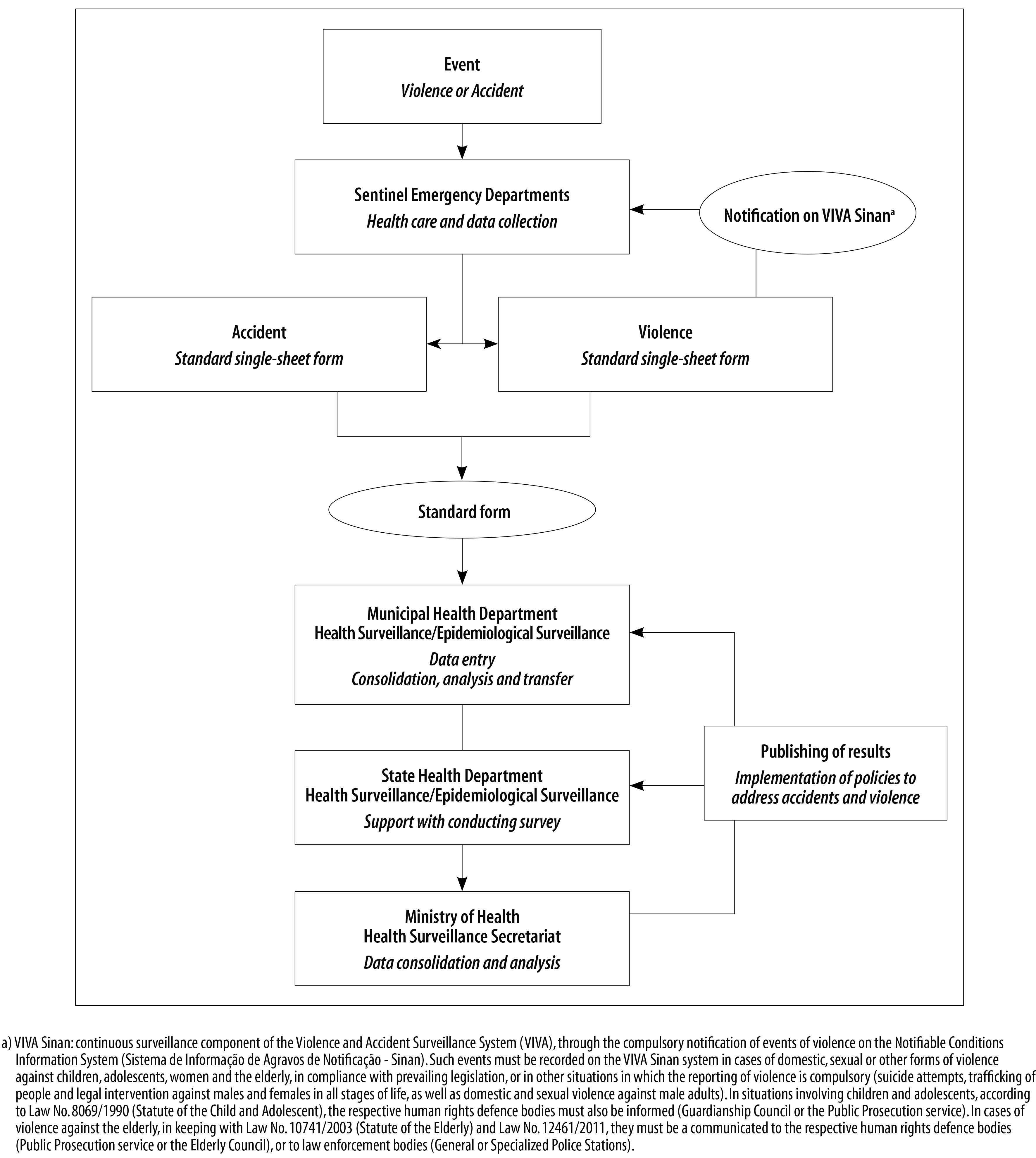
Figure 2 - Data collection, sending, processing and publishing flowchart - Violence and Accidents Survey Conducted in Brazilian Sentinel Emergency Departments (VIVA Survey), 2014
The databases sent by each service taking part in the survey are checked for consistency and double counting. If necessary, databases are returned to the participating services for correction. Finally, they are consolidated into a single VIVA Survey database.
The “VIVA Application Manual” has been produced to assist with data entry and data analysis, with updated versions for each year the survey has been conducted, in keeping with the characteristics of the questionnaire. In 2014 the application reached its fifth version: “VIVA 5.0".
Variables
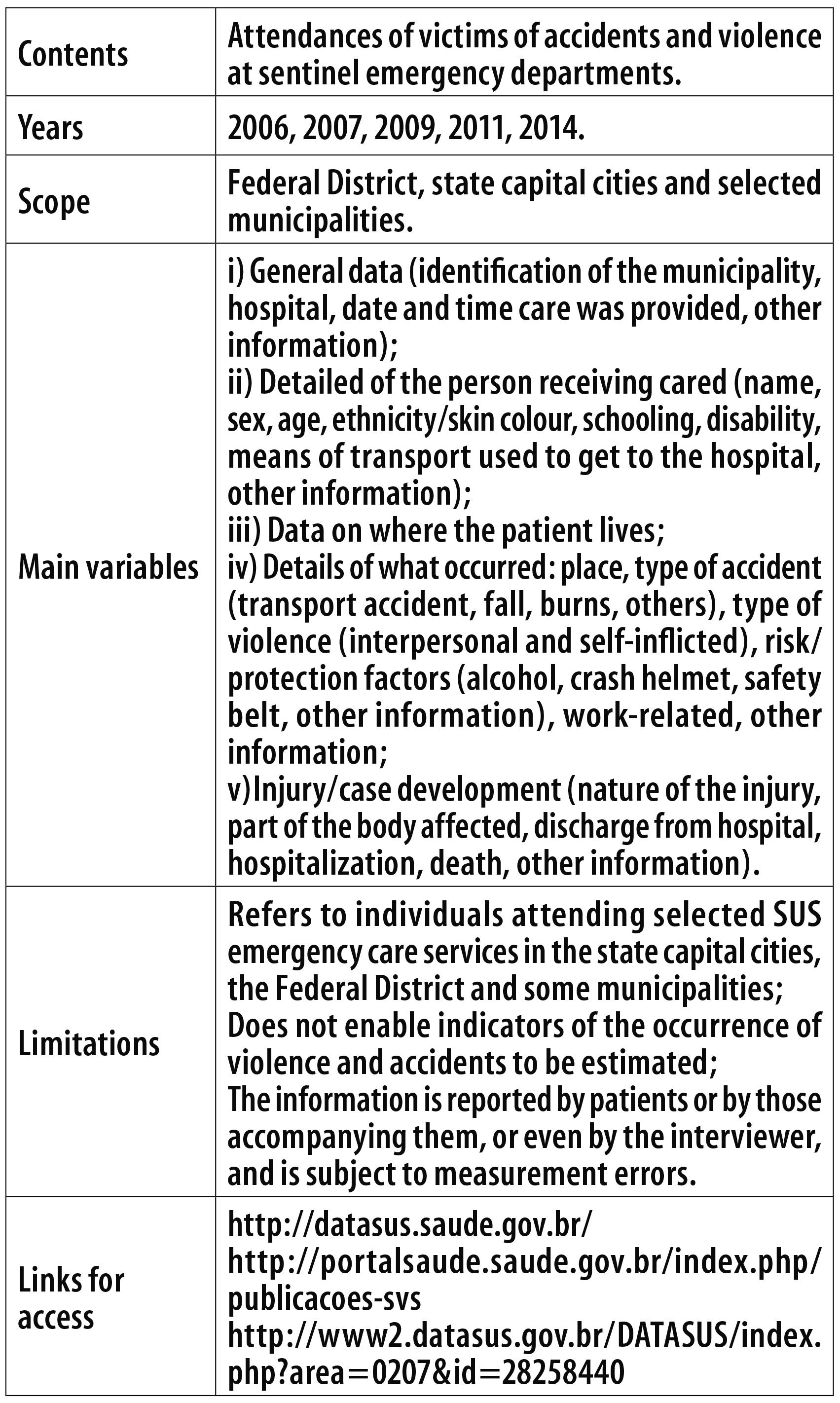
The variables on the standard form are distributed over the following blocks: i) General data (identification of the municipality, hospital, date and time care was provided, other information); ii) Details of the person receiving care (name, sex, age, race/skin color, schooling, means of transport used to get to the hospital, other information); iii) Data on where the individual lives; iv) Details of what occurred (place, type of accident, type of violence, risk factors, work-related, other information); v) Injury/case development (nature of the injury, part of the body affected, discharge from hospital, hospitalization, death, other information).2,4,5,14 These variables underwent slight alterations from one survey to the next in order to enhance them and to meet service management demands, such as inclusion/exclusion of variables and adjustments to wording or categories. The details of these alterations are provided in the supplementary material available in the electronic version of this article (Appendix C).
Notably, in 2014, the consumption accident variable - referring to an accident occurring during the normal use of a product or service - was included, as well as the type of product involved in this type of accident.
Uses
The VIVA Survey data inform the building of indicators which enable the description of the characteristics of accidents and violence, their probable perpetrator in the case of assault, and the investigation of risk/protection factors associated with the event.2,4,5,14
The following indicators are highlighted here. They can be calculated according to sex and age range:
- Proportion of attendances due to accidents
- Proportion of attendances due to transport accidents
- Proportion of attendances due to falls
- Proportion of attendances due to falls at home
- Proportion of attendances due to falls in public thoroughfares
- Proportion of attendances due to burns
- Proportion of attendances due to other accidents
- Proportion of attendances due to violence
- Proportion of attendances due to self-inflicted injuries
- Proportion of attendances due to assault
- Proportion of attendances due to assault at home
- Proportion of attendances due to assault in public thoroughfares
- Proportion of attendances due to violence/accidents among victims of violence/accidents who had consumed alcoholic beverages
- Proportion of attendances due to violence/accidents happening at work/on the way to work
- Proportion of attendances due to transport accidents according to the use of safety equipaments (seat belt, child transport restraint device, helmet, to other use
Having knowledge of the profile of the events and the victims of violence/accidents attending emergency care services enables contributions to be made to the organization of the Emergency Care Network, as well as to the organization of care provided at health centres to patients brought by the Emergency Mobile Care Service (Serviço de Atendimento Móvel de Urgência - Samu).
Updates
Figure 3 shows the main events related to the implementation and updates of VIVA Survey, having as a starting point the creation of the Department of Health Analysis and Situation and CGDANT in the Ministry of Health´s structure in 2003, as a landmark to structure the Surveillance of Noncommunicable Diseases and, furthermore, the organization of surveys.
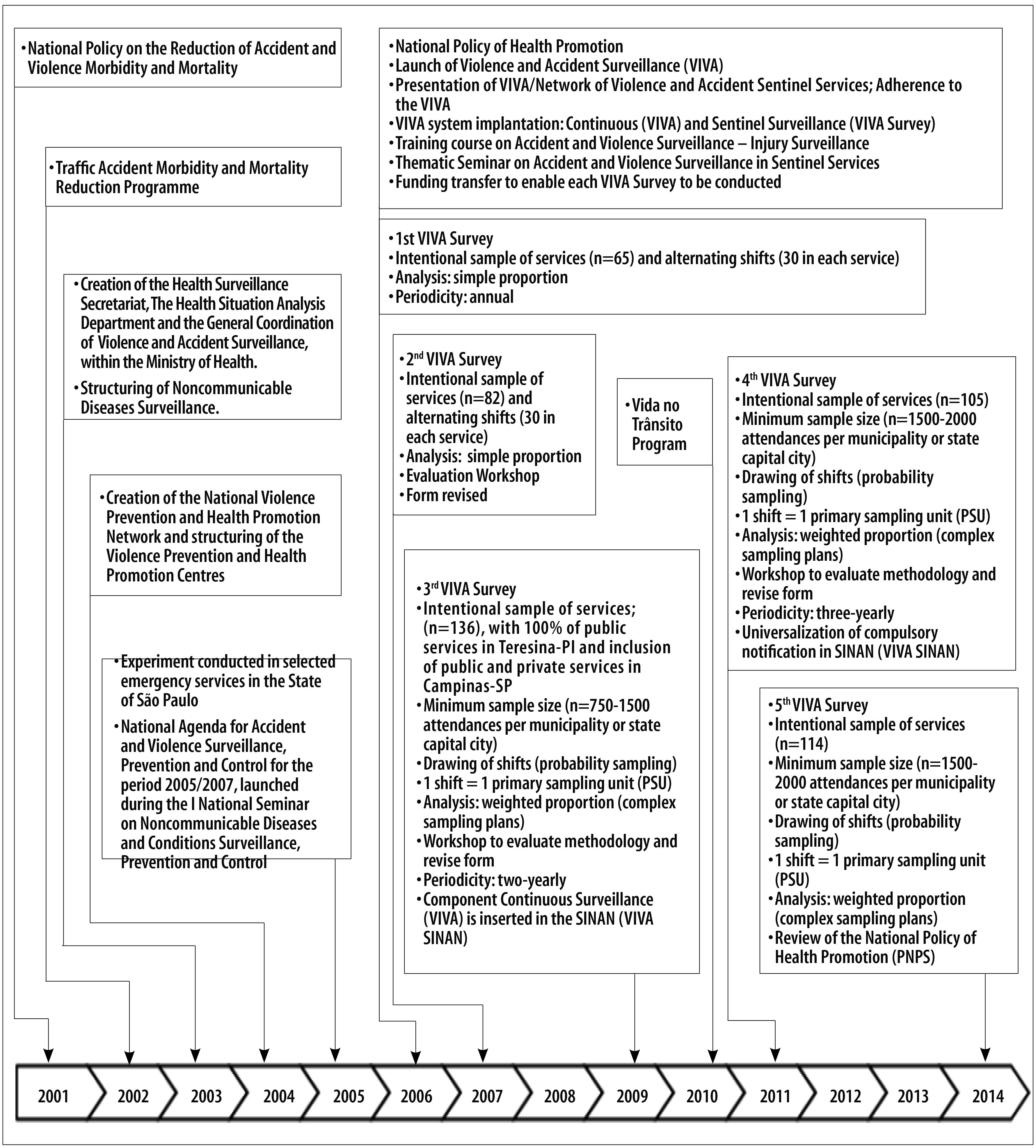
Figure 3 - Timeline of the Violence and Accidents Survey Conducted in Brazilian Sentinel Emergency Departments (VIVA Survey), 2001- 2014
One such highlight in 2005 in the structuring of the Surveillance of Noncommunicable Diseases was the National Agenda for Accident and Violence Surveillance, Prevention and Control for the period 2005/2007, launched during the I National Seminar on Noncommunicable Diseases Surveillance, Prevention and Control.
The first VIVA Survey took place in 2006 with an intentional sample of services (n=65) and alternating shifts (30 shifts in each service). In 2007 the Survey continued with the intentional sample of services (n=82) and alternating shifts (30 shifts in each service). In 2009, the random sampling of shifts was implemanted and weighting procedures were adopted in the analysis (complex sampling plans). In 2011 and 2014 the same sampling procedures were used as in 2009. In all years in which the survey was conducted the forms underwent enhancements, whilst seeking to ensure that the ability to compare the variables was maintained (Figure 3).
Data analysis
As the data is derived from a complex sampling plan, the PSU, stratum and weighting variables should be considered, as these define the VIVA Survey planning variables. These variables are available in the database and should be considered in the analyses.
Limitations
With regard to external validity, it is noteworthy that the population covered by the study is comprised of individuals attending selected SUS emergency care services in the state capital cities, the Federal District and some selected municipalities during the data collection period. The findings cannot therefore be extrapolated to the national context. Nor is it possible to obtain measures of the occurrence of external causes since the sample is not population-based.
There are, however, advantages in spreading the sample over the Brazilian state capital cities, given the large number of sentinel emergency departments spread over the country.20 Moreover, it can be stated that to a great extent the attention provided to victims of accidents and violence in SUS emergency care services is representative of this kind of attention in the state capital cities. Approximately three quarters of the Brazilian population use SUS services exclusively,21 and the majority of hospitalizations occur in a SUS-affiliated hospitals.21 Furthermore, the vast majority of private hospitals only offer emergency services for clinical causes. Patient care flow for victims of external causes in Brazil is determined by Ministry of Health ordinances, which also define that the Mobile Emergency Care Service (Samu) must take its patients initially to public emergency care services.22,23
The information is reported by patients or by those accompanying them, or even by the interviewer, and is subject to measurement errors. In cases of violence, for instance, this fact may result in some cases of assault being ignored due to their being incorrectly classified as accidents, as well as in errors in classifying the probable perpetrators of violence. Some people who suffer domestic violence, for example, may wish to omit the fact for a diversity of reasons, such as fear, guilt, shame and so forth.
Reserve samples were not drawn in the 2014 survey, this being a procedure used in some of the previous surveys which enabled the minimum size of the sample to be achieved. This resulted in a low number of interviews in some municipalities.
Ethical aspects
In accordance with the recommendations of National Health Council Resolution No. 196/1996, the research projects for all the VIVA Surveys performed so far were submitted to and approved by the National Research Ethics Committee as per Reports number 286/2007, 764/2009, 006/2011 and 735.933/2014.2,4,5,14
Owing to the fact that the survey is a specific national epidemiological surveillance action, the signing of the Informed Consent Form was replaced with verbal consent given by the participant or the person responsible for them and this was recorded in a specific field on the data collection form.
All the surveys ensured total anonymity and privacy for participants, health professionals and service managers where the survey was conducted. Survey participants could stop participating at any time, with no detriment whatsoever to them or their family.
Access
The VIVA Survey data are public domain data and can be accessed at the DATASUS website (http://datasus.saude.gov.br/). Use the acesso à informação icon to select Tabnet and then select inquéritos e pesquisas. In the option VIVA - Vigilância de Violências e Acidentes, the survey year can be selected. The system generates a tabulator. The Technical Note available on this website provides information about the survey and the variables available for tabulation.
DANTPS/SVS/MS publishes a book about each VIVA Survey containing the results of the analyses. This can be accessed at: http://portalsaude.saude.gov.br/index.php/publicacoes-svs.
Requests for other information should follow the procedure provided for by Law No. 12527, dated 18/11/2011 and known as the Information Access Law,24 which determined the rules for accessing information from public bodies, state companies and related bodies. With regard to the Federal Government, the on-line Electronic Citizens’ Information System (e-SIC) centralizes requests for information and is available at http://www.acessoainformacao.gov.br/. Users must register before being able to request information. Once the Ministry of Health has received the request it must reply within twenty days.
The 2014 VIVA Survey data were not available on the website at the time this article was approved for publication.
Acknowledgements
We extend our special thanks to DR Nilza Nunes da Silva, who has collaborated with all the VIVA Surveys in the sample selection process, and to DR Otaliba Libânio de Morais Neto, who contributed to the conception and structuring of SUS Violence and Accident Surveillance (VIVA) and lead this process during the earlier surveys.
REFERENCES
1. Ministério da Saúde (BR). Projeto de Vigilância de Violências e Acidentes - VIVA/Rede de Serviços Sentinelas de Violências e Acidentes. Brasília: Ministério da Saúde; 2006. (Mimeo). [ Links ]
2. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Viva: Vigilância de Violências e Acidentes, 2006 e 2007. Brasília: Ministério da Saúde ; 2009 [citado 2016 nov 3]. (Série G. Estatística e Informação em Saúde). Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/viva_vigilancia_violencias_acidentes.pdf [ Links ]
3. Gawryszewski VP, Silva MMA, Malta DC, Mascarenhas MDM, Costa VC, Matos SG, et al. A proposta da rede de serviços sentinela como estratégia de vigilância de violências e acidentes. Cienc Saude Coletiva. 2006;11 supl:1269-78. [ Links ]
4. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Viva: Vigilância de Violências e Acidentes, 2008 e 2009. Brasília: Ministério da Saúde ; 2010 [citado 2016 nov 3]. (Série G. Estatísticas e Informação em Saúde). Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/viva_2008_2009_violencias_acidentes.pdf [ Links ]
5. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise de Situação de Saúde. Viva: Vigilância de Violências e Acidentes, 2010 e 2011. Brasília: Ministério da Saúde ; 2011 [citado 2016 nov 3]. (Série G. Estatísticas e Informação em Saúde). Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/viva_2009_2011_versao_eletronica.pdf [ Links ]
6. Ministério da Saúde. Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos Não Transmissíveis e Promoção da Saúde. Viva: Vigilância de Violências e Acidentes, 2011 e 2012. Brasília: Ministério da Saúde ; 2016 [citado 2016 nov 3]. Disponível em: Disponível em: http://portalsaude.saude.gov.br/images/pdf/2016/junho/14/viva-2011-2012-2jun16-isbn-finalissimo.pdf [ Links ]
7. Brasil. Ministério da Saúde. Portaria nº 737/GM, de 16 de maio de 2001. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2001 mai 18;Seção 1:3. [ Links ]
8. Brasil. Ministério da Saúde. Portaria nº 936, de 18 de maio de 2004. Dispõe sobre a estruturação da Rede Nacional de Prevenção da Violência e Promoção da Saúde e a Implantação e Implementação de Núcleos de Prevenção à Violência em Estados e Municípios. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2004 mai 18;Seção 1:52. [ Links ]
9. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Portaria MS/GM nº 687, de 30 de março de 2006. Aprova a Política de Promoção da Saúde. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2006 mar 31;Seção 1:138. [ Links ]
10. Brasil. Portaria nº 1.356, de 23 de junho de 2006. Institui incentivo aos estados, ao Distrito Federal e aos municípios para a Vigilância de Acidentes e Violências em Serviços Sentinela, com recursos da Secretaria de Vigilância em Saúde (SVS). Diário Oficial da República Federativa do Brasil, Brasília (DF), 2006 jun 26; Seção 1:49. [ Links ]
11. World Health Organization. World report on violence and health. Geneva: World Health Organization; 2002. [ Links ]
12. WHO. World Health Organization. Global status report on violence prevention 2014. Geneva: World Health Organization ; 2014. [ Links ]
13. World Health Organization. Injury surveillance guidelines. Geneva: World Health Organization ; 2001. [ Links ]
14. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos não Transmissíveis e Promoção da Saúde. Viva: vigilância de violências e acidentes, 2013 e 2014. Brasília: Ministério da Saúde ; 2016. No prelo, 2016. [ Links ]
15. Kish L. Survey Sampling. New York: John Wiley & Sons; 1965. [ Links ]
16. Silva NN. Amostragem probabilística: um curso introdutório. 2 ed. São Paulo: Editora da Universidade de São Paulo; 2001. [ Links ]
17. Bernal R, Silva NN. Cobertura de linhas telefônicas residenciais e vícios potenciais em inquéritos epidemiológicos. Rev Saude Publica. 2009 mai-jun;43(3):421-6. [ Links ]
18. United Nations. Secretariat. Department of Economic and Social Affairs. Household sample surveys in developing and transition countries. New York: United Nations; 2005. p. 27-28. [ Links ]
19. Organização Mundial da Saúde. Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde. 10ª revisão. São Paulo: EDUSP; 2000. [ Links ]
20. Luz TCB, Malta DC, Sá NNB, Silva MMA, Lima-Costa MF. Violências e acidentes entre adultos mais velhos em comparação aos mais jovens: evidências do Sistema de Vigilância de Violências e Acidentes (VIVA), Brasil. Cad Saude Publica. 2011 nov;27(11):2135-42. [ Links ]
21. Ministério do Planejamento, Orçamento e Gestão (BR). Instituto Brasileiro de Geografia e Estatística. Diretoria de Pesquisas. Coordenação de Trabalho e Rendimento. Pesquisa Nacional de Saúde 2013: percepção do estado de saúde, estilos de vida e doenças crônicas: Brasil, Grandes Regiões e Unidades da Federação. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2014 [citado 2016 nov 3]. Disponível em Disponível em ftp://ftp.ibge.gov.br/PNS/2013/pns2013.pdf [ Links ]
22. Brasil. Ministério da Saúde. Portaria nº 2.048, de 05 de novembro de 2002. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2002 nov 12; Seção 1:32. [ Links ]
23. Brasil. Ministério da Saúde. Portaria nº 1.010, de 21 de maio de 2012. Redefine as diretrizes para a implantação do Serviço de Atendimento Móvel de Urgência (SAMU 192) e sua Central da Rede de Atenção às Urgências. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2012 mai 22;Seção 1:87. [ Links ]
24. Brasil. Lei nº 12.527, de 18 de novembro de 2011. Regula o acesso a informações previsto no inciso XXXIII do art. 5o, no inciso II do § 3o do art. 37 e no § 2o do art. 216 da Constituição Federal; altera a Lei no 8.112, de 11 de dezembro de 1990; revoga a Lei no 11.111, de 5 de maio de 2005, e dispositivos da Lei no 8.159, de 8 de janeiro de 1991; e dá outras providências. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2011 nov 18;Seção 1:1. [ Links ]
Received: October 10, 2016; Accepted: October 29, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
