










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.2 Brasília abr./jun. 2017
http://dx.doi.org/10.5123/s1679-49742017000200004
ORIGINAL ARTICLE
Coverage trends of the Information System on Live Births in Mato Grosso, Brazil, 2000 to 2012
1Universidade Federal de Mato Grosso, Faculdade de Enfermagem, Cuiabá-MT, Brasil
2Universidade Federal de Mato Grosso, Programa de Pós-Graduação em Enfermagem, Cuiabá-MT, Brasil
3Universidade Federal de Mato Grosso, Instituto de Saúde Coletiva, Cuiabá-MT, Brasil
OBJECTIVE:
to analyze the coverage trends of the Brazilian Information System on Live Births (Sinasc) in the state of Mato Grosso and its Health Regions, in the period from 2000 to 2012.
METHODS:
this is a time series study, coverage was calculated by the ratio between the number of live births registered in the system and the number estimated by the Brazilian Institute of Geography and Statistics (IBGE); the trends were analyzed using polynomial regression models.
RESULTS:
Sinasc coverage in Mato Grosso in the studied period presented increasing trend, with a median of 94.9%; Araguaia Xingu region presented coverage lower than 90% in the period; most of the regions presented coverage increasing trends, except for Baixada Cuiabana, Centro Norte and Vale do Peixoto.
CONCLUSION:
Sinasc coverage in Mato Grosso was satisfactory and has been increasing in most of Health Regions.
Keywords: Vital Statistics; Information Systems; Live Birth; Time Series Studies
Introduction
The Brazilian Information System on Live Births (Sinasc) was created in 1990 in order to monitor aspects related to prenatal, childbirth and puerperal care. Its implementation occurred slowly and gradually in all Brazilian states. The Certificate of Live Birth (CLB) is a standardized, individual and mandatory document used all over the country for all live births to collect data for Sinasc.1,2
Sinasc is a tool with great potential to understand maternal and children health characteristics and for prenatal and childbirth care. It enables the health surveillance through identification of epidemiological profile, assessment and planning of actions capable of promoting improvement in the assistance quality.1,3 The knowledge on the number of live births is also important for calculating birth and fertility rates and maternal mortality ratio. Thus, this information system is essential for the proposition, monitoring and assessment of evidence-based health policies.2
The Brazilian Institute of Geography and Statistics (IBGE) is another source of information regarding the number of live births. The data provided by demographic censuses and the National Household Sample Surveys (PNAD) helps IBGE estimates the population size for all municipalities and macroregions of the country.1,2 However, these surveys only estimate the number of live births, which is a great limitation, due to their own characteristics and inherent differences between real counting and estimates.4
Despite some authors' considerations on underreporting of live births at Sinasc,2,5,6 this system presents many positive aspects, such as information on the health of mothers and newborns, especially where geographic access and information are limited and where researches with primary data are scarce, e.g., some regions in Mato Grosso State.
Sinasc coverage is related to its capacity to reach and capture the occurrence of births.7 After the system's implementation, its coverage was extended and became satisfactory in several Brazilian states.3,8,9 However, in some macroregions such as the North and the Northeast, underreporting of live births was observed in the period from 2000 to 2012.8,10
An assessment study carried out in Brazilian states and macroregions on the adequacy level of vital information systems - Mortality Information System (SIM) and Sinasc - between the three-year period of 1999-2001 and 2008-2010, showed that the information coverage and regularity improved in the first half of the 21st century, especially in regions that presented the worst adequacy of vital information: North and Northeast.11
In Mato Grosso State, Sinasc was standardized in 1997. Nonetheless, a certain shortage of analysis concerning this system coverage was observed. This study aims to analyze the coverage trends of the Brazilian Information System on Live Births in Mato Grosso State and its Health Regions in the period from 2000 to 2012.
Methods
This is a time series study conducted in the Mato Grosso State, which is formed by 141 municipalities and is divided into 16 Health Regions. The analysis comprised the total number of live births available in Mato Grosso's Sinasc, in the period from January 1st, 2000 to December 31st, 2012. The data were provided by the State Health Department.
Mato Grosso is the third biggest state in the country in territorial size, and the 19th most populous, accounting for 3,035,122 inhabitants in 2010. It corresponds to 1.58% of the Brazilian population and it has a population growth rate of 1.9% per year.12 Still according to the 2010 Population Census, approximately 82% of the state inhabitants lived in urban areas, and 1,485,587 were women, of which 999,639 (67.2%) were in reproductive age (10 to 49 years old).12 In the same year, the state had a Gross Domestic Product (GDP) per capita above R$20.500,0013 and its human development index (HDI) was the 11th among the 27 Brazilian federative units.14
Sinasc’s coverage percentage was calculated as the ratio between the number of live births recorded in Sinasc, according to childbirth per mother’s residence, and the estimated number of the resident population in the age group below one year old, for each analyzed year, according to IBGE data.15 All the ratios were calculated for the 16 Health Regions and for Mato Grosso State as a whole, using the following formula:

The Ministry of Health recommends that, in order to use Sinasc data in the direct calculation of health indicators, the system must reach at least 90% coverage.16,17 Thus, in this study the system's coverage was considered satisfactory when it presented values ≥90.0%.
In the descriptive statistics, we chose medians to summarize the historical series. Since we dealt with rates better represented by measures with non-parametric distribution, they were presented in tables, and in a geographic distribution map of the system's coverage medians (according to Health Regions); we considered the cut point of 90.0%. To do so, the ArcGis/ArcMap 10.2.2 software was used.
The trend analysis of Sinasc coverage was carried out in the software Statistical Package for the Social Sciences (SPSS), 18.0 version, through polynomial regression models in which the series' coverage percentages were considered as dependent variables (Y) and the studied years as independent variables (X).
In order to find a curve that best represented the relation between dependent and independent variables, the following polynomial regression models were tested:
Linear:
y = β0 + β1 x,
Quadratic:
y = β1 + β1 x + β2 x2,
Cubic:
y = β0 + β1 x + β2 x2 + β3 x3 e
Exponential:
y = β0 * exp (β1 * x) β↔ln(y) = ln (β0 ) + (β1 x)
The Y and X values represent the dependent and independent variables, respectively; β0, β1, β2 e β3 are the regression coefficients. A total of 17 polynomial regression models were built, having as dependent variable the coverage percentage of Sinasc in Mato Grosso and in each of its 16 Health Regions, and as independent variable, each year of the historical series comprised from 2000 to 2012. The polynomial regression model was considered capable of describing the relation between the dependent and independent variables when the p-value was <0.05; in situations when more than one model contemplated this condition, we chose the one that presented the lowest p-value; when the p-value was coincident, we chose the simplest model.
Even though the study was carried out exclusively with aggregate secondary data, the research project was submitted to the Committee of Ethics in Research of the Júlio Muller University Hospital/ Federal University of Mato Grosso and was approved in August 13th, 2014: Report No. 749.4067/14
Results
During the analyzed period, 643,349 live births were registered in the state of Mato Grosso. Of those, 49,478 live births occurred in the first year of the historical series (2000) and 51,256, in the last year (2012), and more than half of the births that occurred in the state during the studied years were concentrated in three Health Regions: "Baixada Cuiabana", "Sul Mato-Grossense" and "Teles Pires".
Figure 1 shows the distribution of the medians of Sinasc coverage in Mato Grosso, of 94.9% in the analyzed period. Most of the state's Health Regions also presented satisfactory coverage medians (≥90.0%).
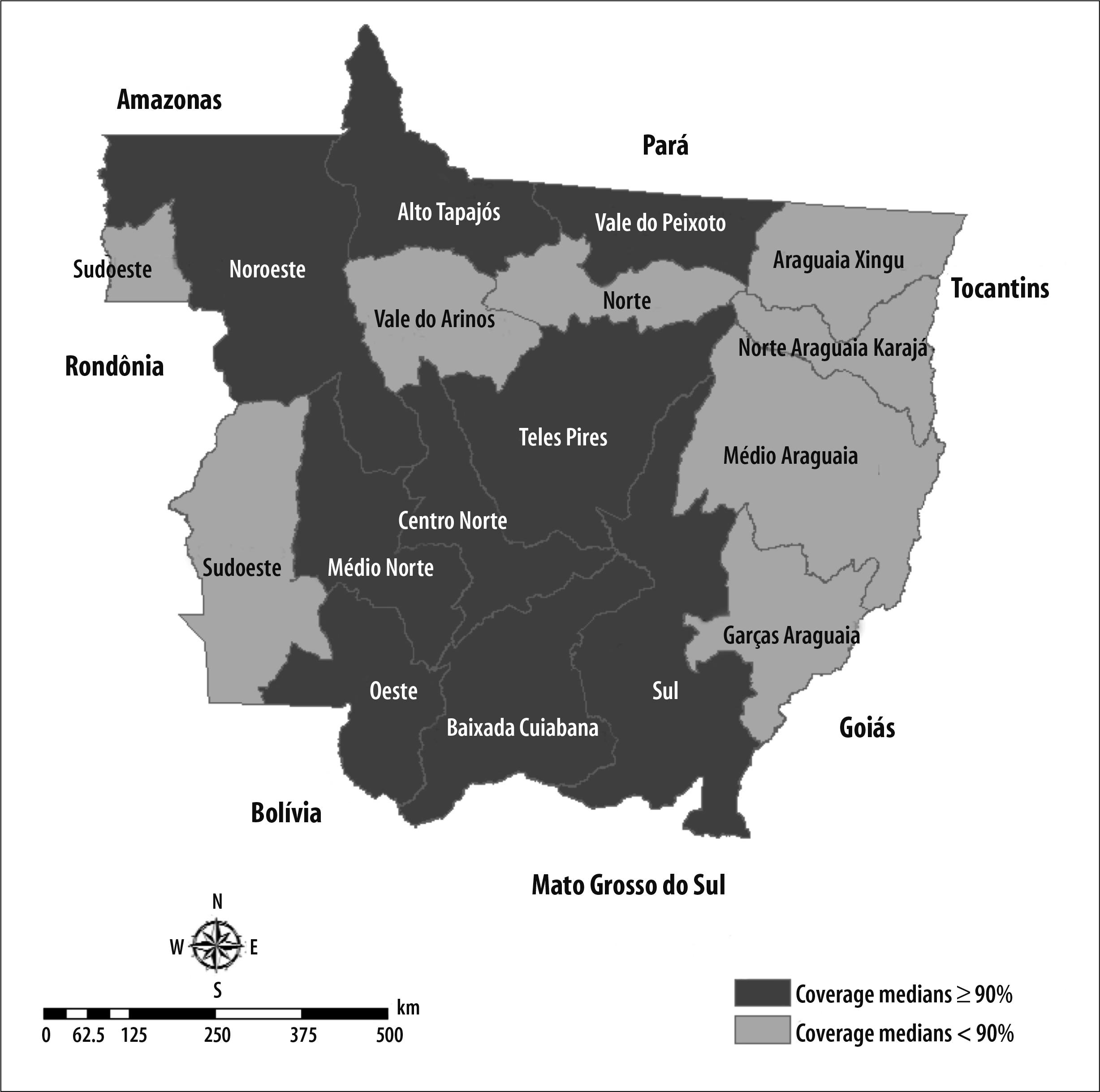
Figure 1- Health Regions and coverage medians of the Brazilian Information System on Live Births (Sinasc) in the state of Mato Grosso, 2000-2012
The Health Regions that showed medians below 90.0% were "Araguaia Xingu", "Garças Araguaia", "Médio Araguaia", "Norte Araguaia Karajá", "Norte Mato-Grossense", "Sudoeste Mato-Grossense" and "Vale do Arinos". Of those, "Garças Araguaia", "Médio Araguaia", "Norte Araguaia Karajá", "Norte Mato-Grossense", "Sudoeste Mato-Grossense" and "Vale do Arinos" presented coverage percentage below 90.0% in more than half of the historical series; "Araguaia Xingu" showed percentages under 90.0% in all assessed years (Table 1).
Table 1 - Coverage percentage of the Brazilian Information System on Live Births (Sinasc) in the state of Mato Grosso and its Health Regions, 2000-2012

Regarding the historical trends, the state of Mato Grosso (Figure 2) as well as the regions of "Garças Araguaia", "Médio Araguaia", "Norte Araguaia Karajá", "Norte", "Oeste", "Sudoeste" and "Sul Mato-Grossenses" presented increasing and statistically significant coverage trends, despite the decrease from 2005 to 2007. The Health Regions of "Baixada Cuiabana", "Centro Norte" and "Vale do Peixoto" presented decreasing and statistically significant coverage trends (Table 2).
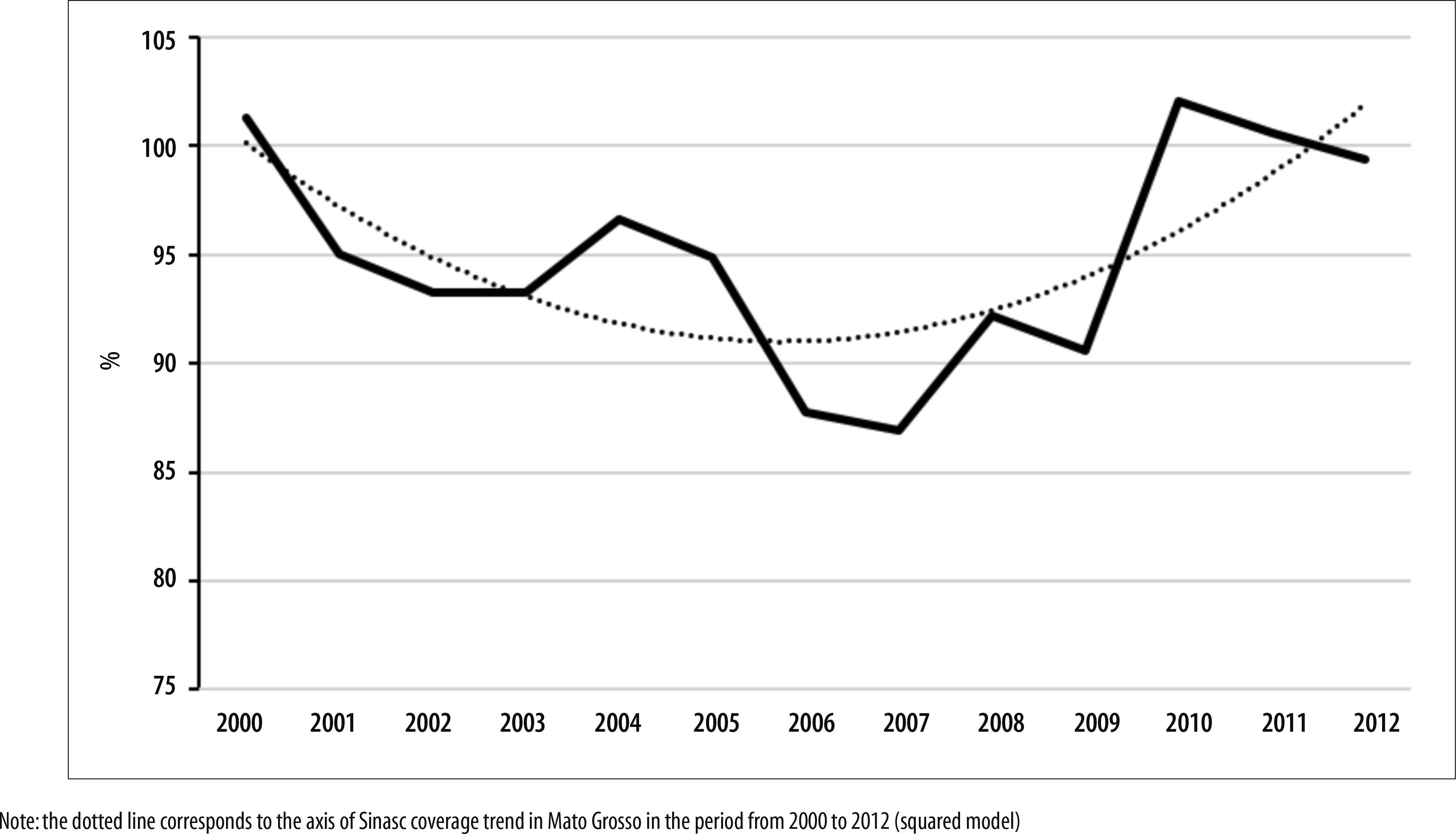
Figure 2 - Coverage trend of the Brazilian Information System on Live Births (Sinasc) in the state of Mato Grosso, 2000-2012
Table 2 - Trend analysis of the coverage percentage of the Brazilian Information System on Live Births (Sinasc) in Mato Grosso and its Health Regions, 2000-2012
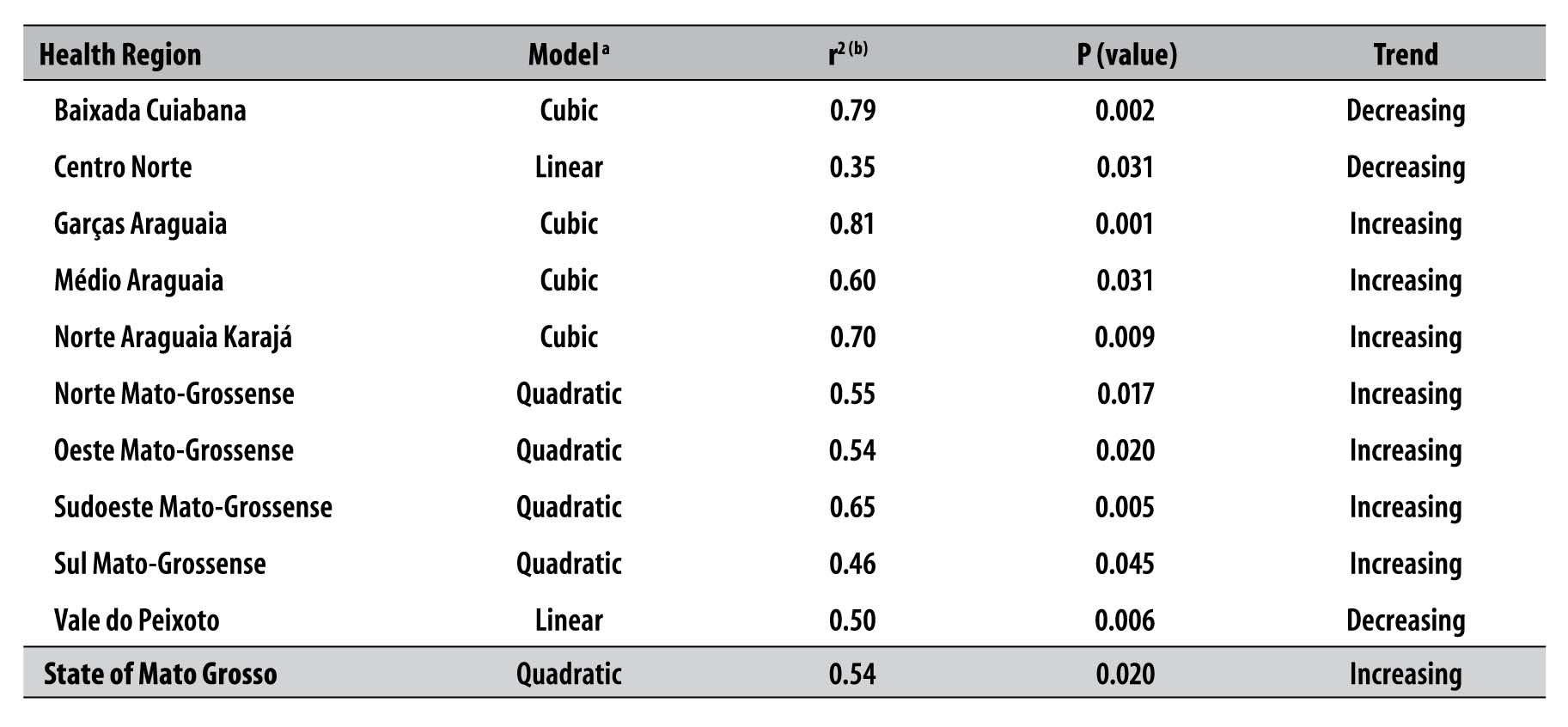
a) Linear polynomial regression models (y = β0 + β1 x), quadratic (y = β0 + β1 x + β2 x2) and cubic (y = β0 + β1 x + β2 x2 + β3 x3)
b) r2: explanation coefficient
Although the regions of "Alto Tapajós", "Araguaia Xingu", "Médio Norte Mato-Grossense", "Noroeste Mato-Grossense", "Teles Pires" and "Vale do Arinos" have not presented a polynomial regression model capable of explaining the coverage percentage trend during the analyzed period (trend analysis not included in Table 2), all of them showed coverage significant decrease, in comparison with the year 2000 (Table 1).
Discussion
This study showed that Sinasc coverage in Mato Grosso reached satisfactory percentages - above 90.0% - in most of the studied period, with increasing trends in the analyzed years. The analysis through polynomial regression models showed a decrease in coverage in the early years, with trends change after 2007, and growth maintenance up to the historical series final years. The result resembles to other regions of the country, and outnumbers birth registers in the system with regard to data released by IBGE. This can be seen in the expansion of Sinasc coverage of all Brazilian macroregions.18
The regions of "Baixada Cuiabana", "Sul Mato-Grossense", "Teles Pires", "Alto Tapajós" and "Oeste Mato-Grossense" also showed satisfactory coverage, since all of them presented medians near 95%. On the other hand, the Health Region of "Baixada Cuiabana" showed decreasing coverage trend in the polynomial regression analysis. The state's most populous towns are in this region, including the capital Cuiabá and Várzea Grande; the latter is the second largest city of Mato Grosso in number of inhabitants.15 Both municipalities comprise health care services of medium to high complexity and have the highest HDI in the state,19 although, paradoxically, they are located in the health regional center that presents the worst coverage of the Family Health Strategy (FHS), admittedly one of the most effective policies for maternal-infant health improvement and information systems coverage, as Sinasc.20,21
The municipalities of Rondonópolis, Sinop, Sorriso, Lucas do Rio Verde and Nova Mutum, which present the highest income per capita and excellent Family Health Strategy (FHS) coverage are located in the regions of "Sul Mato-Grossense" and "Teles Pires". In addition, they belong to the agribusiness belt, presenting good average education levels. These factors are associated with better life quality and satisfactory Sinasc coverage.20,22
The satisfactory median coverage in the "Alto Tapajós" region, specifically in the municipalities of Alta Floresta, Apiacás and Nova Monte Verde, among others, all located in the Amazon biome, need to be considered, as well as the "Oeste Mato-Grossense" region, with the municipalities of Cáceres, Mirassol D’Oeste and São José de Quatro Marcos. The Health Region of "Alto Tapajós" presented the third lowest GDP per capita among the state's regions, and HDI under the state average.19,22 A possible explanation for the quality of Sinasc coverage in the "Alto Tapajós" region is that about 80.0% of its population are assisted by Family Health teams, despite its unequal distribution. In the "Oeste Mato-Grossense" region, the smallest municipalities are satisfactorily assisted by the Family Health Strategy. On the other hand, the two largest municipalities in that region, Cáceres and Mirassol D'Oeste, present Family Health team coverage below 50%.20
The decreasing coverage trends presented by the Health Regions of "Centro Norte" and "Vale do Peixoto" are noteworthy. Despite the difficulty to generalize due to the heterogeneity between the municipalities which belong to these two regions, the fact that they present GDP per capita and HDI below the state average is evident, except for the municipality of Diamantino, which presents mixed characteristics between the ancient Mato Grosso towns and those that served agribusiness expanion.15 Vale do Peixoto has the highest Family Health Strategy coverage when comparing to the other regions of Mato Grosso.20 However, most of its municipalities are located at the Amazon biome, where there are fewer opportunities to access health services. This partly explains the low Sinasc coverage in those regions.
We identified flaws in the coverages of Sinasc in the regions of "Araguaia Xingu", "Garças Araguaia", "Médio Araguaia", "Norte Araguaia Karajá", "Norte Mato-Grossense", "Sudoeste Mato-Grossense" and "Vale do Arinos". If, on the one hand, their coverage medians were all below 90%, on the other hand, most of these regions showed increasing trends on Live Births underreporting, except for "Araguaia Xingu" and "Vale do Arinos", which did not present a polynomial regression model capable of describing Sinasc coverage behavior in the historical series. The aforementioned regions' municipalities present the lowest HDI and GDP per capita of Mato Grosso State.19,22 They are also part of a large territorial extension that is far from the capital. Another characteristic of these regions is the widespread presence of indigenous peoples in their population, with villages difficult to access by primary health care services and, therefore, presenting child births and deaths without Certificate of Live Birth (CLB) or Death Certificate (DC), which contributes to underreporting and decrease of Sinasc coverage percentage.
A similar reality was brought to light by a research that assessed the quality of Live Births registrations in the Brazilian Northeast states in 2000, when they found heterogeneous coverage percentage among some microregions of the same state.8 This finding was reassured by a research carried out in São Luís, capital of Maranhão State, where the authors claim to have local, regional and state differences regarding Sinasc coverage and quality.23
Concerning socio-demographic indicators, we need to consider the effect of the families' individual income, as well as the skin color/ethnicity classification, sometimes recognized as low quality predictive factors of birth statistics. A research carried out in 2008, aiming to assess Sinasc coverage in Vale do Jequitinhonha, in the state of Minas Gerais, also found a different system's coverage percentage among the municipalities in that region: in the smaller municipalities and in underdeveloped regions, there was higher Live Births underreporting and simultaneous conductions of inadequate local interventions concerning maternal-infant health.18 The same authors related the Sinasc low quality coverage to problems that went from the lower capacity of these small municipalities' to performing active search, reporting and typing of Live Birth Certificates, to a lack of integration between local and state management health levels and lack of control of the information flow.18
It is possible that some variations in the adequacy of vital information systems are related to both the network's local peculiarities, and to information register and processing.24 Considering that the calculation of the ratio between Live Births registered in Sinasc and the live births estimated by IBGE is carried out based on births by mother's residence instead of birth place, and the fact that some pregnant women migrate to other municipalities seeking for better conditions and assistance during childbirth (when the mother's residence address is not always the one declared in the Live Birth Certificate), this situation may also reflect underreporting of Sinasc coverage in these regions.
Still, it is worth mentioning the satisfactory Sinasc coverage as a possible reflection of health services decentralization, extension of local services in monitoring process, management and control of health information, and a greater training and commitment of policy-makers and technicians involved in the information production.25
This study analyzed just the dimension of Sinasc coverage. Other aspects, present in different steps of information process regarding live births, such as system's completeness and reliability, are also prone to assessment, which represent important quality elements.1,26 Despite some Brazilian states presenting low coverage of Sinasc, it is worth mentioning that most states reach a system coverage percentage above 90.0%.10 Moreover, the existence of coverage percentage discrepancy among Brazilian regions should be taken into consideration, especially when we compare the South and Southeast, whose coverage is satisfactory, with the North and Northeast, which presented coverage decrease in most states between 2011 and 2012.10 In 2012, the Midwest region states showed satisfactory coverage that varied from 99.4% in Mato Grosso to 102.6% in Goiás, 103.1% in Mato Grosso do Sul and 111.2% in the Federal District.27
Some observations regarding trend series studies should be made. Complicating factors, such as the presence of cyclical and seasonal variations, might be hard to estimate or remove. The models selection is equally hard to decide and interpret. In this study, some decreasing trends were better explained by the linear model, which is the case of "Centro Norte" and "Vale do Peixoto" Health Regions. They pointed out to a constant worsening of Sinasc coverage in those regions. In the other Health Regions, where the selected models were quadratic and cubic, the inconstant aspect in the execution of public health policies and services, as well as the heterogeneous and peculiar situations of each region sometimes indicate an improving coverage, sometimes, the opposite. However, it is important to highlight the fact that most Health Regions in Mato Grosso revealed an increase in Sinasc coverage in the final years of the historical series.
Some limitations in the use of coverage indicators must be considered. There may have been some oscillation in the coverage calculation, since the indicator's denominator uses the IBGE births estimate, which was based on population projections to which the fertility rate is taken into consideration - and have been presenting reduction in the country. This way, a possible overestimate of the population under one year of age cannot be crossed out, causing an apparent decrease of Sinasc coverage.4 From 2005 to 2007, most Brazilian regions presented coverage reduction, a fact also observed in Mato Grosso in the last three years of the historical series. Data underreporting and low quality seem to be common in similar health information systems in many other countries.28
The sharp decrease in Sinasc coverage in Mato Grosso in 2006 and 2007 - and percentage decrease in the historical series - can be explained by the implementation of a new software for Sinasc in 2006. The delay for installing this new software version and the lack of human resources, among others, were pointed out as factors capable of generating structural problems for the process of the system's information production.29
Secondary data analysis, such as those from this study, might offer subsidies to planning, management and proposition of local policies meant to the system use. However, the results must be interpreted with caution, since they may be affected by the quality of information.
Essentially, coverage of the Brazilian Information System on Live Births - Sinasc - in Mato Grosso remained above 90% and presented an increasing trend during the analyzed period. The coverage oscillation observed indicate the need for adopting strategies capable of correcting possible capitation flaws, contributing to the promotion and management of information quality.
REFERENCES
1. Pedraza DF. Qualidade do Sistema de Informações sobre Nascidos Vivos (Sinasc): análise crítica da literatura. Cienc Saude Coletiva. 2012 out; 17(10):2729-37. [ Links ]
2. Gabriel GP, Chiquetto L, Morcillo AM, Ferreira MC, Bazan IGM, Daolio LD, et al. Avaliação das informações das Declarações de Nascidos Vivos do Sistema de Informação sobre Nascidos Vivos (Sinasc) em Campinas, São Paulo, 2009. Rev Paul Pediatr. 2014 jul-set;32(3):183-8. [ Links ]
3. Oliveira NC, Moura ERF, Silva CF. Perfil dos nascidos vivos de Maranguape-CE: a partir da série histórica de 2000 a 2003. Rev Rene. 2007 jan-abr;8(1):52-9. [ Links ]
4. Frias PG, Pereira PMH, Andrade CLT, Lira PIC, Szwarcwald CL. Avaliação da adequação das informações de mortalidade e nascidos vivos no Estado de Pernambuco, Brasil. Cad Saude Publica. 2010 abr;26(4):671-81. [ Links ]
5. Morais CAM, Takano OA, Souza JSF. Mortalidade infantil em Cuiabá, Mato Grosso, Brasil, 2005: comparação entre o cálculo direto e após o linkage entre bancos de dados de nascidos vivos e óbitos infantis. Cad Saude Publica. 2011 fev;27(2):287-94. [ Links ]
6. Gaíva MA, Modes PSSA, Stevanato JM. Fatores associados à prematuridade: análise dos dados do sistema de informações sobre nascidos vivos. Rev enferm UFPE online. 2015 dez;9(12):1110-7. [ Links ]
7. Mello Jorge MHP, Laurenti R, Gotlieb SLD. Avaliação dos sistemas de informação em saúde no Brasil. Cad Saude Colet. 2010;18(1):7-18. [ Links ]
8. Paes NA, Santos CSA. As estatísticas de nascimento e os fatores maternos e da criança nas microrregiões do Nordeste brasileiro: uma investigação usando análise fatorial. Cad Saude Publica. 2010 fev;26(2):311-22. [ Links ]
9. Silva RS, Oliveira CM, Ferreira DKS, Bonim CV. Avaliação da completitude das variáveis do Sistema de Informações sobre Nascidos Vivos - Sinasc - nos Estados da região Nordeste do Brasil, 2000 e 2009. Epidemiol Serv Saude. 2013 abr-jun;22(2):347-52. [ Links ]
10. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde (BR). Saúde Brasil 2013: uma análise da situação de saúde e das doenças transmissíveis relacionadas à pobreza. Brasília (DF): Ministério da Saúde; 2014. [ Links ]
11. Frias PG, Szwarcwald CL, Lira PIC. Avaliação dos sistemas de informações sobre nascidos vivos e óbitos no Brasil na década de 2000. Cad Saude Publica. 2014 out;30(10):2068-80. [ Links ]
12. Instituto Brasileiro de Geografia e Estatística. Censo Demográfico 2010: características da população [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2015 [citado 2014 mar 19]. Disponível em: Disponível em: http://www.ibge.gov.br/estadosat/perfil.php?sigla=mt [ Links ]
13. Ferreira MDP, Coelho AB. Desmatamento recente nos estados da Amazônia Legal: uma análise da contribuição dos preços agrícolas e das políticas governamentais. Rev Econ Sociol Rural. 2015 jan-abr;53(1):91-108. [ Links ]
14. Programa das Nações Unidas para o Desenvolvimento; Instituto de Pesquisa Econômica Aplicada; Fundação João Pinheiro. Atlas do desenvolvimento humano no Brasil [Internet]. Brasília: Programa das Nações Unidas para o Desenvolvimento; [2013][citado 2016 jun 03]. Disponível em: Disponível em: http://www.atlasbrasil.org.br/2013/pt/perfil_uf/mato-grosso [ Links ]
15. Ministério da Saúde (BR). Departamento de Informática do SUS. Informações de Saúde - Demográficas e Socioeconômicas - Censos (1980, 1991, 2000 e 2010), Contagem (1996) e projeções intercensitárias (1981 a 2012), segundo faixa etária, sexo e situação de domicílio [Internet]. Brasília: Ministério da Saúde; 2014 [citado 2016 jan 16]. Disponível em: Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?ibge/cnv/popmt.def [ Links ]
16. Rede Intergerencial de Informações para a Saúde (BR). Características dos indicadores: fichas de qualificação da RIPSA - 2012. Brasília (DF): Rede Intergerencial de Informações para a Saúde; 2012 [citado 2016 fev 15]. Disponível em: Disponível em: http://fichas.ripsa.org.br/2012/ [ Links ]
17. Frias PG, Pereira PMH, Vidal SA, Lira PIC. Avaliação da cobertura do Sistema de Informações Sobre Nascidos Vivos e a contribuição das fontes potenciais de notificação do nascimento em dois municípios de Pernambuco, Brasil. Epidemiol Serv Saude. 2007 abr-jun;16(2):93-101. [ Links ]
18. Girodo AM, Campos D, Bittencourt SDA, Szwarcwald CL, França EB. Cobertura do Sistema de Informações sobre Nascidos Vivos e potenciais fontes de informação em municípios de pequeno porte em Minas Gerais, Brasil. Rev Bras Saude Matern Infant. 2015 jul-set;15(3):317-24. [ Links ]
19. Programa das Nações Unidas para o Desenvolvimento. Ranking IDHM Municípios 2010 [Internet]. Brasília: Programa das Nações Unidas para o Desenvolvimento ; 2016 [citado 2016 jan 16]. Disponível em: Disponível em: http://www.pnud.org.br/atlas/ranking/Ranking-IDHM-Municipios-2010.aspx [ Links ]
20. Ministério da Saúde (BR). Departamento de Informática do SUS. Pacto de Atenção Básica: 2006: Mato Grosso [Internet]. Brasília: Ministério da Saúde ; 2007 [citado 2016 jan 16]. Disponível em: Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?pacto/2006/cnv/pacmt.def [ Links ]
21. Harzheim E, Duncan BB, Stein AT, Cunha CRH, Gonçalves MR, Trindade TG, et al. Quality and effectiveness of different approaches to primary care delivery in Brazil. BMC Health Serv Res. 2006 dez;6:156. [ Links ]
22. Ministério da Saúde (BR). Departamento de Informática do SUS. Renda média domiciliar per capita: Mato Grosso: 2010 [Internet]. Brasília: Ministério da Saúde ; [2010] [citado 2016 jan 16]. Disponível em: Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?ibge/censo/cnv/rendamt.def [ Links ]
23. Nunes FBBF, Prudêncio PS, Carvalho JFS, Mamede FV. Incompletude de informação de nascidos vivos em São Luís/MA no ano de 2012. Rev Pesqui Cuid Fundam (Online). 2016 jan-mar;8(1):3705-13. [ Links ]
24. Rodrigues M, Bonfim C, Frias PG, Braga C, Gurgel IGD, Medeiros Z. Diferenciais na adequação das informações de eventos vitais nos municípios de Pernambuco, 2006-2008. Rev Bras Epidemiol. 2012 jun;15(2)275-84. [ Links ]
25. Silva GF, Aidar T, Mathias TAF. Qualidade do Sistema de Informações de Nascidos Vivos no estado do Paraná, 2000 a 2005. Rev Esc Enferm USP. 2011 mar;45(1):79-86. [ Links ]
26. Pereira CCB, Vidal SA, Carvalho PI, Frias PG. Avaliação da implantação do Sistema de Informações sobre Nascidos Vivos (Sinasc) em Pernambuco. Rev Bras Saude Matern Infant. 2013 jan-mar;13(1):39-49. [ Links ]
27. Ministério da Saúde (BR). Departamento de Informática do SUS (BR). Estatísticas vitais. Brasília (DF): Ministério da Saúde ; 2014 [citado 2016 jan 16]. Disponível em: Disponível em: http://www2.datasus.gov.br/DATASUS/index.php?area=0205 [ Links ]
28. World Health Organization. World Health Statistics. Geneva: World Health Organization; 2010. [ Links ]
29. Guimarães EAA, Carmo RF, Loyola Filho AI, Meira AJ, Luz ZMP. O contexto organizacional do Sistema de Informações sobre Nascidos Vivos segundo profissionais de saúde do nível municipal. Rev Bras Saude Matern Infant. 2014 abr-jun;14(2):165-72. [ Links ]
* Manuscript based on Jaquelline Monte Stevanato’s PhD thesis, entitled ‘Quality of the Information System on Live Births in Mato Grosso’, presented to the Postgraduate Program in Nursing of the Federal University of Mato Grosso, Cuiabá-MT, in 2015. The main author received a Master’s scholarship by the Coordination for the Improvement of Higher Education Personnel (Capes)/ Ministry of Education (MEC).
Received: March 30, 2016; Accepted: August 15, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
