










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.2 Brasília abr./jun. 2017
http://dx.doi.org/10.5123/s1679-49742017000200007
ORIGINAL ARTICLE
Functional disability indicators and associated factors in the elderly: a population-based study in Bagé, Rio Grande do Sul, Brazil
1Universidade Federal de Pelotas, Faculdade de Enfermagem, Pelotas-RS, Brasil
2Universidade Federal de Pelotas, Departamento de Medicina Social, Pelotas-RS, Brasil
3Universidade Federal de Pelotas, Escola Superior de Educação Física, Pelotas-RS, Brasil
OBJECTIVE:
to estimate the prevalence of functional disability in basic and instrumental daily activities and associated factors in elderly who live in the urban area of Bagé-RS, Brazil.
METHODS:
this is a population-based cross-sectional study, conducted in 2008; functional disability was defined by basic and instrumental daily activities, using Katz index and Lawton and Brody scale; Poisson regression was used for crude and adjusted analyses.
RESULTS:
1,593 elderly individuals were investigated; the prevalence of disability for basic activities was of 10.6% (95%CI: 9.1;12.1) and of 34.2% (95%CI: 31.9;36.6) for instrumental activities; both disabilities were statistically associated to the increment of age, low education level, alcohol consumption, history of cerebrovascular diseases, cognitive impairment, hospitalization and home care.
CONCLUSION:
a high proportion of elderly presented functional disability; the outcomes were associated to the following variables: demographic, socioeconomic, behavioral, health status and use of health services.
Keywords: Aged; Disabled Persons; Activities of Daily Living; Cross-Sectional Studies
Introduction
Longevity is one of the greatest achievements of the world population, although it happens differently in each nation and socioeconomic context.1 In high-income countries, the increase in the proportion of older people in the population occurred gradually, following improvements in general living conditions. On the other hand, in low and middle-income countries, this increase has been occurring at an accelerated rate, posing a challenge for current social and health policies.2
The increase of noncommunicable diseases (NCDs) in a greater longevity scenario due to a better health status is one of the main implications entailed in the aging process, consequently changing the epidemiological profile. The growing number of elderly with functional disability is one of the consequences of such change, complicating their adaptation in a social environment and resulting in greater physical and mental vulnerability.3
Functional disability is the difficulty of performing daily activities in any area of one’s lifedue to a health problem.4 Functional disability is associated with multidimensional factors and may be evaluated according to two domains: basic activities of daily living (ADLs), that is, tasks related to self-care, such as feeding and bathing; and instrumental activities of daily living (IADLs), which are related to an individual's independence in society, such as shopping and using means of transport.5
In Brazil, the prevalence of disability among the elderly may vary from 6.9 to 47%, depending on population, considered age group and the assessment tools used.6-9 A study supported by the data from the National Household Sample Survey of 2003 shows that the main factors associated with disability in the elderly are female, older age, presence of chronic diseases, bad self-rated health, low income and low level of education.6
The loss of functional ability carries implications for the elderly, their families and the community. In addition to increasing the risk of death, it enhances the chances of hospitalization and expenditures for the Brazilian National Health System. Therefore, assessing the functional disability in the elderly and its associated factors is essential to elect appropriate interventions in order to help improving quality of life and (re)organizing strategies focused on individuals and population.10
The aim of this study was to estimate the prevalence of the associated factors to functional disability in Basic ADLs and IADLs in elderly who live in the municipality of Bagé, Rio Grande do Sul state, Brazil.
Methods
This is a population-based cross-sectional study, with data collected from July to November 2008 in the urban area covering primary health care services in Bagé-RS, in a sample of elderly people - individuals aged 60 or over. In 2008, Bagé had about 122,461 inhabitants, of which 14,792 (12%) were elderly, mostly residents in the urban area: 82%.
The sample size was calculated for a larger study to evaluate the occurrence of home care according to the primary health care model.16 Considering 10% of losses and refusals and a 1.3 design effect, the study had 80% of efficiency to detect 1.5 relative risks and exposures affecting at least 4% of the population.
The data collection of the larger study respected the 20 Primary Health Care Units (PHU) that existed in the city at that time: 15 Family Health Strategy (FHS) units and 5 traditional PHUs. FHS covered 51% of the urban population, while the traditional model covered 49%. Hence, the study population corresponded to the total elderly urban population of the municipality.
For the sample location, PHUs were divided into micro areas with numerical identification for each block, and the starting point of the data collection and each one of the blocks was picked up randomly. To ensure that all households had the same probability of compounding the study sample, the selection system of one home from a group of five was used. All residents aged 60 or over living in the selected households were asked to participate. The surveys not done after three attempted visits in different days and times were considered losses, and the cases in which the elderly declined to participate were considered refusals.
Hence, elderly - 60 years old or over - who lived in private households in the urban area of Bagé-RS at the reference date of the survey were included in the study. Individuals that were traveling, deprived of their liberty due to a court order or living in long-stay institutions at the time of the survey were excluded. The questionnaire was given to the primary caregiver when the older person was not physically or mentally able to answer it.
The dependent variable 'functional disability' was operationalized to characterize independently the domains of basic and instrumental activities of daily living. Katz index was used to characterize Basic ADLs (bathing, dressing, eating, toileting and making bed-wheelchair transfers),11 whereas Lawton and Brody scale was used to characterize IADLs (using the phone, going to distant places, shopping, preparing meals, doing household chores, managing money, taking drugs, and handling small objects).12 These two tools were selected due to their extensive use in previous surveys13,14 on functional disability in the elderly, in addition to being validated and recognized by the Ministry of Health.15
Three response options were offered for each activity evaluated in each domain: do not receive assistance, receive partial assistance or receive total assistance. Functional disability was defined by the need for partial or total assistance for at least one basic activity and at least one instrumental activity of daily living.
The independent variables included were:
- Sex (female; male);
- Age (in years: 60 to 64; 65 to 69; 70 to 74; 75 or over);
- Living alone (yes; no);
- Self-reported ethnicity/skin color (white; black; brown, indigenous, and Asian);
- Marital status (married or with companion; widowed; single or separated);
- Schooling (in completed years: without formal education; 1-7; 8 or over);
- Economic classification, according to the Brazilian Association of Research Companies - BARC (A/B; C; D/E);
- Tobacco use (former smoker; smoker; never smoked);
- Alcohol consumption in the last 30 days (yes; no);
- Sedentary behavior - watching TV more than 3 hours a day (yes; no);
- Self-rated health (excellent/good, average, poor/very poor);
- Feeling about life (satisfied; dissatisfied);
- Is your health better, equal or worse than other people of your age?;
- History of falls in the last year (yes; no);
- History of fracture in the last year (yes; no);
- Medical diagnosis of systemic hypertension (yes; no);
- Diagnosis of diabetes mellitus (yes, no);
- Medical diagnosis of cerebrovascular accident (yes; no);
- Medical diagnosis of heart disease (yes; no);
- Medical diagnosis of rheumatism, arthritis or osteoarthritis (yes; no);
- Medical diagnosis of cancer (yes; no);
- Cognitive impairment (Mini-Mental State Examination: up to 22/23) (yes; no);
- Use of urgency/emergency services in the last 3 months (yes; no);
- Home care in the last 3 months (yes; no);
- Hospitalization in the last 12 months (yes; no).
Stata® software, version 12.1, performed the analyses. Independent analyzes were performed to characterize functional disability in Basic ADLs and IADLs, and there was not a variable that combined both domains. Descriptive statistics were used to calculate the prevalence and respective 95% confidence intervals (95%CI). In the crude analysis, chi-square tests were used for heterogeneity or linear trend. The adjusted analysis helped to evaluate the association of each field of disability with independent variables, controlling possible confounding factors. The exposure variables were organized according to the following hierarchical model:
1st level - Demographic and socioeconomic characteristics
2nd level - Behavioral characteristics
3rd level - Health status and morbidity
4th level - Use of health services
Backwards selection was applied by hierarchical levels. Poisson regression with robust adjustment of variance was used. The prevalence ratios and their 95%CI were calculated and measured, and the p-values of the Wald test for heterogeneity and linear trend were measured. Associations with a <0.05 p-value were considered statistically significant.
The research protocol was approved by the Ethics Research Committee of the Medical School of the Federal University of Pelotas: Report No. 15/08. Ethical principles were respected, as the participants signed the Free Informed Term of Consent and were guaranteed to have absolute anonymity.
Results
The analyses included the 1,593 elderly surveyed; losses represented 4.0% (n=76) and refusals represented 3.0% (n=44). The sample consisted predominantly of women (63.0%), individuals aged 70 or over (51.4%) and white persons (78.6%); 51.2% of the sample corresponded to elderly who were married or living with a partner, 33.8% were widowers and 17.5% lived alone. Most of the participants (54.6%) reported having 1-7 years of schooling, and 23.6% had no schooling; 38.4% belonged to class C and 34.0% to class D/E. Regarding behavioral variables, 39.6% of the elderly reported having stopped smoking, 15.3% were smokers, 16% had consumed alcohol in the last 30 days, and 59.3% admitted to watch TV more than 3 hours per day. As for the self-rated health, 34.1% of the elderly classified their health as average, 94.3% said they were satisfied with life, and 44.6% of the participants considered their health equal to other people's health in general.
With regard to diseases, 4.0% of the elderly reported having suffered some type of fracture, and 28.0% of them had a fall in the last year. More than half of the participants (55.3%) had medical diagnosis of systemic hypertension, 15.1% had diabetes mellitus and 27.2% had rheumatism, arthritis or osteoarthritis. Amidst the older people surveyed, 9.8% reported having suffered a cerebrovascular accident, 29.6% had a heart disease, 4.9% were diagnosed with cancer, and 34.1% had cognitive impairment. Finally, with respect to the use of health services, 17.7% of the participants said to have been hospitalized in the last 12 months, 12.8% used an emergency medical service, 54.5% had a doctor's appointment, and 6.8% said they had received some form of home care in the three months preceding the interview.
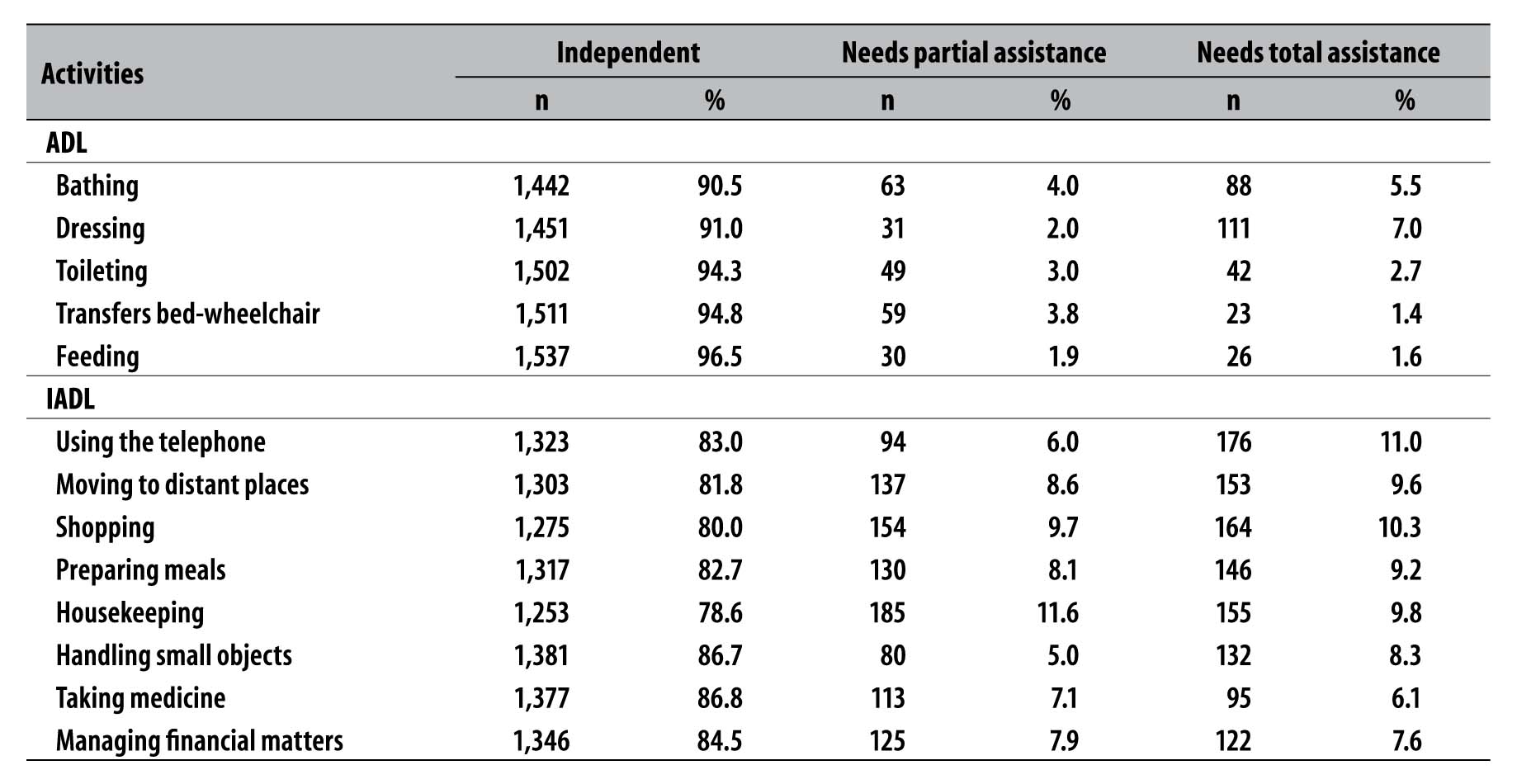
The prevalence of disability in Basic ADLs was 10.6% (95%CI: 9.1; 12.1), and 34.2% in IADLs (95%CI: 31.9, 36.6). Table 1 describes the dependence in each basic and instrumental activity of daily living. Feeding (96.5%) was the most independent activity among the basic activities, followed by making bed-wheelchair transfers (94.8%). The need for partial assistance in bathing was reported by 3.9% of the elderly, and 3.7% of them needed partial assistance in making bed-wheelchair transfers. Regarding the need for total assistance, dressing (7.0%) and bathing (5.5%) were the greater dependences. As for the instrumental activities, the elderly reported having greater independence to handle small objects (86.7%) and take drugs (86.6%), while 11.6% reported needing partial assistance in cleaning the house and 9.7% in shopping. Using the telephone (11.0%) and shopping (10.3%) were the activities which required total assistance more frequently.
Table 1 - Descriptive analysis of functional dependence in every basic activity of daily living (ADL) and instrumental activity of daily living (IADL) among the elderly (n=1,593) in Bagé, Rio Grande do Sul, 2008
Tables 2 and 3 show the crude and adjusted analyses of functional disability in basic and instrumental activities, according to independent variables. The factors that remained associated with functional disability in basic activities in the adjusted analysis were: elderly aged 75 or over (PR=3.55 - 95%CI: 2.23; 5.66), compared with the elderly aged 60 to 64; and elderly who were widowers (PR=1.52 - 95%CI: 1.12; 2.06) compared with those who were married or with a companion. The association with schooling showed a linear trend, with a higher prevalence of desability for Basic ADLs among elderly with a low level of education. Older people who had not consumed alcohol in the last 30 days had a higher prevalence of desability for Basic ADLs (PR=3.06 - 95%CI: 1.37; 6.83). Elderly who were satisfied with life had lower prevalence of desability for Basic ADLs (PR=0.51 - 95%CI: 0.33; 0.78). The prevalence of disability in basic activities was higher among individuals diagnosed with cerebrovascular accident (PR=2.72 - 95%CI: 1.91; 3.87), and with positive screening for cognitive impairment (PR = 3.99 - 95%CI: 2.50; 6.37). Hospitalization in the last 12 months (RP=1.73 - 95%CI: 1.26; 2.40) and home care in the last 3 months (RP=2.50 - 95%CI: 1.62; 3.86) were associated with higher incidence of disability for Basic ADLss (Table 2).
Table 2 Crude and adjusted analysis of the association between independent variables and disability for basic activities of daily living (ADL) among the elderly (n=1,593) in Bagé-RS, 2008
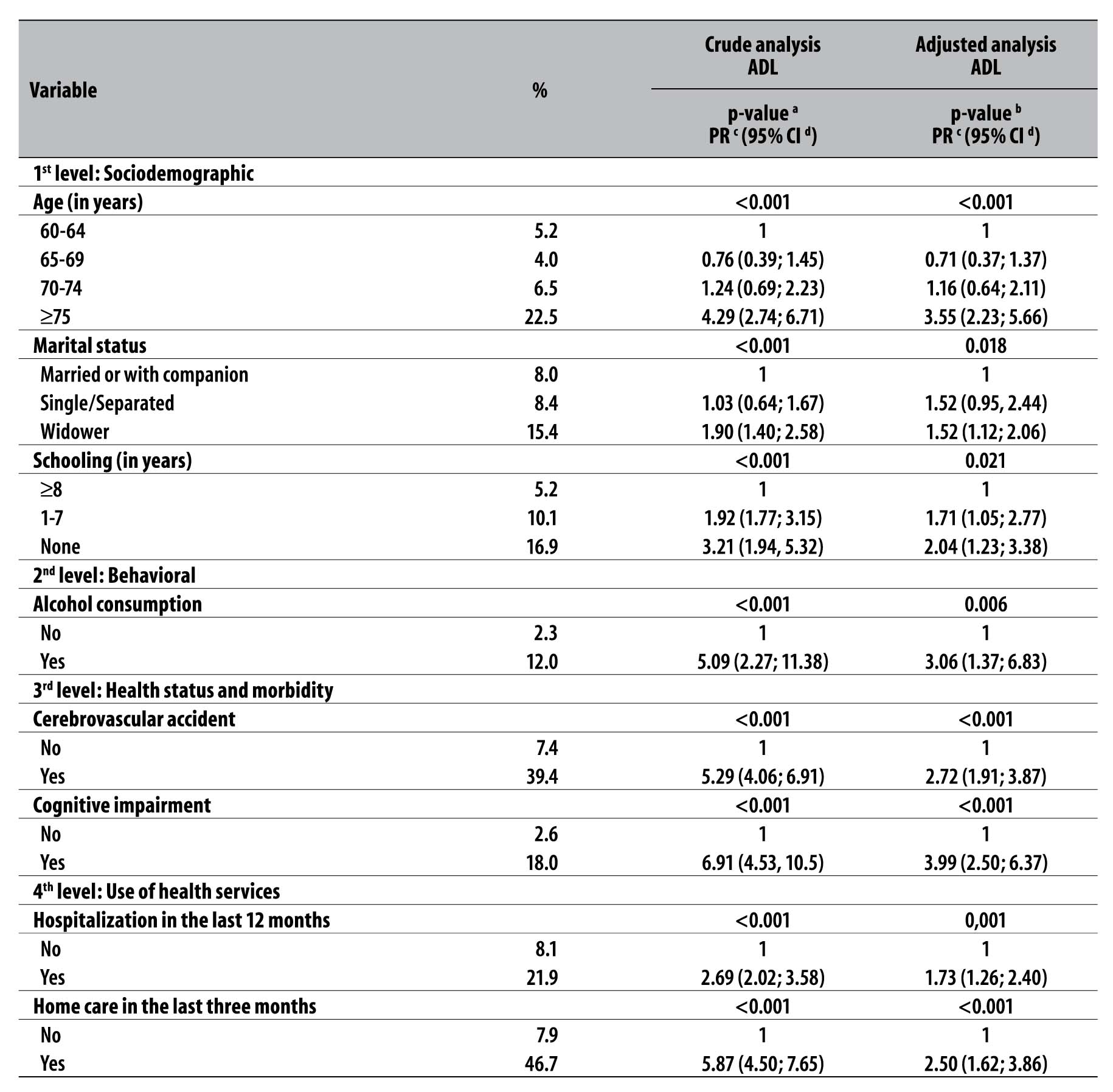
a) p-value calculated with Wald test for heterogeneity
b) p-value calculated with Wald test for linear trend
c) PR: prevalence ratio
d) 95% CI: 95% confidence interval
Note: Adjusted for 1st level - Sociodemographic characteristics -, 2nd level - Behavioral characteristics -, 3rd level - Health status and morbidity -, and 4th level - Use of health services. The variables sex; living alone; ethnicity/skin color; economic classification; tobacco use; sedentary behaviour; feeling about life; health conditions compared to other people; falls; fractures; systemic hypertension; diabetes mellitus; heart disease; rheumatism, arthritis or osteoarthritis; cancer; use of urgency/emergency services; and medical appointment were not described in the tables because they did not present statistically significant association with the outcome.
Table 3 - Crude and adjusted analysis of the association between independent variables and disability for instrumental activities of daily living (IADL) among the elderly (n=1,593) in Bagé-RS, 2008
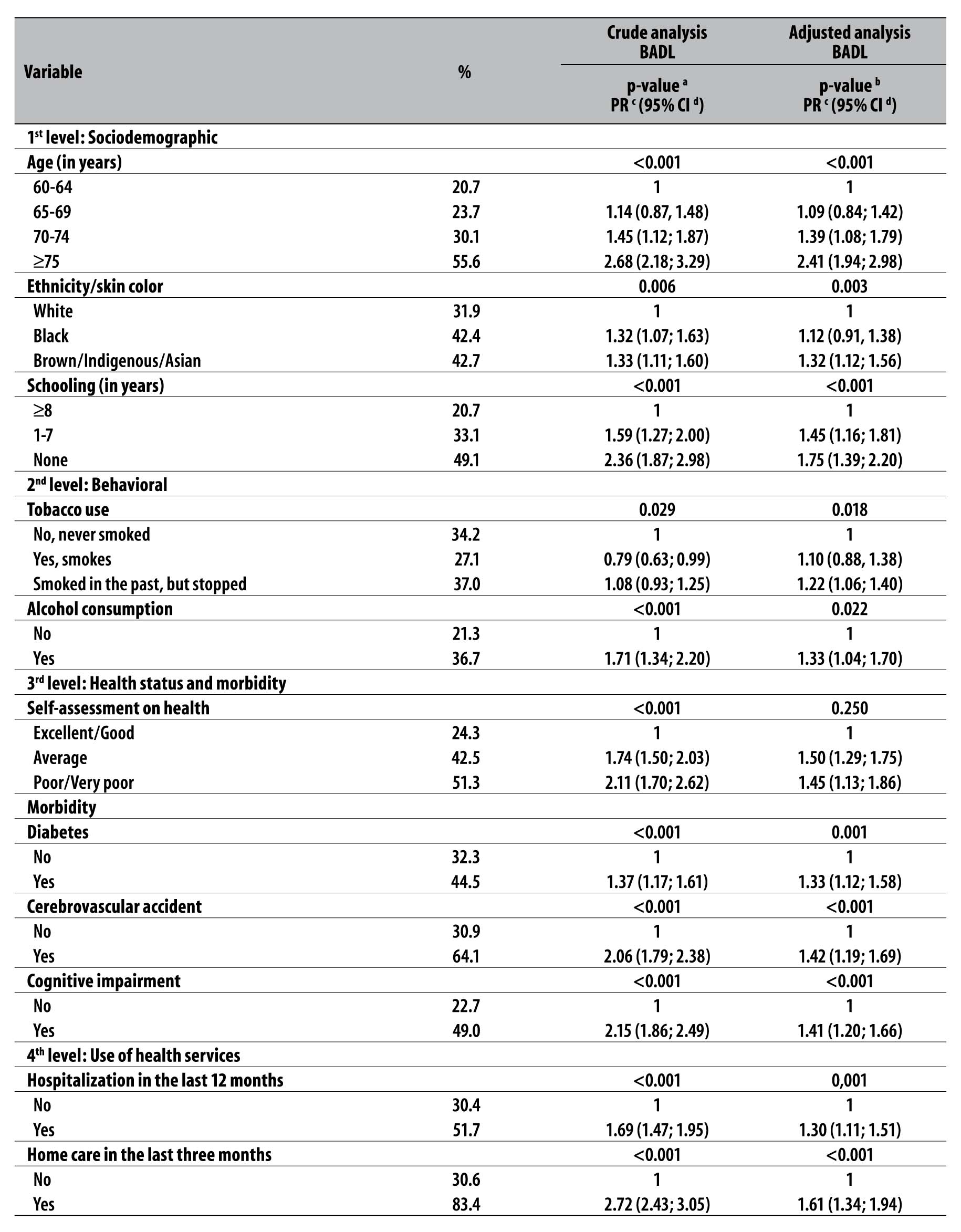
a) p-value calculated with Wald test for heterogeneity
b) p-value calculated by Wald test for linear trend
c) PR: prevalence ratio
d) 95% CI: 95% confidence interval
Note: Adjusted for 1st level - Sociodemographic characteristics -, 2nd level - Behavioral characteristics -, 3rd level - Health status and morbidity -, and 4th level - Use of health services. The variables sex; living alone; ethnicity/skin color; economic classification; tobacco use; sedentary behaviour; feeling about life; health conditions compared to other people; falls; fractures; systemic hypertension; diabetes mellitus; heart disease; rheumatism, arthritis or osteoarthritis; cancer; use of urgency/emergency services; and medical appointment were not described in the tables because they did not present statistically significant association with the outcome.
A similar behavior was observed in disability for IADLs - saving the variables 'marital status', 'feeling about life' and 'health status' - when comparing those who had a statistically significant association with disability for IADLs to those who had not. On the other hand, some variables were associated with disability for IADLs and not with Basic ADLs. Brown/indigenous/Asian elderly had a higher prevalence of disability for IADLs (RP=1.32 95%CI: 1.12; 1.56) than those who identified themselves as white. Former smokers had a higher prevalence of IADLs (PR=1.22 - 95%CI: 1.06; 1.40) than current smokers, and elderly with diabetes had a higher incidence of IADLs (PR=1.33 - 95%CI: 1.12; 1.58). Living alone was statistically associated with a lower incidence of Basic ADLs and IADLs (Table 3).
Discussion
The survey results reinforce the multidimensional condition of functional disability, which is associated with demographic, socioeconomic, and behavioral characteristics, health status and use of health services by the elderly. Most of the elderly surveyed were considered independent to perform basic and instrumental activities of daily living. However, a significant proportion had difficulty or inability to perform some activities, especially instrumental ones.
We believe that the presence of greater limitations on the execution of instrumental activities occur due to the impact of low levels of motor, sensory and cognitive impairment on such functions. On the other hand, performing basic activities require less integrity of such systems, which is why failure to perform them is usually linked to major limitations.14
Similarly to this study, a research that investigated the elderly in Pelotas municipality between 2007 and 2008 found higher prevalences of functional disability in 'bathing', 'dressing', and 'shopping'.17 Evidence suggests that the difficulties in carrying out basic or instrumental activities result from the physiological aging process, which affects cognitive (attention deficit, reasoning and memory), motor (decreased physical strength, mobility and balance limitations), and sensitive functions (impaired vision, touch, proprioception, hearing, taste, and smell).14
In this context, possible strategies to minimize the dependence of the elderly and extend their functionality become more relevant, by reducing architectural barriers, improving the lighting and arrangement of furniture in the house, and using adaptive equipment such as orthoses (canes, crutches, walker, wheelchair, hearing aid and glasses).14
According to this study, elderly aged 75 or over were more prone to functional disability in basic and instrumental activities, as found in national18,6 and international surveys.19,20 The functional decline affects 6% of biological functions in the elderly aged between 60 and 64, reaching about 50% of the physiological capacity after age 75.20
With regard to ethnicity/skin color, brown/indigenous/Asian elderly showed 32% more functional disability in instrumental activities compared to white elderly. With reference to schooling, the shorter the time of schooling, the greater the association with functional disability, both in basic and instrumental activities, coinciding with findings of studies conducted in the country.7.8 Such associations may be related to the socioeconomic status of those elderly, given that, in Brazil, ethnicity/skin color and schooling are directly related to socioeconomic status and, consequently, to living, housing, and work conditions, food safety, leisure, and lifestyle.7,8
Elderly widowers have a higher prevalence of functional disability in basic activities, according to the results of a population-based study, in the Southeast region of Brazil, on the negative impact of the loss of a partner on the daily lives of older people.21 Furthermore, the authors presented evidence of loosen emotional ties and support network, and the resulting damage to one's health, with negative consequences for their functional ability.21
As observed in other studies,21,9 living alone was associated with lower prevalence of functional disability in basic and instrumental activities. This condition shows greater independence and autonomy of the elderly in the performance of daily activities, probably because they still have physical and cognitive conditions for doing such activities.22 This outcome may present reverse causation, as the elderly who live alone may be precisely those who have less difficulty with Basic ADLs and IADLs.
Concerning behavioral characteristics, elderly former smokers have 22% more chances of having functional disability in instrumental activities than those who have never smoked. One hypothesis for this association is that smoking cessation is usually motivated by the worsening of one's health status, which can lead to a functional decline.23 The elderly who did not consume alcohol presented more disability in basic and instrumental functions. Alcohol, a depressant drug of the central nervous system, affects different brain functions, such as cognition, psychomotor coordination, visuospatial ability and perceptual motor skills, and can change one's health status and reduce functional ability.24 Although this is a cross-sectional study, such association may be biased by reverse causation, as disabilities might influence the decline in alcohol consumption.
Studies report that a poor self-rated health is associated with a greater risk of morbidity and mortality, while a good health status predicts a healthy aging.3,7,21 Pessimistic self-rated health usually stem from morbidity and limitations on the performance of daily activities. In this study, however, that was not associated with increased functional disability, that is, feeling satisfied with life was associated with a lower incidence of disability in basic activities.
Among the investigated diseases, the findings showed that having diabetes mellitus increases by 33% the risk of disability in instrumental activities. Having a history of cerebrovascular accident and/or a cognitive impairment was also significantly associated with functional disability in both domains.
Diabetes can trigger various complications, such as vascular disorders, vision loss, renal failure, and cerebrovascular accident, leading to cognitive decline, amputations, physical disability, falls and fractures and threatening the individual's independence.25 Cerebrovascular accident, in turn, is one of the most limiting diseases: in a short period of time, its consequences can drastically reduce the independence of older people.3 Cognitive impairment implies disturbance in the orientation in space and time, and difficulty with attention and memory, limiting social and intellectual activities of the elderly and restricting their functionality.26
Similarly to diabetes and cerebrovascular accidents, hypertension is a disease that compromises the circulatory system and has high mortality rates.27 Although systemic hypertension is quite prevalent (55.3%) among the elderly surveyed, no association between this disease and functional disability in any of the investigated domains was found. Similarly to what occurs in Brazil, investments in public policies related to the treatment of hypertensive patients, which ensure conditions for early diagnosis, give easy access to drug treatment, and encourage healthier lifestyles, reduce the negative consequences of the disease for the health and retard the loss of functionality.27
Just as previous findings,28 the results of this research indicate that elderly hospitalized at least once in the last year presented a probability about 70% higher of having disability in basic activities, and 30% higher in instrumental activities. Likewise, having received home care in the last three months was strongly associated with functional disability in both domains investigated. The literature indicates hospitalization causes losses in vital capabilities and the use of home care is associated with limited mobility to the health service.28
The use of health services is an important sign of one's poor health status. In this context, research shows that, in Brazil, the prevalence of annual hospitalization in public hospitals increases according to the age of older people, as it happens with 8.3% of the 60-69 age group, 10% of the 70-79 age group, and 11.9% of 80 years or over age group. This finding suggests that aging is accompanied by a decline in the health and functional ability of the elderly, causing a higher demand for health services.29
The results of this study allowed us to know the proportion of elderly individuals with impaired functional ability in basic and instrumental activities and associated factors. Amidst the investigated variables, we emphasize the importance of investing in health promotion actions which are related to behavioral characteristics, of health status and use of health services. These are subject to change and affect directly the functional ability of the elderly. The data presented can also be used by research initiatives on functional ability, in daily clinical practice of health professionals, and they allow to estimate the demand for support needed and the response in providing home care. This type of care may include targeted and timely interventions through actions that promote a healthy aging, independence, autonomy, quality of life and reduction in mortality among the elderly. Furthermore, these measures will be noticeable in the reduction of the costs of health services.
Finally, carrying out impact studies to better understand the disability process in the elderly is necessary, for they will allow the development of strategies to reduce damages even more effectively.
REFERENCES
1. Veras R. Envelhecimento populacional contemporâneo: demandas, desafios e inovações. Rev Saude Publica. 2009 mai-jun;43(3):548-54. [ Links ]
2. Lima-Costa MF, Facchini LA, Matos DL, Macinko J. Mudanças em dez anos das desigualdades sociais em saúde dos idosos brasileiros (1998-2008). Rev Saude Publica. 2012 dez;46 supl 1:100-7. [ Links ]
3. Giacomin KC, Peixoto SV, Uchoa E, Lima-Costa MF. Estudo de base populacional dos fatores associados à incapacidade funcional entre idosos na Região Metropolitana de Belo Horizonte, Minas Gerais, Brasil. Cad Saude Publica. 2008 jun;24(6):1260-70. [ Links ]
4. Verbrugge LM, Jette AM. The disablement process. Soc Sci Med. 1994 Jan;38(1):1-14. [ Links ]
5. Alves LC, Leite IC, Machado CJ. Conceituando e mensurando a incapacidade funcional da população idosa: uma revisão de literatura. Cienc Saude Coletiva. 2008 jul-ago;13(4):1199-207. [ Links ]
6. Barbosa BR, Almeida JM, Barbosa MR, Rossi-Barbosa LAR. Avaliação da capacidade funcional dos idosos e fatores associados à incapacidade. Cienc Saude Coletiva. 2014 ago;19(8):3317-25. [ Links ]
7. Alves LC, Leite IC, Machado CJ. Fatores associados à incapacidade funcional dos idosos no Brasil: análise multinível. Rev Saude Publica. 2010 jun;44(3):468-78. [ Links ]
8. Pereira GN, Bastos GAN, Del Duca GF, Bós AJG. Indicadores demográficos e socioeconômicos associados à incapacidade funcional em idosos. Cad Saude Publica. 2012 nov;28(11):2035-42. [ Links ]
9. Rosa TEC, Benício MHAB, LatorreMRDO, Ramos LR. Fatores determinantes da capacidade funcional entre idosos. RevSaude Publica. 2003 fev;37(1):40-8. [ Links ]
10. Alves LC, Leimann BCQ, Vasconcelos MEL, Carvalho MS, Vasconcelos AGG, Fonseca TCO, et al. A influência das doenças crônicas na capacidade funcional dos idosos do município de São Paulo, Brasil. Cad Saude Publica. 2007 ago;23(8):1924-30. [ Links ]
11. Katz S, Ford AB, Moskowitz RW, Jackson BA, Jaffe MW. Studies of Illness in the Aged. The Index of ADL: a Standardized Measure of Biological and Psychosocial Function. JAMA. 1963 Sep;185:914-9. [ Links ]
12. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. 1969;9(3):179-86. [ Links ]
13. Reyes-Ortiz CA, Ostir GV, Pelaez M, Ottenbaher KJ. Cross-national comparison of disability in Latin American and Caribbean persons aged 75 and older. Arch Gerontol Geriatr. 2006 Jan-Feb;42(1):21-33. [ Links ]
14. Maciel ACC, Guerra RO. Influência dos fatores biopsicossociais sobre a capacidade funcional de idosos residentes no nordeste do Brasil. Ver Bras Epidemiol. 2007 jun;10(2):178-89. [ Links ]
15. Ministério da Saúde (BR). Rede Interagerencial de Informações para a Saúde. Indicadores e dados básicos do Brasil - Brasil - 2006: IDB-2006 [Internet]. Brasília: Ministério da Saúde; 2006 [citado 2016 mar 07]. Disponível em: http://tabnet.datasus.gov.br/cgi/idb2006/matriz.htm [ Links ]
16. Thumé E, Facchini LA, Wyshak G, Campbell P. The utilization of home care by the elderly in Brazil's primary health care system. Am J Public Health. 2011 May;101(5):868-74. [ Links ]
17. Del Duca GF, Silva MC, Hallal PC. Incapacidade funcional para atividades básicas e instrumentais da vida diária em idosos. Rev Saude Publica. 2009 out;43(5):796-805. [ Links ]
18. Lopes MCBT, Lage JSS, Vancini-Campanharo CR, Okuno MFP, Batista REA. Fatores associados ao comprometimento funcional de idosos internados no serviço de emergência. Einstein (São Paulo). 2015 abr-jun;13(2):209-14. [ Links ]
19. Gill TM, Gahbauer EA, Murphy TE, Han L, Allore HG. Risk factors and precipitants of long-term disability in community mobility: a cohort study of older persons. Ann Intern Med. 2012 Jan;156(2):131-40. [ Links ]
20. Hairi NN, Bulgiba A, Cumming RG, Naganathan V, Muddla I. Prevalence and correlates of physical disability dwelling older people in rural Malaysia, a middle income country. BMC Public Health. 2010 Aug;10:492. [ Links ]
21. Nunes MCR, Ribeiro RCL, Rosado LEFPL, Franceschini SC. Influência das características sociodemográficas e epidemiológicas na capacidade funcional de idosos residentes em Ubá, Minas Gerais. Rev Bras Fisioter. 2009 set-out;13(5):376-82. [ Links ]
22. Nunes DP, Nakatani AYK, Silveira EA, Bachion, MM, Souza MR. Capacidade funcional, condições socioeconômicas e de saúde de idosos atendidos por equipes de Saúde da Família de Goiânia (GO, Brasil). Cienc Saude Coletiva. 2010 set;15(6):2887-98. [ Links ]
23. Capilheira MF, Santos IS. Fatores individuais associados à utilização de consultas médicas por adultos. Rev Saude Publica. 2006 jun;40(3):436-43. [ Links ]
24. Rigoni MS, Susin N, Trentini CM, Oliveira MS. Alcoolismo e avaliação de funções executivas: uma revisão sistemática. Psico. 2013 jan-mar;44(1):122-9. [ Links ]
25. Gregg EW, Brown A. Cognitive and physical disabilities and aging-related complications of diabetes. Clin Diabetes. 2003 Jul;21(3):113-8. [ Links ]
26. Freitas RS, Fernandes MH, Coqueiro RS, Reis Júnior WM, Rocha SV, Brito TA. Capacidade funcional e fatores associados em idosos: estudo populacional. Acta Paul Enferm. 2012;25(6):933-9. [ Links ]
27. Caskie GI, Sutton MC, Margrett JA. The relation of hypertension to changes in ADL/IADL limitations of Mexican American older adults. J Gerontol B Psico l Sci Soc Sci. 2010 May;65B(3):296-305. [ Links ]
28. Fialho CB, Lima-Costa MF, Giacomin KC, Loyola AIL. Capacidade funcional e uso de serviços de saúde por idosos da Região Metropolitana de Belo Horizonte, Minas Gerais, Brasil: um estudo de base populacional. Cad Saude Publica. 2014 mar;30(3):599-610. [ Links ]
29. Lima-Costa MF, Barreto SMA, Giatti L. Condições de saúde, capacidade funcional, uso de serviços de saúde e gastos com medicamentos da população idosa brasileira: um estudo descritivo baseado na Pesquisa Nacional por Amostra de Domicílios. Cad Saude Publica.2003 jun;19(3):735-43. [ Links ]
Received: April 13, 2016; Accepted: August 17, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
