










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.2 Brasília abr./jun. 2017
http://dx.doi.org/10.5123/s1679-49742017000200009
ORIGINAL ARTICLE
Prevalence and associated factors of self-medication in adults living in the Federal District, Brazil: a cross-sectional, population-based study*
1Universidade de Brasília, Faculdade de Medicina, Brasília-DF, Brasil
2Universidade Estadual de Campinas, Faculdade de Ciências Farmacêuticas, Campinas-SP, Brasil
3Universidade Federal de Uberlândia, Faculdade de Odontologia, Uberlândia-MG, Brasil
4Universidade de Sorocaba, Programa de Pós-Graduação em Ciências Farmacêuticas, Sorocaba-SP, Brasil
OBJECTIVE:
to assess the prevalence of self-medication and to investigate its associated factors in adults living in the Federal District, Brazil.
METHODS:
this is a cross-sectional population-based study conducted with adults selected through probabilistic sampling; self-medication prevalence was obtained from those who reported having used any medicine in the previous seven days; Poisson regression model with robust variance was applied to adjust the prevalence ratios.
RESULTS:
1,820 individuals were interviewed, of which 646 had taken at least one medicine; self-medication prevalence was of 14.9% (95%CI: 12.6%;17.5%); the adjusted analysis showed negative association in people aged 50 to 65 years (PR=0.26; 95%CI: 0.15;0.47) and with chronic diseases (PR=0.38; 95%CI: 0.28;0.51); adults with difficulties in performing daily activities (PR=2.25; 95%CI: 1.43;3.53) practiced more self-medication.
CONCLUSION:
self-medication was associated to young adults and those with problems in performing daily activities.
Keywords: Self Medication; Pharmaceutical Preparations; Pharmacoepidemiology; Cross-Sectional Studies; Prevalence Ratio
Introduction
Medicines are important for treating diseases, and they are responsible for improving the population's life quality. However, indiscriminate use of medicines might cause health risks. The practice of self-medication is worrisome because of the easy access to therapeutic products and potential damages to health caused by such practices.1
For the World Health Organization (WHO), self-medication is the selection and use of medicines to treat symptoms and self-reported diseases without the counseling of a qualified health professional for a certain function, comprising a stage of self-care.2 Within communities, reasonable self-medication might save resources for the treatment of minor diseases, as well as reduce work absences due to minor symptoms.3,4 Although self-medication constitutes an important form of population self-care, it presents inherent risks.3 Using medicines without prescription might cause severe consequences to the population's individual and collective health.5
Several factors induce the practice of self-medication, such as indiscriminate sale of medicines, especially because of the difficulty to access health systems and the costs of health plans and medical consultations.2 On the other hand, little is known about the characteristics of the population associated to this practice. A better understanding of the characteristics presented by individuals who self-medicate will facilitate the observation of groups at higher risk and, therefore, more attention should be dedicated to them.6
In Brazil, notwithstanding cases of intoxication7 involving medicines and the high number of people using them8, there are few studies estimating the prevalence of self-medication and investigating its associated factors.9 The Federal District does not have surveys that analyzed self-medication in its resident adult population. In this context, there are several singularities within the population and in its political and administrative organization. Thus, it is important to investigate the profile of self-medication among the residents.
The aim of this study was to estimate the prevalence and to investigate the associated factors of adult self-medication in the Federal District, Brazil.
Methods
A cross-sectional population-based study was carried out with adults (18 to 65 years old) living in the Federal District (FD). Data from the survey "Medicine consumption by adult population living in the Federal District" (Consumo de medicamentos pela população adulta residente no Distrito Federal) was used, and it refers to the population who used at least one medicine in the last seven days.10
The survey was taken from February, 2012 to May, 2012. The participants were approached at their home, where they answered a questionnaire applied by previously trained interviewers. The questionnaire, which was previously tested in a pilot-study run with 150 individuals, presented most of its questions closed, and was organized in four thematic blocks.
Demographic - sex, age, education, marital status and number of residents per household.
Socioeconomic - economic class and employment situation
Health status - section divided into self-reported chronic conditions: diabetes, hypertension, depression, heart conditions, respiratory diseases, other chronic diseases; and health state measured through an instrument that assess life quality, EuroQol five dimensions questionnaire (EQ-5D), which comprehends five dimensions, (i) mobility; (ii) self-care; (iii) performance of daily activities; (iv) pain or disconfort and (v) anxiety or depression. Answers were absence or presence of limitation in each domain.
Medicine consumption - identification of medicine, availability of medicine bottle and/or medicine package, used dosage, time of use, person who prescribed or recommended the medicine, and access to health services.
Presence or absence of medical prescription was reported for each medicine used.
The sample was selected in three stages: census sector, households and individuals. The 20 Administrative Regions in the Federal District were considered, and census sectors characterized by Brazilian Institute of Geography and Statistics (IBGE) were drawn as "urbanized area of town or village", except for those with less than 200 inhabitants.11 The first two stages were probabilistic, whereas at an individual level the selection was made based on sex and age quota in order to achieve representativeness, considering the Federal District population.
In the first stage, 4.016 sectors were selected, and those with less than 200 inhabitants were disregarded, totalizing 3.886 eligible census sectors.11 These sectors were submitted to an assortment, and 182 were selected to be part of the sample, besides 38 which were separated for replacement. In the second stage, 10 households were systematically elected, and in each census sector a number from 1 up to 20 was randomly selected to define the first residence to be interviewed; after this one, the twentieth residence on the right was visited. In case of refusal or closed household, the same procedure was conducted to the next house on the left until 10 interviews were carried out at the sector. One person was interviewed by household, respecting the previously established quota of sex and age, which were representative of the adult population of the Federal District11 in 2012.
According to the Brazilian Institute of Geography and Statistics (IBGE), the estimative of the adult population of the Federal District was of 1,702,419 inhabitants in the year of the study.12 The sampling time was calculated using a 95% confidence level, a 2.5% margin of error, design effect of 1,5, and a 50% estimative of the prevalence of medicine consumption among the population.10 Considering a 20% rate of no response, and to minimize possible losses, a corrected sample of 1,820 participants was established. The 50% prevalence estimative was used because of the lack of knowledge about the region's prevalence, so the most conservative estimate to calculate the sample size was adopted.
This study used data related to individuals who consumed medicine in the last seven days previous to the inquiry day in order to minimize the chances of recall bias. Information on the use of medicine was obtained by the following questions: 'Are you taking or have you taken any medicine in the last seven days?', 'Have you taken or are you going to take any medicine today?' (day of the interview), 'How many types of medicine are you taking?', 'What is the medicine's name?', 'What is the medicine’s concentration?', 'Who did prescribe the medicine?' and 'How did you get the medicine?'. Whenever possible, the presence or absence of medical prescription was noted down for each medicine the interviewee referred to, in order to obtain higher precision of prevalence of population self-medication. To obtain the prevalence of self-medication, the use of medicines not prescribed by a doctor or dentist was taken into consideration.
It was requested the identification of the medications through the presentation of the package and/or pack or medicine bottle, whenever possible, in order to minimize eventual mistakes when the interviewer takes note on data, as well as to minimize a possible recall bias. The medicines were codified according to the Anatomical Therapeutic Chemical Classification System (ATC);13 Anvisa's eletronic Medicines Compendium (Bulário Eletrônico da Anvisa) was used to identify the medicines' composition and, whenever this engine failed to return with results, the composition was searched through Google®. For the compounds without a specific code in the ATC classification, the limit-code was applied until the identification of the anatomic group, class or therapeutic action was possible. Phytotherapeutic and homeopathic medicines were not taken into consideration so that the ATC classification would be assured for all medicines.
As a quality control procedure, 20% of the interviews conducted were audited by phone and/or e-mail in order to have its authenticity verified.
The prevalence of self-medication was estimated in the population who took medicines in the last seven days, showing its proportion and respective confidence intervals of 95% (95%CI). Among the descriptive variables, the significant differences were assessed by the chi-square Pearson test. To assess the association between self-medication and the independent variables, a bivariate analysis was conducted to obtain prevalence ratio (PR) of self-medication and its respective 95%CI. A Poisson regression model was developed with robust variance to identify self-medication to the associated factors. The analysis between the practice of self-medication and the variables that were included in the model was conducted with subjects who presented complete data. Those who reported not knowing or did not answer some of the variables were excluded from the analysis. For all the analyses, the significance level of 5% was considered.
Data were tabulated on the program Microsoft Excel® 2010 and analyzed on the STATA (version 11.2) program. As to avoid mistakes associated to the study design, lack of answer and population distribution, a weighting factor proportional to the number of households by each census sector was applied to all analyses. The complex sampling effect was considered in all analyses (survey module).
The project was approved by the Ethics Research Committee on Human Research from the University of Brasília, Faculty of Health Sciences - Report No. 003/2012 and Certificate of Presentation for Ethical Consideration (CPEC) No. 00647212.6.0000.003 in 04/16/2012. Data were collected upon signature of the Free Informed Term of Consent, as recommended by the Resolution of the National Health Council (CNS) No. 466, dated December, 12th, 2012.
Results
Considering the adult population living in the Federal District, 2,051 people were invited to participate in the study, of which 1,820 accepted the invitation. Amidst interviewees, 646 (35.5%) reported having taken at least one medicine in the last seven days, and the prevalence of self-medication was assessed upon them (Figure 1).
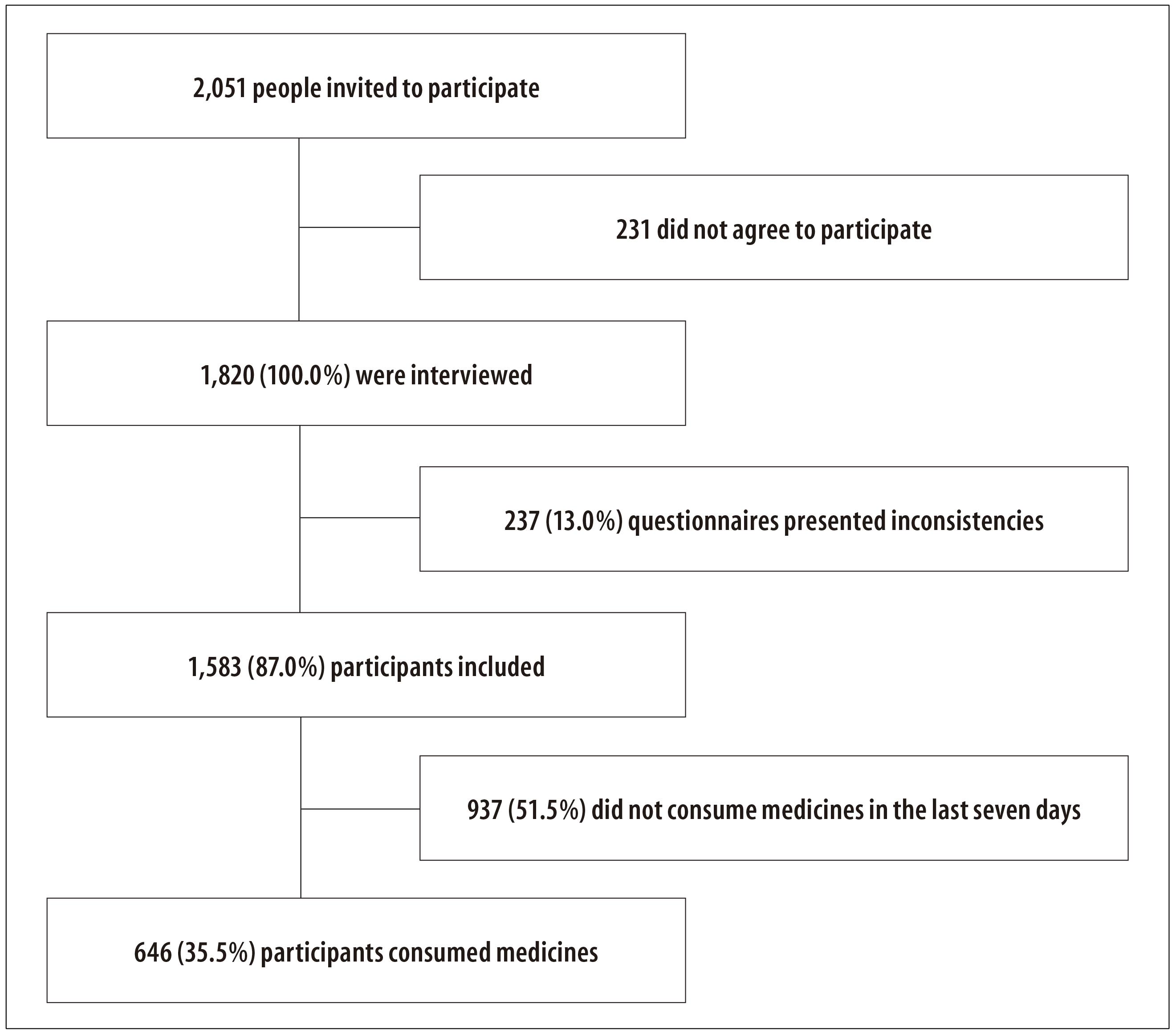
Figure 1 - Recruiting process, selection, inclusion and assessment of surveyed interviewee about medicine consumption by the adult population living in the Federal District, 2012
The majority of participants were women (69.2%), 52.3% were married or had a stable union, and the average of residents per household was 3.8 people (standard deviation: 1,6) . The average age was 42,5 years (standard deviation: 13,1, and there was a predominance of the age group between 35 and 49 years (34.8%) The most recurring educational level was illiterate or incomplete Basic Education, followed by people who completed High School. A higher number of individuals pertaining to 'B' (32.0%) and 'C' (48.2%) economic classes have been observed, and 66.6% of participants reported having an occupational activity (Table 1).
Table 1 Demographic and socioeconomic characteristics of participants who consumed medicines, layered by sex, in the to survey on medicine consumption by the adult population living in the Federal District, Brazil, 2012
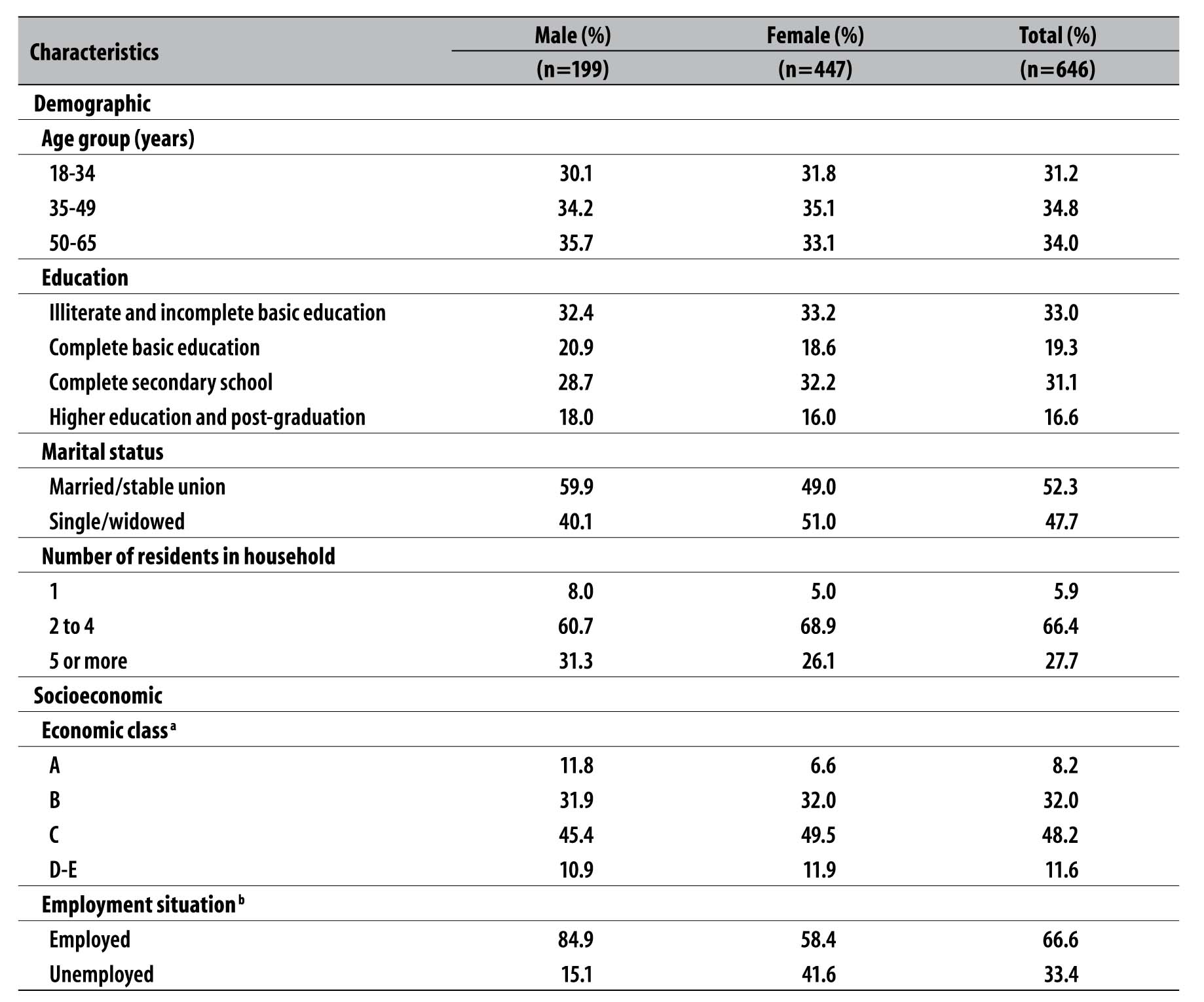
a) Brazilian Criteria for Economic Classification
b) The variable 'Employed' comprise servers or salaried employees with signed portfolio, informal job, domestic work, autonomous or freelancers. The variable 'Unemployed' includes unemployed people, retirees and students.
Regarding health conditions indicators and use of health services, the prevalence of self-reported chronic diseases was of 73.4% (95%CI: 69.8%; 76.6%), hypertension as the most frequent one, followed by diabetes and depression. Hypertension and diabetes were more prevalent on men, whereas the remaining chronic diseases were found more frequently among women. Concerning the use of health services, about one third of the sample (32.8%) maintained a private health insurance, 60% had a consultation in the last three months and 14.7% had been hospitalized in the last 12 months. Women presented higher prevalence on use of health services. More than a half of the interviewees reported presence of pain or discomfort (53.7%), and the women presented most of the complaints about their health status (Table 2).
Table 2 - Characteristics of the self-reported health status and use of health services by the participants who consumed medicines, in the survey on medicine consumed by the adult population living in the Federal District, Brazil, 2012

The prevalence of self-medication was of 14.9% (95%CI: 12.6%;17.5%) in the last seven days. Self-medication was most practiced by women. It was observed in 1.5% (95%CI: 0.8%; 2.8%) among elder adults of age between 50 and 65 years old, whereas in younger ones, of age between 18 and 34 years old, it was observed in 7.9% (95%CI: 6.1%;10.2%).
Among the participants who performed self-medication, 66 took medicines on their own, and 30 took medicines as recommendation provided by someone else other than a doctor or dentist. Of those, 28 people medicated themselves at the drugstore clerk's recommendation, and two followed recommendations of friends, family members or neighbors.
The assessment of how the medicines were obtained by the participants who self-medicated themselves showed that the highest the economic class and education level, there is a higher use of financial resources to obtain the medicine. The majority of medicines used was bought by the participants (74.1%), whereas the minority was acquired from the Brazil Popular Pharmacy (13.9%) and the Brazilian National Health System (SUS) (12.0%).
Among those who self-medicated, 145 medicines were used in the last seven days, which corresponds to a consume average of 1.5 medicine per person. The reported medicines were grouped according to the 1st and 2nd levels of the WHO's ACT classification. Regarding the medicines consumed without a prescription, the most used were the ones that act on the nervous system, digestive system and metabolism, and the cardiovascular system. The most employed therapeutic classes were analgesics (metamizol and combinations - 78.6% - and acetaminophen - 19.6%), anti-inflammatories and anti-rheumatics (diclofenac and combinations - 60%) and sex hormones and genital system modulators (cyproterone and ethinyloestradiol - 35.7%). From the total of medicines used in self-medication, 72 were over-the-counter drugs, 73 needed prescription to be dispensed and, among these, 15 needed a controlled substance prescription form (Table 3).
Table 3 - Description of used medicines by individuals who self-medicated (n=145)
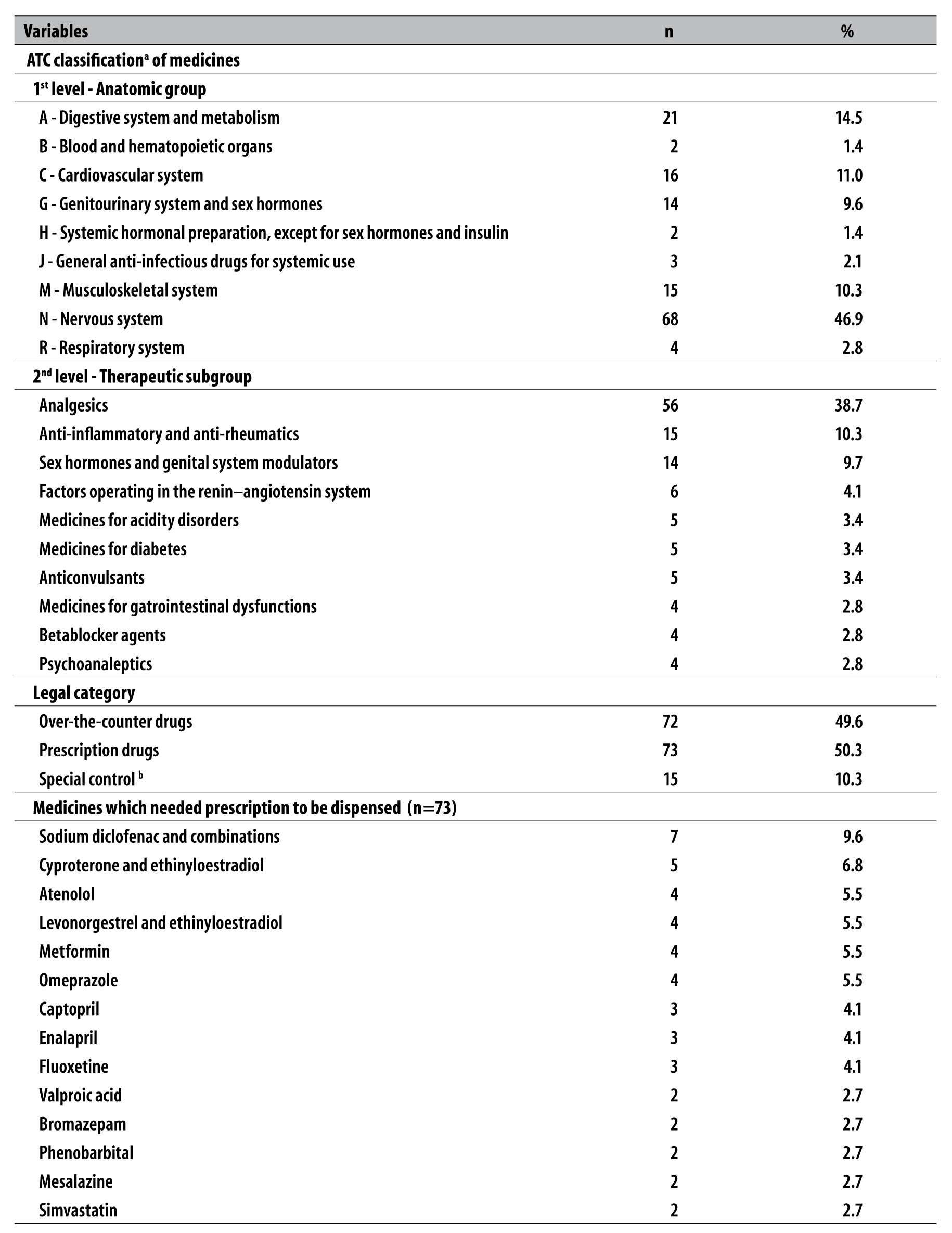
a) ATC: Anatomical Therapeutic Chemical Classification System
b) Medicines listed in the updated attachments of the Ordinance no 344, from 12th May, 1998, and RDC No. 44, from 26th October, 2010.
Note: The 10 subgroups most used in self-medication are included. Grouped ones represent 81.4% of the total of medicines.
The prevalence of self-medication regarding variables assessed in the participants who consumed at least one medicine in the last seven days prior to the interview is presented in Table 4.
Table 4 - Prevalence of self-medication and prevalence ratios of associated factors in the adult population (n=646) living in the Federal District, Brazil, 2012
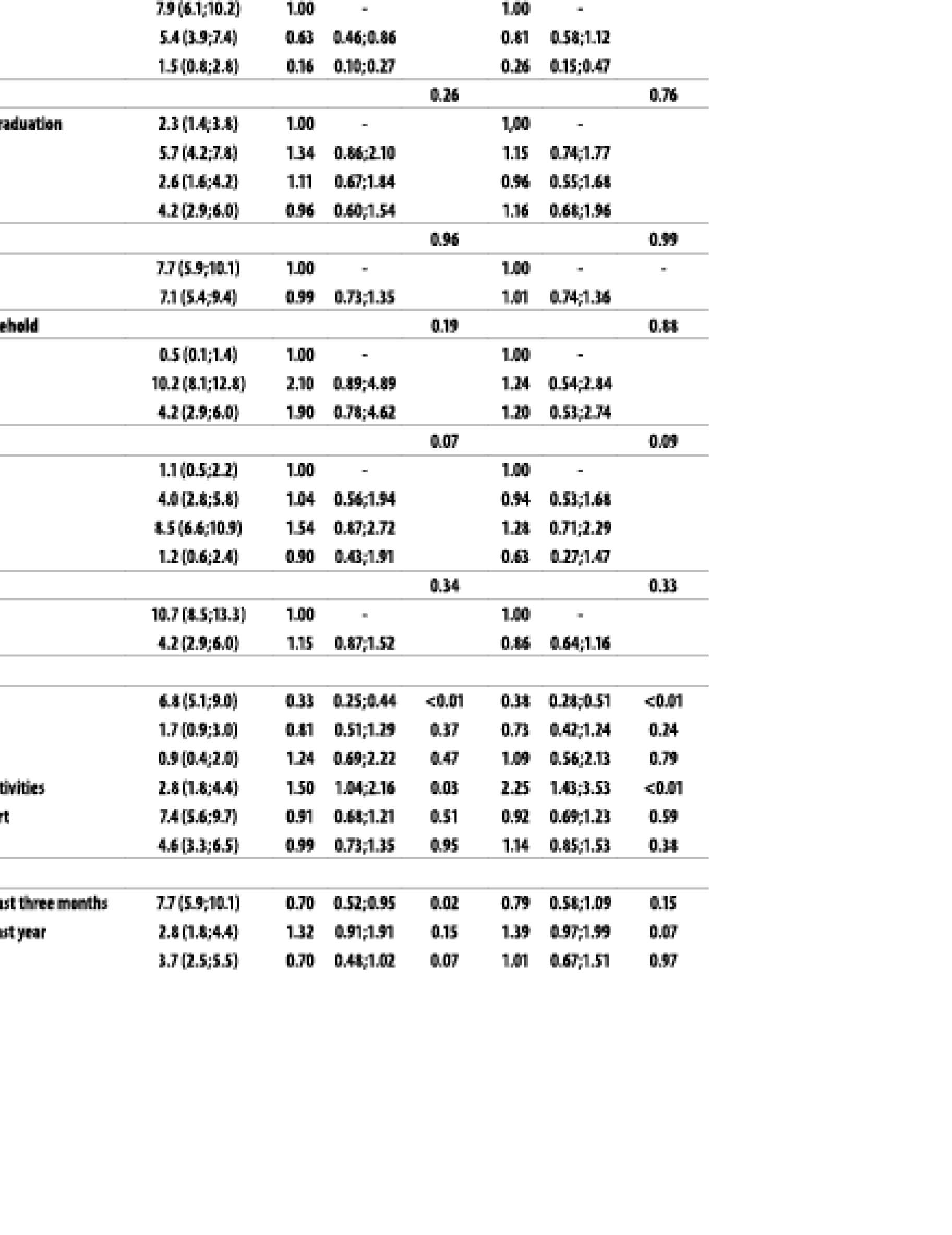
a) 95%IC: confidence interval of 95%
b) PR: prevalence ratio
c) Calculated through Possion regression with robust variance
d) Comparison is made between presence and absence of reference. For instance, considering chronic diseases, it was compared to not having chronic diseases.
After adjustments, there was no association between self-medication, the age group from 35 to 49 years and medical consultation in the last three months. Higher age (from 50 to 65 years) or chronic diseases were factors negatively associated to self-medication, whereas difficulty to perform daily activities was directly associated to self-medication (Table 4).
Discussion
This study's results show that self-medication is practiced by 14.9% of the adult population in the Federal District, and its practice is more frequent in young adults between 18 and 34 years, and performed by one quarter of this population.
The adjusted model showed association between difficulty to perform daily activities and self-medication. Elder adults and those suffering from chronic diseases were the ones who least practiced self-medication, probably because they do not rely on such practice for their therapeutic treatments. It was observed that half the medicines used needed prescription to be dispensed, and analgesics and anti-inflammatories corresponded together to almost half of all medicines consumed.
Some limitations are inherent to this study design and deserve to be highlighted. The investigation may present information bias, because self-medication has been measured by the interviewee’s self-report, without objective confirmation. Another limitation to be considered is the exclusion of phytotherapeutic and homeopathic medicines, which might underestimate the prevalence of self-medication in the population. However, there's a gain in the quality of data treatment, which makes it possible to better identify and classify all medicines assessed. In addition, interviewees who presented old and overdue prescriptions might have answered that they had used the medicine upon prescription, which may underestimate the prevalence of self-medication. Nevertheless, since several characteristics are not influenced by time, the validity of the information is not affected. Likewise, there are uninvestigated factors related to the practice of self-medication, such as the consumption indication, a variable that could explain the real motivation behind the practice and its associated factors, which depends on future studies.
The influence of seasonality in the occurrence of certain diseases14 may affect the use of medicines by the population, mainly because the research did not included the winter and drought seasons in the Federal District.15
Although in the cross-sectional studies the results found may not allow to identify the relation of temporality in the associations, in this study the associations found comprised variables of a relatively stable nature, so that the impediment of temporality determination did not constitute a limitation. As positive aspects, the fact that this is the first cross-sectional population-based study carried out on the matter in the Federal District is highlighted, thereof the importance of its findings for the expansion of the reasonable use of medicine in this site. Not only the findings deserve to be highlighted, but also the methodological care applied in a cross-sectional population-based study, with a representative sample of the Federal District population. To ensure the sample's representativeness, a stratification by sex and age group was performed, as established by the Demographic Census.12 Furthermore, we have followed the WHO recommendation, indicating the use of a recording period of a week as ideal16; the study procedures were standardized, an experienced team conducted the population surveys, the questionnaire has been previously tested in a pilot-study, and 20% of the interviews carried out had been audited. These precautions give more efficacy to this investigation's findings.
A systematic review on self-medication in Brazil's adult population found a higher prevalence (35%) in comparison with the one revealed to the Federal District.9 The prevalence of self-medication found in this study is also lower than the ones found in other Brazilian studies that presented certain methodological similarities with this study.17-20 One possible explanation for these different values is the difference between the recording periods: the present study used the 7 days period, while other three research18-20 used the 15 days period. Other possible reason for the lower prevalence found is that the studies17-19 - with one exception20 - have been initially designed to include adults with age over 65 years.
Half the medicines used in self-medication needed prescription to be dispensed. Approximately 1/5 required controlled substance prescription form (antibiotics and drugs listed in the attachment of the Ordinance No. 344, from 12th May, 1998).21,22 A small part of the interviewees obtained the medicines used in self-medication from the SUS (Brazilian National Health System) or the Brazil Popular Pharmacy, and in both cases, the citizen must present a prescription to acquire the medicine. It is unknown how certain drugs were acquired without a prescription, since the research did not deepen the questioning regarding the access to medicines, focusing exclusively on self-medication. There is also the possibility of interviewee misinformation as one cause for the result found, as well as the sharing of prescription drugs with other people, like family members or friends. Both situations point out to a violation of the Brazilian sanitary laws.21-23
These findings might make it easier to identify the business interest of pharmacies and drugstores. A qualitative research carried out in the Federal District shows dissatisfaction regarding the quality of services in drugstores, seen as commercial establishments that provide easy access to medicines.24 However, studies specially designed for this purpose can give more clear and accurate answers, able to make it possible to expand the reasonable use of medicines.
The low prevalence of adults at a later age (50 to 65 years old) is statistically significant and should be highlighted. Some national and international population based studies also observed this effect,17,25-27 which might be explained by the higher use of health services by this population.28
The practice of self-medication revealed to be negatively associated to chronic diseases. Studies carried out both in developed countries26 and developing29 ones reported an association between self-medication and the presence of minor diseases and conditions, such as flu, cold, headache and muscular pain. It is expected that people with chronic diseases need regular medical orientation and, consequently, make use of medicine that require medical prescription to be dispensed. Other cross-sectional population base studies also showed that the most used therapeutic classes in self-medication were analgesics and anti-inflammatories,27,30 contributing to the premise of association between self-medication and the presence of minor diseases and conditions.
This study revealed that people with difficulty to perform daily activities (work, study, housework, family activity or leisure) are more prone to self-medicate. We suppose that these people tend to use medicine to treat or relieve symptoms that impair their daily activities. Studies designed focused specifically on this matter are recommended in order to elucidate the motivation behind the practice of self-medication by people with difficulty to perform daily activities.
In conclusion, self-medication had low prevalence among the adults from the Federal District who consumed medicines last week. However, whenever practiced, self-medication has been performed in a less reasonable way. Young adults and individuals facing trouble to perform daily activities form the group that most seek self-medication, whereas elder individuals and those with chronic diseases tend not to adopt such practice.
The results might indicate specific targets for the planning of actions regarding health education towards the reasonable use of medicine by the adult population from the Federal District.
REFERENCES
1. Schweim H, Ullmann M. Media influence on risk competence in self-medication and self-treatment. Ger Med Sci. 2015 Jul;13:1-14. [ Links ]
2. World Health Organization. The role of the pharmacist in self-care and self-medication [Internet]. Geneva: World Health Organization; 1998 [cited 2016 Dec 13]. Available from: Available from: http://apps.who.int/medicinedocs/pdf/whozip32e/whozip32e.pdf . [ Links ]
3. World Health Organization. Guidelines for the regulatory assessment of medicinal products for use in self-medication. Geneva: World Health Organization; 2000. [cited 2016 Dec 13]. Available from: Available from: http://apps.who.int/medicinedocs/pdf/s2218e/s2218e.pdf . [ Links ]
4. Eticha T, Mesfin K. Self-medication practices in Mekelle, Ethiopia. PLoS One. 2014 May;9(5):e97464. [ Links ]
5. Gualano MR, Bert F, Passi S, Stillo M, Galis V, Manzoli L, et al. Use of self-medication among adolescents: a systematic review and meta-analysis. Eur J Public Health. 2015 Jun;25(3):444-50. [ Links ]
6. Elseviers M, Wettermark B, Almarsdóttir AB, Andersen M, Benko R, Bennie M, et al. Drug utilization research methods and applications [Internet]. New Jersey: Wiley Blackwell; 2016 [cited 2016 Dec 13]. Available from: Available from: http://onlinelibrary.wiley.com/book/10.1002/9781118949740;jsessionid=E8FCC3039FD658F44085DFB71995EB41.f04t03 [ Links ]
7. Sistema Nacional de Informações Tóxico-Farmacológicas. Tabela: casos registrados de intoxicação humana por agente tóxico e sexo: Brasil, 2011 [Internet]. Rio de Janeiro: Fundação Oswaldo Cruz; 2011 [citado 2016 dez 13]. Disponível em: Disponível em: http://sinitox.icict.fiocruz.br/sites/sinitox.icict.fiocruz.br/files//Tabela%208.pdf [ Links ]
8. Leite SN, Vieira M, Veber AP. Estudos de utilização de medicamentos: uma síntese de artigos publicados no Brasil e América Latina. Cien Saude Colet. 2008 abr;13 supl:793-802. [ Links ]
9. Domingues PHF, Galvão TF, Andrade KRC, Sá PTT, Silva MT, Pereira MG. Prevalence of self-medication in the adult population of Brazil: a systematic review. Rev Saude Publica. 2015;49:36. [ Links ]
10. Galvao TF, Silva MT, Gross R, Pereira MG. Medication use in adults living in Brasilia, Brazil: a cross-sectional, population-based study. Pharmacoepidemiol Drug Saf. 2014 May;23(5):507-14. [ Links ]
11. Instituto Brasileiro de Geografia e Estatística. Geociências [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2012 [citado 2016 dez 13]. Disponível em: http://www.ibge.gov.br/home/download/geociencias.shtm. [ Links ]
12. Instituto Brasileiro de Geografia e Estatística. Censo demográfico 2010: características da população e dos domicílios: resultados do universo. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística ; 2011. [ Links ]
13. World Health Organization. Collaborating Centre for Drug Statistics Methodology. Norwegian Institute of Public Health. Structure and principles [Internet]. Oslo: World Health Organization; 2011 [cited 2016 Dec 13]. Available from: Available from: http://www.whocc.no/atc/structure_and_principles/ . [ Links ]
14. Rosa AM, Ignotti E, Botelho C, Castro HA, Hacon SS. Respiratory disease and climatic seasonality in children under 15 years old in a town in the Brazilian Amazon. J Pediatr. 2008 Nov-Dec;84(6):543-9. [ Links ]
15. Valença LM, Restivo PCN, Nunes MS. Variação sazonal nos atendimentos de emergência por asma em Gama, Distrito Federal. J Bras Pneumol. 2006 jul-ago; 32(4): 284-9. [ Links ]
16. Hardon A, Hodgkin C, Fresle D. How to investigate the use of medicines by consumers. Amsterdam: World Health Organization; 2004. [ Links ]
17. Girotto E, Matos DBS, Oliveira JM. Perfil da automedicação em população residente de Arapongas, Paraná. Espac Saude. 2010;11(2):29-38. [ Links ]
18. Schimid B, Bernal R, Silva NN. Self-medication in low-income adults in Southeastern Brasil. Ver Saude Publica. 2010 Dec;44(6):1-6. [ Links ]
19. Arrais PSD. Epidemiologia do consumo de medicamentos e eventos adversos no município de Fortaleza-CE [tese]. Salvador (BA): Universidade Federal da Bahia; 2004. [ Links ]
20. Mendes CMM. Perfil da automedicação em duas populações do município de Teresina [dissertação]. Fortaleza (CE): Universidade Federal do Ceará; 2010. [ Links ]
21. Brasil. Ministério da Saúde. Secretaria de Vigilância Sanitária. Portaria nº 34, de 12 de maio de 1998. Aprova o regulamento técnico sobre substâncias e medicamentos sujeitos a controle especial. Diário Oficial da República Federativa do Brasil, Brasília (DF), 1998 mai 15;Seção 1:3. [ Links ]
22. Brasil. Ministério da Saúde. Agência Nacional de Vigilância Sanitária. Resolução da Diretoria Colegiada - RDC nº 44, de 26 de Outubro de 2010. Dispõe sobre o controle de medicamentos à base de substâncias classificadas como antimicrobianos, de uso sob prescrição médica, isoladas ou em associação e dá outras providências. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2010 out 26; Seção 1:76 [ Links ]
23. Brasil. Ministério da Saúde. Gabinete do Ministro. Portaria nº 971, de 15 de maio de 2012. Dispõe sobre o Programa Farmácia Popular do Brasil. Diário Oficial de República Federativa do Brasil, Brasília (DF), 2012 mai 15;Seção1:67. [ Links ]
24. Naves JOS, Castro LLC, Carvalho CMS, Merchán-Hamann E. Automedicação: uma abordagem qualitativa de suas motivações. Cien Saude Coletiva. 2010 jun;15 supl 1:1751-62. [ Links ]
25. Carrasco-Garrido P, Jiménez-García R, Barrera VH, Gil de Miguel A. Predictive factors of self-medicated drug use among the Spanish adult population. Pharmacoepidemiol Drug Saf. 2008 Feb;17(2):193-9. [ Links ]
26. Carrasco-Garrido P, Hernández-Barrera V, López de Andrés A, Jiménez-Trujillo I, Jiménez-García R. Sex-differences on self-medication in Spain. Pharmacoepidemiol Drug Saf. 2010 Dec;19(12):1293-9. [ Links ]
27. Loyola Filho AI, Uchoa E, Guerra HL, Firmo JOA, Lima-Costa MF. Prevalência e fatores associados à automedicação: resultados do projeto Bambuí. Rev Saude Publica. 2002 fev;36(1):55-62. [ Links ]
28. Lima-Costa MF, Firmo JOA, Uchôa E. The Bambuí cohort study of aging: methodology and health profile of participants at baseline. Cad Saude Publica. 2011;27 Suppl 3:S327-35. [ Links ]
29. Arrais PSD, Coelho HLL, Batista MCDS, Carvalho ML, Righi RE, Arnau JM. Perfil da automedicação no Brasil. Rev Saude Publica. 1997 fev;31(1):71-7. [ Links ]
30. Jerez-Roig J, Medeiros LF, Silva VA, Bezerra CL, Cavalcante LA, Piuvezam G, et al. Prevalence of self-medication and associated factors in an elderly population: a systematic review. Drugs Aging. 2014 Dec;31(12):883-96. [ Links ]
* This article is part of the Master’s thesis entitled ‘Prevalência e fatores associados à automedicação no Brasil: revisão sistemática da literatura e estudo de base populacional no Distrito Federal’, defended by Paulo Henrique Faria Domingues, to the University of Brasília, in 2014. The research was funded by the National Council for Scientific Development (CNPq)/ Ministry of Science, Technology and Innovation (MCTI): Report No. 564831/2010-7, dated December 14th, 2010.
Received: September 21, 2016; Accepted: November 24, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
