










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.3 Brasília jul./sep. 2017
http://dx.doi.org/10.5123/s1679-49742017000300005
Original article
Time trends of hypertension and diabetes mellitus prevalence among adults registered in the Brazilian National Health System, in Florianópolis, Santa Catarina State, Brazil, 2004-2011*
1Universidade Federal de Santa Catarina, Programa de Pós-Graduação em Nutrição, Florianópolis-SC, Brasil
2Universidade Estadual do Centro-Oeste, Curso de Nutrição, Guarapuava-PR, Brasil
OBJECTIVE:
to investigate the time trend of prevalence of hypertension, diabetes mellitus, and both diseases combined, from 2004 to 2011; and to analyze their association with sociodemographic factors in adults registered in the Brazilian National Health System (SUS) in Florianópolis-SC, Brazil, in 2011.
METHODS:
time-series study using secondary data from the Primary Health Care Information System of adults (≥20 years) at SUS; Prais-Winsten regression was used.
RESULTS:
from 2004 to 2011, prevalences of hypertension (7 to 13.5%), diabetes (2.2 to 4.2%) and both diseases combined (1.2 to 2.9%) increased; after adjustment, the occurrence of the diseases was higher among women (except for the association of hypertension with diabetes), the elderly, less educated and residents in the Mainland and South sanitary districts.
CONCLUSION:
the occurrence of the investigated diseases doubled from 2004 to 2011. However, the prevalences found are below the ones described in the Brazilian scientific literature.
Keywords: Diabetes Mellitus; Hypertension; Unified Health System (SUS); Time Series; Prevalence
Introduction
High blood pressure (HBP) and diabetes mellitus (DM) are non-communicable chronic diseases of high prevalence, and are considered relevant Public Health issues; they are among the five major global mortality risks.1 According to the World Health Organization (WHO), one in three adults presents high blood pressure and one in ten presents DM.1 In the North American population, HBP increased between the 1988-1994 and 2005-2008 periods, rising from 26.4 to 31.6% among men and from 24.4 to 29.8% among women. In that same population, from 2005 to 2008, DM affected 4.0% and 14.0% of them in the 20-44 and 45-64 age groups, respectively.2
In Brazil, in 2011, 22.7% and 5.6% of the population aged 18 or over were diagnosed with HBP and DM, respectively, with a higher prevalence among older and less educated individuals.3 HBP and DM have high costs: in 2005, only, approximately 398 million dollars were spent by the Brazilian National Health System (SUS) with HBP treatment.4
It is possible to prevent the development of HBP and DM, improve the prognostic and quality of life of individuals with these diseases and also avoid health expenditures.1,5 It is in the Primary Health Care that the Brazilian population has its first contact with the prevention and treatment of these diseases. SUS Family Registration enables the collection of information regarding the prevalence of such diseases and conditions. It is important, thus, to further explore these data in order to obtain more knowledge and monitor these morbidities, contributing to the allocation of Health funds to areas of major risk, as well as verifying if the existing public health policies are successful in reducing the incidence of these diseases.
This study aimed to investigate the time trend of prevalence of hypertension, diabetes and both diseases combined (2004-2011), and to analyze their association with sociodemographic factors (2011) in adults registered in SUS in Florianópolis, Santa Catarina State, Brazil.
Methods
A time series study on the prevalence of HBP, DM and both diseases combined among adults (≥20 years old) of both sexes, registered in SUS in Florianópolis, from 2004 to 2011 was conducted. In order to assess sociodemographic factors (sex, age group, education level and sanitary district) associated to these diseases, a cross-sectional analysis was carried out for the year of 2011.
Information was obtained from the SUS Family Registration, data from the Ficha A (A Form) of the Primary Health Care Information System (SIAB)6 performed by all of the 49 Primary Health Care Units (PHU) of the municipality up to 2011. These PHU are distributed among five sanitary districts in the municipality: Center, Mainland, East, North and South.
In 2011, Florianópolis had an estimated population of 427,298 inhabitants, from which 25.6% were children or adolescents (≤19 years old), 62.9% adults (20 to 59 years old) and 11.5% elderly (≤60 years old). In 2010, the municipality presented a human development index (HDI) of 0.875 and a Gini index of 0.40.7
SUS Family Registration is carried out during the household visits performed by community health agents (CHA) to families living in the coverage area of the PHU. All PHU of Florianópolis have CHA working for the Family Health Strategy (FHS). During the registration, socioeconomic, housing and family members’ health information is obtained from the filling of the A Form of the Primary Health Care Information System. After filling the form, each CHA types the data in the software CadFamWeb, created by the Geoprocessing Sector of the Municipal Health Department of Florianópolis in order to gather the information of the Family Registration. From 1999 on, the PHU of Florianópolis were able to access CadFamWeb through the internet. The Family Registration includes not only the population that attends the PHU, but all families which agreed to being registered. Therefore, the analyzed population is not limited to the health services demand.8
The HBP and/or DM diagnosis is obtained during the Family Registration, through self-reported information (when the individual reports that a previous diagnosis has been given by a physician or another health professional) and/or reports of the use of medication for these diseases (antihypertensive drugs, oral hypoglycemic agents and/or insulin). However, the use of medication was not mandatory to confirm the self-reported diagnosis of HBP and/or DM. The distinction between the clinical types of DM was not analyzed.
The variable ‘education level’ was categorized into 0-4, 5-8, 9-11 and ≥12 complete years of schooling. Age was also divided into four groups: 20-39, 40-59, 60-79 and ≥80 years old. All the adult population registered at CadFamWeb during the analyzed periods was included.
To analyze the evolution of the prevalence of DM, HBP and both diseases combined, a time series analysis was conducted, considering the period from 2004 to 2011. In addition to the graphic representation, the Prais-Winsten generalized linear regression method was used for adjusting first order autocorrelation. Thus, it was possible to evaluate whether the prevalence trends were increasing (positive variation and p-value <0.05), decreasing (negative variation and p-value <0.05) or stationary (p≥0.05).9
For the year of 2011, the prevalences of HBP, DM, and both diseases combined were estimated, according to sex, age group, education level and sanitary district where the individual was registered, with calculation of the confidence intervals (95%CI). The odds ratio [OR] and respective 95%CI, both crude and adjusted, were estimated by logistic regression. In the adjusted analysis, all variables were included simultaneously, with the adoption of a single hierarchical level: for all analysis, the significance level considered was 5%. The modification of the effect by sex was tested, in the association of the variables ‘education level’ and ‘age group’ with the outcomes, and p<0.10 was adopted as interaction evidence.
Based on the information for adults available at CadFamWeb for 2011 (52,556), the minimum OR values which the study could identify as statistically significant, considering an 80% power and a 5% alpha, were estimated later. These estimates considered the prevalences of each exposure and outcome variable. By adopting these parameters, the study was able to detect OR values of 1.08 or higher for all analyzed variables.
The research project was authorized by the Municipal Health Department of Florianópolis and approved by the Ethics Research with Human Beings Committee of the Federal University of Santa Catarina on October 3rd, 2011: Report No. 2033.
Results
The time trend (2004 to 2011) considered the 22,135 individuals registered in 2004; 21,417 in 2005; 46,903 in 2006; 64,981 in 2007; 14,107 in 2008; 15,963 in 2009; 21,190 in 2010 and 52,556 in 2011, a total of 259,252 individuals, or 60.7% of Florianópolis’ population in 2011. For 2011, a total of 70,614 individuals presented active Family Registration, and from these, 52,556 were adults (average age = 43.3±16.6 years old; 20-109 age range). Individuals whose data showed inconsistencies were excluded (n=25).
HBP prevalence increased by 6.5 percentage points (p.p.), from 7% in 2004 to 13.5% in 2011. DM prevalence increased by 2.1 p.p., rising from 2.2% in 2004 to 4.2% in 2011. The increase in prevalences was not steady, that is, there were oscillations during the period. In 2006, the diabetes mellitus prevalences were reduced (-0.1%), similarly and significantly, for men and women. The same occurred with HBP and DM among men. In 2007, the prevalence of the analyzed diseases decreased, except for men who presented HBP and DM combined. In the three following years of the time trend (2008, 2009 and 2010) an increase of the studied diseases’ prevalences was observed, in both sexes, with higher increase for HBP. HBP prevalence varied positively between 2008-2009 and 2009-2010, by 2.3% and 2.1%, respectively (Table 1). For HBP and DM combined, there was equal growth among men and women (0.8%) in the 2008-2009 period; in 2010, HBP+DM prevalence was higher among women (3.5%), than men (2.3%). The three outcomes analyzed showed a decrease in prevalences between 2010 and 2011 (Figure 1).
Table 1 - Trend analysis of diabetes mellitus, high blood pressure and diabetes mellitus +high blood pressure, according to sex, among adults registered in the Brazilian National Health System (SUS) in the municipality of Florianópolis, Santa Catarina State, 2004-2011
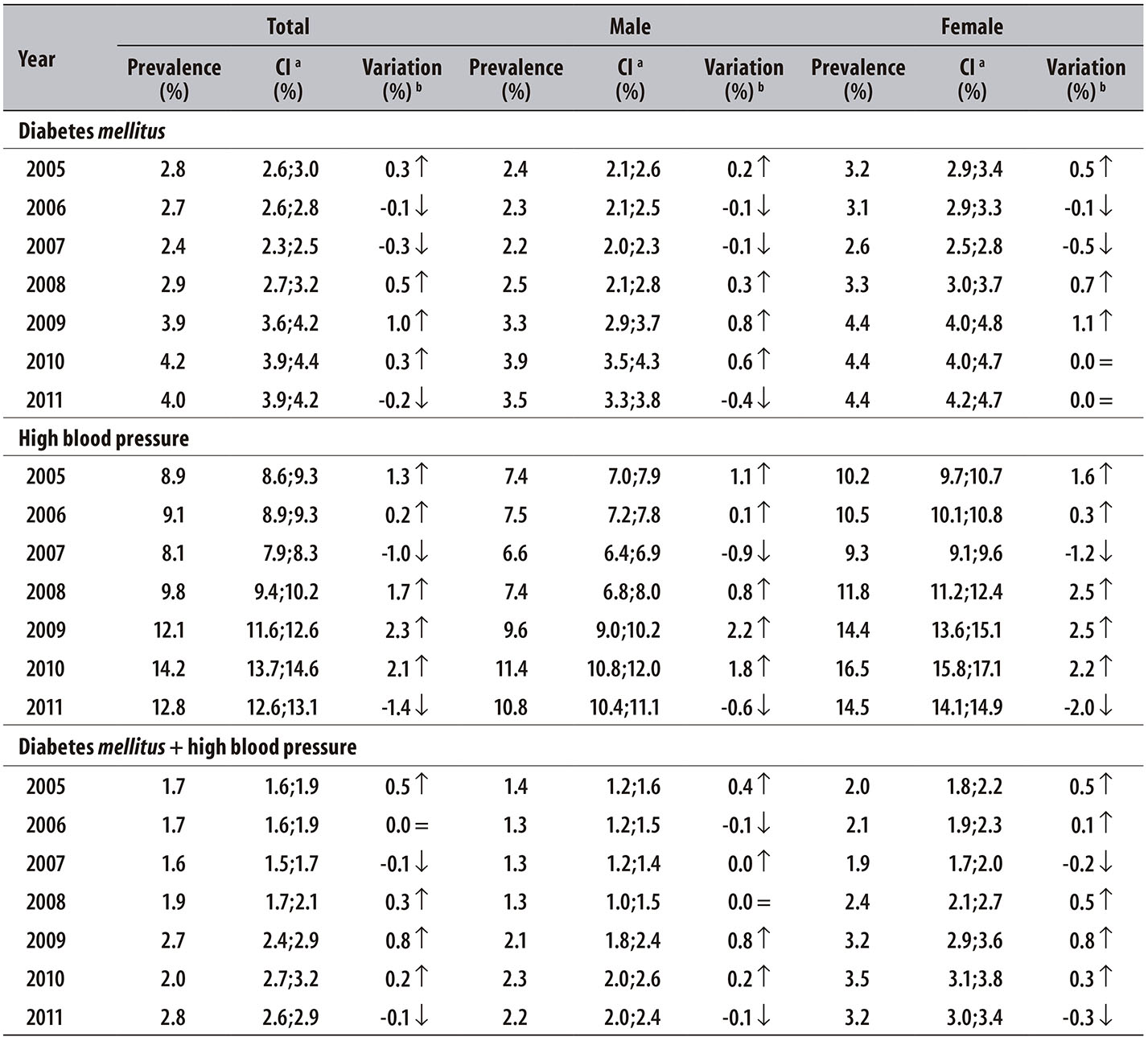
a) CI: confidence interval
b) All variations were significant when p<0.00; Prais-Winsten regression method was used.
Notes:
↓ indicates decreasing trend
↑ indicates increasing trend
= indicates stationary trend
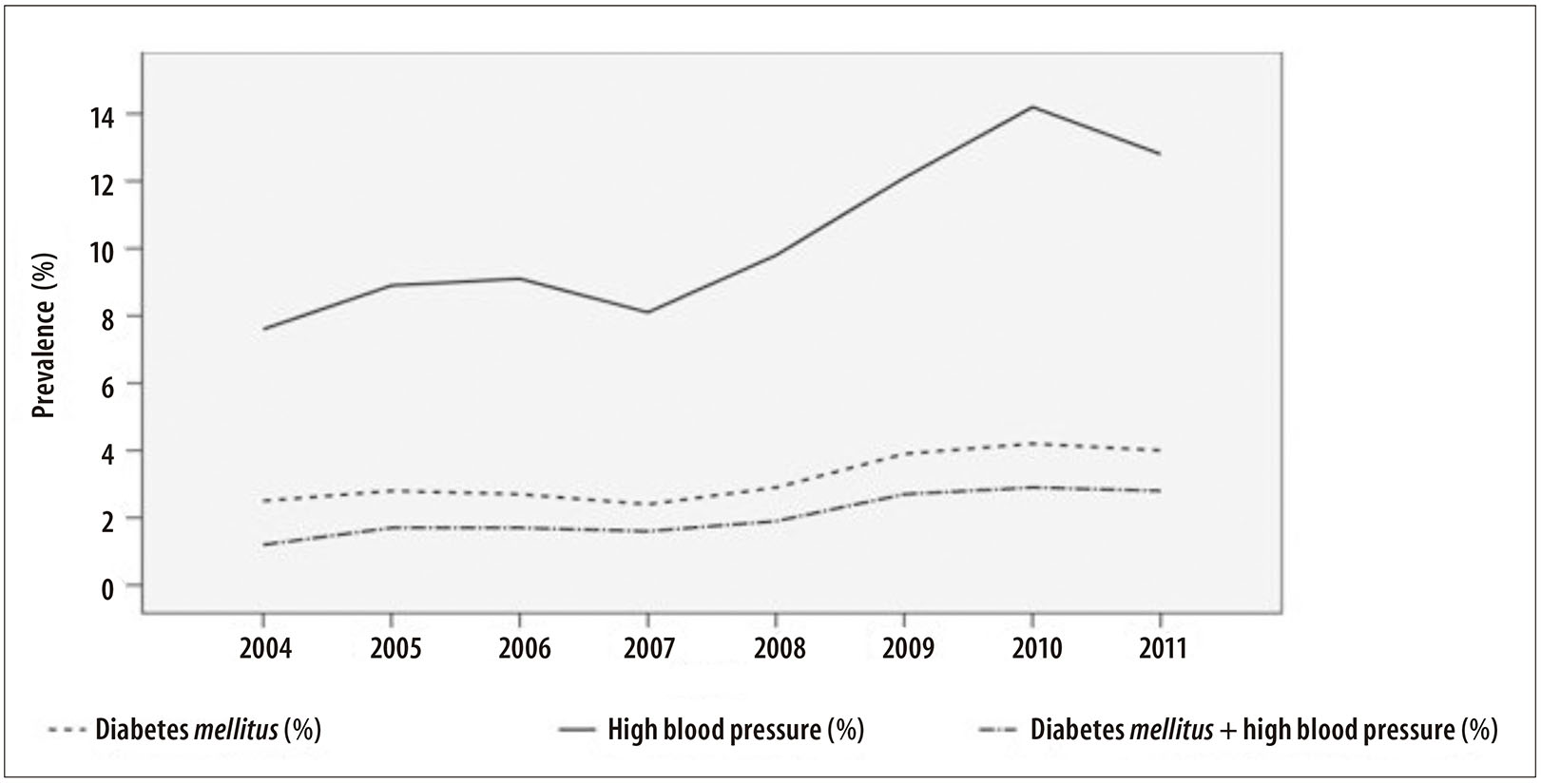
Figure 1 - Evolution of prevalences of diabetes mellitus, high blood pressure and diabetes mellitus + high blood pressure among adults registered in the Brazilian National Health System (SUS) in the municipality of Florianópolis, Santa Catarina State, 2004-2011
Table 2 presents the relative distribution of the population registered in SUS in 2011: most individuals were women (54.9%), the predominant age group was 20-39 years old (48.7%) and the prevailing education level was 9-11 years of schooling (39.0%). The Mainland sanitary district (35.5%) showed the highest number of registers. The total prevalence of HBP identified in 2011 was 13.5% (95%CI: 13.2;13.8) and the total prevalence of DM was 4.2% (95%CI: 4.0;4.4); both diagnoses were present in 2.9% of the population (95%CI: 2.8;3.1) (Table 2).
Table 2 - Population distribution and prevalence of high blood pressure and diabetes mellitus among adults registered in the Brazilian National Health System (SUS) (n=52,556) according to sex, age group, education level and sanitary district of residence in the municipality of Florianópolis, Santa Catarina State, 2011
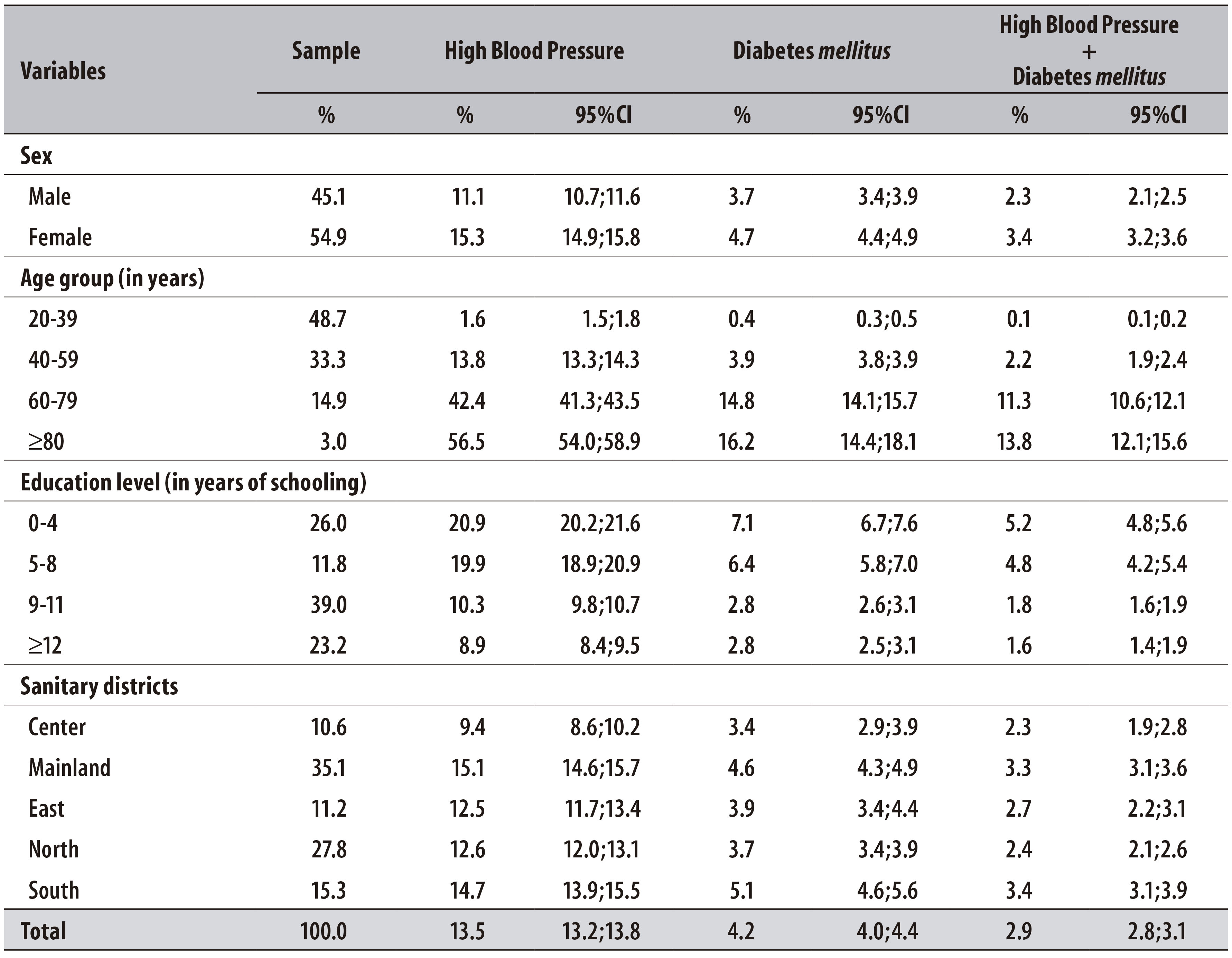
95%CI: 95% confidence interval.
The prevalences of the three outcomes were higher among women. A direct relation between age group and prevalence of the studied diseases was identified, more significant for HBP and DM combined. There was an inverse relation between education level and the prevalence of the three outcomes, although the value for DM was the same among individuals with 9-11 and ≥12 years of schooling. The Mainland and South sanitary districts presented higher prevalences of the diseases (Table 2).
In the crude and adjusted analysis, the variables sex, age group, education level and sanitary district were associated to the outcomes (Table 3). Age group presented a direct relation with HBP; elderly individuals aged 80 and over had 61.2 times more chances of developing the disease when compared to individuals aged 20 to 39. This trend was not observed for DM. Regarding education level, the chances to present HBP or DM were similar among individuals with 0-4 and 5-8 years of schooling, whereas for those who had 9-11 years of schooling, values were closer to those of the reference category. Individuals who lived in the South sanitary district were 2.1 and 1.3 times more likely to present HBP and DM, respectively, when compared to individuals who lived in the Center of Florianópolis; the chances of presenting only DM, among all residents of the other districts, was similar to the one of the Center reference category (Table 3).
Table3 -Crude and adjusted analysis for the association between high blood pressure, diabetes mellitus and high blood pressure + diabetes mellitus combined, according to the variables sex, age group, education level and sanitary district of residence, among adults registered in the Brazilian National Health System (SUS) (N=52,556) in the municipality of Florianópolis, Santa Catarina State, 2011
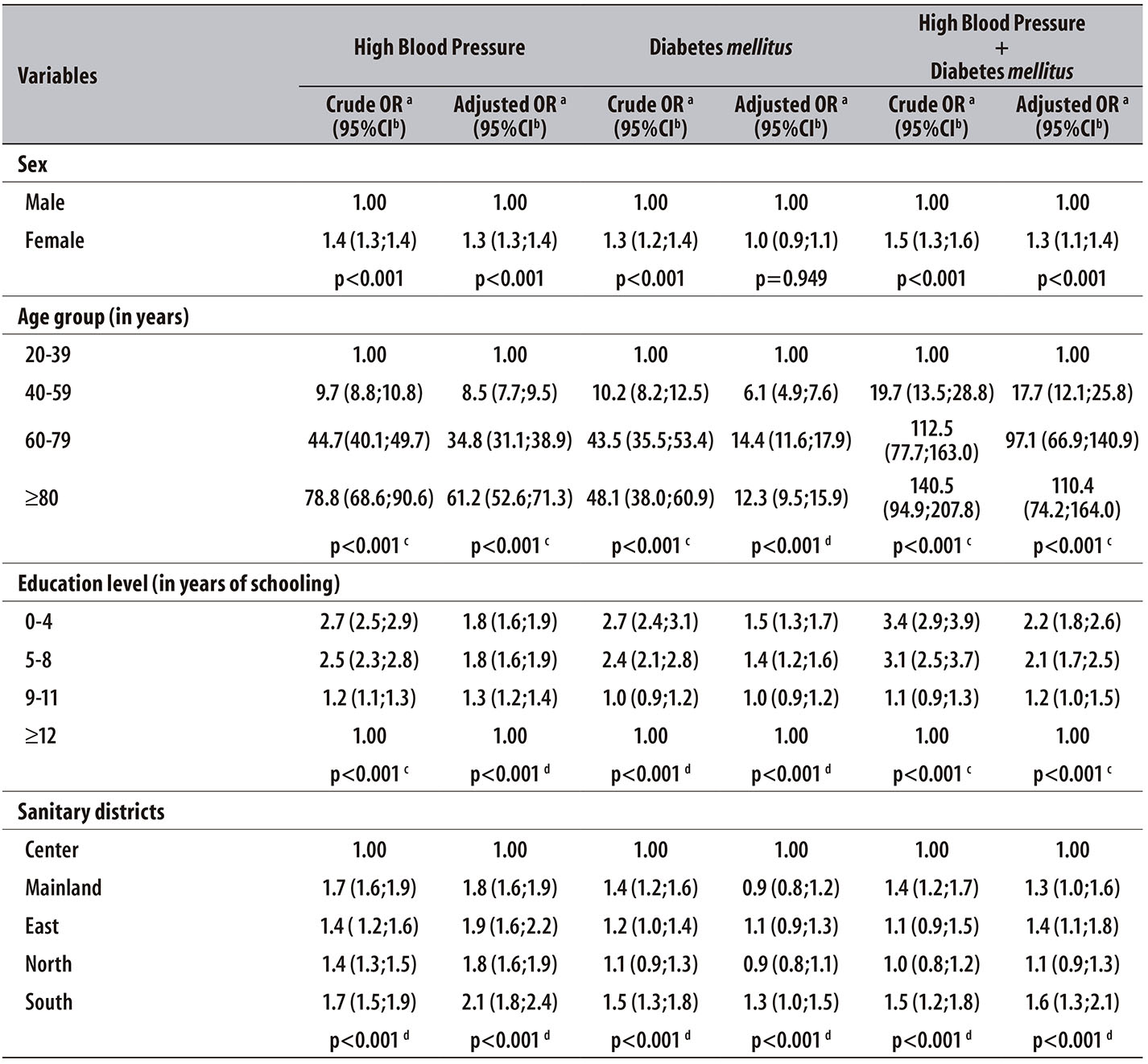
a) OR: odds ratio
b) 95%CI: 95% confidence interval
c) P-value of chi-square for trend
d) P-value of chi-square for heterogeinity
Note:
In the adjusted analysis, all variables were included together, considering a single level of determination.
Figure 2 shows that HBP and DM prevalences among women who had 0-4 and 5-8 years of schooling were almost two times the same prevalences presented among men (p-value of interaction <0.001 in both cases). When comparing the relation in prevalence between the extremes of education level (≥12 years as reference category), among women, the value was 3.4 (95%CI: 3.1;3.8) for HBP and 4.1 (95%CI: 3.4;4.9) for DM; among men, the corresponding values were 1.41 (95%CI: 1.27;1.56) and 1.40 (95%CI: 1.17;1.68). Regarding age group, results were similar among men and women. Only men, however, presented a lower DM prevalence among the elderly aged 80 and over (12.3%) than among men in the 60-79 age group (14.0%) (p-interaction value of 0.3 for DM and 0.04 for HBP).
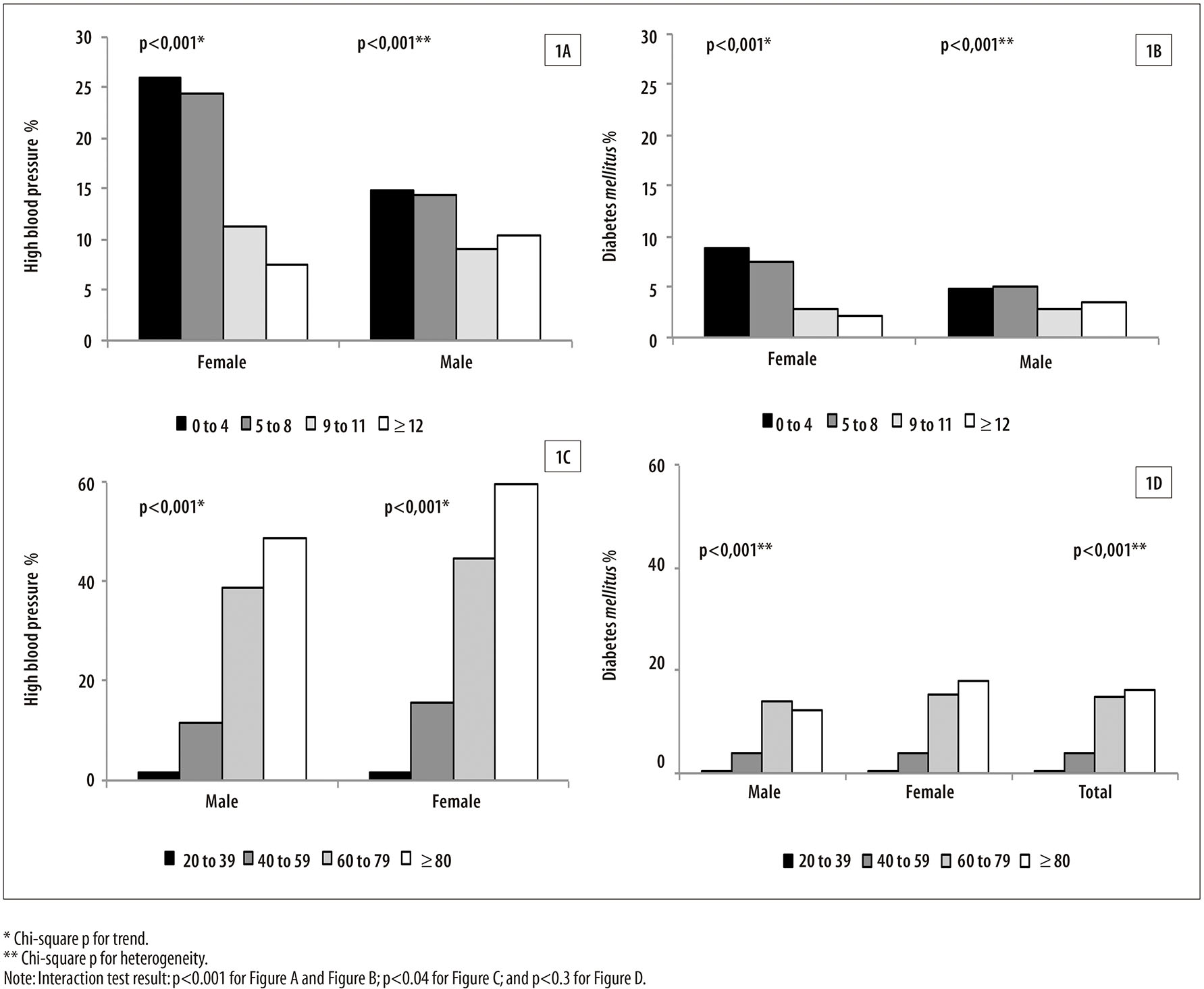
Figure 2 - Prevalences of high blood pressure and diabetes mellitus, according to sex and education level (Figure 1A; Figure 1B), and stratification by sex according to age group (Figure 1C; Figure 1D), among adults registered in the Brazilian National Health System (SUS) in the municipality of Florianópolis, Santa Catarina State, 2011
When analyzing HBP and DM combined (Table 3), statistically significant associations were also observed. Women were 30% more likely to be diagnosed with HBP and DM combined (p<0.001). Cases of both diseases combined have shown a direct relation with age group as well, whereas for education level, the association was inverse. The adjusted chances of both diseases combined were 60% and 40% higher among residents in the South and East of the municipality, respectively, when compared to residents in the Center.
Discussion
In Florianópolis, an increase in the prevalences of HBP and DM was observed during the period from 2004 to 2011. The results are similar to those identified by the 2012 Surveillance System of Risk and Protective Factors for Chronic Diseases by Telephone Survey (Vigitel).3 According to Vigitel, HBP prevalence in Brazil increased in a uniform and statistically significant way, only in the period from 2006 to 2009 (an average increase of 0.7/year). Using data from the National Household Sample Survey, performed by the Brazilian Institute of Geography and Statistics (IBGE), Muniz et al. verified an increase in the self-reported prevalence of HBP, in Brazil and in the South region of the country, from 12.5% in 1988 to 13.9% in 2008.10
In this study, the sharp increase in the prevalences from 2007 onward might be related to the expansion and improvement of the CadFamWeb system (2006) and to the adoption of the internet (2010) for compilation of data from the Family Registration, reducing information loss. The growth of over 100% in the number of Family Health Strategy (FHS) units (from 47 in 2004 to 100 in 2011) in Florianópolis may influence the results. The oscillations in the number of registered individuals each year may be explained by the sociodemographic characteristics of each geographic area - similar to obesity, which, in a period of 34 years, has increased more than four times among men (from 2.8 to 12.4%) and slightly more than two times among women (from 8 to 16.9%).11
In the last two years of the time series, a reduction in HBP prevalence was observed; this behavior was also demonstrated by Vigitel (2012), which identified a HBP prevalence of 24.4% in 2009, and 22.7% in 2011.3 According to WHO, from 1980 to 2008, some high-income countries presented a reduction in the blood pressure average, a fact attributed to Public Health interventions.1 Despite these findings, continuity in the studies related to prevalences is recommended, since they are necessary to confirm such reduction and the efficacy of the actions to tackle HBP.
With regard to DM, according to data from the National Household Sample Survey, an increase in the prevalence of the disease, from 2.9% to 4.3%, in the period between 1998 and 2008, has been observed.12 Data from Vigitel show that the increase in DM prevalence in Brazil, between 2006 and 2011, was significant only for men (+0.2/year; p<0.05),3 a result which differs from the one presented by this study.
In some periods of the time series, the positive variations of prevalences were more marked among women, which is possibly justified by the fact that they use health services more regularly.13
In this study, prevalences of 13.5% for HBP and 4.2% for DM were identified in the year 2011, results similar to those found by Nunes Filho et al. in 2006, in the municipality of Luzerna, located in Santa Catarina State as well (14.7% for HBP and 2.3% for DM).14 Capilheira et al. (2008) found prevalences of 23.8% for HBP and 6.3% for DM in Pelotas, Rio Grande do Sul State, in the year 2003.15 In the municipality of São Paulo, Mion Jr et al. found HBP prevalence of 23%.16 For self-reported DM, a study conducted in Campinas region and in Botucatu, both in São Paulo State, indicated DM prevalence of 15.8%.17 During the same period, international studies performed by Díaz-Apodoca et al., identified DM prevalences of 16.4% in Mexico and 17.2% in the USA, using data obtained by direct measurement or self-reported information.18 In this present study, it was verified that 2.9% of the population registered in SUS in Florianópolis, in the year 2011, presented both HBP and DM. This prevalence is slightly inferior to the prevalences of individuals with HBP and DM in Brazil (3.3%) and in the South region of the country (3.6%) in the year 2008.12
Compared to data from the literature, the prevalences found in this study were less elevated, which can be justified by the fact that 48.7% of the analyzed population was in the age group of 20-39 years old. Although these diseases are less prevalent in this age group, the prevalences found (1.6% for HBP and 0.4% for DM) were inferior to the ones revealed by Vigitel 2011.3 The 20-39 age group is the one that attends health services less regularly,19 which may lead to under-diagnosis. Disease unawareness also occurs among the elderly; in Porto Alegre, capital of Rio Grande do Sul State, from 2005 to 2006, 20.4% of the analyzed elderly were not aware of the DM diagnosis.20
It is important to notice that the population who lives in Florianópolis has a better quality of life and a higher percentage of men (53.0%) and women (30.9%) that practice physical activity when compared to the other Brazilian capitals.3 Considering that it is the third capital with best quality regarding SUS service (IDSUS: 6.67),7 highest income per capita by household and highest HDI, such qualification might favor the verified results.
Prevalences of HBP, DM and HBP+DM were higher among women. Some studies performed in Brazil have also shown this result.21,22 However, this is not a consensus in literature, since studies performed in Luzerna, Santa Catarina and Firminópolis, Goiás, showed higher HBP prevalences among men.14,22 For DM, Nunes Filho et al.14 found higher prevalence among men (4%), and Moraes et al. (2010),24 among women (17%).
The variable ‘sex’ was associated to HBP and also to HBP and DM combined; the association between DM and sex was the only one that did not remain in the adjusted model. Studies conducted with adults in São Carlos, São Paulo State, and Firminópolis, Goiás State, did not identify an association between DM and sex either.16,23
Results also showed that the three outcome prevalences presented direct relation with age group. This relation is documented in other studies.3,25 In two studies, one of them performed by Nascente et al.23 and the other by Moraes et al.,24 age group was preserved in the final model. Here, the highest chances of presenting HBP and DM were identified among individuals aged 60 or over. The body structural changes, natural from the ageing process, cause a diminution in wide caliber arteries, contributing to the increase of blood pressure. For DM, this relation would be connected to preexisting diseases, age-related reduction in the insulin secretion and hormonal transformations in women after the menopause.20
DM prevalence in men decreased among the elderly aged between 60 and 79 and those with 80 or over. In Brazil, in 2010, the expectation men by the age of 60 was to have 19.5 more years of life.7 Thus, the lower DM prevalence in older men might be a consequence of the survival bias;26 and of the unawareness of the disease, reflected on the underreporting of diagnosis.13
Regarding education level, an inverse association with the prevalences of HBP and DM+HBP was observed. Low education level is an indicator capable of influencing the health self-care and treatment compliance.27 The results presented here also showed that the iniquities in health related to education level are more prominent among women. HBP and DM prevalences among women were 3 to 4 times higher in the less educated when compared to the more educated. Among men, this relation was of about 1.5 times for both diseases. Studies emphasize that the magnitudes effects related to obesity and chronic diseases are more noticeable in women, who are the most precociously affected in the nutritional and epidemiological transition process.21,28
In this study, a significant association between education level and the three outcome variables investigated was identified. Moraes et al.24 verified the linear relation between education level and DM, although the variable was not maintained in the final model. However, a study performed in Salvador, capital of Bahia State, in the year 2006, did not find significant association between HBP and education level.21
HBP chances were high in all sanitary districts of Florianópolis when compared to the same chances downtown. Odds were even more significant among residents of the South sanitary district. For DM, only residents of the South region of the municipality presented the highest chances, which might be a consequence of better implementation and maintenance of identification programs in this region. The highest HBP and DM prevalences in the South and Mainland sanitary districts may be related to the greater presence of CHA in these locations: whilst there are 87 CHA in the North district, responsible for 92,031 inhabitants, the South district has 124 CHA for a population of 86,730 inhabitants, and the Mainland has 188 CHA for 85,017 inhabitants.8 The number of CHA per district is determined by the number of Family Health Strategy units; in the Areas of Social Interest, there are more CHA.
A limitation of this study is the possibility of mistakes in the collection and/or typing of data in electronic media, which results from the discrepancies among CHA in the information collection. The self-reported information for HBP and DM diagnosis can be a limitation as well, since it implies the underreporting of patients who are not aware of such diagnoses. Nevertheless, studies of validation of self-reported information show sensitivity and specificity values between 87 and 92%, when compared to values referred by clinical diagnosis, which reduces the biases probability in the results presented.29 In addition, self-reported information about HBP and DM are used in Vigitel, an important population-based survey for monitoring risk and protective factors for chronic diseases in Brazil.3 The highest DM prevalence among women, verified in this study, differs from the results of studies found in literature, which may also be a limitation, due to the highest attendance of health services by women.
Despite some restrictions, the use of secondary data has been growing, and one of its advantages is the low cost involved in population-based studies. Analyses of information collected by community health agents in Family Registration are important, because they can provide guidance for actions aiming at preventing complications caused by HBP and DM in population areas of greater risk. Although Family Registration in SUS does not differentiate between DM types, we believe that this would hardly affect the results of a study as this.5
In the time series, the prevalences of high blood pressure and diabetes mellitus doubled in the period between 2004 and 2011. In spite of this reality, the values found are below the prevalences described in the Brazilian scientific literature. The increase of these conditions’ prevalences and the verified associations are important, considering their potential contribution for planning actions aimed at preventing diseases and promoting health in Primary Care.
REFERENCES
1. World Health Organization. World health statistics: a snapshot of global health. Geneva: World Health Organization; 2012. [ Links ]
2. U. S. Department of Health and Human Services. Center of Disease Control and Prevention. National Center for Health Statistics. Hyattsville: National Center for Health Statistics; 2010 [cited 2017 Apr 12]. Available from: Available from: http://www.cdc.gov/nchs/data/hus/hus10.pdf [ Links ]
3. Secretaria de Vigilância em Saúde. Vigitel Brasil 2011: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico. Brasília: Ministério da Saúde; 2012. [ Links ]
4. Dib MW, Riera R, Ferraz MB. Estimated annual cost of arterial hypertension treatment in Brazil. Rev Panam Salud Publica. 2010 Feb;27(2):125-31. [ Links ]
5. Sociedade Brasileira de Diabetes. Diretrizes da Sociedade Brasileira de Diabetes. 3 ed. Itapevi, SP: Sociedade Brasileira de Diabetes; 2009. [ Links ]
6. Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. SIAB: manual do sistema de informação de atenção básica. Brasília: Ministério da Saúde; 2003. [ Links ]
7. Instituto Brasileiro de Geografia e Estatística. Diretoria de Pesquisas. Coordenação de População e Indicadores Sociais. Nota: Estimativas da população residente com data de referência 1º de julho de 2011. Rio de Janeiro: Fundação Instituto Brasileiro de Geografia e Estatística; 2012. [ Links ]
8. Secretaria Municipal de Saúde (Florianópolis). Secretaria Municipal de Saúde [Internet]. Florianópolis: Prefeitura de Florianópolis; 2011 [citado 2011 mai 7]. Disponível em: Disponível em: http://portal.pmf.sc.gov.br/entidades/saude/ [ Links ]
9. Antunes JLF, Cardoso MRA. Uso de análise de séries temporais em estudos epidemiológicos. Epidemiol Serv Saude. 2015 jul-set;24(3):565-76. [ Links ]
10. Muniz LC, Cascaes AM, Wehrmeister FC, Martínez-Mesa J, Barros AJD, Menezes AMB. Trends in self-reported arterial hypertension in Brazilian adults: an analysis of data from the Brazilian National Household Sample Survey,1998-2008. Cad Saude Publica. 2012 Aug;28(8):1599-607. [ Links ]
11. Instituto Brasileiro de Geografia e Estatística. Diretoria de Pesquisas. Coordenação de Trabalho e Rendimento. Pesquisa de Orçamentos Familiares 2008-2009: antropometria e estado nutricional de crianças, adolescentes e adultos no Brasil [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2010 [citado 2011 mai 7]. Disponível em: Disponível em: http://biblioteca.ibge.gov.br/visualizacao/livros/liv45419.pdf [ Links ]
12. Freitas LRS, Garcia LP. Evolução da prevalência do diabetes e deste associado à hipertensão arterial no Brasil: análise da Pesquisa Nacional por Amostra de Domicílios, 1998, 2003 e 2008. Epidemiol Serv Saude. 2012 jan-mar;21(1):7-19. [ Links ]
13. Instituto Brasileiro de Geografia e Estatística. Indicadores Sociodemográficos e de Saúde no Brasil: 2009 [Internet]. Rio de Janeiro: Fundação Instituto Brasileiro de Geografia e Estatística; 2009 [citado 2011 mai 7]. (Estudos e pesquisas Informação Demográfica e Socioeconômica, 25). Disponível em: Disponível em: http://www.ibge.gov.br/english/estatistica/populacao/indic_sociosaude/2009/indicsaude.pdf [ Links ]
14. Nunes Filho JR, Debastiani D, Nunes AD, Peres KG. Prevalência de fatores de risco cardiovascular em adultos de Luzerna, Santa Catarina, 2006. Arq Bras Cardiol. 2007 nov;89(5):319-24. [ Links ]
15. Capilheira MF, Santos IS, Azevedo Júnior MR, Reichert FF. Fatores de risco para doenças crônicas não-transmissíveis e a Iniciativa CARMEN: estudo de base populacional no sul do Brasil. Cad Saude Publica. 2008 dez;24(12):2767-74. [ Links ]
16. Mion Júnior D, Pierin AM, Bensenor IM, Marin JCM, Costa KRA, Henrique LFO, et al. Hipertensão arterial na cidade de São Paulo: prevalência referida por contato telefônico. Arq Bras Cardiol. 2010 jul;95(1):99-106. [ Links ]
17. Francisco PMSB, Belon AP, Barros MBA, Carandina L, Alves MCGP, Goldbaum M, et al. Diabetes auto-referido em idosos: prevalência, fatores associados e práticas de controle. Cad Saude Publica. 2010 jan;26(1):175-84. [ Links ]
18. Díaz-Apodaca BA, Ebrahim S, Mccormack V, De Cosío FG, Ruiz-Holguín R. Prevalence of type 2 diabetes and impaired fasting glucose: cross-sectional study of multiethnic adult population at the United States-Mexico border. Rev Panam Salud Publica. 2010 Sep;28(3):174-81. [ Links ]
19. Sala A, Cohen DD, Dalmaso ASW, Lima AMM, Teixeira RR. Avaliação do processo de atendimento a pacientes portadores de doença crônico-degenerativa em uma unidade básica de saúde. Rev Saude Publica. 1993 dez;27(6):463-71. [ Links ]
20. Viegas K. Prevalência de diabete mellitus na população de idosos de Porto Alegre e suas características sociodemográficas e de saúde [tese]. Porto Alegre: Pontifícia Universidade Católica do Rio Grande do Sul, Departamento de Geriatria e Gerontologia; 2009. [ Links ]
21. Lessa I, Magalhães L, Araújo MJ, Almeida Filho N, Aquino E, Oliveira MMC. Hipertensão arterial na população adulta de Salvador (BA) - Brasil. Arq Bras Cardiol. 2006 dez;87(6):747-56. [ Links ]
22. Oliveira LPM, Assis AMO, Silva MCM, Santana MLP, Santos NS, Pinheiro SMC, et al. Fatores associados a excesso de peso e concentração de gordura abdominal em adultos na cidade de Salvador, Bahia, Brasil. Cad Saude Publica. 2009 mar;25(3):570-82. [ Links ]
23. Nascente FMN, Jardim PCBV, Peixoto MRG, Monego ET, Barroso WKS, Moreira HG, et al. Hipertensão arterial e sua associação com índices antropométricos em adultos de uma cidade de pequeno porte do interior do Brasil. Rev Assoc Med Bras. 2009;55(6):716-22. [ Links ]
24. Moraes AS, Freitas ICM, Gimeno SGA, Mondini L. Prevalência de diabetes mellitus e identificação de fatores associados em adultos residentes em área urbana de Ribeirão Preto, São Paulo, Brasil, 2006: Projeto OBEDIARP. Cad Saude Publica. 2010 mai;26(5):929-41. [ Links ]
25. Carnelosso ML, Barbosa MA, Porto CC, Silva AS, Carvalho MM, Oliveira ALI. Prevalência de fatores de risco para doenças cardiovasculares na região leste de Goiânia (GO). Cienc Saude Coletiva. 2010 jun;15 supl 1:1073-80. [ Links ]
26. Ministério da Saúde (BR). Sistema de Informações do SUS. Informações de Mortalidade - Santa Catarina (Brasil) [Internet]. Brasília: Ministério da Saúde; 2011 [citado 2012 jun 28]. Disponível em: Disponível em: http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sim/cnv/obt10sc.def (acessado em: 28/Jun/2012). [ Links ]
27. Gallegos EC, Ovalle-Berúmen F, Gomez-Meza MV. Metabolic control of adults with type 2 diabetes mellitus through education and counseling. J Nurs Scholarsh. 2006;38(4):344-51. [ Links ]
28. González D, Nazmi A, Victora CG. Pobreza na infância e obesidade abdominal na vida adulta: revisão sistemática. Cad Saude Publica. 2009;25supl 3:S427-40. [ Links ]
29. Chrestani MAD, Santos IS, Matijasevich AM. Hipertensão arterial sistêmica auto-referida: validação diagnóstica em estudo de base populacional. Cad Saude Publica. 2009 nov;25(11):2395-2406. [ Links ]
*Article based on the Master's thesis entitled 'Hipertensão arterial sistêmica e diabetes mellitus em adultos e idosos cadastrados no Sistema Único de Saúde (SUS) na cidade de Florianópolis-SC', defended by Catiuscie Cabreira da Silva at the Programme of Post-graduation in Nutrition of the Federal University of Santa Catarina, in 2012. To support the research, the main author received a scholarship from the Coordination for the Improvement of Higher Education Personnel, which belongs to the Ministry of Education (CAPES/MEC).
Received: July 09, 2016; Accepted: January 22, 2017
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
