










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde v.26 n.3 Brasília jul./set. 2017
http://dx.doi.org/10.5123/s1679-49742017000300006
ORIGINAL ARTICLE
Breast Cancer screening in Minas Gerais: assessment of data from information health systems of the Brazilian National Health System*
1Universidade Federal de Juiz de Fora, Núcleo de Assessoria, Treinamento e Estudos em Saúde, Juiz de Fora-MG, Brasil
2Universidade Federal de Juiz de Fora, Departamento de Saúde Coletiva, Juiz de Fora-MG, Brasil
3Universidade Federal de Juiz de Fora, Programa de Pós-Graduação em Saúde Coletiva, Juiz de Fora-MG, Brasil
4Universidade Federal de Juiz de Fora, Departamento de Saúde Coletiva, Juiz de Fora-MG, Brasil
OBJECTIVE:
to assess the results of indicators related to the supply of mammography and level of adequacy of diagnostic confirmation for mammograms with suspicious findings of malignancy in Minas Gerais state and its health macroregions.
METHODS:
this is an evaluation study performed with data from the Breast Cancer Information System and the Outpatient Information System for the years 2010 and 2011.
RESULTS
: the ratio of mammograms in women aged 50 to 69 years was of 0.14 in 2010 (goal: 0.12) and 0.15 in 2011 (goal: 0.16); most mammograms were performed on annual basis, and a high percentage of exams conducted in age groups which are not recommended by the Ministry of Health was observed; the ratio between biopsies and mammograms with suspicious findings of malignancy was of 0.31 (2010) and 0.42 (2011).
CONCLUSION:
the screening of breast neoplasms did not reach its goal in 2011 and there was a low rate of diagnostic confirmation for mammograms with suspicious findings of malignancy.
Keywords: Breast Neoplasms; Mass Screening; Women's Health; Mammography; Health Services Evaluation
Introduction
After non-melanoma skin cancer, breast cancer was the most incident in women of almost all the major regions of Brazil, in 2014 - except in the Northern region, where the cervical cancer occupies the first position in the ranking that year.1 The mortality rate for breast cancer, adjusted by the world's population, is growing and represents the leading cause of death by cancer in Brazilian women: 12.66 deaths/100 thousand women in 2015.2
Mammography is considered a effective method of early detection of breast cancer, being widely used in screening programs.3 This exam aims to identify non-detectable tumors on clinical examination of the breast, allowing the early beginning of treatment, and consequently it improves the prognosis.4 It is estimated that mammography screening conducted through organized programs reduce breast cancer mortality around 20% after 13 years of follow-up.5 In Brazil, from the early 1990, the breast cancer showed a decline trend in mortality in the capitals of Southern and Southeastern regions, possibly related to greater access to mammography and the specialized treatment services.6
Regarding the age range and frequency of screening, there are differences in recommendations amidst the main institutions of the world. The American Cancer Society recommends the annual mamographic screening in women in the age range from 45 to 54 years. Women from 40 up to 44 years old should have the chance to initiate the annual. The regularity recommended by the American Cancer Society starts to be biennial to women from 55 years old or more.7 The screening must continue until the moment at which it is considered that women are in good health condition, and with a life expectancy of ten years or more.7 In the United kingdom, the age range recommended is more extensive, from 50 to 70 years old, with triennial regularity, though.5 The World Health Organization (WHO) recommends the accomplishment of the screening by programs organized to assist women from 50 to 69 years old, with biennial regularity.3
In Brazil, the Ministry of Health recommends the accomplishment of mammography in women in the age range from 50 to 69 years old, with biennial regularity.1 In the country, screening is carried out through a so-called opportunistic manner, which means that the request of examination depends on the spontaneous demand for the health service. On the other hand, in developed countries, there is active search for the target population.8 In addition to the opportunistic screening being less effective, its impact on the mortality attributed to the tracked condition is more onerous to the health system.9
In 2009, the Ministry of Health implemented the Breast Cancer Information System (SISMAMA), a subsystem of the SUS Ambulatory Care Information System (SIA/SUS), in order to enable the management of actions to early detect breast cancer.10
Due to the great extension of the state of Minas Gerais and its regional diversity, the evaluation of the result of the state-level screening actions allows to monitor the agreed indicators, to identify its relevant regional differences and to contribute to the health planning in the state.
The objective of this study was to evaluate the result of indicators related to the supply of mammography, and to the degree of adequacy of the diagnostic confirmation for mammographies with suspicious results of malignity in the state of Minas Gerais and its health’s macroregions.
Methods
This is an evaluation study based on secondary data, related to Minas Gerais state and its health macroregions in the period of 2010 and 2011. The state has 853 municipalities, 77 micro-regions and 13 macroregions characterized by great socioeconomic disparity. In 2010, the population in Minas Gerais state was of 19,597,330 inhabitants, 50.8% female, being 1,730,927 (17.4%) of these women in the age range from 50 to 69 years old.
The secondary data were originated from SISMAMA and SIA/SUS, extracted from the IT Department of the Brazilian National Health System (Datasus: www.datasus.gov.br). Among other functions, the SISMAMA allows monitoring actions of screening, standardizes and improves the quality of mammographic reports, and allows the follow-up of women with altered tests.11 As SISMAMA presents data from July 2009, we decided to analyze the figures for 2010 and 2011, consulted in the months of May and June 2016. The data concerning the female population used in the denominator were obtained from the Census of population estimates of 2010 and 2011 conducted by the Brazilian Institute of Geography and Statistics. The description of the calculated indicators and their data sources are in Figure 1.

Figure 1 - Description of the calculated indicators and their data sources of evaluation studies for breast cancer screening in Minas Gerais state, 2010-2011
Mammographic supply was analyzed by the indicator ratio of mammograms in women from 50 to 69 years old, used in the Pact for Health,12 considered proxy of coverage, which includes the total number of mammograms, regardless of clinical indication.13 This indicator's goal was obtained from the Information System of the Pact for Health (SISPACTO) and for its calculation, we used the data of SIA/SUS, which featured the largest number of registered examinations in relation to the SISMAMA. When identified unilateral mammography registry in SIA/SUS, half of procedures were performed, in order to be equivalent to the number of women examined.14 In relation to the characterization of the supply indicators of mammography (mammography ratio by age group, frequency, clinical indication, categorization of the mammography report) and indicators related to the time of the examination, the data were obtained from SISMAMA, because the foundations of the SIA/SUS no availability of this information.
Mammographic report generated in SISMAMA is based on the categorization of the Breast Imaging Reporting and Data System (BI-RADS), which standardizes the reports and guides the conduct to be taken. BI-RADS categories 4 and 5 are classified as 'suspicious findings of malignancy' and 'highly suggestive findings of malignancy', respectively, and the conduct recommended for these findings is to perform a biopsy. So we used the indicator ratio of biopsies and number of mammograms with BI-RADS 4 and 5 results in order to assess the degree of adequacy of diagnostic confirmation for mammograms suspected of malignancy.14
The raw data were analyzed descriptively by TabWin (version 3.2) and Microsoft Excel 2007, upon the calculation of the indicators expressed in ratios and proportions. Proportions were compared to the Chi-square test (c2).
This study is part of a wider research project, which aimed to analyze the results of the stipulated actions for Live Life Network (Rede Viva Vida) related to cervix and breast cancer screening in the period from 2006 to 2011, and was approved by the Research Ethics Committee of the Universidade Federal de Juiz de Fora under the Report n° 1,376,660, in 18 December 2015.
Results
In Minas Gerais, the ratio of mammograms in women from 50 to 69 years old was 0.14 and surpassed the goal agreed in 2010 (0.12); in 2011, however, it was of 0.15, shorter than the goal of 0.16 (Table 1).
Table 1 - Ratio of mamogramms a in women in the age group from 50 to 69 years old (N=502.588), per year, and proportional distributions of screening mammography acoording to the age group (N=800.423), per year, in the health macroregions of Minas Gerais state, 2010-2011
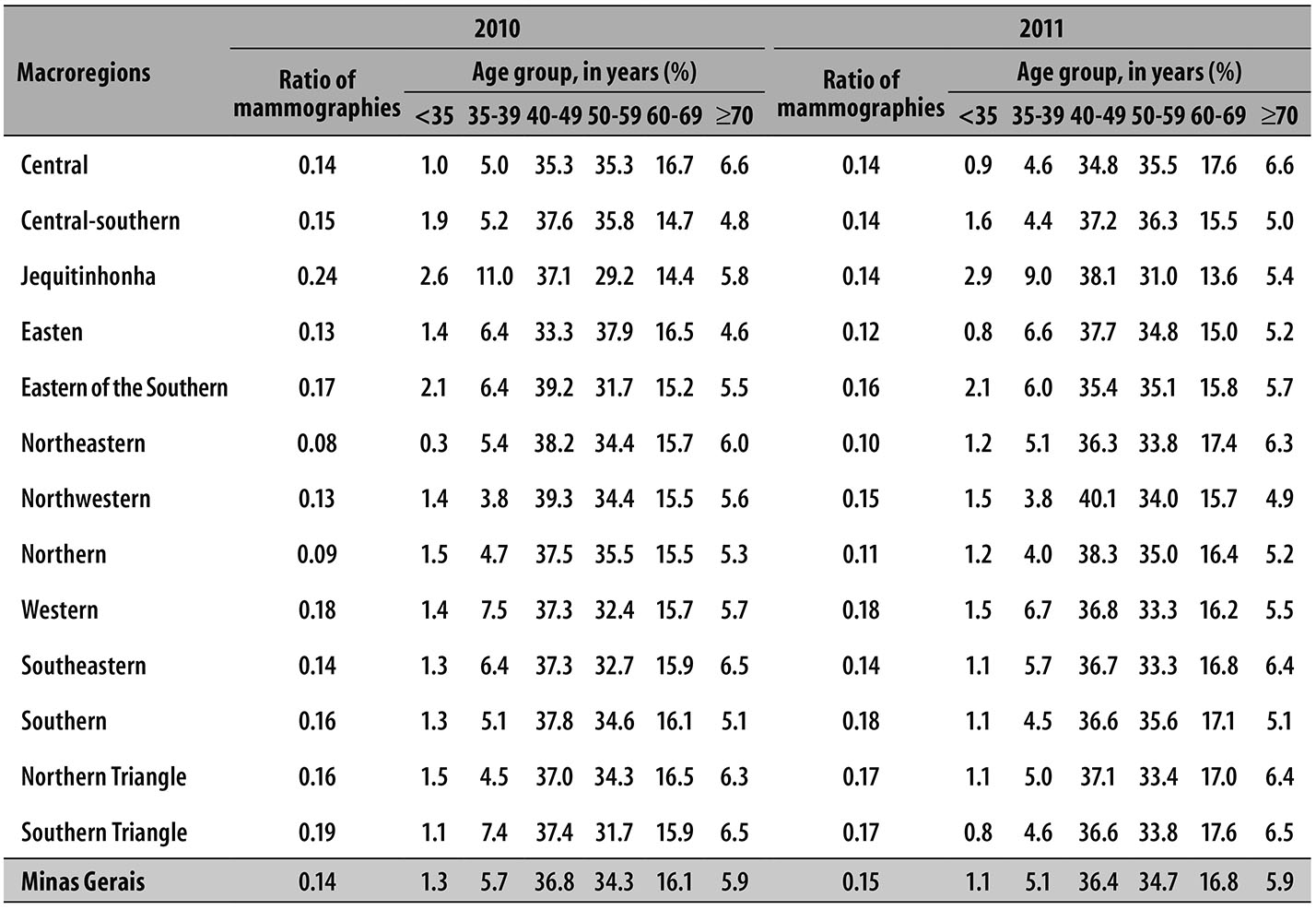
a) Ratio of mammograms: ratio between the number of mammograms in women from 50 to 69 years and the total amount of women in this age group.
Nearly half of the screening mammographies in Minas Gerais was conducted in women younger than 50 years old. In the State and in most of its macroregions, during the two years analyzed, the percentage of exams at the age range from 40 to 49 years old exceeds the percentage of the age range from 50 to 59 years old and from 60 and the 69. Jequitinhonha macroregion stands out in this period, with the highest percentage of screening mammography comprehending the age group below 50 years old (Table 1).
Considering the proportion of mammography screening performed in women from 50 to 69 years old with previous examination (data not presented), most women from Minas Gerais state from 50 to 54 years old reported they had already undergone a mammogram previously: 76.1% in 2010 and 78.4% in 2011. In the age group from 65 to 69 years old, contrary to expectations, the State of Minas Gerais and most of its macroregions showed lower percentage of previous mammogram, in comparison to the age range from 50 to 54 years old. On this indicator, Jequitinhonha macroregion draws attention in 2010: only 27.3, 23.4, and 21.4% of women who had undergone screening mammography in the age groups of 55-59, 60-64 and 65-69 years, respectively, reported previous examination.
The proportional distribution analysis of the time since the previous mammogram in women from 50 to 69 years old who underwent screening mammography (Table 2)
Table 2 - Proportional distribution for the time lapse of performance of previous mammogram in women in the age group from 50 to 69 years old (N=261.936) who had undergone screening mammography, according to age group, in the health macroregions of Minas Gerais, 2010-2011
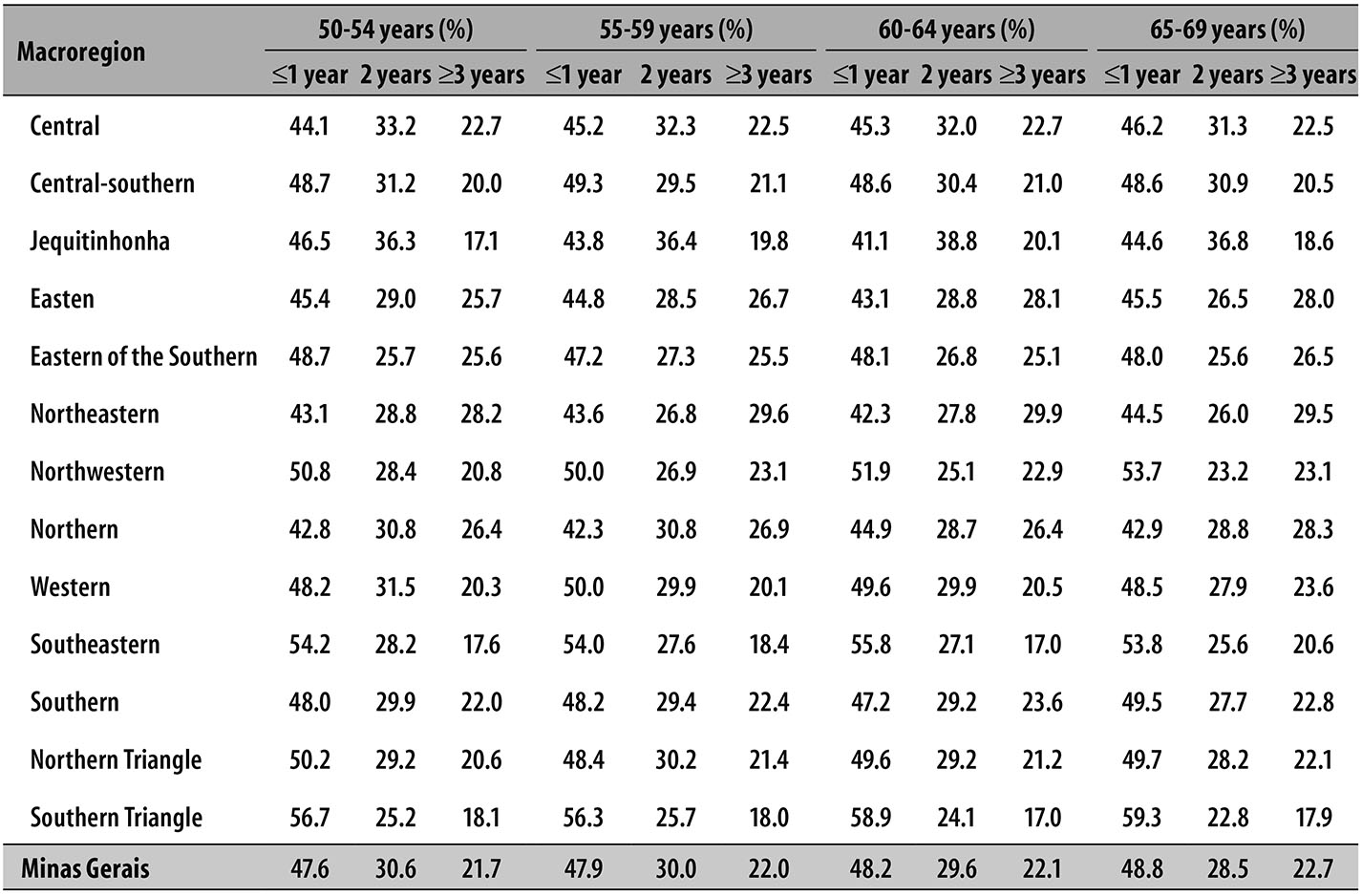
Note: The age above 70 years old was excluded from this analysis for being outside the target age group of the screening program.
showed that, for all age groups, most of previous mammograms was held in the period of up to one year.
Most mammographic exams performed in Minas Gerais state had the clinical indication for screening: 96.7% in 2010 and 96.8% in 2011 (data not presented). In all analyzed age groups, the percentage of screening mammographies was superior to the diagnostic ones, including the age at which mammographm is not recommended. In the age group from 40 to 49 years old and 70 years and over, most of the macroregions showed percentage above 98% for screening mammographies.
According to the proportional distribution of BI-RADS category, as per clinical indication of mammograms in Minas Gerais state (Table 3), there is greater concentration of examinations in BI-RADS categories 1 and 2 for screening mammography, in all age groups. For diagnostic mammographies, in 2010, there was a higher concentration of BI-RADS examinations 2 and 3 in the age groups from 50 to 59 years, 60 to 69, and 70 and more; in 2011, for all age groups, except from 40 to 49 years old. As expected, the percentage of BI-RADS 4 and 5 is greater for diagnostic mammographies in all age groups.
Table 3 - Proportional distribution for mammograms (N=828.016) within each BI-RADSa category according to clinical indication for mammograms, per year and age group, in Minas Gerais state, 2010-2011
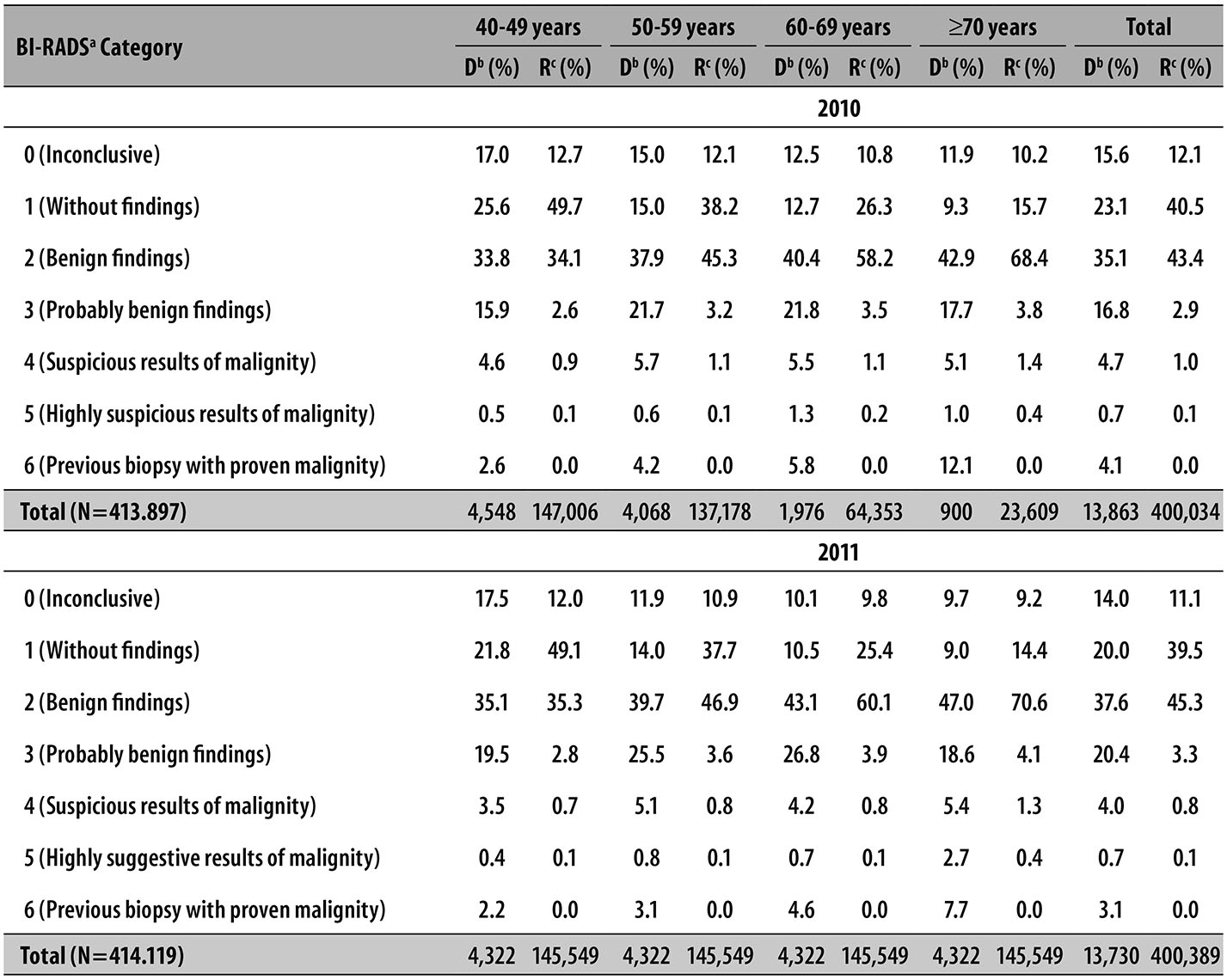
a) BI-RADS: Breast Imaging Reporting and Data System
b) D: diagnostic
c) S: screening
In Minas Gerais state, more than 58% of mammograms were performed within up to 30 days (data not presented). In 2010, the percentage of diagnostic mammographies completed in up to a 30 days was higher than the screening mammography (68.9% and 65.7%, respectively). In 2011, the former was lower than the latter (59.0% to 62.9%, respectively), both statistically significant (p < 0.01). In 2011, Jequitinhonha macroregion presented only 38.7% of diagnostic mammographies carried out in up to 30 days. Considering the release of the result, most mammograms presented results released in up to 30 days (up to 89%). In Minas Gerais state, in 2010, the percentage of results of diagnostic mammographies that were released in up to 30 days was lower than the ones of screening mammographies (89.5% and 92.3%, respectively), while in the following year, 2011, these same percentages were very close (92.2% and 92.4%, respectively). In 2011, the Jequitinhonha macroregion presented the worst percentage, 40.7%, and the Southeastern region, the better, with 100% of their diagnostic mammographies with result released in up to 30 days.
Considering the ratio of biopsies performed and classified mammograms as BI-RADS 4 or 5 (Table 4), there is great difference amongst the macroregions, and the Western macroregion presented the worst ratio for all age groups, except for women from 50 to 59 years and with 70 or more years in 2011, when the Central-southern macroregion presented the worst ratio. In 2011, the Southeastern macroregion presented the best ratio - except for the age group from 40 to 49 years, with emphasis on the age group of 70 years old and over, in which the ratio was 0.99. In Minas Gerais state, in 2011, there was an improvement in that ratio, for all age groups.
Table 4 - Ratio between biopsy and mammograms (N=4.030) with BI-RADSa 4 results (suspicious of malignity) and 5 (highly suggestive of malignity), per age group, in the health macroregions of Minas Gerais state, 2010-2011
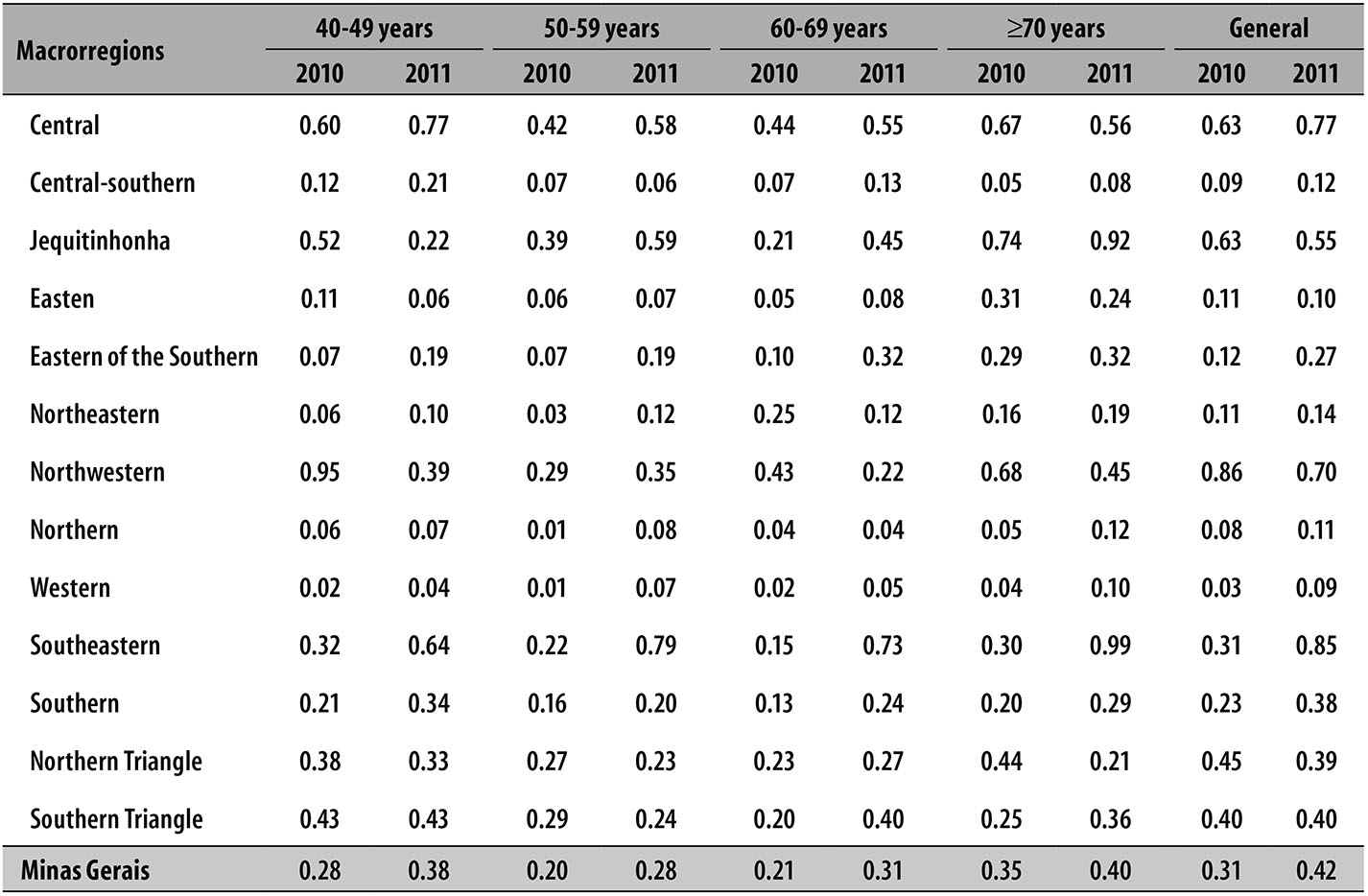
a) BI-RADS: Breast Imaging Reporting and Data System
Note: To the calculation of the ratio, it was used the highest number of biopsies (according to the Breast Cancer Information System [SISMAMA] or the SUS Ambulatory Care Information System [SIA/SUS]).
Discussion
Minas Gerais state did not reach the goal of the indicator ratio of mammograms in women from 50 to 69 years, in 2011. Most of the tests were conducted in women who do not belong to the target age range recommended by the Ministry of Health and most of the mammograms had annual periodicity. Additionally, it was found low ratio of diagnostic confirmation for suspect of malignancy mammographic findings.
Minas Gerais state is characterized by great economic disparity amidst its health macroregions, two clusters deserves to be highlighted due to their Gross Domestic Product (GDP) per capita in 2011: on the one hand the Northeastern, Jequitinhonha, Northern and Eastern of the Southern macroregions which present the lowest GDP; on the other hand, the Northern Triangle, Central, Southern Triangle and Southern present the highest values. Thus, the State is considered a representation of Brazilian regional structure, with a poorer and less developed region northern/northeastern, and a rich and developed region to the South.15
The analysis of the indicator ratio mammograms in women from 50 to 69 years old in Minas Gerais state indicates low access of the target population to the screening program in 2011, not reaching the goal agreed for the State in that year (0.16). Northern and Northeastern macroregions, the poorest of the State, presented the smallest ratios, while Southern Wester and Triangle ones, which are richer than the first, presented greater values. Central and Southeastern macroregions, which also present better socioeconomic level, showed intermediate values. The present study is based only on data of the SUS. It is worth mentioning that macroregions with high supplementary health coverage may show lower ratio in relation to others with greater use of the SUS network, once your denominator considers the total female population and not only the SUS-dependent women. In addition, it does not portray the real coverage of the target population of the screening, since it is evaluated the provision of mammogram based on the number of exams and not on the examined women.12
An ecological study conducted in Minas Gerais state also found smaller ratios in mammograms in women from 50 to 69 years old in the State's poorest macroregions (Northwestern, Northern and Northeastern), during the period from 2008 to 2012. This study verified high health vulnerability in the Northern, Northwestern, Northeastern, Jequitinhonha and Eastern macroregions, and low vulnerability in the Triangle, Central and Southern micro-regions. As the availability of equipment in the 77 microregions of the State, only in six of them, located in the Northern and Northeastern macroregions, presented the number of mammograms for 100 thousand inhabitants below the recommended by the Ministry of Health (less than 0.42) in the analyzed period.16 Therefore, in Minas Gerais state, the amount of mammograms available by the SUS is satisfactory, except in the Northern and Northeastern macroregions, which are poorer. This fact may be related to lower ratio of mammograms verified in these macroregions by the present study.
Most mammography screening in Minas Gerais state was held with annual periodicity and high percentage of exams in age groups not recommended, especially in women from 40 to 49 years. Considering age groups,17 it was observed similar results in the municipality of Goiânia-GO in 2010: 44% of screening mammographies were performed in the age group from 40 to 49 years, 31.7%, from 50 to 59 years, and 13.2% from 60 to 69 years. Another study conducted with SISMAMA which considered Brazil, for the period from September 2009 to July 2010, also found that 44% of screening mammographies were performed in women under 50 years old.18
According to INCA,19 it is expected a small percentage of mammograms in women outside the target age group of the screening program, because the Ministry of Health recommends that the screening gets started before the age of 50 years old in those women who present high risk for breast cancer. As only 1% of the female population presents such a risk,19 the percentage of tests under 50 years old is excessively high,18 indicating that many women initiate the screening before the recommended period.
As medical advice is a strong predictor for mammogram,20 such findings may be related to the recommendations of other scientific societies,14 such as the Brazilian Society of Mastology and the Brazilian Federation of Gynecology and Obstetrics Associations, which advocate screening mammography in the age group from 40 to 69 years, with annual periodicity.21 Corroborating this, a study conducted in a SUS reference center in Pernambuco state found that most screening mammography performed on women from 40 to 49 years was requested by gynecologists and breast specialists: 84% and 16%, respectively.22
Considering screening mammography in women with habitual risk who are less than 50 years old, it is worth noting that, due to the higher breast density in this age group, there is a lower sensitivity to mammography23 and, consequently, a higher number of false-positive results, leading to the implementation of other interventions and, therefore, increased costs without proof of effectiveness in reducing mortality.22,23
A study conducted with data from the National Household Sample Survey (PNAD) of 200320 also showed less frequent realization of mammogram in the age group from 60 to 69 years old, compared to the age group from 50 to 59. A possible explanation for this finding, according to the authors, would be the cohort effect on the spread of examination, which would be increasing in younger cohorts.20 Another study observed reduction in the ratio of adherence to the screening mammography with the follow-up time extension, representing a lack of vigilance on the next steps and the absence of convocation of women, typical characteristics of the opportunistic screening.24
According to the Ordinance of SISMAMA (SAS/MS No. 779, of December 31st, 2008), the production of procedures related to bilateral mammography and biopsy must be notified by this system. Nevertheless, the comparison of data from SISMAMA with the production of registered examinations in SIA/SUS indicates underreporting in the first. Besides, an evaluation of the system right after its deployment noted that it was underutilized by technicians, doctors and other professionals involved: not everyone knew its operation and gave due weight to its fill with the greatest possible accuracy of data, which doesn’t seem to have changed over the past few years.25 As SISMAMA's main objective is to manage the control of breast cancer, the insertion of inaccurate data record represents an obstacle to be overcome by public managers as a strategy for health planning.17 Training the professionals involved is, therefore, of most importance so that the data transferred to the Ministry of Health reflect the reality, reducing underreporting, wrong notifications and consequent inappropriate allocation of financial resources.25
BI-RADS category for diagnostic mammographies presented distinct proportional distribution in Minas Gerais state, with BI-RADS 3 percentage higher when compared to other studies.14,23 According to Vieira and Toigo,26 the variability in dependent interpreter and the diversity and difficulty in characterization of incipient lesions lead to variability in BI-RADS categorizing among services, especially in class 3. In this perspective, a study that evaluated the performance of diagnostic centers concerning mammographic exam reports conducted by the SUS in the municipality of Goiânia-GO concluded that the performance of diagnostic centres is unequal in regard to the classification of SISMAMA reports, reinforcing the need for training of professionals responsible for examination reports.17
It is expected that the time for completion and release of the report of diagnostic mammographies is less than the one dedicated to mammography screening.23 Therefore, 90% of diagnostic mammographies should have the result released by up to 30 days.18 This study revealed that the majority of mammograms in Minas Gerais state, regardless of clinical indication, was carried out and their results were available up to 30 days, although there was a prioritization of symptomatic women.
In Minas Gerais state, the ratio of biopsies and mammograms that are classified as BI-RADS 4 or 5 was only 0.31 in 2010; in 2011, despite the observed increase (0.42), the indicator still was unfavorable - before an expected ratio close to 1.0 -, suggesting a low degree of adequacy of diagnostic confirmation for suspicious findings of malignancy. These results are compatible with the low ratio (0.36) observed in Brazil in 2010.14 We emphasize the big difference that this indicator presents among the macroregions of Minas Gerais state, this variance is also observed among the major regions of Brazil.14,23 This finding points out the need for assessing the loss and/or sending of information, and the quality of data.23 In addition to this possibility, another interpretation for the low ratio observed would be the referral to surgery - without biopsy done in the SUS -, held by direct payment or by private health plans that cover this type of procedure. These results suggest that the health system is not yet ready to meet the demand for diagnostic confirmation.14 It is worth noting that a screening program should not offer only quality tests to population, but also access to the diagnostic procedures of suspicious lesions and early referral to quality treatment for confirmed cases.4
Compared to mammography screening, recent studies indicate that the benefit provided by the reduction of mortality is accompanied by significant damage in women tracked, being the overdiagnosis the leading cause.27,28 According to a meta-analysis study published in 2013,27 considering a 15% reduction in mortality, screening is associated with an overdiagnosis rate and excessive treatment of 30% approximately. That is: for every 2,000 women participants of a screening program during a time lapse of 10 years, a death by breast cancer is prevented, while ten healthy women are overdiagnosed and treated unnecessarily.
The limitations of this study are mainly related to the quality of the data used. This data were originated in the information systems that chiefly present underreporting and faults still existing in the SISMAMA. Nevertheless, the data of this system allowed the construction of core indicators to evaluate the actions of the breast cancer screening in Minas Gerais state, and may subsidize the planning of control activities. With the implementation of the SISCAN (Cancer Information System), which replaces and integrates the SISMAMA and the SISCOLO (Cervical Cancer Information System), some limitations of these systems will be overcome and will allow longitudinal screening of users, because the registry will have as observation unit the woman and not the exam.29
The results demonstrate the need of enhancing the program of breast cancer screening among the target population, ensuring access to the diagnostic procedures of suspicious lesions and early treatment of confirmed cases.
REFERENCES
1. Ministério da Saúde (BR). Instituto Nacional de Câncer José Alencar Gomes da Silva. Diretrizes para a detecção precoce do câncer de mama no Brasil. Rio de Janeiro: Instituto Nacional de Câncer José Alencar Gomes da Silva; 2015. [ Links ]
2. Ministério da Saúde (BR). Instituto Nacional de Câncer José Alencar Gomes da Silva. Atlas da mortalidade [Internet]. Rio de Janeiro: Instituto Nacional de Câncer José Alencar Gomes da Silva; 2014[citado 2016 dez 23]. Disponível em: Disponível em: http://mortalidade.inca.gov.br/Mortalidade/ [ Links ]
3. World Health Organization. WHO position paper on mammography screening. Geneva: World Health Organization; 2014. [ Links ]
4. Silva RCF. Mamografia e rastreamento mamográfico: o debate da detecção precoce do câncer de mama contextualizado para a realidade brasileira. In: Teixeira L. Câncer de mama, câncer de colo de útero: conhecimentos, políticas e práticas. Rio de Janeiro: Outras Letras; 2015. p.165-209. [ Links ]
5. Marmot MG, Altman DG, Cameron DA, Dewar JA, Thompson SG, Wilcox M, et al. The benefits and harms of breast cancer screening: an independent review: a report jointly commissioned by Cancer Research UK and the Department of Health (England) October, 2012. Br J Cancer. 2013 Jun;108(11):2205-40. [ Links ]
6. Girianelli VR, Gamarra CJ, Azevedo e Silva G. Os grandes contrastes na mortalidade por câncer do colo uterino e de mama no Brasil. Rev Saude Publica. 2014 jun;48(3):459-67. [ Links ]
7. Oeffinger KC, Fontham ET, Etzioni R, Herzig A, Michaelson JS, Shih YC, et al. Breast cancer screening for women at average risk: 2015 guideline update from the American Cancer Society. JAMA. 2015 Oct;314(15):1599-614. [ Links ]
8. Azevedo e Silva G, Zeferino LC, Thuler LCS, Bustamante-Teixeira MT, Guerra MR. A situação dos cânceres do colo do útero e da mama no Brasil. In: Teixeira L. Câncer de mama, câncer de colo de útero: conhecimentos, políticas e práticas. Rio de Janeiro: Outras Letras; 2015. p. 41-73. [ Links ]
9. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Rastreamento. Brasília: Ministério da Saúde; 2010. (Série A. Normas e manuais técnicos); (Cadernos de atenção primária; vol. 29) [ Links ]
10. Ministério da Saúde (BR). Instituto Nacional de Câncer José Alencar Gomes da Silva. SISMAMA: informação para o avanço das ações de controle do câncer de mama no Brasil [Internet]. Instituto Nacional de Câncer José Alencar Gomes da Silva; 2010 [citado 2016 dez 23]. Disponível em: Disponível em: http://dms.ufpel.edu.br/ares/bitstream/handle/123456789/228/5%20%20%202010%20Sismama%20relat%C3%B3rio%20e%20dados.pdf?sequence=1 [ Links ]
11. Brasil. Ministério da Saúde. Portaria nº 779, de 31 de dezembro de 2008. Define o Sistema de Informação do Controle do Câncer de Mama (SISMAMA), altera a tabela de procedimentos, medicamentos e órteses, próteses e materiais especiais - OPM do SUS. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2008 dez 31; Seção 1:145 [ Links ]
12. Ministério da Saúde (BR). Secretaria-Executiva. Departamento de Apoio à Gestão Descentralizada. Instrutivo da pactuação de prioridades, objetivos, metas e indicadores de monitoramento do pacto pela vida e de gestão para o biênio 2010-2011: conforme Portaria nº 2669 GM/MS de 03 de novembro de 2009. Brasília: Ministério da Saúde; 2009. [ Links ]
13. Ministério da Saúde (BR). Instituto Nacional de Câncer José Alencar Gomes da Silva. Informativo detecção precoce: monitoramento das ações de controle dos cânceres do colo do útero e de mama. Bol. 2012 jan- mar;3(1):1-7. [ Links ]
14. Azevedo e Silva G, Bustamante-Teixeira MT, Aquino EML, Tomazelli JG, Silva IS. Acesso à detecção precoce do câncer de mama no Sistema Único de Saúde: uma análise a partir dos dados do Sistema de Informações em Saúde. Cad Saude Publica. 2014 jul;30(7):1537-50. [ Links ]
15. Domingues EP, Magalhães AS, Faria WR. Infraestrutura, crescimento e desigualdade regional: uma projeção dos impactos dos investimentos do Programa de Aceleração do Crescimento (PAC) em Minas Gerais. PPE. 2009 abr;39(1):121-58. [ Links ]
16. Duarte DAP. Iniquidade social e câncer em mulheres: análise da mortalidade por câncer de mama e colo do útero nas microrregiões de saúde de Minas Gerais no período de 2008-2012 [ dissertação]. Juiz de Fora (MG): Universidade Federal de Juiz de Fora; 2016. [ Links ]
17. Rodrigues DCN, Freitas-Junior R, Corrêa RS, Peixoto JE, Tomazelli JG, Rahal RMS. Avaliação do desempenho dos centros de diagnóstico na classificação dos laudos mamográficos em rastreamento oportunista do Sistema Único de Saúde (SUS). Radiol Bras. 2013 mai-jun;46(3):149-55. [ Links ]
18. Passman LJ, Farias AMRO, Tomazelli JG, Abreu DMF, Dias MBK, Assis M, et al. SISMAMA: implementation of an information system for breast cancer early detection programs in Brazil. Breast. 2011 Apr;20 Suppl2:S35-9. [ Links ]
19. Ministério da Saúde (BR). Instituto Nacional de Câncer José Alencar Gomes da Silva. Coordenação Geral de Prevenção e Vigilância. Divisão de Detecção Precoce e Apoio à Organização de Rede. Ficha técnica de indicadores relativos às ações de controle do câncer de mama. Rio de Janeiro: Instituto Nacional de Câncer José Alencar Gomes da Silva; 2014. [ Links ]
20. Lima-Costa MF, Matos DL. Prevalência e fatores associados à realização da mamografia na faixa etária de 50-69 anos: um estudo baseado na Pesquisa Nacional por Amostra de Domicílios (2003). Cad Saude Publica. 2007 jul;23(7):1665-73. [ Links ]
21. Urban LABD, Schaefer MB, Duarte DL, Santos RP, Maranhão NMA, Kefalas AL, et al. Recomendações do Colégio Brasileiro de Radiologia e Diagnóstico por Imagem, da Sociedade Brasileira de Mastologia e da Federação Brasileira das Associações de Ginecologia e Obstetrícia para rastreamento do câncer de mama por métodos de imagem. Radiol Bras. 2012 out-dez;45(6):334-9. [ Links ]
22. Silva FX, Katz L, Souza ASR, Amorim MMR. Mamografia em mulheres assintomática na faixa etária de 40 a 49 anos. Rev Saude Publica. 2014 dez;48(6):931-9. [ Links ]
23. Ministério da Saúde (BR). Instituto Nacional de Câncer José Alencar Gomes da Silva. Informativo detecção precoce: monitoramento das ações de controle dos cânceres do colo do útero e de mama. Bol. 2012 ago-dez;3(3):1-9. [ Links ]
24. Marchi AA, Gurgel MSC. Adesão ao rastreamento mamográfico oportunistíco em serviços de saúde públicos e privados. Rev Bras Ginecol Obstet. 2010 abr;32(4):191-7. [ Links ]
25. Santos SBL, Koch HA. Análise do Sistema de Informação do Programa de controle do Câncer de Mama (SISMAMA) mediante avaliação de 1.000 exames nas cidades de Barra Mansa e Volta Redonda. Radiol Bras. 2010 set-out;43(5):295-301. [ Links ]
26. Vieira AV, Toigo FT. Classificação BI-RADS: categorização de 4.968 mamografias. Radiol Bras. 2002 jul-ago;35(4):205-8. [ Links ]
27. Olsen O, Gotzsche PC. Screening for breast cancer with mammography. Cochrane Database Syst Rev. 2001;4:CD001877. [ Links ]
28. Tesser CD, D’Ávila TLC. Por que reconsiderar a indicação do rastreamento do câncer de mama? Cad Saude Pública. 2016 maio;32(5):e00095914. [ Links ]
29. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Instituto Nacional de Câncer José Alencar Gomes da Silva. Sistema de informação do câncer: manual preliminar para apoio à implantação. Rio de Janeiro: Instituto Nacional de Câncer José Alencar Gomes da Silva; 2013. [ Links ]
Received: September 05, 2016; Accepted: December 04, 2016
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
