










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde vol.26 no.4 Brasília dez. 2017
http://dx.doi.org/10.5123/s1679-49742017000400006
ORIGINAL ARTICLE
Factors associated with homicide in Manaus, Amazonas, Brazil, 2014
1Fundação Oswaldo Cruz, Instituto Leônidas e Maria Deane, Manaus-AM, Brasil
2Fundação Oswaldo Cruz, Escola Nacional de Saúde Pública Sergio Arouca, Rio de Janeiro-RJ, Brasil
3Universidade Federal do Amazonas, Escola de Enfermagem de Manaus, Manaus-AM, Brasil
4Universidade Federal de Pelotas, Faculdade de Medicina, Pelotas-RS, Brasil
OBJECTIVE:
to identify characteristics, magnitude and factors associated with homicide in Manaus-AM, Brazil.
METHODS:
cross-sectional study, with data from the Mortality Information System (SIM); homicide rates and odds ratio (OR) were estimated, comparing to other external causes, for 2014; logistic regression was used.
RESULTS:
of the 1,657 violent deaths, 913 were due to homicide; homicide rate was of 55.8/100 thousand inhabitants (95%CI 52.1;59.7); odds ratio was higher among males (OR 3.4; 95%CI 2.3;5.1) when compared with females; among single (OR 1.6; 95%CI 1.1;2.5) and widowed individuals (OR 4.1; 95%CI 1.1;15.6), when compared with married individuals; at night/early hours (OR 2.1; 95%CI 1.6;2.9) and in the afternoon (OR 1.7; 95%CI 1.2;2.4), when compared with the morning period; the probability was higher among individuals under 35 years, with less schooling.
CONCLUSION:
homicide mortality in Manaus was high, especially among males and young individuals with less schooling.
Keywords: Homicide; Violence; Odds Ratio; Cross-Sectional Studies
Introduction
Homicide represents the utter violence in a society and reflects serious economic, social, political, and, often, religious problems.1 Homicide is a complex, multifactorial, and heterogeneous phenomenon, and it not only impacts on the populations' quality of life, but also on their life expectancy.2-4 Estimates from the United Nations Office on Drugs and Crime (UNODC) suggest that in 2012 nearly half a million people were victims of homicide worldwide.5 From this amount, 36% of occurrences were in the Americas and only 5% in Europe.
In Brazil, homicide remains as the cause of death that has more impact on violence statistics. In 2007, mortality rate due to homicide was of 26.8/100 thousand inhabitants, with important regional contrasts.2 Although a significant decrease in the national homicide rate has been recorded as of 2004, comparing to the period from 1999 to 2003, a change was observed in its regional pattern. On the one hand, in the Southeast region of the country, which is more developed economically, there was a reduction of about 45.0% in those rates. On the other hand, in the North and Northeast regions, economically less developed, there were increases close to 50.0% and 65.0%,2 respectively, although both regions have also benefited from important progress in the economic and social area since the 2000s.4,6
The few available studies on homicidal violence are usually restricted to the Southeast and Northeast regions, and they explore time and spatial dimensions of homicide. Regarding Manaus, for instance, no studies on mortality due to homicide have been found in the indexed literature. Because of this, understanding the magnitude and the main factors associated with homicide is not only useful for the identification of its determinants, but also for proper planning, implementation and assessment of prevention actions/programs regarding homicidal violence, having as example the current Brazilian legislation that regulates gun license.
This study aimed to identify characteristics, magnitude and factors associated with homicide in Manaus, Amazonas, in 2014, and to compare data on mortality due to homicide in Manaus with those from other capitals of the country.
Methods
This is a cross-sectional study with data on mortality taken from the digital records of the Brazilian Mortality Information System (SIM), provided by the Amazonas State Health Department (Susam).
The metropolitan area of Manaus, capital of Amazonas State, is the most important area economically in the Amazon region.7 In 2014, it had 1,990,149 inhabitants and concentrated more than half of the state's population.6 Although the gross domestic product of Manaus was among the largest of Brazilian municipalities in 2010, its Gini index, which reflects social inequalities, was the sixth worst among the Brazilian state capitals: 0.63.6
We analyzed all data on death due to external causes occurred in Manaus in 2014. They refer to the chapter XX from the International Statistical Classification of Diseases and Related Health Problems - Tenth Revision (ICD-10).8
All deaths with underlying cause using codes X85 to Y09 of the ICD-10 were counted as homicides, among individuals at the age of 15 or over. Violent deaths among individuals under the age of 15 were excluded from the analysis, given its low relative importance regarding the "homicide" outcome, usually fewer than 4%.
Other external causes of death with underlying causes under the codes V01 to X59 (Accidents), X60 to X84 (Intentional self-harm), Y35 to Y36 (Legal interventions and operations of war), V01 to X59 (Complications of medical and surgical care), Y85 to Y89 (Sequelae of external causes of morbidity and mortality), Y90 to Y98 (Supplementary factors related to causes of morbidity and mortality classified elsewhere) and Y10 to Y34 (Events of undetermined intent), were considered as comparison groups.
Although part of the ‘Events of undetermined intent’ may represent misclassified homicides, we decided to maintain it in the comparison group because of its low proportion - less than 1% - concerning other external causes of death.
Furthermore, for the year 2014, relative frequencies of homicides, in which the underlying cause of death used the code X99 (Assault by sharp object), have been calculated for Brazil and for the municipalities of Fortaleza, Florianópolis, Rio de Janeiro, and São Paulo, aiming to compare these numbers with those of Manaus.
In this study, we assessed the association of the following variables with the occurrence of homicide: age (in years); sex (male; female); ethnicity/skin color (white; black + brown); marital status (married; single; divorced; widowed; other); education level (years of schooling: 0 to 3; 4 to 7; 8 to 11; 12 and over); place of occurrence (hospital + other health facilities; public areas; household; other); and time of occurrence (morning [from 06:00 a.m. to 11:59 a.m.]; afternoon [from 12:00 p.m. to 05:59 p.m.]; and night/early hours [from 06:00 p.m. to 05:59 a.m.]).
Due to the low relative importance regarding the ‘homicide’ outcome, the categories of ethnicity/skin color Asian (0.1%), and indigenous (0.1%) were not included in the regression analysis. The categories of ethnicity/skin color black (0.7%) and brown (92.8%) were gathered.
For comparative purposes, we calculated triennial average standardized homicide mortality rates (SHMR) for the municipalities of Manaus, Fortaleza, Florianópolis, Rio de Janeiro, and São Paulo, and for Brazil, by dividing the frequencies of deaths in the population ≥15 years old, extracted from SIM, by the size of the population of the same age group in the 2012-2014 triennium. The population estimates that composed the denominator of rates were obtained through annual geometric interpolation, based on data from the 2000 and 2010 Demographic Censuses, provided by SUS IT Department (DATASUS).6 The same strategy was used to estimate the SHMR of Manaus for the year 2014. The rates were standardized by age, using the direct standardization method. The world population, of the World Health Organization (WHO), was used as standard.9 Confidence intervals of the rates were estimated at 95% (95%CI).
Unconditional logistic regression analysis was used to estimate the odds ratios (OR) of death among homicide victims and the set of deaths concerning other violent causes. This procedure allows the comparison of death odds between the cause of interest, represented by the causes of homicide, and other causes, represented by other causes of violent death.10
The Pearson's chi-squared test was used to assess differences among proportions. The logistic regression analysis was performed in two stages. First, the effect of each covariate was assessed separately through crude analysis, regarding the outcome, by selecting only the covariates that presented missing data below 15.0% of the observations and p<0.2. Then, multivariate logistic models were tested. The selection of the covariates was done manually with a sequential introduction of the covariates, following a decreasing order of the p values obtained in the previous stage. The corrected Akaike information criterion (AICc) was used to assist in the selection of the most appropriate model, so that the AICc of a model was compared with the AICc of the next model, thus, opting for the model with the lowest AICc value until the final model was chosen.
The inclusion of possible interactions was tested (education level versus ethnicity/skin color; education level versus quadratic function for age; marital status versus quadratic function for age; education level versus marital status), as well as the quadratic function (age) in the model, through odds-ratio test, in order to minimize bias or distortion in the interpretation of results. The confidence intervals for the OR of the final model were estimated at 95% (95%CI). Effect display graphics were built11 with 95% confidence intervals, so these effects could be seen, adjusting for the variables included in the final model. The data were analyzed using the R statistical software, version 3.1.112 (The R Project for Statistical Computing).
Although this study has been carried out exclusively with secondary data without identifying the subjects, its protocol was submitted to the Research Ethics Committee of the National Research Institute of Amazon (CEP/Inpa), and approved on January 27th, 2016, Report No. 1,422,840.
Results
In 2014, 1,657 deaths due to external causes were recorded in Manaus, from which 913 individuals (55%) died from homicide. The standardized homicide mortality rate (SHMR) was of 55.8/100 thousand inhabitants (95%CI 52.1; 59.7) (data not presented in the table). In the 2012-2014 triennium, the SHMR in Manaus was of 60.3/100 thousand (95%CI 59.8; 64.0), the tenth highest among the 27 state capitals of the country. In the same period, the highest SHMR among the assessed capitals of the country (Table 1) was from Fortaleza (110.3/100 thousand inhabitants; 95%CI 107.7; 113.0). Florianópolis presented the lowest SHMR (19.3/100 thousand inhabitants; 95%CI 16.6; 22.4). The municipality of Rio de Janeiro presented SHMR of 36.0/100 thousand inhabitants (95%CI 34.3; 37.7), the municipality of São Paulo, 25.4/100 thousand inhabitants (95%CI 24.4; 26.5), and Brazil, 42.6/100 thousand (95%CI 42.3; 42.9).
Table 1 - Standardized homicide mortality rate (SHMR) in selected Brazilian state capitals and Brazil, 2012-2014
| Selected state capitals and Brazil | SHMR/100 thousand inhabitants | 95%CI a |
|---|---|---|
| Fortaleza b | 110.3 | 107.7;113.0 |
| Manaus c | 60.3 | 59.8;64.0 |
| Rio de Janeiro | 36.0 | 34.3;37.7 |
| São Paulo | 25.4 | 24.4;26.5 |
| Florianópolis d | 19.3 | 16.6;22.4 |
| Brasil | 42.6 | 42.3;42.9 |
a) 95%CI: 95% confidence interval.
b) Capital with the highest SHMR in the triennium 2012-2014.
c) Capital with the tenth highest SHMR in the triennium 2012-2014.
d) Capital with the lowest SHMR in the triennium 2012-2014.
Most homicide victims were male (93.9%), aged 25-39 years old (43.7%), brown skinned (92.8%), single (92.3%) and with 4 to 7 years of schooling (51.5%). The deaths occurred mostly on public areas (46.0%), and during the night/early hours (67.4%) (Table 2). In almost 36% of death certificates concerning homicide there was no record of autopsy (Table 2).
Table 2 - Characteristics of fatal victims of homicide and other external causes in Manaus, Amazonas, 2014
| Victims characteristics | Homicides a | Other external causes b | ||
|---|---|---|---|---|
| N | % | N | % | |
| 913 | 55.0 | 744 | 45.0 | |
| Age group (in years) | ||||
| 15-24 | 351 | 38.9 | 236 | 31.7 |
| 25-39 | 394 | 43.7 | 237 | 31.8 |
| 40-59 | 130 | 14.4 | 165 | 22.2 |
| ≥60 | 26 | 2.9 | 106 | 14.2 |
| Sex | ||||
| Female | 56 | 6.1 | 140 | 18.8 |
| Male | 856 | 93.9 | 604 | 81.2 |
| Ethnicity/skin color | ||||
| White | 56 | 6.3 | 70 | 9.5 |
| Black | 6 | 0.7 | 9 | 1.2 |
| Asian | 1 | 0.1 | 3 | 0.4 |
| Brown | 825 | 92.8 | 659 | 88.9 |
| Indigenous | 1 | 0.1 | - | - |
| Marital status | ||||
| Married | 52 | 5.9 | 101 | 13.7 |
| Single | 816 | 92.3 | 605 | 82.2 |
| Divorced | 8 | 0.9 | 10 | 1.4 |
| Widowed | 5 | 0.6 | 11 | 1.5 |
| Other | 3 | 0.3 | 9 | 1.2 |
| Education level (years of schooling) | ||||
| 0-3 | 176 | 19.5 | 169 | 22.9 |
| 4-7 | 465 | 51.5 | 280 | 37.9 |
| 8-11 | 235 | 26.0 | 233 | 31.6 |
| ≥12 | 27 | 3.0 | 56 | 7.6 |
| Place of occurrence | ||||
| Hospital | 352 | 38.5 | 356 | 47.8 |
| Other health facilities | 41 | 4.5 | 41 | 5.6 |
| Household | 52 | 5.7 | 131 | 17.6 |
| Public place | 420 | 46.0 | 163 | 21.9 |
| Other | 48 | 5.3 | 53 | 7.1 |
| Time of occurrence | ||||
| Morning | 108 | 12.8 | 180 | 25.3 |
| Afternoon | 168 | 19.8 | 155 | 21.8 |
| Night/early hours | 570 | 67.4 | 377 | 52.9 |
| Weekdays of occurrence | ||||
| Monday | 119 | 13.0 | 104 | 14.0 |
| Tuesday | 100 | 10.9 | 82 | 11.0 |
| Wednesday | 123 | 13.5 | 93 | 12.5 |
| Thursday | 115 | 12.6 | 88 | 11.8 |
| Friday | 122 | 13.4 | 121 | 16.3 |
| Saturday | 153 | 16.8 | 121 | 16.3 |
| Sunday | 181 | 19.8 | 135 | 18.1 |
| Autopsy | ||||
| No | 328 | 35.9 | 316 | 42.5 |
| Yes | 585 | 64.1 | 428 | 57.5 |
a) Homicides: codes X85-Y09 of the International Statistical Classification of Diseases and Related Health Problems - Tenth Revision (ICD-10).
b) Other external causes: codes V01-X59, X60-X84, Y35-Y36, V01-X59, Y85-Y89, Y90-Y98 and Y10-Y34 of ICD-10.
The most common method used to commit homicide was firearm, appearing in 67.3% of cases for both sexes: 69.3% in males and 40% in females (p=0.01). Sharp objects were the second most used means, with (20.0%) for both sexes: 19.6% in males and 25.7% in females (p=0.51).
Among females, of the total number of deaths due to sharp objects, excluding the records in which the death was verified at health care facilities, 55.6% of them occurred at home, whilst among males this proportion was of 17.9%, significantly lower than that of females (p=0.03) (Table 3).
Table 3 - Distribution of the main types of weapons used to commit homicide, according to the place of occurrence and sex in Manaus, Amazonas, 2014
| Type of weapon used | Place of occurrence a | |||||||
|---|---|---|---|---|---|---|---|---|
| Public place | Household | Other | Total | |||||
| N | % | N | % | N | % | N | % | |
| Male | ||||||||
| Firearm | 296 | 88.1 | 16 | 4.8 | 24 | 7.1 | 336 | 69.3 |
| Sharp object | 71 | 74.7 | 17 | 17.9 | 7 | 7.4 | 95 | 19.6 |
| Other assaults | 22 | 73.3 | 4 | 13.4 | 4 | 13.3 | 30 | 6.2 |
| Non-specified | 16 | 66.7 | 3 | 12.5 | 5 | 20.8 | 24 | 4.9 |
| Female | ||||||||
| Firearm | 9 | 64.3 | 3 | 21.4 | 2 | 14.3 | 14 | 40.0 |
| Sharp object | 2 | 22.2 | 5 | 55.6 | 2 | 2.2 | 9 | 25.7 |
| Other assaults | 4 | 36.4 | 2 | 18.2 | 3 | 27.3 | 9 | 25.7 |
| Non-specified | - | - | 2 | 66.7 | 1 | 33.3 | 3 | 8.6 |
| Both sexes | ||||||||
| Firearm | 305 | 87.1 | 19 | 5.4 | 26 | 7.4 | 350 | 67.3 |
| Sharp object | 73 | 70.2 | 22 | 21.2 | 9 | 8.6 | 104 | 20.0 |
| Other assaults | 26 | 66.7 | 6 | 15.4 | 7 | 17.9 | 39 | 7.5 |
| Non-specified | 16 | 59.2 | 5 | 18.5 | 6 | 22.3 | 27 | 5.2 |
a) Public place, household, and other. Hospitals and other health facilities were excluded.
In Manaus, in 2014, 19.1% (174/913) of the total number of homicides were caused by assault with sharp object; in Fortaleza, 6.2% (138/2,222); in Florianópolis, 12.3% (8/65); in Rio de Janeiro, 5.8% (79/1,351); and in São Paulo, 15.2% (249/1.632) (data not presented in the table).
In the unadjusted analysis, all selected covariates presented a value of p<0.05 (Table 4) and were included in the final logistic model, whose adjustment was adequate and included the following covariates: age in years (quadratic function), marital status, sex, time of occurrence, education level, ethnicity/skin color, and place of occurrence, besides the interaction term (p=0.02) between the covariates ‘age’ in years and ‘education level’ in number of schooling years. According to the data presented in Table 4, single individuals were 60% (95%CI 1.1; 2.5) more likely to die from homicide than those who were married; and men had 240% (95%CI 2.3; 5.1) more chances to die from homicide than women. The odds of dying from homicide at night/early hours were 110% (95%CI 1.6; 2.9) higher than the odds of dying in the morning, and the individuals who died in public areas were 100% (95%CI 1.5; 2.6) more likely to die from homicide than those who died in hospitals or other health care facilities, when compared with those who died from other external causes.
Table 4 - Odds ratio (OR) of crude and adjusted mortality of the association with deaths from homicide regarding all other causes of violent deaths, according to the characteristics of the victims in Manaus, Amazonas, 2014
| Victims characteristics | OR a (95%CI) b | p value (LR-test) c | OR d ( 95%CI) b | p value (LR-test) c |
|---|---|---|---|---|
| Age 2 (in years) | 0.969 (0.976;0.988) | <0.001 | 0.999 (0.998;1.001) | <0.718 |
| Marital status | ||||
| Married | 1.0 | <0.001 | 1.0 | 0.029 |
| Single | 2.6 (1.8;3.7) | 1.6 (1.1;2.5) | ||
| Divorced | 1.6 (0.6;4.2) | 2.1 (0.7;6.5) | ||
| Widowed | 0.9 (0.3;2.7) | 4.1 (1.1;15.6) | ||
| Other | 0.6 (0.2;2.5) | 0.3 (0.1;1.5) | ||
| Sex | ||||
| Female | 1.0 | <0.001 | 1.0 | <0.001 |
| Male | 3.5 (2.6;4.9) | 3.4 (2.3;5.1) | ||
| Time of occurrence | ||||
| Morning | 1.0 | <0.001 | 1.0 | <0.001 |
| Afternoon | 1.8 (1.3;2.5) | 1.7 (1.2;2.4) | ||
| Night/early hours | 2.5 (1.9;3.3) | 2.1 (1.6;2.9) | ||
| Education level (years of schooling) | ||||
| ≥12 | 1.0 | <0.001 | 1.0 | <0.019 |
| 0-3 | 2.2 (1.3;3.6) | 3.8 (1.5;9.9) | ||
| 4-7 | 3.4 (2.1;5.6) | 2.3 (0.9;5.6) | ||
| 8-11 | 2.1 (1.3;3.4) | 1.3 (0.5;3.3) | ||
| Ethnicity/skin color | ||||
| White | 1.0 | 0.019 | 1.0 | 0.478 |
| Black + brown | 1.6 (1.1;2.2) | 0.9 (0.5;1.3) | ||
| Place of occurrence | ||||
| Hospitals and other health facilities | 1.0 | <0.001 | 1.0 | <0.001 |
| Public place | 2.6 (2.1;3.3) | 2.0 (1.5;2.6) | ||
| Household | 0.4 (0.3;0.6) | 0.3 (0.2;0.5) | ||
| Other | 0.9 (0.6;1.4) | 0.7 (0.4;1.2) | ||
| Age 2 (in years) versus Education level (years of schooling) | ||||
| Age versus 0-3 years of schooling | - | 0.99 (0.97;0.99) | 0.023 | |
| Age versus 4-7 years of schooling | 0.99 (0.93;1.01) | |||
| Age versus 8-11 years of schooling | - | 0.98 (0.94;1.02) | ||
a) Crude odds ratio.
b) 95%CI: 95% confidence interval.
c) Odds-ratio test.
d) Odds ratio according to the adjusted final model, including the quadratic function (covariate 'age', in years), the covariates 'marital status', 'sex', 'time of occurrence', 'education level' in number of years of schooling, ethnicity/skin color and place of death, as well as the interaction term between the covariate 'age' and 'education level'.
Note: Number of observations in the final model = 1,492.
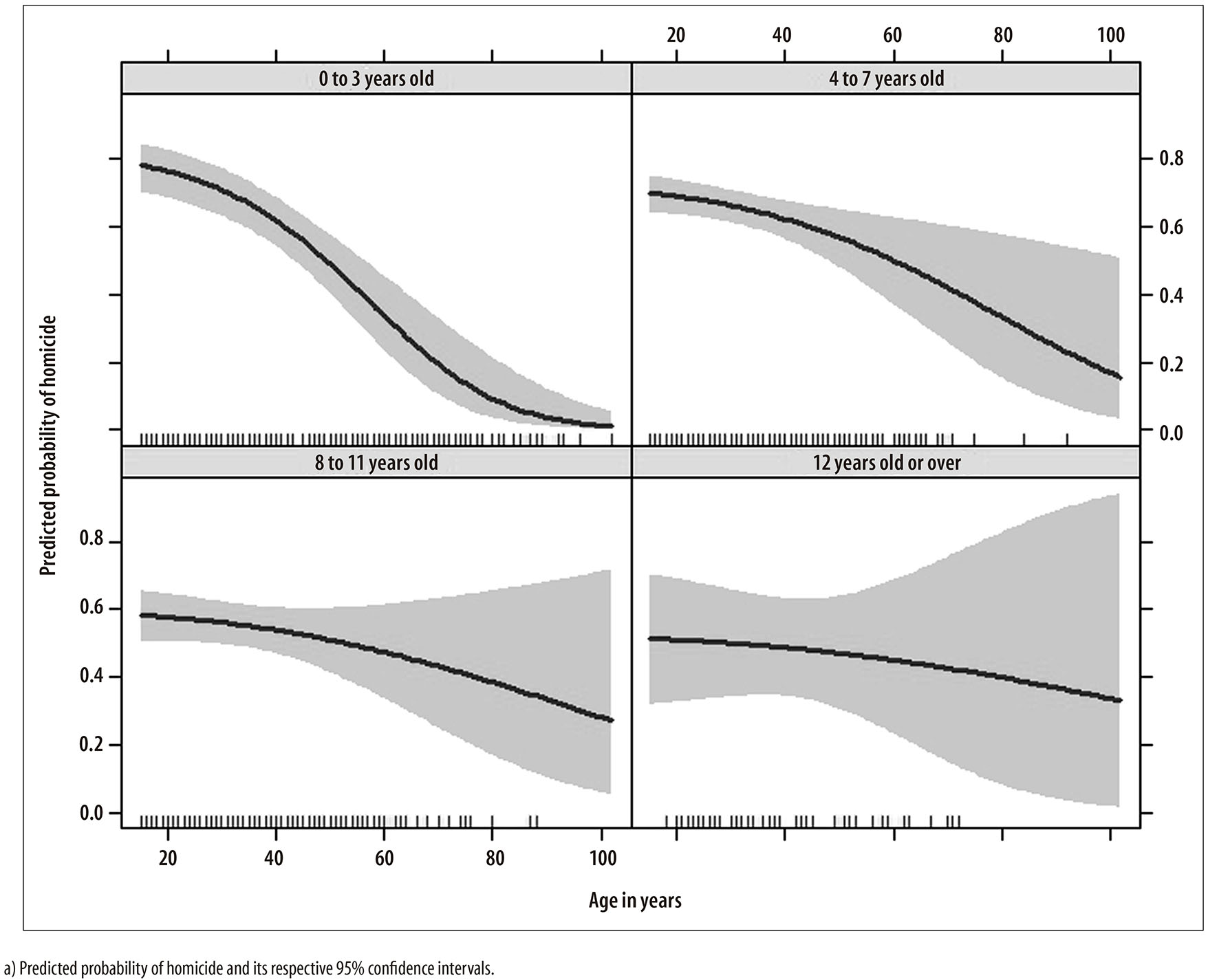
Due to the inclusion of the interaction term (age versus education level) in the regression model, we chose to demonstrate the effect of the covariates ‘age’ and ‘education level’ in the predicted probability of homicide, adjusted by the average effect of covariates from the final model. The modifying effect arising from the interaction between the covariates ‘age’ and ‘education level’ indicates that the predicted probability of homicide is not the same, once the education level of the victims varies, suggesting that low schooling or the lack of schooling is an important factor associated with deaths from homicide.
Figure 1 shows a peak of probability of homicide of about 79% at the age of 21 among the victims with low schooling; however, it can progressively decrease with the increase in the education level. On the other hand, individuals with high education level presented a predicted probability of dying from homicide at the age of 21 about 20% lower than those with low education level. Nevertheless, the predicted probability of dying from homicide seems not to differ so much until the age of 50, slightly dropping henceforth among the victims with high education level.
Discussion
The standardized homicide mortality rate (SHMR) in Manaus was high, as well as the proportion of homicides caused by sharp objects. We observed a greater odds of deaths from external causes concerning homicide, when compared with other external causes of deaths in males, in single individuals, and those with less than 12 years of schooling. The predicted probability of dying from homicide was higher in individuals with no schooling or with less than 3 years of schooling, consistently decreasing after the age of 35.
Males were 3.4 times more likely to die from homicide than females, following a common standard in some other regions of Brazil and the world.2-4 Gender inequalities of a patriarchal and sexist society such as the Brazilian one are said to contribute to worsen violence, affecting mostly males, sometimes as perpetrators, sometimes as victims.13
The afternoon and night periods (night + early hours) were also associated with deaths from external causes due to homicide. This was the time of the day which showed the highest magnitude. This was possibly related to drug trafficking and abusive use of alcohol and psychoactive drugs, especially those derived from cocaine such as crack, which is associated with high mortality rates among its users.14-17
Homicides occurred mostly in public areas. It is important to highlight that of the 67.3% of homicides in which the assault mean was firearm, nearly half of the victims died in public areas; that is, they died even before they could receive medical care, highlighting the lethality of firearms and their possible relation to illegal activities, especially with drug trafficking.
Socioeconomic inequality is widely acknowledged as having great influence on deaths from homicide and it may be expressed through different indicators, mostly composed, which represents contexts, not individuals.2,18,19 This study also highlighted the different pattern regarding the predicted probability of homicide among different education levels, in which a greater probability falls on young individuals and those with lower education level (social class proxy). Young individuals with lower education level usually have low qualification and are excluded from the job market due to their vulnerability. Thus, they often find attractive options in illegal activities, such as drug trafficking and interpersonal violence, to fulfill their need of consumption and leisure.4.20 Among the victims with higher education level, the predicted probability of homicide is quite low, basically steady until the age of 50, which means a possible indication that that group of victims is composed mostly of individuals whose motivations of death are different from the group of young victims. Therefore, more studies appear to be necessary in order to understand the relations of those deaths with robbery followed by death, for example.
The odds of homicide were higher among single individuals than married ones. Not by chance, 96.0% of homicide victims under the age of 40 were single, highlighting the importance regarding the individuals' marital status in the assessed setting. The fact that widowed individuals were more likely to be victims of homicide when comparing to married individuals should be interpreted with caution, since the interval estimate associated with this punctual measurement is inaccurate, probably influenced by the reduced frequency of widowed individuals in the sample.
The mode of age of homicides in Manaus was 21 years (56 cases), coinciding with the greatest probability regarding the outcome in our sample. Moreover, nearly 83.0% of all homicide victims were under the age of 40, which reinforces not only its earliness, but also its high magnitude. Other studies found that young individuals in a productive age constitute the main risk group for homicide.2-4,20 This is an important aspect for the demographic composition of the population and also compromises the future generations, in short and long terms, given the negative potential of those losses in workforce.20,21
The use of firearms as the main means of perpetrating homicides is similar to what was observed in other regions of the country and the world.2,4 It must be emphasized that even with the implementation of the Statute of Disarmament, since 2003, a mechanism that built barriers against the use and indiscriminate carrying of firearms in Brazil, the relative importance of these weapons to the practice of homicide in Manaus remains high, close to 70%.
On the other hand, the use of sharp objects in homicides reported in Manaus was higher than the observed in Brazil in the municipalities of São Paulo and Florianópolis. The percentage of homicides caused by sharp objects in Manaus was almost three times higher in 2014, when compared with capitals such as Rio de Janeiro and Fortaleza. Furthermore, the fact that 55.6% of the deaths caused by sharp object among females have occurred at home not only highlights its importance in the female group, but also suggests a link with domestic, family or sexual violence against women and, therefore, the need to qualify and organize the records on violence in order to provide proper visibility to femicide, especially in the Midwest, Northeast and North regions of the country, where its magnitude is worrisome.22 Likewise, the relevance of the sharp object is a fine but neglected distinction concerning homicidal violence in Manaus, and in most capitals of Amazon region, given the high frequency of deaths that happens outside the household.
Another relevant aspect was the high homicide frequency in Manaus, which reached nearly a thousand cases in just one year, almost twice the total of the homicides recorded in 2012 in the whole Chile, which has a population nine times bigger than Manaus.5 In the 2012-2014 triennium, considering the country's set of capitals, Manaus was responsible for the 10th highest SHMR. Fortaleza held the highest SHMR of all (110.3/100 thousand; 95%CI 107.7; 113.0) and Florianópolis held the lowest (19.3/100 thousand; 95%CI 16.6; 22.4). Manaus, besides having overcome the national average rate, (42.6/100 thousand; 95%CI 42.3; 42.9), showed a considerably higher SHMR (60.3/100 thousand; 95%CI 59.8; 60.4) than that of large urban centers in the same triennium, such as Rio de Janeiro (36.0/100 thousand; 95%CI 34.3; 37.7) and São Paulo (25.4/100 thousand; 95%CI 24.4;26.5). This change of pattern reinforces the thesis about a worrisome phenomenon of homicidal violence in Brazil: this kind of violence has been moving from the coast to the countryside, especially to the north of the Amazon region, where there has been a widespread growth over the last two decades.2,9,23
Although the autopsy is mandatory and important to properly classify the cause of death, there was no record of its performance in more than one-third of homicides that occurred in Manaus, in 2014. In 2006, the Ordinance No. 1,405 of the Brazilian Ministry of Health instituted the National Network Services of Death Investigation (SVO) and Clarification of Death Causes,24 which recommended the existence of at least one size III SVO in municipalities like Manaus. However, until July 2014, due to the lack of the aforementioned service, the Institute of Forensic Medicine (IFM) issued the death certificates (DC), both for undefined natural causes or with no medical care, and for violent causes. From then on, the IFM stopped issuing death certificates for undefined natural causes or with no medical care, and Manaus spent the rest of the year without the SVO implemented.
This is a relevant aspect that may have important repercussion not only in the quality of SIM, but also in its coverage concerning especially causes of death by violence. The deficit or lack of these services may be responsible not only for the high percentage (nearly 12%) of ill-defined causes of death in 2014, but also for a portion of the high percentage regarding homicide records with no autopsy in Manaus. This does not necessarily mean that those autopsies are no longer carried out, but that this procedure is not recorded in DC anymore. Therefore, the need of new and more efficient investments to qualify and expand the coverage of SIM in all the Amazon region of Brazil seems to be unquestionable.
Although the vital statistics related to violence and accidents are acknowledged as being more reliable than those deaths deemed as natural,25,26 and even considering that from 2000 to 2010, significant progresses were recorded in the coverage of SIM in the country,27 as highlighted by Jorge et al.,20 several challenges need to be overcome to achieve the ideal filling of DC;4,28 especially in Amazonas, which was among the ten states of Brazil with the highest underestimation of deaths from homicide in the period from 1996 to 2010.29
This means that the results of this study should be interpreted with caution, in particular, the frequency of homicides and the magnitude of their rates, which might be underestimated. A potential source of bias may be the fact that this study has considered the set of deaths classified under the codes Y10 to Y34 (events of undetermined intent) in the comparison group, since cases of homicides might have been misclassified, for instance, as 'Events of undetermined intent', because of the high work overload of Manaus IFM. However, given its low proportion, which is less than 1% comparing to the rest of the deaths from external causes, we believe that its impact did not affect significantly the estimates presented in this study. Moreover, the factors associated that were assessed did not take into account the influence of psychosocial, behavioral, and spatial factors, and of use of alcohol and other illicit drugs, for example.4,30
There is no doubt that the homicidal violence in Manaus is a significant social and public health issue, implying unequal risks of mortality among young, male, and low-schooling individuals. Furthermore, we reinforce the need for more studies on this topic to understand sociopolitical and gender determinants of homicide in the Amazon region of Brazil. We also recommend studies to measure the impact of sharp objects in mortality statistics and an update in the discussion about the current legislation in Brazil, regarding its license of use, as strategy to reduce the homicides and, therefore, to achieve improvements in the population's quality of life and longevity.
Acknowledgments
We thank to Health Surveillance Foundation of Amazonas State for allowing the access to electronic files on mortality.
REFERENCES
1. Wieviorka M. O novo paradigma da violência. Tempo Social. 1997 maio;9(1):5-41. [ Links ]
2. Reichenheim ME, Souza ER, Moraes CL, Jorge MHPM, Silva CMFP, Minayo MCS. Saúde no Brasil 5: violência e lesões no Brasil: efeitos, avanços alcançados e desafios futuros. Lancet. 2011 maio;6736(11):75-89. [ Links ]
3. González-Pérez GJ, Vega-López MG, Cabrera-Pivaral CE. Impacto de la violencia homicida en la esperanza de vida masculina de México. Rev Panam Salud Publica. 2012 nov;32(5):335-42. [ Links ]
4. Murray J, Cerqueira DR, Kahn T. Crime and violence in Brazil: Systematic review of time trends, prevalence rates and risk factors. Aggress Violent Behav. 2013 Sep;18(5):471-83. [ Links ]
5. United Nations Office on Drugs and Crime. Global study on homicide 2013: trends, contexts, data. Vienna: United Nations Office on Drugs and Crime; 2014. [ Links ]
6. Ministério da Saúde (BR). Departamento de Informática do SUS [Internet]. Brasília: Ministério da Saúde; 2016 [citado 2017 maio 31]. Disponível em: Disponível em: http://www.datasus.gov.br [ Links ]
7. Cruz SHR, Castro ER, Sá MER. Grandes projetos urbanos em metrópoles amazônicas: modernização e conflito. Novos Cadernos NAEA. 2011 dez;14(2):89-116. [ Links ]
8. Organização Mundial de Saúde. Classificação estatística internacional de doenças e problemas relacionados à saúde: décima revisão. São Paulo: EDUSP; 2000. [ Links ]
9. Ahmad OB, Bochi-Pinto C, Lopez AD, Murray CJL, Lozano R, Imone M. Age standardization of rates: a new WHO standard. Geneva: World Health Organization; 2001. [ Links ]
10. Miettinen OS, Wang JD. An alternative to the proportional mortality ratio. Am J Epidemiol. 1981 Jul;114(1):144-8. [ Links ]
11. Fox J. Effect displays in R for generalised linear models. J Stat Softw. 2003;8(15):1-9. [ Links ]
12. The R Foundation.The R Project for Statistical Computing [Internet]. Vienna: The R Foundation; 2017 [cited 2017 May 31]. Avaliable from: Avaliable from: http://www.R-project.org / [ Links ]
13. Souza ER. Masculinidade e violência no Brasil: contribuições para a reflexão no campo da saúde. Cien Saude Coletiva. 2005 jan-mar;10(1):59-70. [ Links ]
14. Darke S. The toxicology of homicide offenders and victims: a review. Drug Alcohol Rev. 2010 Mar;29(2):202-15. [ Links ]
15. Morris SD. Drug trafficking, corruption, and violence in Mexico: mapping the linkages. Trends Organ Crim. 2013 Jun;16(2):195-220. [ Links ]
16. World Health Organization. Preventing violence by reducing the availability and harmful use of alcohol. Geneva: World Health Organization; 2009. [ Links ]
17. Dias AC, Araújo MR, Dunn J, Sesso RC, Castro V, Laranjeira R. Mortality rate among crack/cocaine-dependent patients: a 12-year prospective cohort study conducted in Brazil. J Subst Abuse Treat. 2011 Oct;41(3):273-8. [ Links ]
18. Nadanovsky P, Cunha-Cruz J. The relative contribution of income inequality and imprisonment to the variation in homicide rates among Developed (OECD), South and Central American countries. Soc Sci Med. 2009 Nov;69(9):1343-50. [ Links ]
19. Roberts A, Willits D. Income inequality and homicide in the United States: consistency across different income inequality measures and disaggregated homicide types. Homicide Stud. 2015 Feb;19(1):28-57. [ Links ]
20. Neves ACM, Garcia LP. Mortalidade de jovens brasileiros: perfil e tendências no período 2000-2012. Epidemiol Serv Saude. 2015 out-dez;24(4):595-606. [ Links ]
21. Nascimento AGO, Rodrigues RN, Machado CJ, Fioravante EF. Mortalidade em Manaus: aplicação de técnica de ajuste para medir os anos de vida perdidos devido a mortes violentas entre 1980 e 2009. In: Anais do XVIII Encontro Nacional de Estudos Populacionais; 2012 nov 19-23; Água de Lindóia. Rio de Janeiro. Associação Brasileira de Estudos Populacionais; 2012. [ Links ]
22. Garcia LP, Freitas LRS, Silva GDM, Höfelmann DA. Estimativas corrigidas de feminicídios no Brasil, 2009 a 2011. Rev Panam Salud Publica. 2015; 37(4/5):251-7. [ Links ]
23. Andrade LT, Diniz AMA. A reorganização espacial dos homicídios no Brasil e a tese da interiorização. R Bras Est Pop. 2013;30 Suppl:171-91. [ Links ]
24. Brasil. Ministério da Saúde. Portaria nº 1.405, de 29 de junho de 2006. Institui a Rede Nacional de Serviços de Verificação de Óbito e Esclarecimento da Causa Mortis (SVO). Diário Oficial da República Federativa do Brasil, Brasília (DF), 2006 jun 30; Seção 1:243. [ Links ]
25. Jorge MHPM, Gotlieb SLD, Laurenti R. O sistema de informações sobre mortalidade: problemas e propostas para o seu enfrentamento II - mortes por causas externas. Rev bras epidemiol. 2002 ago;5(2):212-23. [ Links ]
26. França EB, Souza FM, Ishitani LH, Teixeira R, Szwarcwald CL. Strengthening vital statistics in Brazil: investigation of ill-defined causes of death and implications on mortality statistics. Lancet. 2013 Jun;381 (Suppl.2):51. [ Links ]
27. Szwarcwald CL, Frias PG, Souza Júnior PRB, Almeida WS, Morais Neto OL. Correction of vital statistics based on a proactive search of deaths and live births: evidence from a study of the North and Northeast regions of Brazil. Popul Health Metr. 2014 Jun;12:16. [ Links ]
28. Jesus T, Mota E. Fatores associados à subnotificação de causas violentas de óbito. Cad Saude Coletiva. 2010;18(3):361-70. [ Links ]
29. Cerqueira D. Mapa de homicídios ocultos no Brasil [Internet]. Brasília: Instituto de Pesquisa Econômica Aplicada; 2013 [citado 2017 maio 31]. (Textos para Discussão; 1848). Disponível em: Disponível em: http://www.ipea.gov.br/portal/images/stories/PDFs/TDs/td_1848.pdf [ Links ]
30. Briceño-Leon R., Villaveces A., Concha-Eastman A. Understanding the uneven distribution of the incidence of homicide in Latin America. Intern J Epidemiol. 2008 Aug;37(4):751-7. [ Links ]
Received: November 17, 2016; Accepted: May 05, 2017
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
