










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2337-9622
Epidemiol. Serv. Saúde vol.26 no.4 Brasília dez. 2017
http://dx.doi.org/10.5123/s1679-49742017000400019
Research note
Characteristics of suicide mortality among indigenous and non-indigenous people in Roraima, Brazil, 2009-2013*
1Instituto Leônidas e Maria Deane da Fundação Oswaldo Cruz, Laboratório de Estudos Interdisciplinares em Saúde Indígenas e Populações Vulneráveis, Manaus-AM, Brasil
OBJECTIVE:
to describe suicide characteristics and mortality rates among indigenous and non-indigenous people in Roraima, Brazil.
METHODS:
descriptive study using data from the Mortality Information System (SIM) about the suicides in individuals over 10 years old, recorded in the period from 2009 to 2013; suicide mortality rates were adjusted by sex and age.
RESULTS:
170 suicide cases were reported, being 17.1% among indigenous people; median ages were 24 years among indigenous and 29 among non-indigenous people; four municipalities concentrated 25/29 of the suicides among indigenous people; the 141 suicides among non-indigenous people were distributed in 13/15 municipalities in the state; suicide mortality rates were 15.0/100,000 among indigenous people and 8.6/100,000 among non-indigenous people.
CONCLUSION:
ethnic-racial peculiarities stood out in suicide mortality; among the indigenous people, rates were higher, younger ages prevailed and deaths were concentrated in a smaller number of municipalities, when compared to non-indigenous people.
Keywords: Suicide; Indigenous Population; Epidemiology, Descriptive
Introduction
In different countries, indigenous and native populations have higher suicide mortality rates than those of their general populations.1-4 In Brazil, there are few studies that investigate suicide in these groups of expressive diversity, although they represent only 0.4% of the national population.5
From 2006 to 2010, suicide mortality rate among indigenous people in the country was estimated at 12.6/100 thousand inhabitants, 2.3 times higher than the rate among non-indigenous people. The Brazilian states of Amazonas, Mato Grosso do Sul and Roraima explicitly reported indigenous over-mortality by suicide.6 There are comparative studies between indigenous and non-indigenous suicide mortality rates in the states of Amazonas and Mato Grosso do Sul.7,8 However, no studies were found in Roraima, the Brazilian state with the highest proportion of self-reported indigenous people. The objective of this study was to describe suicide characteristics and mortality rates among indigenous and non-indigenous people in Roraima State in order to increase knowledge about the ethnic-racial peculiarities of mortality due to this cause of death in Brazil.
Methods
This is a descriptive study which covered the period from 2009 to 2013.
Roraima, a state located in the Brazilian North region, had 450,479 inhabitants in 2010, of which 11.2% were self-reported indigenous, and about 63% of them lived in its capital, Boa Vista.5
Mortality data were obtained from the Mortality Information System (SIM) of the Ministry of Health.9 We selected all causes of death classified as ‘Intentional self-harm’ (codes X60 to X84 of the International Statistical Classification of Diseases and Related Health Problems - ICD-10),10 among Roraima residents aged over 10 years old, as recommended in the literature.4,11
The variables analyzed were:
- ethnicity/skin color (indigenous and non-indigenous people, including white, black, brown and Asian individuals in the latter);
- sex (male, female);
- marital status (single; married/cohabitation; widowed; divorced; unknown);
- age (in years: 10-14; 15-24; 25-39; 40-59; ≥60; and medians);
- place of death (hospital; household; public places; others; unknown);
- method of suicide (hanging; drowning; shot by firearm; poison; others); and
- municipality of residence.
Suicide mortality rates were calculated per 100,000 inhabitants. Data obtained from the 2000 and 2010 demographic censuses were used as denominators;12 the annual geometric progression was used to calculate the populations of the inter-census and post-census periods.
The rates were adjusted by age, using the direct method of standardization, taking the standard-population of the World Health Organization (WHO)13 as a reference.
The presentation of municipal suicide rates follows the categories used in a previous study:14 null; low (0.1 to 4.9/100,000); medium (5.0 to 14.9/100,000); high (15.0 to 29.9/100,000); and very high (over 30.0/100,000).
Thematic maps with municipal mortality rates among indigenous and non-indigenous people were developed using the QGIS 2.16 geoprocessing program.
Only secondary data of public domain were used, so this study did not need to be subject to ethical assessment, in accordance with the Resolution No. 510/201615 of the National Health Council (CNS).
Results
A total of 170 deaths were recorded as suicide: 29 (17.1%) among indigenous and 141 (82.9%) among non-indigenous people. In both groups, there was a predominance of deaths in single individuals and men. Most of these deaths occurred by hanging and in the household. Among indigenous people, no suicide was recorded in hospitals or public places, and there was no suicide by poison (Table 1).
Table 1 - Demographic and epidemiological characteristics of suicide records among indigenous and non-indigenous people, Roraima, 2009-2013
| Characteristics | Indigenous (N=29) | Non-indigenous (N=141) | Total (N=170) | |||
|---|---|---|---|---|---|---|
| n | n | % | n | % | ||
| Sex | ||||||
| Male | 19 | 107 | 75.9 | 126 | 74.1 | |
| Female | 10 | 34 | 24.1 | 44 | 25.9 | |
| Age group (in years) | ||||||
| 10-14 | 2 | 4 | 2.8 | 6 | 3.5 | |
| 15-24 | 13 | 46 | 32.6 | 59 | 34.7 | |
| 25-39 | 11 | 49 | 34.8 | 60 | 35.3 | |
| 40-59 | 3 | 30 | 21.3 | 33 | 19.4 | |
| ≥60 | - | 12 | 8.5 | 12 | 7.1 | |
| Marital status | ||||||
| Single | 21 | 104 | 73.8 | 125 | 73.5 | |
| Married/Cohabitation | 3 | 24 | 17.0 | 27 | 15.9 | |
| Widowed | - | 3 | 2.1 | 3 | 1.8 | |
| Divorced | - | 3 | 2.1 | 3 | 1.8 | |
| Unknown | 5 | 7 | 5.0 | 12 | 7.1 | |
| Place of death | ||||||
| Hospital | - | 8 | 5.7 | 8 | 4.7 | |
| Household | 21 | 103 | 73.0 | 124 | 72.9 | |
| Public place | - | 04 | 2.8 | 4 | 2.4 | |
| Others | 7 | 26 | 18.4 | 33 | 19.4 | |
| Unknown | 1 | - | - | 1 | 0.6 | |
| Suicide method | ||||||
| Hanging | 26 | 121 | 85.8 | 147 | 86.5 | |
| Drowning | - | 4 | 2.8 | 6 | 3.5 | |
| Shot by firearm | 1 | 5 | 3.5 | 6 | 3.5 | |
| Poison | - | 8 | 5.7 | 8 | 5.7 | |
| Others | - | 3 | 2.1 | 3 | 1.8 | |
The median age was 29 years among non-indigenous people and 24 years among indigenous people. In both groups, the minimum age was 12 years, whilst the maximum age was 80 years for non-indigenous people and 41 years for indigenous people.
In Roraima, the adjusted mortality rates by suicide were 15.0/100,000 indigenous and 8.6/100,000 non-indigenous people.
These rates were 20.3/100,000 males and 9.3/100,000 females among indigenous people; and 12.9 and 4.2/100,000, respectively, among non-indigenous people.
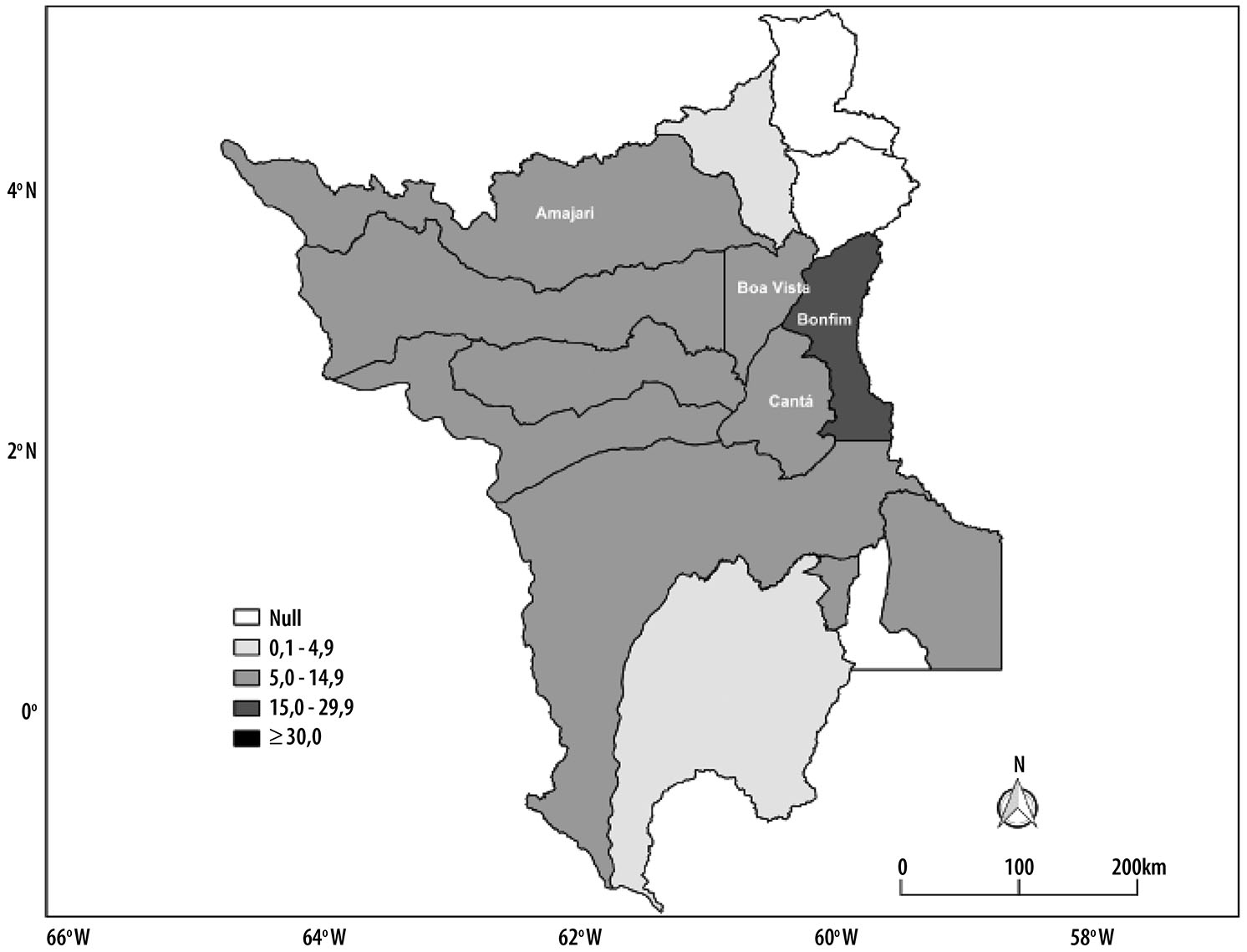
The rates among indigenous people were null in 8 of 15 municipalities, and high or very high in four: Cantá (84.2/100,000), Amajari (29.8/100,000), Bonfim (20.4/100,000) and Boa Vista (17.7/100,000). Out of the 29 cases of suicides among indigenous people, 25 happened in those four municipalities (Figure 1). Null suicide mortality rates among non-indigenous people were found in 3 of 15 municipalities. Boa Vista had 67.6% of non-indigenous suicides, corresponding to a rate of 7.4/100,000.
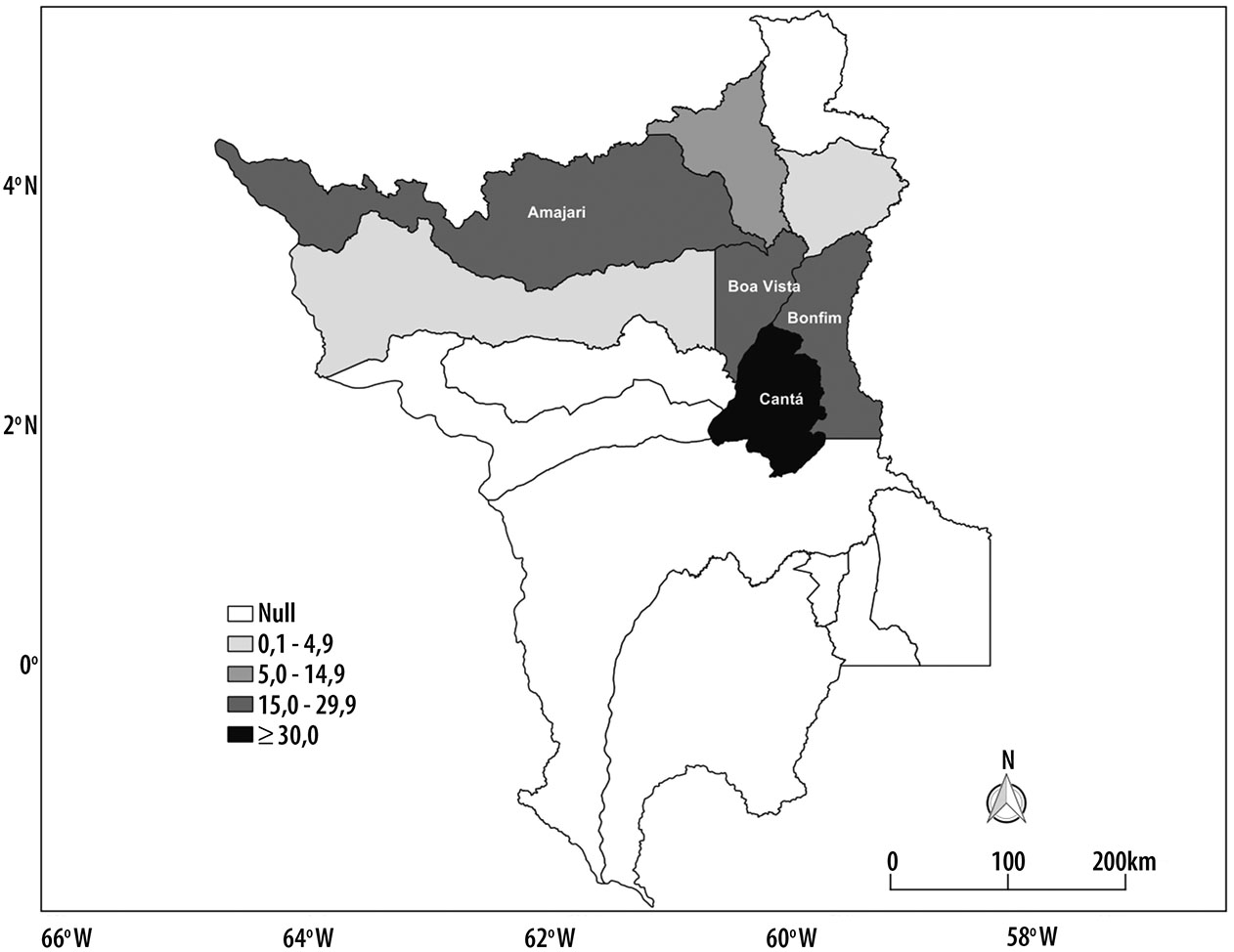
Figure 1 - Suicide mortality rates (per 100,000 inhabitants) among indigenous people, according to municipalities, Roraima, 2009-2013
In Bonfim, this rate was of 25/100,000 among non-indigenous people (Figure 2).
Discussion
Some ethnic-racial peculiarities on suicide mortality in Roraima stood out: younger age among indigenous people; no deaths recorded in hospitals or public places, nor by poison in the indigenous group; indigenous cases were concentrated in less than half of the municipalities; and the suicide mortality rate among indigenous people was 1.7 times higher than in non-indigenous people.
Some limitations of this study include those inherent to the use of secondary data of SIM. Missing data did not allow the analysis of important variables, such as education level and occupation. Despite some progress, SIM presents problems in the coverage of case records, especially in the North region of the country.16,17 Literature indicates that suicide deaths are usually underreported, especially among indigenous people.18 Thus, the mortality rates presented in this study may be even higher.
Despite these limitations, the comparison between the findings of this study and those researches carried out in the states of Amazonas7 and Mato Grosso do Sul8 may increase the knowledge on the ethnic-racial peculiarities of suicide mortality in Brazil. Such comparison can provide more information on the mortality situation due to suicide in this vulnerable group, as 80% of the suicides among indigenous people occurred in those states.11
In Roraima, as observed in Amazonas7 in 2006-2010 and in Mato Grosso do Sul8 in 2009-2011, the recorded suicides occurred mainly among men and single individuals; hanging was the main suicide method and most cases occurred in the household, both among indigenous and non-indigenous people. This profile, similar to the Brazilian general population in 2000-2012,18 does not show any ethnic-racial peculiarity of suicide mortality.
The indigenous people from Roraima died less in hospitals and were younger; this was also observed in Amazonas7 and Mato Grosso do Sul.8 In Roraima, there was no suicide recorded by poison, unlike the other two states.
The lower occurrence of deaths in hospitals among indigenous people, observed in these three states, may be associated with higher difficulty to access health services by this population, as well as - in certain cases - higher fatality of the methods used by them to commit suicide.8
In Roraima, there was no case of an indigenous person whose cause of death was suicide after the age of 45 years.
In the states of Amazonas7 and Mato Grosso do Sul,8 the highest mortality rates were found among youngsters from 15 to 24 years old. These data confirm international findings, which point to the fact that among indigenous people, youngsters and young adults suicides are numerically higher, when compared to other age groups.1
Suicide is heterogeneous, and is higher among indigenous people, as observed in Roraima. Suicide mortality rate among indigenous people was higher than in the Brazilian population in 2012 (6.4/100,000).19 The number of cases, however, is lower than what was observed among the indigenous populations of Amazonas7 and Mato Grosso do Sul,8 as well as what was found among native populations of the northwestern Russia (79.8/100,000)4 and the Kimberley region, in Australia (74/100,000);2 however, it is closer to what was observed among the Sami people from Norway (about 20/100,000).3 Differences in the quality of data records on death between the countries should be considered in this comparative analysis.
Another important aspect is that, although suicide mortality rates are higher in men, the indigenous/non-indigenous ratio rate is higher among women. This finding, previously highlighted in Amazonas7 and Mato Grosso do Sul,8 indicates higher relative participation of women in suicide mortality among indigenous; it characterizes a recurrent gender peculiarity in these ethnic groups, including in other countries.3,4
Another difference between the occurrence of suicide among indigenous and non-indigenous people is its distribution by municipalities.
In Roraima, as in Amazonas7 and in Mato Grosso do Sul,8 indigenous suicides are concentrated in certain municipalities, whilst those of non-indigenous people are spread. In Roraima, indigenous cases were concentrated in its capital, Boa Vista, and three neighboring municipalities, which presented high rates. Most indigenous suicides occurred in those municipalities.
This study design and the lack of specific literature on indigenous suicide in Roraima limit the capacity to elaborate an explanatory hypothesis for this finding.
We propose the development of more detailed studies, including ethnographic studies, capable of investigating the link between suicide and the process of urbanization of the state's indigenous population. Peculiarities were highlighted in the suicide mortality among the indigenous people of Roraima.
These peculiarities, which seem to extend to other Brazilian indigenous contexts, are related to the unique characteristics of the individuals who committed suicide, to higher rates, and to the existence of municipalities that concentrate a significant amount of cases. A deep understanding of these peculiarities requires additional studies so they can be taken into account in the development of specific policies to address this issue.
Acknowledgments
To Carlos Coimbra Jr., senior scholarship holder of Amazonas State Research Support Foundation - FAPEAM -, for the critical reading of this study.
To Fernanda R. Fonseca, for the development of thematic maps.
REFERENCES
1. World Health Organization. Preventing suicide: a global perspective [Internet]. Geneve: World Health Organization; 2014 [cited 2017 May 17]. 92 p. Available from: Available from: http://www.who.int/mental_health/suicide-prevention/world_report_2014/en/ [ Links ]
2. Campbell A, Balaratnasingam S, McHugh C, Janca A, Chapman M. Alarming increase of suicide in a remote Indigenous Australian population: an audit of data from 2005 to 2014. World Psychiatry. 2016 Out;15(3):296-7. [ Links ]
3. Silviken A. Prevalence of suicidal behavior among indigenous Sami in northern Norway. Int J Circumpolar Health. 2009 Jun;68(3):204-11. [ Links ]
4. Sumarokov YA, Brenn T, Kudryavtsev AV, Nilssen O. Suicides in the indigenous and non-indigenous populations in the Nenets Autonomous Okrug, Northwestern Russia, and associated socio-demographic characteristics. Int J Circumpolar Health. 2014 May 6;73:2430-8. [ Links ]
5. Instituto Brasileiro de Geografia e Estatística (IBGE). Os indígenas no censo demográfico 2010: primeiras considerações com base no quesito cor ou raça [Internet]. Rio de Janeiro: IBGE; 2012 [citado 2017 Maio 17]. 31 p. Disponível em: http://www.ibge.gov.br/indigenas/indigena_censo2010.pdf [ Links ]
6. Souza MLP, Orellana JDY. Suicide among the indigenous people in Brazil: a hidden public health issue. Rev Bras Psiquiatr. 2012 Dec; 34(4):489-90. [ Links ]
7. Souza MLP, Orellana JDY. Desigualdades na mortalidade por suicídio entre indígenas e não indígenas no estado do Amazonas, Brasil. J Bras Psiquiatr. 2013 Dez;62(4):245-52. [ Links ]
8. Orellana JDY, Balieiro AA, Fonseca FR, Basta PC, Souza MLP. Spatial-temporal trends and risk of suicide in Central Brazil: an ecological study contrasting indigenous and non-indigenous populations. Rev Bras Psiquiatr. 2016 Jan 19;38(3):222-30. [ Links ]
9. Informações de Saúde. Mortalidade. Óbitos por causas externas - Roraima [Internet]. Brasília: Ministério da Saúde. 2017 - [citado 2016 Jun 15]. Disponível em: Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sim/cnv/obt10sp.def [ Links ]
10. Organização Mundial da Saúde. Classificação estatística internacional de doenças e problemas relacionados à saúde (CID-10). 8. ed. 10. rev. São Paulo: Universidade de São Paulo; 2000. [ Links ]
11. Soole R, Kõlves K, De Leo D. Suicides in Aboriginal and Torres Strait Islander children: analysis of Queensland Suicide Register. Aust N Z P Public Health. 2014 Dec;38(6):574-8. [ Links ]
12. Instituto Brasileiro de Geografia e Estatística (IBGE). SIDRA. Sistema IBGE de recuperação automática. Censo demográfico 2000. [Internet]. Brasília: Instituto Brasileiro de Geografia e Estatística. 2012 - [citado 2016 Jun 15]. Disponível em: Disponível em: http://www2.sidra.ibge.gov.br/cd/cd2000cgp.asp?o=27&i=P [ Links ]
13. Ahmad OB, Bochi-Pinto C, Lopez AD, Murray CJL, Lozano R, Inoue M. Age standardization of rates: a new WHO standard [Internet]. Geneva: WHO; 2001 [cited 2017 May 17]. 14 p. Available from: Available from: http://www.who.int/healthinfo/paper31.pdf [ Links ]
14. Diekstra RF, Gulbinat W. The epidemiology of suicidal behaviour: a review of three continents. World Health Stat Q. 1993;46(1):52-68. [ Links ]
15. Ministério da Saúde (BR). Conselho Nacional de Saúde. Resolução nº 510, de 7 de abril de 2016. Diário Oficial da República Federativa do Brasil, Brasília, DF. 2016 Maio 24. Seção 1. p. 44-46. [ Links ]
16. Laurenti R, Mello Jorge MHP, Gotlieb SLD. Mortalidade segundo causas: considerações sobre a fidedignidade dos dados. Rev Panam Salud Publica. 2008 Maio;23:349-56. [ Links ]
17. Szwarcwald CL, Morais Neto OL, Frias PG, Souza Jr. PRB, Cortez Escalante JJ, Lima RB, Viola RC. Busca ativa de óbitos e nascimentos no Nordeste e na Amazônia Legal: estimação das coberturas do SIM e do Sinasc nos municípios brasileiros. In: Ministério da Saúde (BR). Departamento de Análise de Situação de Saúde. Secretaria de Vigilância em Saúde. Saúde Brasil, 2010: uma análise da situação de saúde e de evidências selecionadas de impacto de ações de vigilância em saúde [Internet]. Brasília: Ministério da Saúde; 2011 [citado 2017 Maio 17]. p. 79-98. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/saude_brasil_2010.pdf [ Links ]
18. De Leo D, Dudley MJ, Aebersold CJ, Mendoza JA, Barnes MA, Harrison JE, Ranson DL. Achieving standardized reporting of suicide in Australia: rational and program for change. Med J Aust. 2010 Apr;192(8):452-6. [ Links ]
19. Machado DB, Santos DN. Suicídio no Brasil, de 2000 a 2012. J Bras Psiquiatr. 2015 Mar;64(1):45-54. [ Links ]
Received: February 17, 2017; Accepted: April 28, 2017
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
