










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
Print version ISSN 1679-4974On-line version ISSN 2237-9622
Epidemiol. Serv. Saúde vol.27 no.2 Brasília June 2018 Epub June 26, 2018
http://dx.doi.org/10.5123/s1679-49742018000200014
ORIGINAL ARTICLE
Congenital syndrome associated with Zika virus infection among live births in Brazil: a description of the distribution of reported and confirmed cases in 2015-2016
1Ministério da Saúde, Secretaria de Vigilância em Saúde, Brasília, DF, Brasil
2Ministério da Saúde, Secretaria de Atenção à Saúde, Brasília, DF, Brasil
3Instituto de Pesquisa Econômica Aplicada, Diretoria de Estudos e Políticas Sociais, Brasília, DF, Brasil
Objective:
to describe the temporal and spatial distribution of reported and confirmed cases of congenital Zika virus syndrome (CZS) in live births in Brazil during 2015-2016.
Methods:
we conducted a descriptive study with data from the Public Health Events Registry, including cases born in 2015 or 2016, and registered between epidemiological week 45/2015 and 2/2017.
Results:
we analyzed 9.953 reported cases, of which 2.018 (20.3%) were confirmed and 2.819 (28.3%) were still under investigation at the epidemiological week 2/2017; 404 (4.1%) out of the 9.953 cases had laboratory confirmation for Zika virus; the prevalence of confirmed cases of CZS was 3.8/10 thousand livebirths in 2015 and 3.1/10 thousand live births in 2016.
Conclusion:
one fifth of the cases reported in 2015-16 were confirmed the CZS, reinforcing their relevance as a public health problem; efforts aimed at the diagnostic confirmation of the syndrome should be prioritized.
Keywords: Zika Virus Infection; Zika Virus; Microcephaly; Epidemics; Epidemiology, Descriptive
Introduction
The congenital Zika virus syndrome (CZS) comprises a set of signs and symptoms presented by children born to mothers infected by this virus during pregnancy.1 The microcephaly, defined as head circumference (HC) -2 standard definitions below the mean for age and sex according to the curves of reference is the manifestation more striking of this syndrome. The CZS can also include eye abnormalities, craniofacial disproportion and some articular deformities and members, even in the absence of microcephaly.2 Not yet fully known IS the spectrum and the consequences of the CZS to health and life expectancy of affected children, although it is remarkable the severity of cases, with evidence of harm to the child growth and development.3-5
The teratogenic potential of Zika virus was not described in the literature until the occurrence the epidemic in Brazil.6 On 22 October 2015, the State Health Department of Pernambuco reported and asked for support to the Secretariat of Health Surveillance (SVS), Brazilian Ministry of Health to perform the initial investigations of 26 cases of children with microcephaly. Initially, microcephaly was defined as HC less than 33cm for both sexes. As it is a rare event, in comparison with the with clinical and epidemiological profile of microcephaly in the state, it was considered as an event of great importance for the State Public Health.
On 11 November 2015, the Brazilian Ministry of Health declared Public Health Emergency of National Concern (PHENC) because of the alteration in the pattern of occurrence of microcephaly in Brazil (Decree no. 1.813/2015) and notified the fact to the Pan American Health Organization (PAHO)/World Health Organization (WHO).7,8
On 1st February 2016, WHO declared that the cluster of cases of microcephaly and other neurological disorders reported in Brazil after a similar situation observed in French Polynesia in 2014, constituted a Public Health Emergency of International Concern (PHEIC), in accordance with the International Health Regulations.9
The originality and the severity of the epidemiological situation on screen, together with the declaration of PHENC and PHEIC, motivated the articulation of a rapid response, in the national and international scenarios. As a result, the evidence produced by the national epidemiological surveillance, together with the results of epidemiological studies, clinical and laboratory data, made possible, in a short period of time, proving that Zika virus infection in pregnant women could cause microcephaly and other congenital malformations.10-12
The consensus on the implication of the Zika virus in the causality of the CZS was extremely relevant. However, this finding does not exclude the need for new investigations, neither the continuous work of the vigilance and health care on the detection and monitoring of cases. Notwithstanding the actions performed by the Brazilian Ministry of Health and Secretaries of State and Municipal for Health and other sectors of government and society, the epidemic of epidemic of Zika virus disease had spread to all Brazilian regions.13
The objective of this study was to describe the temporal and spatial distribution of notified and confirmed cases of SCZ of live births in Brasil, in 2015-2016.
Methods
This is a descriptive study with data from the Public Health Events Registry - Microcephaly (RESP-Microcephaly) - established by the Brazilian Ministry of Health on November 19th, 2015, in the context of the ESPIN.14 It is an electronic form prepared for notification of all cases and deaths suspected of alterations in growth and development in the growth and development related to infection by the Zika virus and other infectious etiologies. In addition to the notifications of births, suspected cases involving fetuses, abortions and stillbirths are also recorded in the RESP-Microcephaly. Although it was made available in November 2015, the RESP-Microcephaly allowed the registration of cases born earlier, from January 1st, 2015 and was based on the definitions in force at the time.
In this study, only the livebirths in the years 2015 and 2016, reported at RESP-Microcephaly, among epidemiological weeks 45/2015 and 2/2017 (11/08/2015 to 14/01/2017) were included. The data analyzed in this study were extracted on 18 January 2017, at 10:00 a.m. (GMT).
Between 2015 and 2016, different case definitions for notification were adopted along the epidemic:15
17 November 2015 to 12 December 2015: preterm newborn infants with HC less than or equal to percentile 3 in the curve of Fenton16 according to gestational age at birth and sex; full-term newborn or post-term with HC less than or equal to 33 cm for both sexes.
13 December 2015 to 12 March 2016: preterm newborn with HC less than or equal to percentile 3 in the Fenton curve16 according to gestational age at birth and sex; full-term newborn or post-term with HC less than or equal to 32 cm for both sexes.
13 March 2016 to 31 December 2016:17 preterm newborn with HC -2 standard deviations below the mean for gestational age at birth and sex according to the reference of the intergrowth;18 newborn at term or post-term with HC below -2 standard deviations for gestational age at birth and sex, according to the reference of the WHO.19
For confirmation of cases, epidemiological investigations were carried out under the responsibility of the surveillance teams of Secretaries of Health of States and Municipalities, based on the review of medical charts, interviews with those responsible for the child, clinical evaluation, imaging and laboratory, in compliance with the guidelines of the Ministry of Health.17 In the final classification, the results of imaging examinations and laboratory tests specific to the Zika virus were considered, as well as for syphilis, toxoplasmosis, rubella, cytomegalovirus and herpes virus (STORCH), described in the literature as infections that commonly cause congenital anomalies.20 The definitions adopted for confirmation of cases were:17
- Case confirmed by laboratory criteria for Zika: notified case presenting specific laboratory diagnosis and conclusive for Zika virus, identified in samples of newborns and/or of the mother.
- Case confirmed by laboratory criteria for STORCH: notified case presenting specific laboratory diagnosis and conclusive for syphilis, toxoplasmosis, rubella, cytomegalovirus or herpes simplex virus, identified in samples of newborns and/or of the mother.
- Case confirmed by imaging exam: notified case presenting alterations suggestive of congenital infection by any imaging method (ultrasound, computed tomography or magnetic resonance imaging), according to the protocol established by the Brazilian Ministry of Health, and1 without laboratory results.
In this study, we considered as confirmed cases of CZS only those with laboratory evidence for Zika and/or imaging exams suggestive of congenital infection by this virus, excluding the cases with laboratory confirmation for at least one of the STORCH. Cases without valid information on the date of birth were also excluded from the study.
The monthly time series of notified and confirmed cases in the period 2015-2016 were described for Brazil and its macroregions. Coefficients of prevalence were calculated (per 10 thousand live births) notified and confirmed cases in the country, macroregions and Federation Units (FU). We considered as the numerator the annual number of cases notified/confirmed recorded in the RESP-Microcephaly, and the denominator as the average number of births by region or FU in the period 2010-2014, based on data from the Information System on Live Births (Sinasc).21 We chose to use the average number of births in the denominator, considering that data were not available in Sinasc for the year of 2016.
The analyses were carried out using Stata version13.0 (StataCorp. 2013). The coefficients of prevalence of notified and confirmed cases were mapped separately, by FU, for 2015 and 2016, using the Quantum GIS software.
For conducting this study, was extracted from the RESP-Microcephaly a database without presentation variables that would allow the identification of individuals and their families. Only the first author had access to the database, being responsible for the analyses. The other authors consulted only consolidated results. The study was conducted in the context of the epidemiological surveillance actions developed by professionals from the Brazilian Ministry of Health and in the context of the of ESPIN; therefore, the project was not eligible for of registration and evaluation by the system of Ethics Research Committees of the National Committee for Ethics in Research (CEP/CONEP), as defined in the resolution of the National Health Council (CNS) No. 510, of 7 April 2016.
Results
10,200 suspected cases of CZS among live births in the period 2015-2016 were notified in the RESP-Microcephaly; of these cases, 138 (1.4% of the total) were laboratory confirmed for at least a STORCH. These cases were excluded from this analysis, as well as those who had no valid information for the date of birth (n=109; 1.1%; Figure 1).

a) STORCH: Syfilis, toxoplasmosis, rubella, cytomegalovirus, herpes simplex virus.
Figure 1 - Distribution of notified cases of congenital syndrome associated with Zika virus infection in live births, according to year of birth, final classification and criterion for confirmation. Brazil, 2015-2016
Of the total number of notifications included in the study (n=9,953), 2,819 (28.3%) remained under investigation until the epidemiological week 2/2017, most of them related to born in 2016 (72.1%; data not shown on table). Among the 2,018 confirmed cases born in 2015-2016, 404 (20.0%) had laboratory evidence for the Zika virus. Of the 4,749 reported cases born in 2015, 1,161 (24.4%) had laboratory confirmation for the Zika virus or had an imaging exam showing alterations suggestive of congenital infection, while the same proportion for the notifications of 2016 was 16.5% (857/5.204).
The coefficient of prevalence of CZS, considering only those confirmed cases, was 3.8 per 10 thousand live births in 2015 and 3.1 per 10 thousand live births in 2016, being higher in the Northeast region in both years (12.6 in 2015 and 7.1 in 2016). We observed an increase in prevalence rates in 2016 for the Midwest (1.1 to 3.7) and North regions (0.4 to 1.4), when compared to the same coefficients for the year 2015 (Table 1).
Table 1 - Distribution of notified and confirmed cases of congenital syndrome associated with Zika virus infection in live births, according to year of birth, Region and Federative Unit of mother’s residence, Brazil, 2015-2016
| Region Federation Unit | 2015 | 2016 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Notified cases | Confirmed cases | Notified cases | Confirmed cases | |||||||
| n | n | % | Prevalence ratea | % with laboratory confirmation | n | n | % of total Notified | Prevalence ratea | % with laboratory confirmation | |
| Midwest | 251 | 28 | 11.2 | 1.1 | 17.9 | 386 | 81 | 21.0 | 3.7 | 43.2 |
| Distrito Federal | 12 | 2 | 16.7 | 0.3 | 50.0 | 55 | 8 | 14.5 | 1.6 | 25.0 |
| Goiás | 65 | 5 | 7.7 | 0.6 | 40.0 | 139 | 22 | 15.8 | 3.0 | 86.4 |
| Mato Grosso | 166 | 19 | 11.4 | 3.4 | 5.3 | 149 | 30 | 20.1 | 5.9 | 23.3 |
| Mato Grosso do Sul | 8 | 2 | 25.0 | 0.5 | 50.0 | 43 | 21 | 48.8 | 5.0 | 33.3 |
| Northeast | 3,969 | 1,071 | 27.0 | 12.6 | 21.0 | 2,651 | 555 | 20.9 | 7.1 | 14.8 |
| Alagoas | 162 | 25 | 15.4 | 4.8 | 0.0 | 195 | 58 | 29.7 | 12.5 | 0.0 |
| Bahia | 704 | 232 | 33.0 | 11.4 | 6.5 | 734 | 163 | 22.2 | 8.4 | 6.1 |
| Ceará | 263 | 43 | 16.3 | 3.2 | 25.6 | 288 | 61 | 21.2 | 4.9 | 24.6 |
| Maranhão | 168 | 81 | 48.2 | 7.0 | 2.5 | 128 | 59 | 46.1 | 5.6 | 22.0 |
| Paraíba | 719 | 94 | 13.1 | 16.0 | 17.0 | 192 | 80 | 41.7 | 14.6 | 28.8 |
| Pernambuco | 1,345 | 332 | 24.7 | 22.7 | 48.5 | 828 | 64 | 7.7 | 4.9 | 28.1 |
| Piauí | 118 | 65 | 55.1 | 12.6 | 3.1 | 71 | 28 | 39.4 | 5.7 | - |
| Rio Grande do Norte | 313 | 99 | 31.6 | 20.0 | 3.0 | 128 | 15 | 11.7 | 3.6 | - |
| Sergipe | 177 | 100 | 56.5 | 27.6 | 15.0 | 87 | 27 | 31.0 | 8.3 | 11.1 |
| North | 120 | 12 | 10.0 | 0.4 | 16.7 | 379 | 58 | 15.3 | 1.9 | 24.1 |
| Acre | 9 | - | - | - | - | 42 | 1 | 2.4 | 0.6 | 100.0 |
| Amapá | 4 | 2 | 50.0 | 1.2 | - | 8 | 3 | 37.5 | 1.8 | - |
| Amazonas | 3 | - | - | - | - | 54 | 24 | 44.4 | 3.2 | 20.8 |
| Pará | 13 | 2 | 15.4 | 0.1 | 100.0 | 99 | 6 | 6.1 | 0.5 | 100.0 |
| Rondônia | 10 | 5 | 50.0 | 1.8 | - | 35 | 7 | 20.0 | 2.7 | 14.3 |
| Roraima | 1 | 1 | 100.0 | 0.9 | - | 29 | 11 | 37.9 | 10.1 | 9.1 |
| Tocantins | 80 | 2 | 2.5 | 0.8 | - | 112 | 6 | 5.4 | 2.6 | - |
| Southeast | 379 | 48 | 12.7 | 0.4 | 2.1 | 1,621 | 161 | 9.9 | 1.4 | 24.2 |
| Espírito Santo | 54 | 2 | 3.7 | 0.4 | - | 156 | 16 | 10.3 | 3.2 | 50.0 |
| Minas Gerais | 33 | - | - | - | - | 217 | 15 | 6.9 | 0.6 | 6.7 |
| Rio de Janeiro | 150 | 42 | 28.0 | 1.8 | 2.4 | 616 | 103 | 16.7 | 4.8 | 14.6 |
| São Paulo | 142 | 4 | 2.8 | 0.1 | - | 632 | 27 | 4.3 | 0.5 | 55.6 |
| South | 30 | 2 | 6.7 | 0.0 | - | 167 | 2 | 1.2 | 0.1 | 50.0 |
| Paraná | 16 | - | - | - | - | 30 | 1 | 3.3 | 0.1 | 100.0 |
| Rio Grande do Sul | 13 | 2 | 15.4 | 0.1 | - | 131 | - | 0.0 | 0.0 | - |
| Santa Catarina | 1 | - | - | - | - | 6 | 1 | 16.7 | 0.1 | - |
| Brazil | 4,749 | 1,161 | 24.4 | 3.8 | 20.1 | 5,204 | 857 | 16.5 | 3.1 | 20.0 |
a) Coefficient of prevalence: number of cases per 10 thousand live births.
Figure 2 presents the distribution of notifications of live births for the years 2015 and 2016, as well as the cases confirmed durings the period, by month of birth. We observed a peak of notifications in November 2015, with subsequent reduction until April 2016. Then, there was an stabilization in the monthly number of notifications until the month of August, when they began to fall. The number of confirmed cases followed the curve of notifications, with a peak in November and December 2015. Analyzing the cumulative distribution, there was an increase in notifications from October 2015, with an accelerated increment until March 2016, when we note a reduction in the monthly increment.
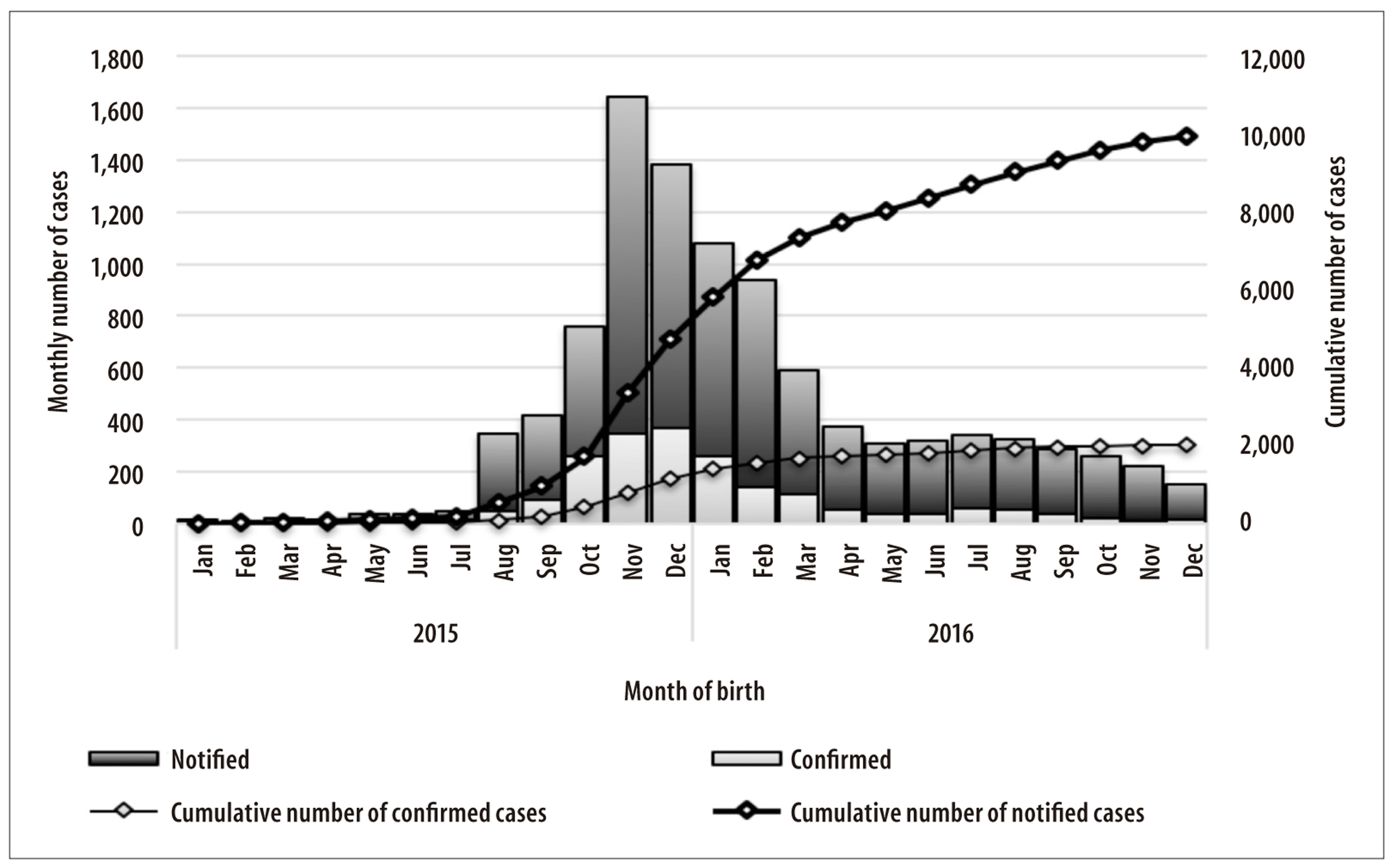
Figure 2 - Monthly and cumulate distribution of notified and confirmed of congenital syndrome associated with Zika virus infection in live births, according to year of birth, region and Federative Unit of mother’s residence, Brazil, 2015-2016
One third of Brazilian municipalities (33.2%) presented at least one suspect case notified; less than half of these municipalities presented confirmed cases (40.8%). The Northeast region concentrated a greater number of cities with cases and deaths, notified and confirmed, affecting 1,049 (58.5%) of the 1,794 municipalities in the region. Most of the notified cases was concentrated in the Northeast region of Brazil (65.7%), followed by the Southeast regions (20.6%) and Midwest regions (6.5%). The five states with the highest number of notified cases were Pernambuco (21.3%), Bahia (14.3%), Paraíba (9.0%), São Paulo (8.1%) and Rio de Janeiro (7.8%) (data not shown in table).
The distribution of notified and confirmed cases of CZS of live births per month of birth and region of residence of the mother, is presented in Figure 3. The Northeast was the region with the largest number of monthly notifications of suspected cases born between the months of August 2015 and May 2016, as well as of confirmed cases in the same period. Most of the other regions maintained a similar number of monthly notifications, throughout this period; the exception was the Southeast region, where we found an increase in the number of notifications from December 2015, although without an increase in the number of confirmed cases.
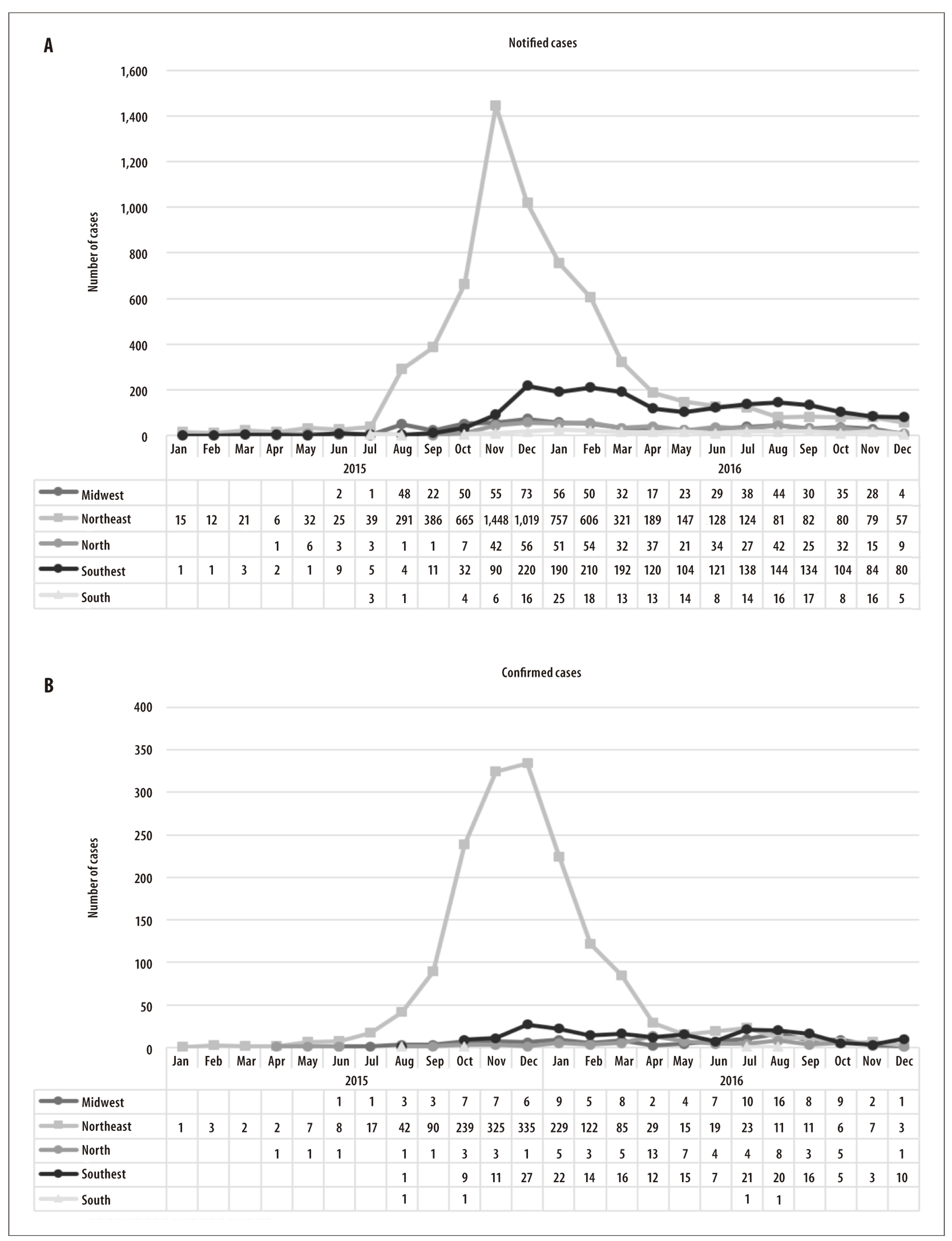
Figure 3 - Distribution of notified (A) and confirmed cases (B) per month of congenital syndrome associated with Zika virus infection in livebirths, according to year of birth and region of mother´s residence, Brazil, 2015-2016
In 2015, we observed a prevalence rate of notifications equal to or greater than 10 to 20 cases per thousand live births in most of the states of the Northeast region, as well as in the states of Mato Grosso and Tocantins (Figure 4). In the same year, Rio Grande do Norte, Pernambuco and Sergipe presented 20 or more cases confirmed per 10 thousand live births, while the states of Piauí, Paraíba and Bahia reported prevalence rates of confirmed cases in the range of 10 to 19 cases per 10 thousand live births.
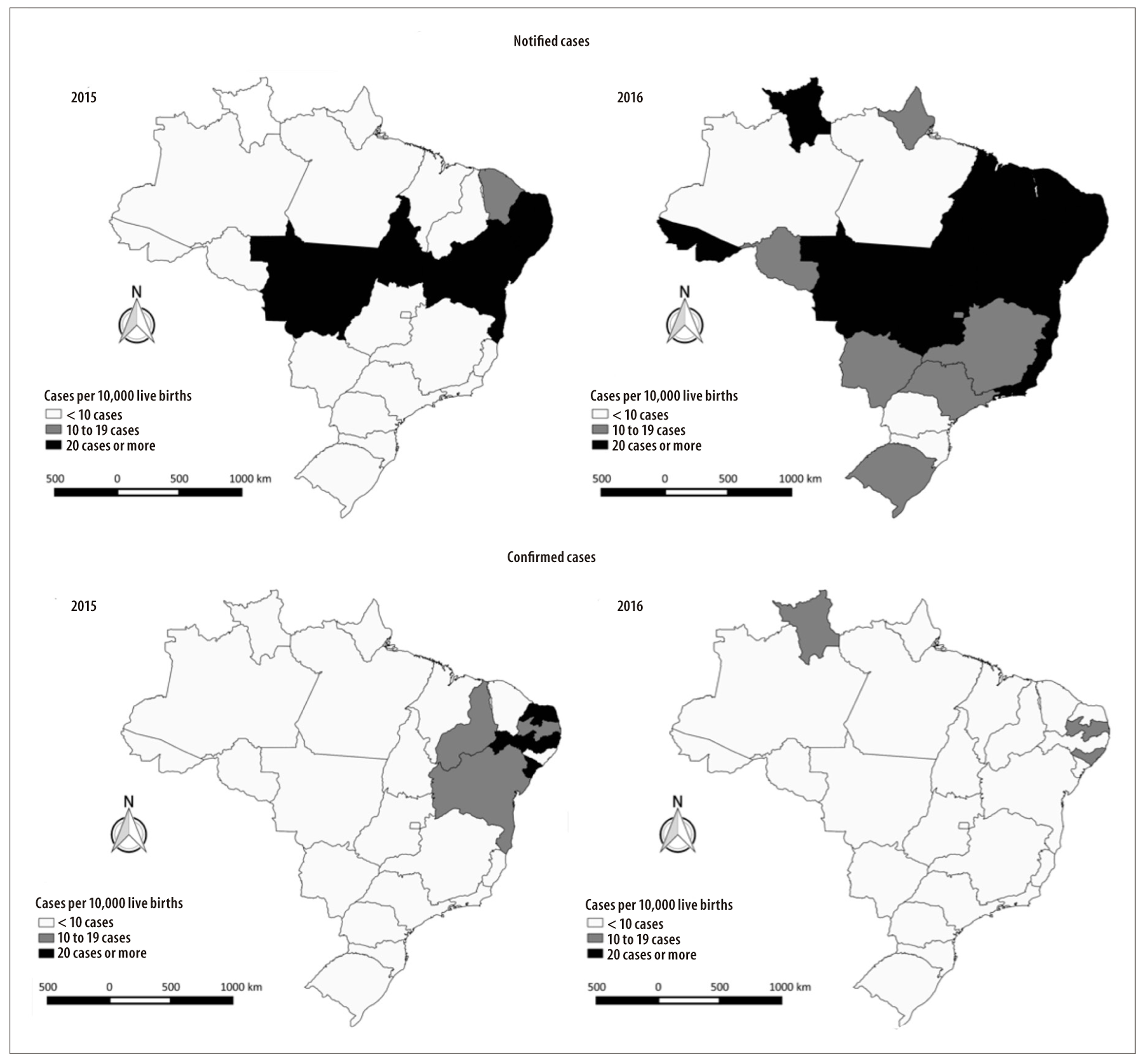
Figure 4 - Spatial distribution of the prevalence rates (per 10 thousand livebirths) of notified and confirmed cases of congenital syndrome associated with Zika virus infection in livebirths, according to year of birth and Federative Unit of mother´s residence Brazil, 2015-2016
In 2016, all the states of the Northeast presented coefficients of prevalence of reported cases ≥20 cases per 10 thousand live births, as well as the states of Acre, Roraima, Tocantins, Goiás, Mato Grosso, Espírito Santo and Rio de Janeiro. In the same year, confirmed cases showed the highest rates (in the range of 10 to 19 cases per 10 thousand live births) in the states of Paraiba and Alagoas in the Northeast region, and Roraima in the North region (Figure 4).
Discussion
The present study showed the distribution of notified and confirmed cases of CZS countrywide since the emergence of the epidemic, in August 2015, through the epidemic peak in the last bimester of the same year and covering its decline until the end of next year. The Northeast region presented the higher prevalence of cases, followed by the Midwest and North regions.
We observed a short period between the emergence and the decline of the epidemic, with subsequent maintenance of a low number of new cases of CZS throughout 2016. This behavior of the CZS is consistent with the “explosive” characteristic of the epidemic of the Zika virus disease, previously observed in Southeast Asia.22 It is estimated that approximately three quarters of the 7,500 inhabitants of Yap island in Federated States of Micronesia were infected by the Zika virus during the outbreak occurred in 2007. This outbreak disappeared in three months, with no record of admissions or deaths related to the disease. In the outbreak occurred in French Polynesia in 2013-2014, more than 32,000 inhabitants (12% of the population of the country) sought health care services presenting clinical symptoms suggestive of infection.23
In Brazil, the Northeast region has concentrated the greatest number of cases of CZS, indicating that the region was, possibly, the entry point of the virus in the country.24 It is important to emphasize, in addition, that Brazil, since the decade of 1940, has been facing of epidemics caused by dengue. However, the most intense circulation of the four serotypes of the virus occurred in the decade of 1980. Historically, states in the Northeast, Midwest and Southeast have been responsible for the higher incidence of dengue cases. In 2014, 15.3% (n=90,192) of probable cases of dengue were registered in the country among residents in the Northeast region.25
The presence of the vector, Aedes aegypti, combined with favorable environmental conditions for their proliferation, enabled the transmission of the dengue virus, chikungunya, and the Zika virus. In this context, a study using the Sinasc database revealed a higher prevalence of microcephaly among livebirths to mothers with low education level, black skin color and unmarried, which indicate poor socioeconomic conditions.26
The actions to prevent and control the Zika virus disease carried out in Brazil, mainly focused on combating A. aegypti, may have contributed to the decrease in the number of live births with CZS observed throughout the year of 2016, and in 2017.27 Concomitantly to the declaration of PHENC in November 2015, the Interministerial Strategic Group on Public Health Emergency of National and International Importance was activated. In the following month, the National Coordination and Control Room was set up to deal with diseases transmitted by A. aegypti. Local rooms were also deployed in all FU, with participation of representatives from the Brazilian Ministry of Health and Secretariats of Health, from other sectors, such as Education, Civil Defense, Armed Forces and Social Services.28
Among the actions carried out by the Ministry of Health with the objective of speeding up the investigations and conclusion of the cases, we highlight the implementation of the Rapid Action Strategy for Strengthening Health Care and Social Protection of Children with microcephaly through the Interministerial Ordinance No. 405 of March 15, 2016, of Brazilian National Health System (SUS) and the Brazilian National Social Services (SUAS). In March to October 2016, task forces were performed in different reference services for diagnosis, allowing to (i) close epidemiological investigations on a substantial number of cases and (ii) better referrals of cases for continuity of care at health points.28
Some limitations of the present study need to be considered, for adequate interpretation of the findings. First, the majority of confirmed cases were concluded on the basis of signs observed by imaging exams, which indicate alterations related to congenital infections, although not specific to the Zika virus. The mostly described alterations were the calcifications and ventriculomegaly, used for confirmation without etiological identification because there are no pathognomonic alterations for CZS.15 In December 2016, with the publication of the document 'Integrated guidelines for surveillance and health care in the context of the Public Health Emergency of National Concern',1 a compilation of signs and symptoms related to SCZ was made available, based on a consensus of specialists built at a meeting held in the city of Recife, Pernambuco, Brazil, by PAHO/WHO. This publication has allowed a better characterization of morphological, physiological and neurological findings considered for notification of suspected cases. However, important gaps in knowledge about the consequences of congenital infection by Zika virus remain, making it impossible until now, a final characterization of the CZS.
The limitations for laboratory confirmation of cases were and remain important challenges for a more efficient investigation of cases. The laboratory confirmation of cases was only possible by means of reverse-transcriptase polymerase chain reaction (RT-PCR), with detection and differentiation of viral RNA. The greatest difficulty, however, was in the time restriction for the collection of biological material necessary to carry out the test, given the short period of viremia. In this way, obtaining a negative result did not discard the occurrence of infection, given that the material for examination could not have been collected in the appropriate time interval. During the emergency, the rapid tests for Zika were introduced as part of the screening, but because these tests must be confirmed by serology, they could not be used for diagnostic confirmation of CZS. Challenges persist regarding the validity of existing tests, especially of the rapid test and of commercial kits for serological tests.
During the PHENC, different case definitions were adopted for notification and final classification of cases, previously presented here. These changes, by itself, hinder the understanding of the real epidemic curve, once the largest number of suspected cases reported at the end of 2015 can be - even if only partially - explained by the greater sensitivity of the notification criteria, by including newborn infants who would not fit into the international definition of microcephaly. However, the adoption of more sensitive definitions, initially, allowed the identification of newborns who did not present microcephaly, according to the international definition, but which had alterations in the central nervous system as a result of infection by Zika virus. In addition, such changes reflect the dynamic nature of the emergency and the active participation of experts in the construction and update of surveillance protocols, especially by Brazilian researchers, as new scientific evidence was presented.
Among the positive points in the response to the PHENC, we highlight the rapid implementation of the RESP-Microcephaly, enabling the registry of notification, research and investigation of cases throughout the national territory. This was fundamental for the adhesion of the states responsible for data management. In addition, the integration of actions of the vigilance and health care during the PHENC enabled the production of more efficient responses, both for the situational diagnosis and for an institutional response to the emergency. The information produced were indispensable for a better understanding of the manifestations of the infection by Zika virus and its potential consequences.29
It is important to highlight that this study presents the largest series of cases already published, offering information additional to those provided by the Brazilian Ministry of Health regularly, in the epidemiological bulletins. In addition, the exclusion of cases confirmed for STORCH from the analysis has led to a greater specificity in relation to CZS, in comparison with other previous studies.
The findings of this study reinforce the importance of CZS as a serious public health problem, which still imposes challenges to the research of almost one third of the cases notified in 2015-2016. Given the lack of knowledge about the Zika virus and its consequences, the results presented here reinforce the need for active and constant surveillance, especially aimed at the CZS.
Acknowledgments
The authors are grateful to the Secretaries of State and Municipal Health of 26 Brazilian states and the Federal District, especially to teams of vigilance and health care, as well as the members of the Network of Centers of Strategic Information in Health Surveillance (CIEVS) which did not measure efforts to carry out the notification and investigation of reported cases, playing a fundamental role in coping with the PHENC.
REFERENCES
1. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Secretaria de Atenção à Saúde. Orientações integradas de vigilância e atenção à saúde no âmbito da Emergência de Saúde Pública de Importância Nacional: procedimentos para o monitoramento das alterações no crescimento e desenvolvimento a partir da gestação até a primeira infância, relacionadas à infecção pelo vírus Zika e outras etiologias infeciosas dentro da capacidade operacional do SUS [Internet]. Brasília: Ministério da Saúde; 2017 [citado 2018 mar 14]. 158 p. Disponível em: Disponível em: http://portalarquivos.saude.gov.br/images/pdf/2016/dezembro/12/orientacoes-integradas-vigilancia-atencao.pdf [ Links ]
2. Del Campo M, Feitosa IM, Ribeiro EM, Horovitz DD, Pessoa AL, França GV, et al. The phenotypic spectrum of congenital Zika syndrome. Am J Med Genet A. 2017 Apr;173(4):841-57. [ Links ]
3. Costello A, Dua T, Duran P, Gülmezoglu M, Oladapo OT, Perea W, et al. Defining the syndrome associated with congenital Zika virus infection. Bull World Health Organ. 2016 Jun;94(6):406-A. [ Links ]
4. Eickmann SH, Carvalho MDCG, Ramos RCF, Rocha MAW, Linden V, Silva PFS. Síndrome da infecção congênita pelo vírus Zika. Cad Saúde Pública. 2016 jul;32(7):e00047716. [ Links ]
5. Moore CA, Staples JE, Dobyns WB, Pessoa A, Ventura CV, Fonseca EB, et al. Characterizing the pattern of anomalies in congenital Zika syndrome for pediatric clinicians. JAMA Pediatr. 2017 Mar;171(3):288-95. [ Links ]
6. Oliveira WK, Cortez-Escalante J, Oliveira WTGHD, Carmo GMI, Henriques CMP, Coelho GE, et al. Increase in reported prevalence of microcephaly in infants born to women living in areas with confirmed zika virus transmission during the first trimester of pregnancy - Brazil, 2015. MMWR Morb Mortal Wky Rep. 2016 Mar;65(9):242-7. [ Links ]
7. World Health Organization. WHO statement on the first meeting of the International Health Regulations (2005) (IHR 2005) Emergency Committee on Zika virus and observed increase in neurological disorders and neonatal malformations [Internet]. 2016 [cited 2017 Sep 21]. Available from: Available from: http://www.who.int/mediacentre/news/statements/2016/1st-emergency-committee-zika/en/ [ Links ]
8. World Health Organization. International health regulations [Internet]. 3rd ed. Geneva: World Health Organization; 2016 [cited 2018 Mar 14]. 74 p. Available in: Available in: http://apps.who.int/iris/bitstream/10665/246107/1/9789241580496-eng.pdf [ Links ]
9. Heukelbach J, Alencar CH, Kelvin AA, Oliveira WK, Cavalcanti LPG. Zika virus outbreak in Brazil. J Infect Dev Ctries. 2016 Feb;10(2):116-20. [ Links ]
10. Oliveira Melo AS, Malinger G, Ximenes R, Szejnfeld PO, Sampaio SA, Filippis AMB. Zika virus intrauterine infection causes fetal brain abnormality and microcephaly: tip of the iceberg? Ultrasound Obstet Gynecol. 2016 Jan;47(1):6-7. [ Links ]
11. Rasmussen SA, Jamieson DJ, Honein MA, Petersen LR. Zika virus and birth defects - reviewing the evidence for causality. N Engl J Med. 2016 May;374(20):1981-7. [ Links ]
12. Krauer F, Riesen M, Reveiz L, Oladapo OT, Martínez-Vega R, Porgo TV, et al. Zika virus infection as a cause of congenital brain abnormalities and guillain-barré syndrome: systematic review. PLoS Med. 2017 Jan;14(1):e1002203. [ Links ]
13. Oliveira WK, França GVA, Carmo EH, Duncan BB, Kuchenbecker RS, Schmidt MI. Infection-related microcephaly after the 2015 and 2016 Zika virus outbreaks in Brazil: a surveillance-based analysis. The Lancet. 2017 Aug;390(10097):861-70. [ Links ]
14. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Registro de Eventos em Saúde Pública (RESP-Microcefalia) [Internet]. 2015 [citado 2018 mar 14]. Disponível em: Disponível em: http://www.resp.saude.gov.br/microcefalia#/painel [ Links ]
15. França GVA, Schuler-Faccini L, Oliveira WK, Henriques CMP, Carmo EH, Pedi VD, et al. Congenital Zika virus syndrome in Brazil: a case series of the first 1501 livebirths with complete investigation. The Lancet. 2016 Aug;388(10047):891-7. [ Links ]
16. Fenton TR, Kim JH. A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatr. 2013 Apr;13:59. [ Links ]
17. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Protocolo de vigilância e resposta à ocorrência de microcefalia e/ou alterações do sistema nervoso central (SNC): emergência de saúde pública de importância internacional - ESPII 2016 [Internet]. Brasília: Ministério da Saúde; 2015 [citado 2018 mar 14]. 55 p. Disponível em: Disponível em: http://portalarquivos.saude.gov.br/images/pdf/2016/marco/24/Microcefalia-Protocolo-vigil--ncia-resposta-versao2.1.pdf [ Links ]
18. Villar J, Ismail LC, Victora CG, Ohuma EO, Bertino E, Altman DG, et al. International standards for newborn weight, length, and head circumference by gestational age and sex: the Newborn Cross-Sectional Study of the Intergrowth-21st Project. The Lancet. 2014 Sep;384(9946):857-68. [ Links ]
19. World Health Organization. WHO child growth standards: methods and development: head circumference-for-age, arm circumference-for-age, triceps skinfold-for-age and subscapular skinfold-for-age: head circumference-for-age, arm circumference-for-age, triceps skinfold-for-age and subscapular skinfold-for-age [Internet]. Geneva: World Health Organization; 2007 [cited 2018 Mar 14]. 217 p. Available in: Available in: http://www.who.int/childgrowth/standards/second_set/technical_report_2.pdf [ Links ]
20. Stegmann BJ, Carey JC. TORCH infections. Toxoplasmosis, other (syphilis, varicella-zoster, parvovirus b19), rubella, cytomegalovirus (CMV), and herpes infections. Curr Womens Health Rep. 2002 Aug;2(4):253-8. [ Links ]
21. Ministério da Saúde (BR). Departamento de informática do SUS. Sistema de informações de nascidos vivos. Eventos vitais [Internet]. 2016 [citado 2018 mar 14]. Disponível em: Disponível em: http://www2.datasus.gov.br/DATASUS/index.php?area=060702 [ Links ]
22. Duffy MR, Chen T-H, Hancock WT, Powers AM, Kool JL, Lanciotti RS, et al. Zika virus outbreak on yap island, federated states of Micronesia. N Engl J Med. 2009 Jun;360:2536-43. [ Links ]
23. Cao-Lormeau VM, Roche C, Teissier A, Robin E, Berry AL, Mallet HP, et al. Zika virus, French polynesia, South pacific, 2013. Emerg Infect Dis. 2017 Jun;20(6):1085-6. [ Links ]
24. Faria NR, Quick J, Claro IM, Thézé J, Jesus JG, Giovanetti M, et al. Establishment and cryptic transmission of Zika virus in Brazil and the Americas. Nature. 2017 Jun;546(7658):406-10. [ Links ]
25. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Monitoramento dos casos de dengue e febre de chikungunya até a Semana Epidemiológica (SE) 53 de 2014. Bol Epidemiológico. 2015;46(3):1-7. [ Links ]
26. Marinho F, Araújo VEM, Porto DL, Ferreira HL, Coelho MRS, Lecca RCR, et al. Microcefalia no Brasil: prevalência e caracterização dos casos a partir do Sistema de Informações sobre Nascidos Vivos (Sinasc), 2000-2015. Epidemiol Serv Saúde. 2016 out-dez;25(4):701-12. [ Links ]
27. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Monitoramento dos casos de dengue, febre de chikungunya e febre pelo vírus Zika até a Semana Epidemiológica 49, 2017. Bol Epidemiológico. 2017;48(5):1-13. [ Links ]
28. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Vírus Zika no Brasil: a resposta do SUS [Internet]. Brasília: Ministério da Saúde; 2017 [citado 2018 mar 14]. 136 p. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/virus_zika_brasil_resposta_sus.pdf [ Links ]
29. Garcia LP, Duarte E. Evidências da vigilância epidemiológica para o avanço do conhecimento sobre a epidemia do vírus Zika. Epidemiol Serv Saúde. 2016 out-dez;25(4):679-81 [ Links ]
In the article “Congenital syndrome associated with Zika virus infection among live births in Brazil: a description of the distribution of reported and confirmed cases in 2015-2016”, DOI: 10.5123/S1679-49742018000200014, published on Epidemiology and Health Services, 27(2):1-12, page 10:
Original text:
França GVA and Garcia LP participated in the conception and design of the study. França GVA, Garcia LP, I RV, Carmo GMI, loyal MB and Garcia MHO performed the analysis and interpretation of the results, writing and critical review of the manuscript.
Corrected text:
França GVA and Garcia LP participated in the conception and design of the study. França GVA, Garcia LP, Pedi VD, Carmo GMI, Leal MB and Garcia MHO performed the analysis and interpretation of the results, writing and critical review of the manuscript.
Received: December 04, 2017; Accepted: February 17, 2018
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
