










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.27 no.4 Brasília dez. 2018 Epub 13-Nov-2018
http://dx.doi.org/10.5123/s1679-49742018000400008
ORIGINAL ARTICLE
Syphilis in pregnancy and congenital syphilis and their relationship with Family Health Strategy coverage, Goiás, Brazil, 2007-2014: an ecological study*
1Universidade Federal de Goiás, Instituto de Patologia Tropical e Saúde Pública, Goiânia, GO, Brasil
2Secretaria de Estado da Saúde de Goiás, Coordenação Estadual de DST/Aids, Goiânia, GO, Brasil
3Instituto Federal de Educação, Ciência e Tecnologia de Goiás, Núcleo de Estudos e Pesquisas em Promoção da Saúde, Goiânia, GO, Brasil
Objective:
to analyze the incidence of syphilis in pregnant women (SPW) and congenital syphilis (CS) and the correlation of these indicators with Family Health Strategy (FHS) coverage in Goiás, Brazil, from 2007 to 2014.
Methods:
this was an ecological study using Notifiable Diseases Information System (SINAN) data and data from the Health Ministry’s Department of Primary Care; Spearman's correlation was used to evaluate the relationship between FHS coverage and syphilis incidence.
Results:
SPW incidence increased from 2.8 to 9.5/1,000 live births, while CS incidence increased from 0.3 to 2.5/1,000 live births (p<0.05) in the period 2007-2014; there was a significant increase in CS cases in municipalities with percentage FHS coverage below 75% (p<0.001).
Conclusion:
the concomitant increase in SPW and CS incidence suggests failures in the prevention of vertical transmission of syphilis, especially in regions with lower FHS coverage.
Keywords: Syphilis; Syphilis, Congenital; Pregnant Women; Family Health Strategy; Ecological Studies.
Introduction
The World Health Organization (WHO) estimates that, every year there are more than a million new cases of pregnant women with Treponema pallidum infection worldwide, with risk of adverse outcomes in 65% of these pregnancies. 1 In view of this scenario, global initiatives were rolled out to eliminate vertical transmission of syphilis by 2015, with the aim of achieving incidence rates below 0.5 cases per 1,000 live births. In order to achieve this target, it was stipulated that at least 90% of pregnant women with syphilis should receive adequate treatment. 1,2
It is known that pregnant women diagnosed and treated early have reduced risk of vertical transmission of syphilis and less likelihood of having unfavorable outcomes for the baby, when compared to those receiving late antibiotic intervention. 3 Inadequate antenatal care, in turn, is a critical factor for increased cases of congenital syphilis (CS), given that for the most part the opportunity for diagnosis and treatment arises during this period. 4,5
The Family Health Strategy (FHS), proposed as a health care model by the National Primary Health Care Policy, has contributed to the scaling up of health service provision in Brazil. Nevertheless, FHS faces substantial challenges with regard to the population having comprehensive and timely access to these services. 6
Antenatal care is an important component of the care offered by family health teams and is a key moment for adequate management of infections that can be transmitted from mother to child, such as syphilis, a disease capable of raising the risk of fetal loss in up to 21% of infected pregnant women, when compared to their uninfected counterparts. 7
The Rede Cegonha (Stork Network) was created within the Brazilian Unified Health System (SUS) in 2011. It established guidelines for quality maternal and child care. Reducing congenital syphilis (CS) was proposed as an essential strategy within its antenatal component. Scaling up rapid testing for syphilis in the first and third trimesters of pregnancy was recommended with the aim of making timely diagnosis and treatment feasible. 8 The assumption is that scaling up pregnant women’s access to the antenatal care service network in Brazil, preferably in FHS primary health care facilities, 8 is an important ally in reducing harm to the health of mother and child, including vertical transmission of syphilis.
The objective of this study was to analyze the incidence of syphilis in pregnant women (SPW) and congenital syphilis (CS) and the correlation of these indicators with FHS coverage in the state of Goiás between 2007 and 2014.
Methods
We conducted an ecological study of recorded cases of CS and SPW in the state of Goiás and also of FHS coverage in municipalities in Goiás reporting cases for the period 2007 to 2014.
In 2015 the population of the state of Goiás was estimated to be 6,778,772 inhabitants distributed over 246 municipalities which, in turn, are grouped into five Health Macroregions: Northeast, West Central, North Central, Southeast and Southwest. 9
The study’s target population was comprised of all CS and SPW cases reported in Goiás, by municipality and health macroregion during the study period. FHS was taken to be a proxy for access to health services including antenatal care.
The dependent variables were the CS incidence coefficient and the SPW detection coefficient per 1,000 live births. The independent variables included FHS coverage in the municipalities reporting CS and SPW cases, clustered into four intervals according to percentage Family Health coverage - 1st interval, ≤25%; 2nd interval, >25% and <50%; 3rd interval, ≥50% and <75%; and 4th interval, ≥75%) - and the state’s health macroregions (West Central, Northeast, North Central, Southeast and Southeast Central).
Data was retrieved from the following health information systems in Goiás: Notifiable Diseases Information System (SINAN); Live Births Information System (SINASC); and Primary Care Information System (SIAB), via the Primary Health Department (DAB) of the Health Care Secretariat/Ministry of Health.
The data relating to percentage FHS coverage per municipality were imported from DAB’s website, taking the month of June of each year.
In order to calculate CS incidence coefficients, we used the number of cases reported per year of diagnosis and place of residence, divided by the number of live births in the same place and year, multiplied by 1,000. The SPW detection coefficients were derived from the ratio between the number of pregnant women reported as having syphilis and the number of live births in the same year and place, multiplied by the constant of 1,000 live births.
In order to analyze the correlation between FHS coverage and syphilis incidence (SPW and CS), we considered those municipalities that reported at least one case between 2007 and 2014, excluding places reporting no cases and places with no information on cases. Scatter graphs were produced for the syphilis incidence coefficients (SPW and CS) in relation to percentage FHS coverage. Spearman’s correlation (r=rho) was applied as a statistical test, with the purpose of verifying the relationship between FHS coverage and CS and SPW incidence for each year being studied.
Fisher’s exact test (mid-P method) 10 was used to compare differences in FHS coverage proportions between the SPW and CS incidence coefficients for the period 2007-2014. The cumulative incidence ratios were also calculated, i.e. the rate ratios (RR) for the indicators between the first year and the last year of the time series.
Data analysis was performed using Microsoft® Excel 2010 and IBM® SPSS Statistics 22.0. P-values of <0.05 were taken to be statistically significant for all the statistical tests.
The study project was approved by the Federal University of Goiás Research Ethics Committee as per Consolidated Report No. 882.963/2014 and Consolidated Report No. 1.005.446/2015, in accordance with the guidelines of National Health Council Resolution No. 466, dated December 12th 2012.
Results
Between 2007 and 2014, 3,890 cases of SPW and 663 cases of CS were reported for the whole of the state of Goiás. Of total CS cases, 99.0% (657) were reported in children aged under one year old, 75.2% (499) of whom were born to mothers who had had antenatal care. In 2014 alone, 236 CS cases were reported, accounting for 35.6% of total reported cases for the entire period studied. The SPW detection coefficient in Goiás increased 3.4 times in the period, from 2.8/1,000 live births in 2007 to 9.5/1,000 live births in 2014 (RR=3.4; p<0.001). Similarly, between 2007 and 2014, the CS incidence coefficient increased 8.3 times, from 0.3 to 2.5 cases per 1,000 live births (RR=8.3; p<0.001) (Table 1).
Table 1 - Percentage difference in congenital syphilis incidence and syphilis detection coefficients and Family Health Strategy coverage, per Health Macroregion, Goiás, 2007 and 2014
| Health Macroregion | Congenital syphilis incidence coefficient (per 1,000 live births) | Syphilis detection coefficient for pregnant (per 1,000 live births) | Family Health Strategy coverage (%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2007 | 2014 | RRa | p-valueb | 2007 | 2014 | RRa | p-valueb | 2007 | 2014 | RRa | p-valueb | |
| West Central | 0.2 | 2.9 | 14.5 | <0.001 | 2.6 | 9.8 | 3.8 | <0.001 | 60.0 | 70.0 | 1.7 | <0.001 |
| Northeast | 0.8 | 0.5 | 0.6 | 0.262 | 3.3 | 5.7 | 1.7 | <0.001 | 52.0 | 66.0 | 1.3 | <0.001 |
| North Central | 0.3 | 2.4 | 8.0 | <0.001 | 3.7 | 8.3 | 2.2 | <0.001 | 71.0 | 82.0 | 1.5 | <0.001 |
| Southeast | 0.1 | 2.6 | 26.0 | <0.001 | 4.1 | 11.4 | 2.8 | <0.001 | 58.0 | 59.0 | 1.0 | <0.001 |
| Southeast Central | 0.2 | 3.2 | 16.0 | <0.001 | 1.4 | 11.1 | 7.9 | <0.001 | 61.0 | 70.0 | 1.1 | <0.001 |
| Goiás | 0.3 | 2.5 | 8.3 | <0.001 | 2.8 | 9.5 | 3.4 | <0.001 | 55.9 | 64.6 | 1.5 | <0.001 |
a) RR: ratio rate.
b) Fisher’s exact test (mid-P method).
In 2014, all of Goiás’ health macroregions had CS incidence coefficients equal to or greater than 0.5 cases per 1,000 live births, in particular the Southeast macroregion, which had the largest incidence coefficient increase among all the state’s macroregions (RR=26.0; p<0.001). Only the Northeast macroregion showed a fall in the CS indicator between 2007 and 2014, although it was not statistically significant (RR=0.6; p=0.262). In the same period (2007-2014), the SPW detection coefficient increased in all the health macroregions (p<0.001) (Table 1).
In 2007, 51 municipalities reported cases of SPW, compared to 127 in 2014: a positive variation of 149.0% during the period. In 2007, 15 municipalities reported at least one case of CS; compared to 54 municipalities in 2014 (Figures 1 and 2).
A positive correlation was found between percentage increase in FHS coverage and the increase in the SPW detection coefficient in almost all years (p<0.05), the only exception being 2012 (r=0.106; p=0.320) (Figure 1). This positive correlation was also found in relation to CS incidence in the majority of years studied (p<0.05), with the exception of 2008 (r=0.477; p=0.117), 2012 (r=0.463; p=0.053) and 2014 (r=0.241; p=0.079), these being years in which statistical significance was not achieved (Figure 2).
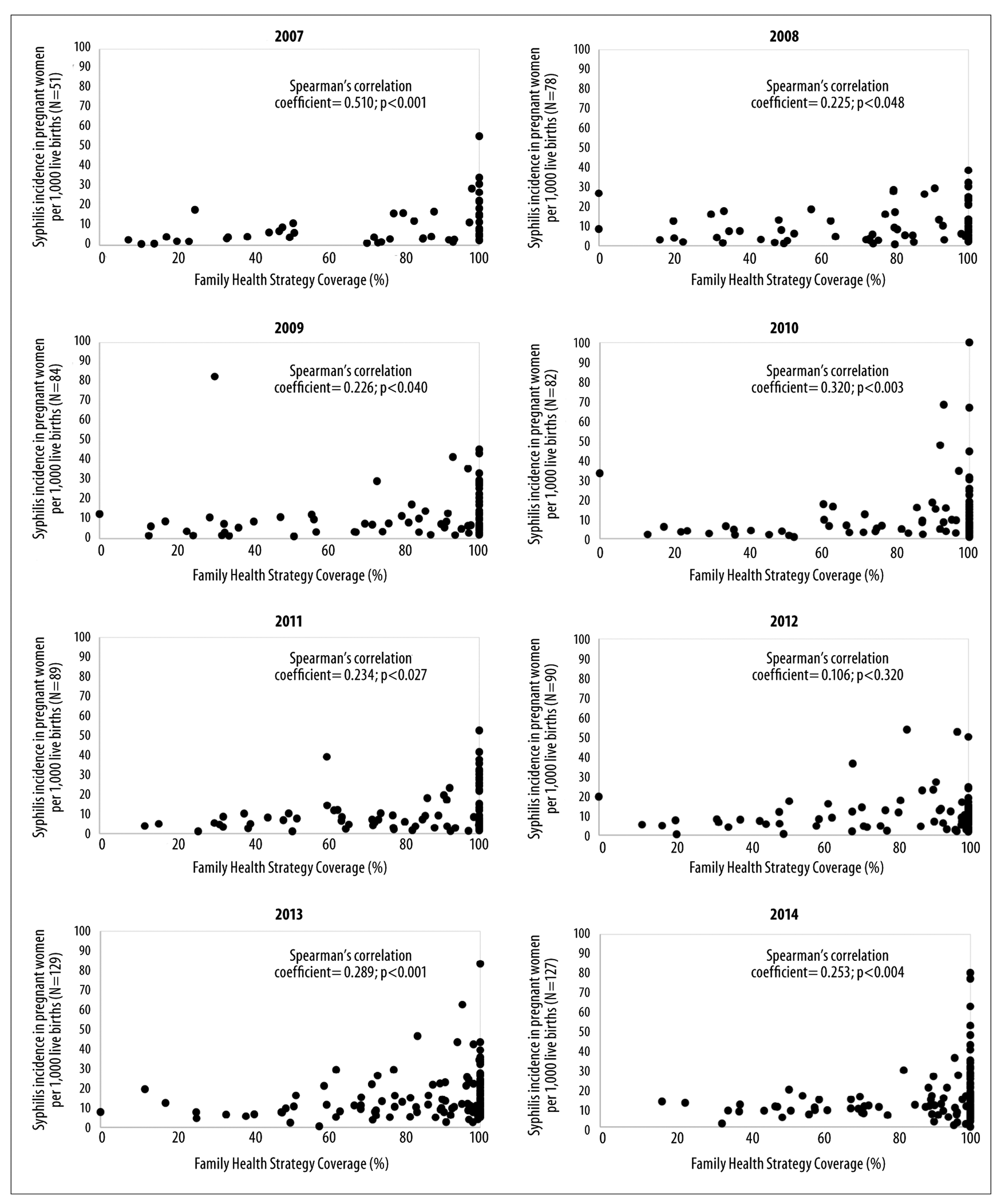
Figure 1 - Correlation between Family Health Strategy coverage and the detection coefficient for syphilis in pregnant women, Goiás, 2007-2014
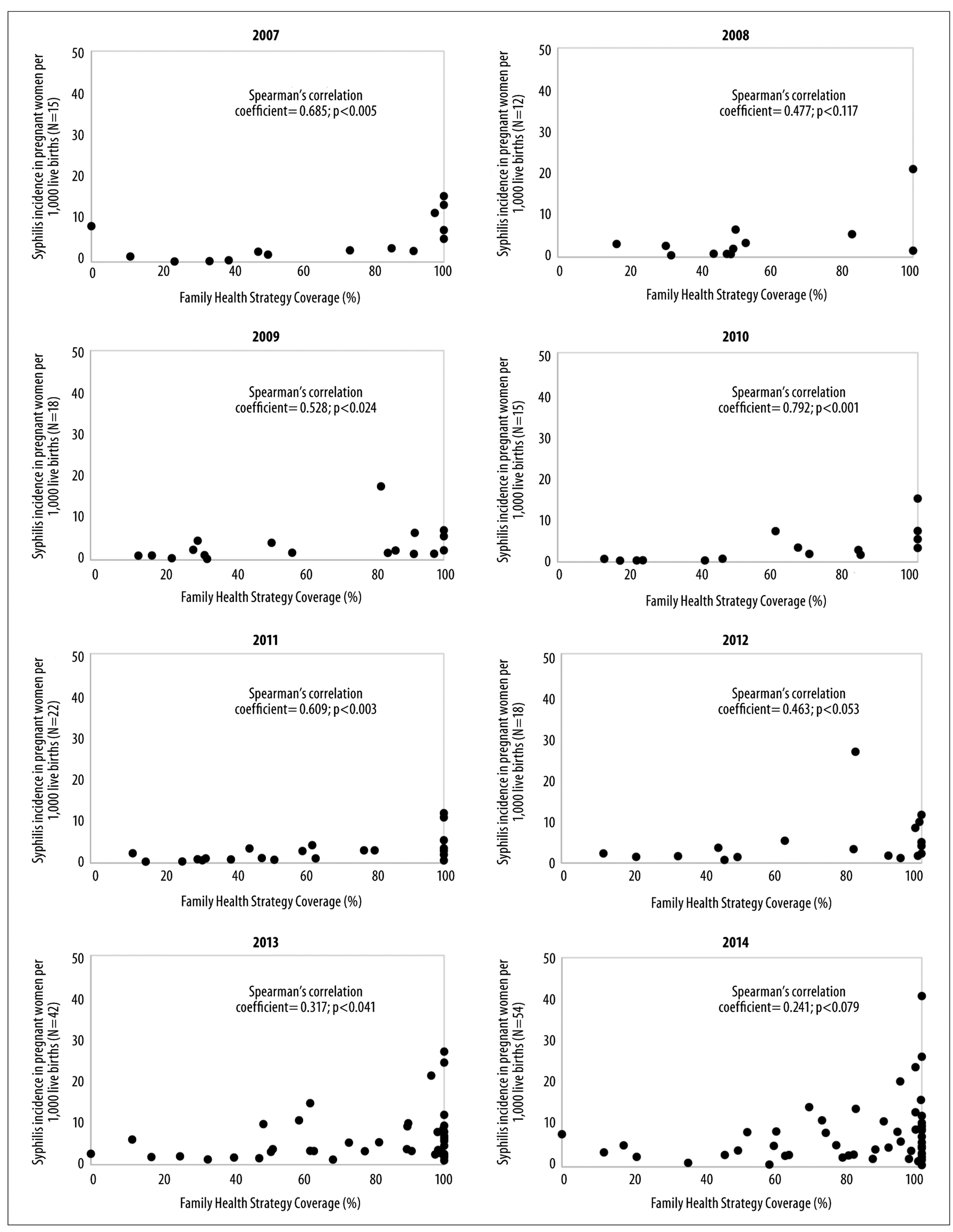
Figure 2 - Correlation between Family Health Strategy coverage and the congenital syphilis incidence coefficient, Goiás, 2007-2014
When comparing the first and last years of the time series, i.e. 2007 and 2014, a significant increase was found in the CS incidence coefficient in municipalities with FHS coverage ≤25% (RR=5.8; p<0.001), >25% and <50% (RR=7.5; p<0.001) and ≥50% and <75% (RR=1.6; p-value<0,001). Notwithstanding, in the highest FHS coverage stratum (≥75%) no statistical difference was found in the CS incidence coefficient between 2007 and 2014 (RR=0.9; p=0.602) (Table 2).
Table 2 - Variation of congenital syphilis incidence coefficients per Family Health Strategy coverage strata, Goiás, 2007 and 2014
| Family Health Strategy coverage (%) | Municipalities | Congenital syphilis incidence coefficient (per 1,000 live births) | RRa | p-valueb | ||
|---|---|---|---|---|---|---|
| 2007 (n=15) | 2014 (n=54) | 2007 | 2014 | 2007 | ||
| ≤25 | 3 | 4 | 0.6 | 3.5 | 5.8 | <0.001 |
| >25 and <50 | 3 | 3 | 0.4 | 3.0 | 7.5 | <0.001 |
| ≥50 and <75 | 2 | 9 | 2.8 | 4.5 | 1.6 | <0.001 |
| ≥75 | 7 | 38 | 5.7 | 5.1 | 0.9 | 0.602 |
a) RR: ratio rate.
b) Fisher’s exact test (mid-P method).
Discussion
There was an increase in both the number of municipalities reporting cases and also in SPW and CS incidence in the state of Goiás between 2007 and 2014. Percentage FHS coverage showed positive correlation with the number of SPW and CS cases in the majority of the years studied. It is noteworthy that the increase in the number of CS cases between 2007 and 2014 was more evident in municipalities with FHS coverage below 75%.
The design of our study does not enable a causal relationship between FHS coverage in the municipalities and the number of SPW and CS cases to be proven. FHS coverage was used as an indirect measurement of access to antenatal care; however, this is not the only indicator of access to this service. 11,12 The use of secondary data coming from passive reporting of syphilis cases, may only account for part of existing cases. Nevertheless, we believe that possible underreporting would not substantially change the direction taken by the results our study found, given that the coefficients increased over the period. There is also the possibility of the number of cases being overestimated as a result of difficulties in investigating these cases in order to confirm CS diagnosis, given that the same case reporting criteria were maintained throughout the period analyzed.
Our study investigated the relationship between syphilis incidence (CS and SPW) and FHS coverage, regardless of the length of time in service and the experience of the FHS teams. Moreover, no adjustment was made regarding the sociodemographic profile of the municipalities reporting cases.
The growth in the number of SPW and CS cases both in Goiás and also in Brazil as a whole, above all with effect from 2012, may suggest an increase in surveillance actions, in addition to indicating a real increase in the number of cases as sexually transmitted infections (IST) become more widespread, as has been observed in different regions of the world. 13,14
Greater occurrence of acquired syphilis in the Brazilian states in recent years suggests growth of unprotected sexual practices, impacting on the growth of SPW cases and having repercussions on the difficulty in interrupting the syphilis transmission chain, principally through pregnant women getting reinfected via untreated sex partners. 14,15
The ‘Handbook of Good Practices: penicillin use in primary care to prevent congenital syphilis in Brazil’ was released in 2015. Its emphasis was placed on the need for health teams to initiate treatment of pregnant women without hesitation. This recommendation was justified by rare occurrences of adverse reactions and by the existence of a specific care protocol for urgent situations in Primary Care. 15 Another important practice has been the prioritization of pregnant women regarding penicillin use in the event of penicillin stockouts. 16
Notwithstanding the existence of this and other strategies to ensure the use of penicillin by pregnant women in Primary Care especially with effect from 2015, the increase in cases in 2014, the final year of the time series we studied, may be related to factors such as: shortage of penicillin on the market; decentralized distribution of rapid syphilis tests in Primary Care leading, to increased access to screening for infection; or it may also be related to late and inadequate treatment of infection, with loss of patient follow-up in the health care network. 5,17,18
The positive correlation between the SPW detection coefficient and FHS coverage found in our study reinforces the hypothesis of scaling up syphilis testing coverage and reporting cases of infected pregnant women within FHS services. These actions are contributing to strengthening antenatal services, especially following the implantation of the stork network in 2011 and the Health Surveillance Action Qualification Program in 2013. 8,19
CS is considered to be a sentinel event regarding the quality of antenatal care. Effective health actions are capable of avoiding CS. 20 Municipalities with percentage FHS coverage below 75% had the greatest increase in the number of CS cases over the period studied when compared to those with higher FHS coverage. Within this context, apart from the need to scale up access, it is also important to investigate the response capacity of the primary health service network in the state, with the aim of proposing improvements to access to diagnosis and, above all, to adequate and timely intervention, these being aspects indicated as being weaknesses in the interruption of the transmission chain. These are conclusions reached by studies conducted in the Brazilian states of Ceará and São Paulo. 21,22
Scaling up of FHS coverage in Goiás’ health macroregions has followed the national trend. According to the Health Ministry’s Primary Care Department, in Brazil as a whole, over 15 years, expanded by more than four times the population covered by Family Health, from 14.1% in 2000 to 59.7% in 2014. 23 In Goiás, 240 family health teams were implanted between 2007 and 2014, increasing FHS coverage from 55.9% to 64.6%. 23
There was no significant decrease in CS in municipalities with higher FHS coverage (≥75%) in the period studied. This shows the need to investigate other factors interfering in the response to this congenital infection, such as sociodemographic conditions and health care conditions in these municipalities. A time series study conducted in Brazil between 2003 and 2008 found more intense CS reduction in municipalities with greater FHS coverage strata; however, the negative correlation between CS incidence and FHS coverage was not maintained following adjustment for potential confounding variables, thus suggesting that the reduction in CS might not be attributable to FHS but rather to the municipalities’ antenatal coverage and their demographic characteristics. 24
Another important aspect to raise, which is a challenge to preventing vertical transmission of syphilis, is the adequate training of health professionals, especially those working in antenatal services. 25 A study conducted in Brazil on hospitalizations owing to primary care sensitive conditions found that FHS has contributed to progress in addressing certain health conditions; however, the same investigation highlighted the need for health team training and better targeting of actions. 26
Another national study this time conducted between 2011 and 2012, found that despite high antenatal coverage, only one fifth of women attending the services received adequate care in terms of minimum procedures recommended by the Health Ministry. According to the same study, less than 50% of pregnant women had the recommended two blood tests for syphilis during pregnancy. These factors reduce the possibility of adequate intervention and contribute to increased cases of vertical transmission, as our study reveals. 19,27
The difficulties encountered in combating syphilis are countless. With the aim of providing better elucidation as to the main obstacles in controlling vertical transmission of syphilis within the context of the different Brazilian realities, the Ministry of Health encourages the creation of committees to investigate CS cases. Furthermore, in late 2014 the Ministry released its ‘Protocol for the Investigation of Vertical Transmission’ with regard to STI, HIV/AIDS and viral hepatitis surveillance, prevention and control, including cases of early CS. The publication is a guidance tool for investigating individual, care service and management vulnerabilities which have direct impact on increased cases. 28
FHS is a privileged space for territorial intervention. However, there needs to be more in-depth discussion on the issue of SPW and CS with regard to intersectoral public policies, so as to integrate FHS with other health care network points, which in turn need to be integrated with other social sectors. 6 Furthermore, the creation of spaces of social participation should be encouraged in order to jointly build actions capable of having an effective impact on the reality of this infection.
SPW and CS incidence increased over the period, and had positive correlation with increased FHS coverage in the majority of the years studied. The spread of the epidemic and loss of opportunities in preventing vertical transmission of syphilis can be seen, including in municipalities with high Family Health Strategy coverage. This indicates the need to strengthen Primary Care, in particular with regard to those aspects related to quality of antenatal care and quality of the investigation of the factors involved in vertical transmission of syphilis with the aim of achieving more assertive interventions.
REFERENCES
1. Newman L, Kamb M, Hawkes S, Gomez G, Say L, Seuc A, et al. Global estimates of syphilis in pregnancy and associated adverse outcomes: analysis of multinational antenatal surveillance data. PLoS Med. 2013;10(2):e1001396. doi: 10.1371/journal.pmed.1001396. [ Links ]
2. World Health Organization. Global guidance on criteria and processes for validation: elimination of mother-to-child transmission (EMTCT) of HIV and Syphilis [Internet]. Geneve: World Health Organization; 2014 [cited 2018 Jul 3]. 32 p. Available from: Available from: http://apps.who.int/iris/bitstream/handle/10665/112858/9789241505888_eng.pdf?sequence=1 [ Links ]
3. Hawkes SJ, Gomez GB, Broutet N. Early antenatal care: does it make a difference to outcomes of pregnancy associated with syphilis? A systematic review and meta-analysis. PLoS One. 2013;8(2):e56713. doi: 10.1371/journal.pone.0056713. [ Links ]
4. Mesquita KO, Lima GK, Filgueira AA, Flôr SMC, Freitas CASL, Linhares MSC, et al. Análise dos casos de sífilis congênita em Sobral, Ceará: contribuições para assistência pré-natal. DST-J Bras Doenças Sex Transm. 2012;24(1):20-7. doi: 10.5533/2177-8264-201224107. [ Links ]
5. Cardoso ARP, Araújo MAL, Cavalcante MS, Frota MA, Melo SP. Análise dos casos de sífilis gestacional e congênita nos anos de 2008 a 2010 em Fortaleza, Ceará, Brasil. Ciênc Saúde Coletiva. 2018 fev;23(2):563-74. doi: 10.1590/1413-81232018232.01772016. [ Links ]
6. Arantes LJ, Shimizu HE, Merchán-Hamann E. Contribuições e desafios da estratégia saúde da família na atenção primária à saúde no Brasil: revisão da literatura. Ciênc Saúde Coletiva. 2016 maio;21(5):1499-510. doi: 10.1590/1413-81232015215.19602015. [ Links ]
7. Gomez GB, Kamb ML, Newman LM, Mark J, Broutet N, Hawkes SJ. Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis. Bull World Health Organ. 2013 Mar;91(3):217-26. doi: 10.2471/BLT.12.107623. [ Links ]
8. Brasil. Ministério da Saúde. Portaria MS/GM no 1.459, de 24 de julho de 2011. Institui, no âmbito do Sistema Único de Saúde - SUS - a Rede Cegonha. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2011 jul 11; Seção I, p. 109. [ Links ]
9. Instituto Brasileiro de Geografia e Estatística. Estados@ Goiás 2015 [Internet]. 2018 [citado 2018 out 5]. Disponível em: Disponível em: http://www.ibge.gov.br/estadosat/perfil.php?lang=&sigla=go [ Links ]
10. Martin DO, Austin H. Exact estimates for a rate ratio. Epidemiology. 1996 Jan;7(1):29-33. [ Links ]
11. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Gestação de alto risco: manual técnico [Internet]. 5.ed. Brasília: Ministério da Saúde; 2012 [citado 2018 out 5]. 302 p. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/manual_tecnico_gestacao_alto_risco.pdf [ Links ]
12. Ministério da Saúde (BR). Programa nacional de melhoria do acesso e da qualidade da atenção básica (PMAQ): ficha de qualificação de indicadores [Internet]. Brasília: Ministério da Saúde ; 2012 [citado 2018 out 5]. 80p. Disponível em: Disponível em: http://189.28.128.100/dab/docs/sistemas/Pmaq/manual_instrutivo_pmaq_site_anexo.pdf [ Links ]
13. Kenyon C, Buyze J, Colebunders R. Classification of incidence and prevalence of certain sexually transmitted infections by world regions. Int J Infect Dis. 2014 Jan;18:73-80. doi: 10.1016/j.ijid.2013.09.014. [ Links ]
14. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Sífilis 2017. Bol Epidemiol. 2017 nov;48(36):1-41. [ Links ]
15. Ministério da Saúde (BR). Secretaria de Vigilancia em Saúde. Departamento de DST, Aids e Hepatites Virais. Caderno de boas práticas: o uso da penicilina na atenção básica para a prevenção da sífilis congênita no Brasil [Internet]. Brasília: Ministério da Saúde ; 2015 [citado 2018 out 5]. 96 p. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/penicilina_para_prevencao_sifilis_congenita%20_brasil.pdf [ Links ]
16. Brasil. Ministério da Saúde. Secretaria de Vigilância em Saúde. Secretaria de Ciência, Tecnologia e Insumos Estratégicos. Nota informativa conjunta n° 109/2015 GAB/SVS/MS, GAB/SCTIE/MS, de 28 outubro de 2015. Orienta a respeito da priorização da penicilina G benzatina para sífilis em gestantes e penicilina cristalina para sífilis congênita no país e alternativas para o tratamento da sífilis [Internet]. Brasília: Ministério da Saúde , 2015 [citado 2018 out 5]. 3 p. Disponível em: Disponível em: http://www.aids.gov.br/pt-br/legislacao/nota-informativa-conjunta-no-109105gabsvsms-gabsctiems [ Links ]
17. Pan American Health Organization. Elimination of mother-to-child transmission of HIV and syphilis in the Americas. Update 2016 [Internet]. Washington, D.C.: Pan American Health Organization; 2016 [cited 2018 Oct 5]. 62 p. Available: Available: http://iris.paho.org/xmlui/bitstream/handle/123456789/34072/9789275119556-eng.pdf?sequence=4&isAllowed=y [ Links ]
18. Taylor MM, Nurse-Findlay S, Zhang X, Hedman L, Kamb ML, Broutet N, et al. Estimating benzathine penicillin need for the treatment of pregnant women diagnosed with syphilis during antenatal care in high-morbidity countries. PLoS One. 2016 Jul;11(7):e0159483. doi: 10.1371/journal.pone.0159483. [ Links ]
19. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Programa de qualificação das ações de vigilância em saúde (PQA-VS): ficha de qualificação dos indicadores [Internet]. Brasília: Ministério da Saúde ; 2013 [citado 2018 out 5]. 18 p. Disponível em: Disponível em: http://www.saude.sp.gov.br/resources/ccd/homepage/acesso-rapido/gpa/caderno_indicadores_do_pqavs.pdf [ Links ]
20. Domingues RMSM, Saracen V, Hartz ZMA, Leal MC. Sífilis congênita: evento sentinela da qualidade da assistência pré-natal. Rev Saúde Pública. 2013 fev;41(1):147-57. doi: 10.1590/S0034-891020130001.00019. [ Links ]
21. Costa CC, Freitas LV, Sousa DMN, Oliveira LL, Chagas ACMA, Lopes MVO et al. Sífilis congênita no Ceará: análise epidemiológica de uma década. Rev Esc Enferm USP. 2013 fev;47(1):152-9. doi: 10.1590/S0080-623420130001.00019. [ Links ]
22. Donalísio MR, Freire JB, Mendes ET. Investigação da sífilis congênita na microrregião de Sumaré, Estado de São Paulo, Brasil - desvelando a fragilidade do cuidado à mulher gestante e ao recém-nascido. Epidemiol Serv Saúde. 2007 jul-set;16(3):165-73. doi: 10.5123/S1679-49742007000300003. [ Links ]
23. Ministério da Saúde (BR). Departamento de Atenção Básica. Histórico de cobertura saúde da família [Internet]. 2015 [citado 2018 out 5]. Disponível em: Disponível em: http://dab.saude.gov.br/portaldab/historico_cobertura_sf.php [ Links ]
24. Araújo CL, Shimizu HE, Sousa AIA, Hamann EM. Incidência da sífilis congênita no Brasil e sua relação com a estratégia saúde da família. Rev Saúde Pública. 2012 jun;46(3):479-86. doi: 10.1590/S0034-8910201200300010. [ Links ]
25. Kiarie J, Mishra CK, Temmerman M, Newman L. Accelerating the dual elimination of mother-to-child transmission of syphilis and HIV: why now? Int J Gynaecol Obstet. 2015 Jun;130(Suppl 1):S1-3. doi: 10.1016/j.ijgo.2015.05.002. [ Links ]
26. Ceccon RF, Meneghel SN, Viecili PR. Hospitalization due to conditions sensitive to primary care and expansion of the Family Health Program in Brazil: an ecological study. Rev Bras Epidemiol. 2014 Dec;17(4):968-77. [ Links ]
27. Domingues RM, Dias MA, Leal MC, Gama SG, Theme-Filha MM, Torres JA, et al. Adequacy of prenatal care according to maternal characteristics in Brazil. Rev Panam Salud Publica. 2015 Mar;37(3):140-7. [ Links ]
28. Ministério da Saúde (BR). Protocolo de infestigação de transmissão vertical [Internet]. Brasília: Ministério da Saúde ; 2014 [citado 2018 out 5]. 83 p. Disponível em: Disponível em: http://www.aids.gov.br/pt-br/pub/2014/protocolo-de-investigacao-de-transmissao-vertical [ Links ]
Received: May 27, 2018; Accepted: September 25, 2018
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
