










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.28 no.2 Brasília jun. 2019 Epub 04-Jul-2019
http://dx.doi.org/10.5123/s1679-49742019000200015
ORIGINAL ARTICLE
Evaluation of the quality of oral health care in Primary Health Care in Pernambuco, Brazil, 2014*
1Prefeitura do Recife, Secretaria Municipal de Saúde, Recife, PE, Brasil
2Fundação Instituto Oswaldo Cruz, Instituto Aggeu Magalhães, Recife, PE, Brasil
3Universidade Federal de Pernambuco, Departamento de Medicina Social, PE, Brasil
Objective:
to evaluate the quality of oral health care in Primary Health Care services in Pernambuco state, Brazil, 2014.
Methods:
this was an ecological health evaluation study based on the Donabedian model, involving secondary data from the 2nd cycle of the National Program for Improving Access and Quality of Primary Health Care (PMAQ-AB); comparison between the structure, process and outcome variables was done using the Kruskal-Wallis test (p<0.050); variables showing statistical significance (p<0.05) were portrayed through thematic and spatial dependence maps.
Results:
the standard of quality in the municipalities for the ‘Structure’ dimension gained better scores than the ‘Work process’ dimension; correlations were identified between the indicators for dental urgency, supervised tooth brushing coverage and treatments completed, in quality strata related to the work process of the Oral Health teams.
Conclusion:
organization of the work process was seen to be a determining factor in the impact on some indicators of service use.
Keywords: Primary Health Care; Health Evaluation; Quality of Health Care; Indicators of Health Services; Oral Health
Introduction
In Brazil, with the evolution of public policies on oral health in the last 20 years, improvements in oral health coverage have been made all over the country. However, important challenges still need to be overcome, such as increasingly precarious labor relations, difficulty in changing work processes, lack of integration between Primary Health Care and the health care network as a whole, infrastructure problems, shortage or disruption of supplies provision, among others.1,2 In order to overcome these obstacles, which are common to Primary Health Care (PHC) throughout Brazil, the Ministry of Health has developed practices for introducing, monitoring and evaluation processes and obtaining measurable results. One of these initiatives is the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB).
PMAQ-AB represents an important step towards making health action evaluation and monitoring actions effective in Brazil. In relation to oral health care, PMAQ-AB represents the possibility of motivating teams to think about the work process they develop, by providing the opportunity to change the way care is provided and managed, and thus enable better qualified actions and services.3
Nevertheless, the significant increase in the number of Oral health care teams (OHt), with effect from the inclusion of their work in the Family Health Strategy (FHS),2 has resulted in the need to assess the quality of the services these teams provide. It is expected that oral health, within FHS, will produce the same positive impact on service use, both by increasing service provision and also through the quality of care provided. In this sense, evaluation processes are essential tools for improving the organizational development of health services, and intensify efforts to improve their quality.3
Achieving better organization of oral health care practices in PHC is a constant challenge. Moreover, proportionally speaking, indicator performance with regard to first dental consultation, supervised tooth brushing and average individual basic dental procedures has not kept up with the percentage increase in OHt coverage in the Pernambuco state time series.4,5 This status may be related to the persistence of dental care that either cures or mutilates, to the detriment of preventive care.6 This scenario points to the need to investigate and reorganize oral health care in Pernambuco state, based on issues relating to the structure and the work process of its oral health care teams.
As such, taking as our basis health quality evaluation as proposed by the Donabedian systemic model7 involving the “structure, process and outcome” triad, in order for the population to have adequate health care, the Oral Health care teams need to have essential minimum resources (equipment, materials, supplies) and to develop their actions according to established standards. With regard to Donabedian model, although criticisms regarding its limitations are legitimate,8 nevertheless it continues to be a reference instrument for evaluating the quality of health services.3
This study aimed to evaluate oral health care in Primary Health Care services in the Brazilian state of Pernambuco, in 2014.
Methods
This is a health evaluation study based on ecological data. Its units of analysis were the 168 municipalities of the state of Pernambuco and its offshore territory known as the Fernando de Noronha archipelago, which had OHt participating in the 2nd PMAQ-AB cycle.
PMAQ-AB is comprised of four different phases, which complement each other and form a continuum of cycles. The first cycle took place in 2011 and the second in 2014. PMAQ-AB external evaluation (third phase) is a time for checking health team access and quality status through observation of aspects related to service structure and work process. In order to build the municipal quality standards for structure and process (independent variables), we used secondary data from the database created by the Ministry of Health from modules V (Structure) and VI (Process) of the PMAQ-AB (2nd cycle) external evaluation instrument in Pernambuco. The “Structure and working conditions of the primary health care unit (PHU)” dimension included 88 questions, whereas the “the OHt work process” dimension had 74 questions.9 Four indicators of oral health, described as follows, were used as dependent variables.
a) First programmatic dental consultation coverage
Number of first programmatic dental consultations carried out, in a specific place and period, divided by the population of the same place and period, multiplied by 100.
b) Dental urgencies
Number of urgent dental services provided per inhabitant, in a specific place and period, divided by the population registered at the same place and period.
c) Coverage of supervised collective tooth brushing
Annual average number of people participating in supervised collective tooth brushing, in a specific place and period, divided by the total population of the same place and period, multiplied by 100.
d) Treatments completed (proportion of treatments completed in relation to first programmatic consultations)
Number of treatments completed by the OHt divided by the number of first programmatic dental consultations carried out, multiplied by 100.
Oral health indicator data corresponded to the annual averages for the year 2014 retrieved from the SUS Outpatient Information System (SIA/SUS).10 Information on the population of each municipality was retrieved from the website of the Brazilian National Health System Information Technology Department (DATASUS), although it is based on intercensal estimates made by the Brazilian Institute of Geography and Statistics (IBGE).11
The data were systematized on Microsoft Excel spreadsheets. Following this, we analyzed and processed the data using the Statistical Package for Social Sciences - SPSS® version 20 - for Windows®, whereby we computed the number of compliances (option “yes” in answer to the variables on the questionnaire) and non-compliances (option “No”), per OHt, for each of the dimensions evaluated. Each dimension, in turn, was represented by the average adequacy scores of the subdimensions comprising it, expressed by the number of compliances or items in agreement with the PMAQ-AB parameters for each variable analyzed.
Taking the scores obtained by the 1,440 Pernambuco OHt participating in the PMAQ-AB external evaluation, that had their data processed and validated by the Sergio Arouca/Oswaldo Cruz Foundation (ENSP/Fiocruz) National School of Public Health, we calculated the averages for each municipality, with the aim of building municipal quality standards. The parameters for classifying and analyzing municipal quality standards for the teams were created from quartiles. When presenting this data, we opted for joining intermediate intervals. This way we classified the municipalities regarding the organization of their teams: Unsatisfactory, in municipalities with values ≤25%; intermediate, in municipalities with values >25% to <75%; and satisfactory, in municipalities with values ≥75%.
After processing, we applied the Kolmogorov-Smirnov test and found that the variables did not follow normal distribution. We therefore chose to use the Kruskal-Wallis non-parametric test for the comparative analysis of the scores for the PHU “Structure” dimension and the OHt “work process” dimension, as well as for the PHC dental care indicators medians. We adopted a significance level of 5%.
To estimate the spatial dependence of the dependent and independent variables, we calculated Moran’s global spatial autocorrelation index. This index, when measured at the same place, will always be 1. However, when the correlation of a variable is measured in neighboring areas, it will have a value varying between -1 and 1: The closer it is to 1, the greater the similarity between neighboring areas; 0 means there is no correlation; and negative values indicate dissimilarity. Moran’s global index allows analysis of the extent to which the level of a variable for one area is similar, or not, to those of neighboring areas.12 We also carried out a local test, which creates four spatial correlation situations:
positive values and positive averages (high-high);
negative values and negative averages (low-low);
positive values and negative averages (high-low); and
negative values and positive averages (low-high).
The first two situations indicate points of spatial association that are positive or similar to their neighboring areas, while the last two situations indicate points of spatial association that are negative, with municipalities having values different to those of their neighbors.12 We opted to only represent the spatial dependence of variables that had a spatial significance level of 5% when Moran’s global index was calculated.
The study project was approved by the Research Ethics Committee of the Aggeu Magalhães Institute/Oswaldo Cruz Foundation (IAM/Fiocruz): Report No. 2.147.398, issued on 29 June 2017, in accordance with National Health Council (CNS) Resolution No. 466, dated 12 December 2012.
Results
The overall performance score of the municipalities and the classification of the three groups in relation to the quality standards studied are shown in Table 1. We found that the “Structure” dimension quality standard had a higher score in the three classifications analyzed, when compared to the OHt “work process” dimension quality standard.
Table 1 - Score of municipalities in the state of Pernambuco and the territory of Fernando de Noronha, according to quality standards of the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB), 2014
| Quality standardsa | Unsatisfactoryb (N=42) | Intermediateb (N=85) | Satisfactoryb (N=42) | |||
|---|---|---|---|---|---|---|
| Score | Score | Score | ||||
| Minimum | Maximum | Minimum | Maximum | Minimum | Maximum | |
| Structure | 0.00 | 61.85 | 61.59 | 67.58 | 67.59 | 78.00 |
| Work process | 0.00 | 35.67 | 35.68 | 47.84 | 47.85 | 62.05 |
a) According to the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB).9
b) Analysis of the groups per quartiles, joining intermediate intervals.
We did not identify statistical significance in the comparisons of the oral health indicators among the strata of municipal quality standards relating to structure (Table 2). Regarding the quality standards relating to work process and the “dental urgency”, “supervised tooth brushing coverage” and “treatments completed” indicators, we found significant differences between the median of the indicators in the municipal quality standard strata (Table 3).
Table 2 - Distribution of oral health indicators by quality standards referring to the structure of oral health care teams, according to the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB), Pernambuco, 2014
| Quality standards | First programmatic dental consultation coverage | |||
|---|---|---|---|---|
| Median | Average | Standard deviation | Pc | |
| Unsatisfactory | 10.624 | 12.313 | 9.686 | |
| Intermediate | 14.391 | 15.425 | 9.589 | 0.069 |
| Satisfactory | 12.942 | 15.527 | 8.982 | |
| Dental urgency | 12.942 | 15.527 | 8.982 | |
| Unsatisfactory | 0.014 | 0.016 | 0.012 | |
| Intermediate | 0.013 | 0.017 | 0.017 | 0.419 |
| Satisfactory | 0.016 | 0.022 | 0.018 | |
| Supervised tooth brushing coverage | 0.016 | 0.022 | 0.018 | |
| Unsatisfactory | 0.510 | 1.143 | 1.657 | |
| Intermediate | 0.950 | 1.414 | 1.724 | 0.237 |
| Satisfactory | 0.911 | 1.526 | 1.922 | |
| Treatments completed | 0.911 | 1.526 | 1.922 | |
| Unsatisfactory | 9.495 | 17.535 | 18.829 | |
| Intermediate | 9.379 | 12.319 | 11.192 | 0.468 |
| Satisfactory | 10.219 | 14.853 | 13.254 | |
| Satisfatório | 10.219 | 14.853 | 13.254 | |
a) According to the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB).9
b) Analysis of the groups per quartiles, joining intermediate intervals.
c) P-value calculated using the Kruskal-Wallis test.
Table 3 - Distribution of oral health indicators by quality standards referring to the work process of oral health care teams, according to the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB), Pernambuco, 2014
| Quality standards | First programmatic dental consultation coverage | |||
|---|---|---|---|---|
| Median | Average | Standard deviation | Pc | |
| Work processa,b | ||||
| Unsatisfactory | 12.121 | 14.754 | 10.164 | 0.927 |
| Intermediate | 12.749 | 14.565 | 9.753 | |
| Satisfactory | 13.516 | 14.856 | 8.492 | |
| Dental urgency | ||||
| Unsatisfactory | 0.012 | 0.014 | 0.013 | 0.013 |
| Intermediate | 0.013 | 0.018 | 0.019 | |
| Satisfactory | 0.019 | 0.023 | 0.018 | |
| Supervised tooth brushing coverage | ||||
| Unsatisfactory | 0.679 | 1.135 | 1.379 | 0.012 |
| Intermediate | 0.631 | 1.157 | 1.444 | |
| Satisfactory | 1.166 | 2.054 | 2.411 | |
| Treatments completed | ||||
| Unsatisfactory | 8.231 | 11.832 | 10.747 | 0.007 |
| Intermediate | 9.295 | 13.959 | 16.225 | |
| Satisfactory | 16.318 | 17.238 | 11.654 | |
a) According to the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB).9
b) Analysis of the groups per quartiles, joining intermediate intervals.
c) P-value calculated using the Kruskal-Wallis test.
We identified positive spatial correlation (p=0.030) among the variables for the OHt work process quality standard; consequently, the hypothesis of spatial autocorrelation (positive values, positive averages) for this variable (Figure 1) should not be rejected. Still regarding the work process, we noticed areas of spatial dependence concentrated in municipalities of the Zona da Mata Norte region in Pernambuco, categorized as having a satisfactory quality standard in relation to the organization and development of oral health care services.
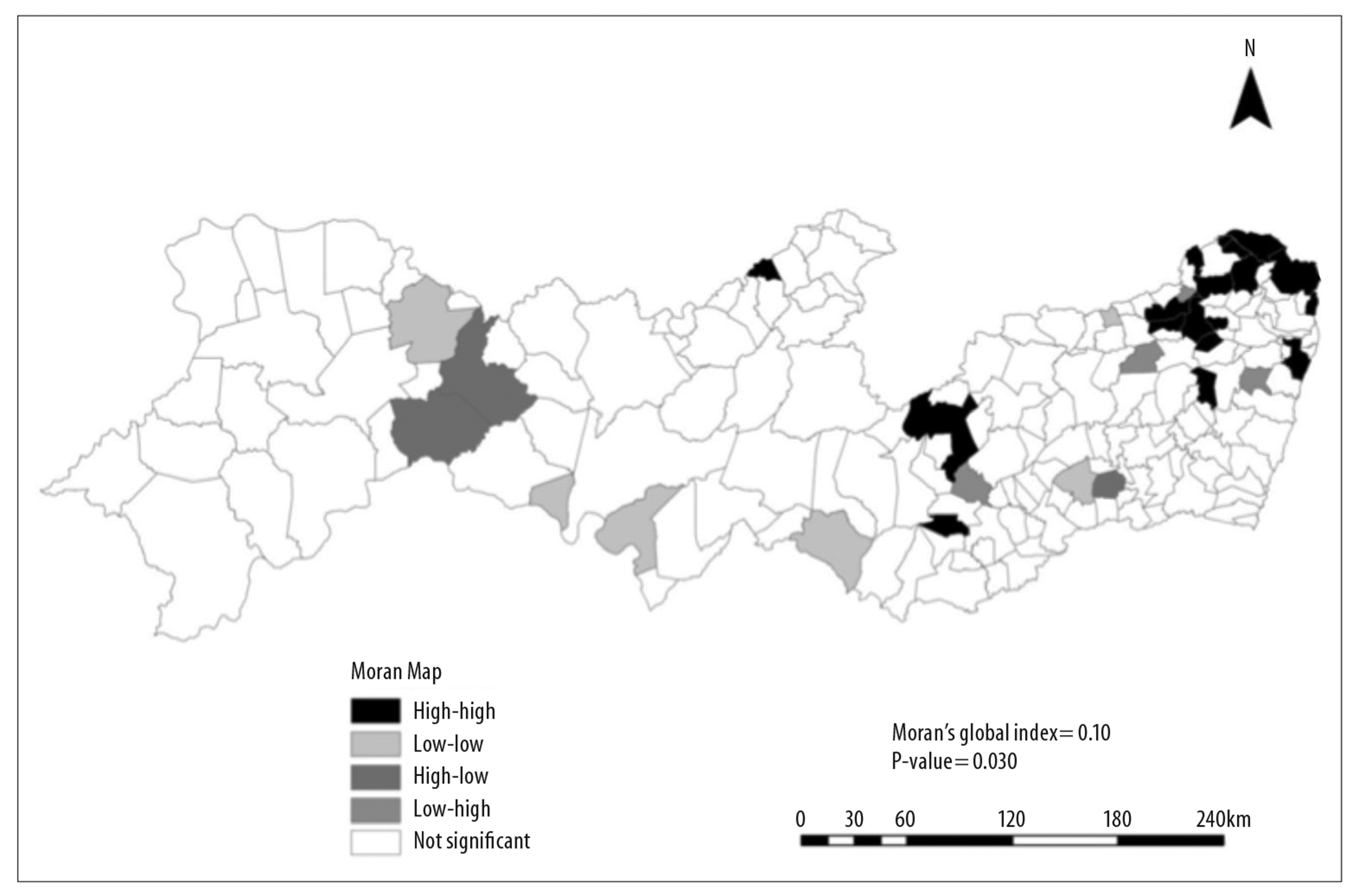
Figure 1 - Spatial analysis (Moran Map) of municipal quality standards for oral health care team work process according to the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB), Pernambuco, 2014
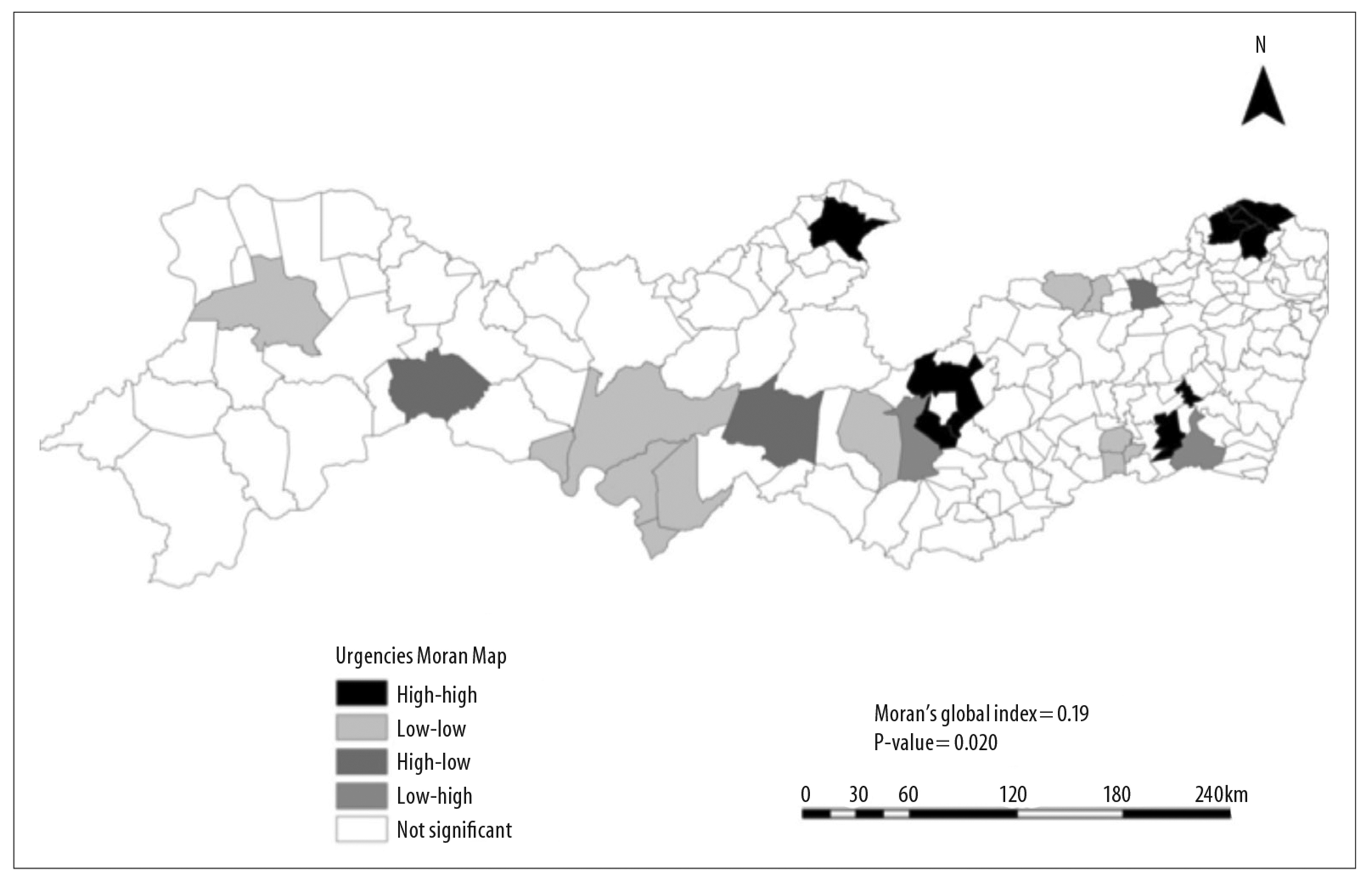
Concerning the test for spatial dependence of dependent variables, only the dental urgency indicator had positive spatial correlation (p=0,020); Moran’s index showed areas of spatial correlation in the Zona da Mata Norte region, with averages that are high for this indicator (positive values, positive averages) and also a hub of municipalities in the Sertão region with lower averages (negative values, negative averages) for the OHt service (Figure 2).
Discussion
With regard to the relationship between oral health indicators and work process, we verified higher medians for the “treatments completed” and “supervised tooth brushing coverage” indicators in municipalities with satisfactory quality standards for oral health care services. Regarding the relationship between the “dental urgency” indicator and the level of organization of the OHt work process, we expected that the closer the practices were to the FHS recommendations, the lower the records of dental urgencies would be. However, we found that the better the standard of work process organization, the higher the averages were for this indicator. The results also showed that in relation to structure, the values of the indicators studied were very close to each other among municipalities with satisfactory, intermediate and unsatisfactory quality standard; the only exception was the “first programmatic dental consultation coverage” indicator, which presented a significantly higher median in municipalities with a satisfactory standard, having a significance level very close to the one considered in this study.
Despite there being no relation between the medians of the “first programmatic dental consultation coverage” indicator and the material resources that served as the analysis unit for building the municipal OHt structure quality standard (facilities, equipment and supplies) in Pernambuco, it is worth mentioning that lack of material and poor equipment maintenance are barriers to service users’ access and impact on the provision of the first dental consultation.13,14
With regard to the “dental urgency” indicator, some studies have pointed to structure shortcomings (shortage of supplies, damaged equipment and few instruments) as being factors preventing clinical care for these urgencies.14,15 However, this conjecture was not endorsed by the results of our research, which did not identify differences between the scores in the quality strata analyzed.
Other studies have associated the performance of supervised collective tooth brushing with structural factors, related to the availability of oral hygiene kits (toothbrush and toothpaste) and to physical spaces for doing supervised brushing (“escovódromo”).16,17 However, our research on the quality standard of service structure did not analyze these aspects. As such, the scenario outlined by this study may explain the absence of differences between scores, since among the aspects examined for the structure dimension, only one item (dental arch macromodel) had a direct relation with collective tooth brushing (information not shown).
Even though we did not find significant differences in the quality strata of the available structure in relation to the “treatments completed” indicator, the literature points to structure shortcomings as being limiting factors for oral health care services, hindering the completion of programmatic dental treatments.18 Moreover, frequent stockouts in public services, in general, not only reduce material resources available for activities but also increase disbelief and, consequently, dental treatment abandonment by the population.15 Such supply failures may possibly have contributed to services being insufficient and ineffective, this being a recurrent aspect of oral health care.
Although the provision of infrastructure-related resources is considered a relevant factor for health service use by the population, this relationship is not clearly established. Service structure conditions may directly impact the OHt working process but, in themselves, do not guarantee increased service use, nor improved quality of services provided.13,14
Regarding the work process, we did not find differences between the strata for the “first programmatic dental consultation coverage” indicator. This result differs from the findings of a study on the organization of oral health care services supply in the Brazilian state of Bahia, where this indicator appeared more for OHt that were closer to what was expected for an FHS work process.14 Some authors support this relationship: a more organized service (with political support, technical planning for its implementation and managers with capacity to govern and control the work process) is associated with more programmatic use of dental procedures provided.19,20 We also highlight that despite the significant expansion of oral health care services availability within FHS, programmatic use of and access to them is still low, due to the reproduction of the biomedical model typical of individual and merely clinical intervention, without taking into consideration psychological, environmental and social influences of the setting.5,21
With regard to the relationship between work process organization and dental urgencies, we found more records of these services in municipalities classified as having a satisfactory oral health care standard, when compared to those with intermediate and unsatisfactory standards. This finding differs from the literature, which generally repeats the following: the further the Oral Health teams are from the FHS care model, the higher the number of urgent consultations. The same studies highlight that to a certain extent the number of urgent consultations reflects the characteristics of service provision.22,23
In the face of this divergence, it is important to consider the high level of unmet user demand for urgency services: most PHUs are not able to attend to all the dental needs of the population in their catchment areas. The combination of underprivileged communities and populations with poor oral health generates more demand for the OHt and, consequently, more urgent consultations.23 It is necessary to discuss the population coverage of each OHt, because the higher the number of people under a team’s responsibility, the greater the probability of this population’s spontaneous demand hindering the organization of the programmed consultation services routine.24 Moreover, sociocultural aspects may influence the frequency of urgent care: many users do not place importance on dental treatment as a way to prevent future problems, they prefer to seek care services when their health condition becomes more critical. This creates a vicious circle, in that the population’s oral health care continues to be precarious and the number of urgent and emergency consultations remains considerable.14
With regard to supervised tooth brushing and the municipal quality standards for the OHT “Work process” dimension, the results reinforce the fundamental importance of the organization of OHt services for this indicator’s behavior, indicating that the health system’s ability to carry out collective actions is closely related to having FHS practices effectively in place.25 In turn, the undervaluing of preventive actions by the OHt may often be a consequence of the priority given to clinical procedures.24 This occurs because institutional structures tailor themselves to the demands of patients and those of the community as a whole, creating a dental care service model that leaves little margin for continuous preventive dental treatment.26 Therefore, despite the significant expansion of OHt throughout the Brazilian territory, oral health care in Brazil is, however, characterized by the insufficiency of collective procedures.22
Regarding the “treatments completed” indicator, there is agreement that factors related to the type of reception adopted in the FHS, the capacity of team professionals to convince users about the importance of completing their treatment, the possibility of community health agents doing active tracing and the guarantee of being able to have further consultations appear to contribute to higher frequency of treatment completion.27 Notwithstanding the difference identified between the medians of this indicator in the strata, we emphasize the problem of continuous and completed dental treatment, which is complex and influenced by various factors, such as low social status, access difficulties, lack of information on oral health, its maintenance and treatment, lack of motivation or fear of treatment, the relationship between the patient and the professional team.28
The spatial analysis found areas of spatial dependence concentrated in the Zona da Mata Norte region, among municipalities categorized as having a satisfactory work process standard. This fact may be explained by increased municipal public expenditure in that region, as indicated by a study on public health expenditure in the state of Pernambuco in the period from 2000 to 2007.29 The good performance of oral health care in this health region has been confirmed by other studies, which found a considerable decrease in the number of tooth extraction procedures in municipal public health services between 2000 and 2008,30 and the improvement of the “first programmatic consultation coverage” indicator in these municipalities, when comparing 2001 data with 2009 data.5 In relation to the high averages of dental urgency identified in this region, even though almost all its municipalities had 100% OHt population coverage, this situation may be related to high unmet demand and low appraisal of completed treatment. Indeed, further studies are needed into the factors that influence such behavior.
In the Sertão region, in turn, the hub of municipalities with lower averages for the “dental urgencies” indicator also requires studies of the conditioning and determinant factors of lower regularity found regarding care for the population of this region. It is important to recall that factors that can influence the frequency of dental urgencies are complex and have to do with organizational and sociocultural issues.23 Notwithstanding the irregularity observed in urgency services - one of the aspects of the organizational dimension - we underline that three out of five municipalities in this hub in the Sertão region in Pernambuco achieved total OHt population coverage in 2014 (data not shown).
Furthermore, it is appropriate to point out the importance of knowledge on the behavior of the variables studied in this territory, in the sense of understanding health events and planning actions capable of intervening positively in the health-illness process.12 Nevertheless, the very complexity of factors influencing the performance of these variables indicates the need for new studies with the objective of explaining patterns of spatial distribution found in our study.
Regarding the limitations of this research, caution is needed as to the reliability of records used as indicators of dental care services use, besides possible OHt misrepresentation of reality during the PMAQ-AB external evaluation. It is possible, however, that the results presented may encourage reflection on OHt care and work processes.
We conclude that in Pernambuco, the municipalities’ standard of quality for the “Structure” dimension of oral health care services had better scores than the “Work process” dimension, according to the National Primary Health Care Access and Quality Improvement Program (PMAQ-AB) criteria adopted in 2014. We identified differences between the “dental urgency”, “supervised tooth brushing coverage” and “treatments completed” indicators, in the quality strata related to the Oral Health care teams’ work processes. Their organization may be a determining factor for the quality of the services provided by Oral Health care teams in Pernambuco.
REFERENCES
1. Fausto MCR, Giovanella L, Mendonça MHM, Seidl H, Gagno J. A posição da Estratégia Saúde da Família na rede de atenção à saúde na perspectiva das equipes e usuários participantes do PMAQ-AB. Saúde Debate [Internet]. 2014 out [citado 2019 abr 18];38(esp):13-33. Disponível em: Disponível em: http://www.scielo.br/pdf/sdeb/v38nspe/0103-1104-sdeb-38-spe-0013.pdf . doi: 10.5935/0103-1104.2014S003 [ Links ]
2. Pimentel FC, Albuquerque PC, Souza WV. A estratégia saúde da família no estado de Pernambuco: avaliação da estrutura das equipes por porte populacional. Saúde Debate [Internet]. 2015 jan-mar [citado 2019 abr 18];39(104):88-101. Disponível em: Disponível em: http://www.scielo.br/pdf/sdeb/v39n104/0103-1104-sdeb-39-104-00088.pdf . doi: 10.1590/0103-110420151040138 [ Links ]
3. Moraes PN, Iguti AM. Avaliação do desempenho do trabalhador como forma peculiar de prescrição do trabalho: uma análise do PMAQ-AB. Saúde Debate [Internet]. 2013 jul-set [citado 2019 abr 18];37(98):416-26. Disponível em: Disponível em: http://www.scielo.br/pdf/sdeb/v37n98/a05v37n98.pdf . doi: 10.1590/S0103-11042013000300005 [ Links ]
4. Silva SF, Martelli PJL, Sá DA, Cabral AP, Pimentel FC, Monteiro IS, et al. Análise do avanço das equipes de saúde bucal inseridas na estratégia saúde da família em Pernambuco, região Nordeste, Brasil, 2002 a 2005. Ciênc Saúde Coletiva [Internet]. 2011 jan [citado 2019 abr 18];1(16):211-20. Disponível em: doi: 10.1590/S1413-81232011000100024 [ Links ]
5. Viana IB, Martelli PJL, Pimentel FC. Análise do acesso aos serviços odontológicos através do indicador de primeira consulta odontológica programática em Pernambuco: estudo comparativo entre os anos 2001 e 2009. Rev Bras Promoç Saúde [Internet]. 2012 abr-jun [citado 2019 abr 18];25(2)151-60. Disponível em: Disponível em: http://www.redalyc.org/pdf/408/40823359004.pdf [ Links ]
6. Aquilante AG, Aciole GG. O cuidado em saúde bucal após a Política Nacional de Saúde Bucal - ‘Brasil Sorridente’: um estudo de caso. Ciênc Saúde Colet [Internet]. 2015 jan [citado 2019 abr 18];20(1):239-48. Disponível em: Disponível em: http://www.scielo.br/pdf/csc/v20n1/pt_1413-8123-csc-20-01-00239.pdf [ Links ]
7. Donabedian A. The quality of care. How can it be assessed? JAMA [Internet]. 1988 Sep [cited 2019 Apr 18];260(12):1743-8. Disponível em: Disponível em: https://jamanetwork.com/journals/jama/article-abstract/374139 . doi: 10.1001/jama.1988.03410120089033 [ Links ]
8. Silva LMV, Formigli VLA. Avaliação em saúde: limites e perspectivas. Cad Saúde Pública [Internet]. 1994 jan-mar [citado 2019 abr 18];10(1):80-91. Disponível em: Disponível em: http://www.scielo.br/pdf/csp/v10n1/v10n1a09.pdf . doi: 10.1590/S0102-311X1994000100009 [ Links ]
9. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Programa nacional de melhoria do acesso e da qualidade da atenção básica (PMAQ): manual instrutivo [Internet]. Brasília: Ministério da Saúde; 2013 [citado 2019 abr 18]. 128 p. Disponível em: Disponível em: http://189.28.128.100/dab/docs/portaldab/documentos/instrumento_ae_sfp.pdf [ Links ]
10. Ministério da Saúde (BR). Departamento de Informática do Sistema Único de Saúde. Sistema de Informações ambulatoriais do Sistema Único de Saúde (SIA-SUS). Produção ambulatorial do SUS - Pernambuco - por local de atendimento - 2014 [Internet]. Brasília: Ministério da Saúde ; 2014 [citado 2019 abr 18]. Disponível em: Disponível em: http://www2.datasus.gov.br/DATASUS/index.php?area=0202&id=19122&VObj=http://tabnet.datasus.gov.br/cgi/deftohtm.exe?sia/cnv/qa [ Links ]
11. Ministério da Saúde (BR). Departamento de Informática do Sistema Único de Saúde. Informações de saúde. Demográficas e socioeconômicas. Estimativas população - Pernambuco - 2014 [Internet]. Brasília: Ministério da Saúde ; 2014 [citado 2019 abr 18]. Disponível em: Disponível em: http://www2.datasus.gov.br/DATASUS/index.php?area=0206&id=6942 [ Links ]
12. Carvalho MS, Souza-Santos R. Análise de dados espaciais em saúde pública: métodos, problemas, perspectivas. Cad Saúde Pública [Internet]. 2005 mar-abr [citado 2019 abr 18];21(2):361-78. Diponível em: Diponível em: http://www.scielo.br/pdf/csp/v21n2/03.pdf . doi: 10.1590/S0102-311X2005000200003 [ Links ]
13. Viegas APB, Carmo RF, Luz ZMP. Fatores que influenciam o acesso aos serviços de saúde na visão de profissionais e usuários de uma unidade básica de referência. Saúde Soc [Internet]. 2015 abr-jun [citado 2019 abr 18];24(1):100-12. Disponível em: Disponível em: http://www.scielo.br/pdf/sausoc/v24n1/0104-1290-sausoc-24-1-0100.pdf . doi: 10.1590/S0104-12902015000100008 [ Links ]
14. Tavares RP, Costa GC, Falcão MLM, Cristino PS. A organização do acesso aos serviços de saúde bucal na estratégia de saúde da família de um município da Bahia. Saúde Debate [Internet]. 2013 out-dez [citado 2019 abr 18];37(99):628-35. Disponível em: Disponível em: http://www.scielo.br/pdf/sdeb/v37n99/a10v37n99.pdf . doi: 10.1590/S0103-11042013000400010 [ Links ]
15. Mendes Júnior FIR, Bandeira MAM, Tajra FS. Percepção dos profissionais quanto à pertinência dos indicadores de saúde bucal em uma metrópole do Nordeste brasileiro. Saúde Debate [Internet]. 2015 jan-mar [citado 2019 abr 18];39(104):147-58. Disponível em: Disponível em: http://www.scielo.br/pdf/sdeb/v39n104/0103-1104-sdeb-39-104-00147.pdf . doi: 10.1590/0103-110420151040205 [ Links ]
16. Cruz LMFS, Caldas AFJ. Características da organização da política de saúde bucal na atenção primária de municípios de Pernambuco. In: Memorias Convención Internacional de Salud Pública; 2012 dez; Habana, Cuba [Internet]. Cuba: eCIMED; 2012 [citado 2017 abr 03]. Disponível em: Disponível em: http://actasdecongreso.sld.cu/index.php?P=FullRecord&ID=1398 [ Links ]
17. Araújo PC, Garbín CAS, Moimaz SAS, Saliba NA, Reatto D, Arcieri RM. Evaluación comparativa del conocimiento sobre salud oral entre equipos pedagógicos que recibieron y no recibieron promoción en salud. Int J Odontostomat [Internet]. 2017 jun [citado 2019 abr 18];11(2):198-206. Disponível em: Disponível em: https://scielo.conicyt.cl/pdf/ijodontos/v11n2/art13.pdf . doi: 10.4067/S0718-381X2017000200013 [ Links ]
18. Matos PES. Análise da atenção em saúde bucal no Brasil sob a ótica do Sistema de Informação da Atenção Básica [tese]. São Paulo (SP): Universidade de São Paulo; 2014. Disponível em: http://www.teses.usp.br/teses/disponiveis/25/25144/tde-10102014-144648/pt-br.php. doi: 10.11606/T.25.2014.tde-10102014-144648 [ Links ]
19. Chaves SCL, Cruz DN, Barros SG, Figueiredo AL. Avaliação da oferta e utilização de especialidades odontológicas em serviços públicos de atenção secundária na Bahia. Cad Saúde Pública [Internet]. 2011 jan [citado 2019 abr 18];27(1):143-54. Disponível em: Disponível em: http://www.scielo.br/pdf/csp/v27n1/15.pdf . doi: 10.1590/S0102-311X2011000100015 [ Links ]
20. Rossi TRA, Chaves SCL. Implementação da atenção especializada em saúde bucal em dois municípios na Bahia/Brasil. Saúde Debate [Internet]. 2015 dez [citado 2019 abr 18];39(esp):196-206. Disponível em: Disponível em: http://www.scielo.br/pdf/sdeb/v39nspe/0103-1104-sdeb-39-spe-00196.pdf . doi: 10.5935/0103-1104.2015S005186 [ Links ]
21. Bulgareli J, Cortellazzi KL, Ambrosano GMB, Meneghim MC, Faria ET, Mialhe FL, et al. A resolutividade em saúde bucal na atenção básica como instrumento para avaliação dos modelos de atenção. Ciênc Saúde Coletiva [Internet]. 2014 fev [citado 2019 abr 18];19(2):383-91. Disponível em: Disponível em: http://www.scielo.br/pdf/csc/v19n2/1413-8123-csc-19-02-00383.pdf . doi: 10.1590/1413-81232014192.20102012 [ Links ]
22. Soares SS, Lima LD, Castro ALB. O papel da atenção básica no atendimento às urgências: um olhar sobre as políticas. J Manag Prim Health Care [Internet]. 2014 jun [citado 2019 abr 18];5(2):170-77. Disponível em: Disponível em: http://www.jmphc.com.br/jmphc/article/download/213/216/ [ Links ]
23. Magri LV, Aciole GG, Salomão FGD, Tagliaferro EPS, Ribeiro LG. Estudo comparativo de indicadores de saúde bucal em município do estado de São Paulo. Saúde Debate [Internet]. 2014 jan-mar [citado 2019 abr 18];40(108):144-55. Disponível em: Disponível em: http://www.scielo.br/pdf/sdeb/v40n108/0103-1104-sdeb-40-108-00144.pdf . doi: 10.1590/0103-1104-20161080012 [ Links ]
24. Pimentel FC, Albuquerque PC, Martelli PJL, Acioli RML, Souza WV. Análise dos indicadores de saúde bucal do Estado de Pernambuco: desempenho dos municípios segundo porte populacional, população cadastrada no sistema de informação da atenção básica e proporção na estratégia saúde da família. Cad Saúde Colet [Internet]. 2014 mar [citado 2019 abr 18];22(1):54-61. Disponível em: Disponível em: http://www.scielo.br/pdf/cadsc/v22n1/1414-462X-cadsc-22-01-00054.pdf . doi: 10.1590/1414-462X201400010009 [ Links ]
25. Faccin D, Sebold R, Carcereri DL. Processo de trabalho em saúde bucal: em busca de diferentes olhares para compreender e transformar a realidade. Ciênc Saúde Coletiva [Internet]. 2010 jun [citado 2019 abr 18];15(Supl.1):1643-52. Disponível em: Disponível em: http://www.scielo.br/pdf/csc/v15s1/076.pdf . doi: 10.1590/S1413-81232010000700076 [ Links ]
26. Harris RV. Do 'poor areas' get the services they deserve? The role of dental services in structural inequalities in oral health. Community Dent Health [Internet]. 2016 Jun [cited 2019 Apr 18];33(2):164-67. Disponível em: Disponível em: https://www.cdhjournal.org/issues/33-2-june-2016/708-do-poor-areas-get-the-services-they-deserve-the-role-of-dental-services-in-structural-inequalities-in-oral-health?downloadarticle=download . doi: 10.1922/CDH_3718-Harris04 [ Links ]
27. Thurow LE, Castilhos ED, Costa JSD. Comparação das práticas odontológicas segundo modelos de atendimento: tradicional e da Saúde da Família, Pelotas, RS, 2012-2013. Epidemiol Serv Saúde [Internet]. 2015 jul-set [citado 2019 abr 18];24(3):545-50. Disponível em: Disponível em: http://www.scielo.br/pdf/ress/v24n3/2237-9622-ress-24-03-00545.pdf . doi: 10.5123/S1679-49742015000300021 [ Links ]
28. Scaramuzzi PBM. Estímulo à continuidade do tratamento odontológico na Policlínica Odontológica Santa Emília - Mario G. da C. Lima na Rede Municipal de Saúde de Campo Grande/MS [monografia]. Campo Grande (MS): Universidade Federal de Mato Grosso do Sul; 2011. Disponível em: https://ares.unasus.gov.br/acervo/handle/ARES/3463 [ Links ]
29. Santo ACE, Fernando VCN, Bezerra AFB. Despesa pública municipal com saúde em Pernambuco, Brasil, de 2000 a 2007. Ciênc Saúde Coletiva [Internet]. 2012 abr [citado 2019 abr 18];17(4):861-71. Disponível em: Disponível em: http://www.scielo.br/pdf/csc/v17n4/v17n4a09.pdf . doi: 10.1590/S1413-81232012000400009 [ Links ]
30. Correia Júnior WLM. Estudo sobre procedimentos exodônticos na rede assistencial pública do Estado de Pernambuco, no período de 2000 a 2008 [monografia]. Recife (PE): Centro de Pesquisa Aggeu Magalhães/Fundação Instituto Oswaldo Cruz; 2012. Disponível em: http://www.cpqam.fiocruz.br/bibpdf/2012correia-junior-wlm.pdf [ Links ]
Received: May 03, 2018; Accepted: April 03, 2019
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
