










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.28 no.3 Brasília set. 2019 Epub 14-Ago-2019
http://dx.doi.org/10.5123/s1679-49742019000300001
ORIGINAL ARTICLE
Spatial analysis of avoidable infant deaths in Espírito Santo, Brazil, 2006-2013*
1Escola Nacional de Saúde Pública Sergio Arouca, Programa de Pós-graduação em Epidemiologia em Saúde Pública, Rio de Janeiro, RJ, Brasil
2Universidade Federal do Espírito Santo, Departamento de Medicina Social, Vitória, ES, Brasil
3Universidade Federal do Espírito Santo, Departamento de Estatística, Vitória, ES, Brasil
Objective:
to analyze spatial distribution of avoidable infant deaths in Espírito Santo state, Brazil, 2006-2013.
Methods:
this was an ecological study of infant deaths recorded on the Mortality Information System and classified according to the method used by the International Collaborative Effort on Perinatal and Infant Mortality (ICE). Avoidable death rates were calculated and smoothed by global and local Bayesian estimators. Local Moran’s Index was used to verify local spatial correlation.
Results:
of the 5,089 deaths, 4,805 were classified as per ICE, 77.2% of which were avoidable. The crude mean rate was 9.68/1.000 live births, reducing to 8.96/1.000 live births after applying the global Bayesian estimator. The municipality of Jerônimo Monteiro had the highest rate (20.1/1.000 live births). The Local Moran’s Index showed weak spatial correlation of 0.197 (p-value=0.02).
Conclusion:
there were clusters of municipalities in the Central and Southern regions of the state, suggesting the need for adequate monitoring in these areas where there is a higher risk of avoidable deaths.
Keywords: Infant Mortality; Cause of Death; Epidemiology, Descriptive; Spatial Analysis
Introduction
Infant mortality represents the living and health conditions of a given population.1 According to Ministry of Health estimates,2 in 2000 Brazil’s infant mortality rate (IMR) was 26.1/1.000 live births, while in 2015 it had reduced to 12.4/1.000. Espírito Santo state had an IMR of 18.1/ live births in 2000, while in 2015 its IMR became Brazil’s lowest at 9.2 deaths/1.000 live births.3
This significant decline in infant mortality is due, above all, to improvements in the living conditions of the population, including expansion of the water supply network, increase in the level of schooling and reduction in fertility rates, as well as the adoption of public policies targeting specific actions, such as vaccination campaigns, breastfeeding programs, the introduction of rotavirus vaccine and oral rehydration therapy in Primary Health Care.4
However, despite its considerable fall over the years, in 2016, Brazil’s IMR increased for the first time since 1990.2 This suggests that infant deaths remain high even though the majority of them can be considered avoidable in view of technological progress and existing knowledge, which allow for effective interventions to tackle its causes.5 In this sense, with effect from 1950, internationally several systems of infant death classification were proposed intended to reflect possible causes of infant mortality, such as the Taucher6 and Wigglesworth7,8 methods and the International Collaborative Effort (ICE) on Infant Mortality.9 In Brazil the following classifications have been proposed: the State Data Analysis System - (SEADE)10 and the List of Causes of Death Avoidable by Brazilian National Health System Interventions.11
The objective of these preventability classifications is to reduce deaths and obtain a reliable assessment of the effectiveness of health care services for pregnant women and newborns, even in the face of their different criteria for classifying avoidable and non-avoidable deaths.12 However, classifying deaths in this way is subject to the limitations of death certificate information,13 which, in turn, is a complicating factor.
As such, it is essential to investigate causes of death in order to decide as to their preventability. This is the role of the health professionals who do death surveillance in the municipality in which the mother is resident. At the end of the investigation of cause of death, the monitoring team should encourage discussions with other professionals involved in child care, with the aim of examining the case, and then conclude on the preventability of the death so as to prevent future deaths from similar causes.14 In addition, the Infant and Fetal Death Prevention Committees are a strategy for improving health care, reducing avoidable deaths, as well improving mortality records.14
Despite these efforts aimed at preventing infant death, there is a need to analyze the geographic distribution of this phenomenon, given its relationship with territorial inequalities. In addition, spatial analysis has been an important method for epidemiological health studies in order to highlight areas of greatest risk of diseases and deaths.15,16
In view of the above, the objective of this study was to analyze spatial distribution of avoidable infant deaths in Espírito Santo state, Brazil, from 2006 to 2013.
Methods
This is an ecological study of infant deaths in Espírito Santo state between 2006 and 2013, according to the municipality of mother’s residence. Espírito Santo state is comprised of 78 municipalities in an area equivalent to 46,096.925 km². Its capital city is Vitória. In 2010, the state had 3,514,952 inhabitants and gross domestic product (GDP) per capita of 0.558 and a Gini index of 0.4928.3
The period from 2006 to 2013 was selected for this study due to data availability. All deaths of children under one year old recorded on the Mortality Information System (SIM) were included in the study. We excluded deaths that occurred in the gestational period below 22 weeks and weighing less than 500 grams. In addition to this we used the SIM database provided by the Espírito Santo State Health Department (SESA-ES) to retrieve underlying cause of death, variables of interest and also to calculate mortality rates. We also used the Brazilian Life Birth Information System (SINASC) to calculate avoidable death rates.
Initially, the underlying causes of deaths coded according to the 10th Revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10), were classified as avoidable or non-avoidable, according to the ICE preventability method9 since this method had greater capacity for distinguishing between avoidable and non-avoidable causes of death.12 This method proposed eight groupings of causes of avoidable infant deaths, namely: congenital; suffocation; immaturity; infection; sudden infant death syndrome (SIDS); external causes; specific conditions; and other causes.9 All causes of infant deaths were then classified as avoidable or non-avoidable according to these groups. More information on ICE can be found in a previous publication.12
After classification of infant deaths as avoidable or non-avoidable, we estimated absolute and relative frequencies for the following variables of interest: year of occurrence of infant death; type of death (neonatal or postneonatal mortality); the child's sex; ethnicity/skin color (white, black, brown, Asian, indigenous); type of delivery (vaginal, cesarean section); child's weight at birth (500-2,499g, 2,500-2,999g, 3,000-3999g, ≥4000g); and municipality of residence of the mother.
Sequentially, the avoidable death rates were calculated by summing the avoidable deaths that occurred over the years by municipality, divided by the sum of live births per municipality in the same period, multiplied by 1,000.
For the spatial analysis of the data we applied the global and local Bayesian estimators, with the objective of correcting the avoidable infant death rates. These are known as methods of spatial smoothing, since they are useful for avoiding random fluctuations that can result in false interpretations. Therefore, comparing the rates between the municipalities using these two methods was important to understand the behavior of the avoidable death rates. While the Global Empirical Bayesian estimator (GEBayes) seeks an approximation of the average rate for all municipalities, the Local Empirical Bayesian estimator (LEBayes) works with mean incidence found in municipality neighborhoods, given that neighboring regions tend to have rates that are more similar than those of regions distant from each other.17
The local empirical Bayes estimator is a rate adjusted as follows:
In the equation, wi is the weight between 0 and 1, which depends on the size of the population in area i, ti is the risk rate in the area and m is the overall rate for Espírito Santo state. The larger the population in area i, the closer weight wi, which means that in areas where the population is greater, the empirical Bayes estimate is very close to ti. In areas with a small population, the value of bi will be intermediary between ti and m.17
The Local Moran Index was also calculated to verify whether distribution of avoidable infant death rates in space occurs randomly or follows a pattern of occurrence. For this reason, a significance level of 5% was considered when areas were delimited in which there were local spatial structures influencing these rates.18
The result of this index varies from -1 to +1, i.e., positive values indicate spatial dependence, while negative values indicate inverse correlation. Furthermore, when the value is close to 0 this indicates lack of spatial correlation in the data.18
The calculations to determine preventability of infant deaths were performed using Microsoft Excel, version 2010. We used the SIRGAS 2000 reference system (GRS80 ellipsoid geographic coordinates projection system) for information georeferencing and performance of spatial analysis, together with the Espírito Santo state 2010 digital mesh, provided by the Brazilian Institute of Geography and Statistics (IBGE). All analysis was performed using TerraView, version 4.2.2.
The study was submitted to the Federal University of Espírito Santo (UFES) Health Sciences Center Research Ethics Committee and was approved on 25 March 2015, Opinion No. 999.562. In addition, formal authorization was obtained to use SESA-ES data on the condition that the confidentiality of the information of the subjects listed in the database would be guaranteed.
Results
In the period from 2006 to 2013, there were 5,089 deaths among children younger than 1 year old; of these, 4,805 deaths were classified according to the ICE method as being avoidable (77.2%) or non-avoidable (22.8%). We found a reduction in avoidable deaths from 28.7% between 2006 and 2007, to 22.9% between 2012 and 2013 (Table 1).
Table 1 - Characteristics of infant death preventabilitya, Espírito Santo, 2006-2013
| Variables | Non-avoidable n (%) | Avoidable n (%) | Sampleb n (%) |
|---|---|---|---|
| Year of Death | |||
| 2006-2007 | 307 (28.0) | 1,066 (28.7) | 1,373 (28.6) |
| 2008-2009 | 290 (26.5) | 949 (25.6) | 1,239 (25.8) |
| 2010-2011 | 290 (26.5) | 844 (22.7) | 1,134 (23.6) |
| 2012-2013 | 208 (19.0) | 851 (22.9) | 1,059 (22.0) |
| Type of death | |||
| Neonatal | 831 (75.9) | 2,587 (69.7) | 3,418 (71.1) |
| postneonatal | 264 (24.1) | 1,123 (30.3) | 1,387 (28.9) |
| Sex | |||
| Male | 574 (53.3) | 2,093 (57.0) | 2,667 (56.2) |
| Female | 503 (46.7) | 1,578 (43.0) | 2,081 (43.8) |
| Ethnicity/skin color | |||
| White | 382 (43.2) | 1,271 (43.0) | 1,653 (43.1) |
| Black | 25 (2.8) | 97 (3.3) | 122 (3.2) |
| Brown | 467 (53.8) | 1,578 (53.5) | 2,045 (53.3) |
| Asian | 4 (0.4) | 0 (0.0) | 4 (0.1) |
| Indigenous | 6 (0.7) | 5 (0.2) | 11 (0.3) |
| Type of delivery | |||
| Vaginal | 389 (42.9) | 1,469 (47.4) | 1,858 (46.4) |
| Cesarean | 518 (57.1) | 1,627 (52.6) | 2,145 (53.6) |
| Weight ranges | |||
| <2,500g | 615 (69.3) | 1,925 (63.8) | 2,540 (65.0) |
| 2,500-2,999g | 128 (14.4) | 381 (12.6) | 509 (13.0) |
| 3,000-3,999g | 129 (14.5) | 628 (20.8) | 757 (19.5) |
| <4,000g | 16 (1.8) | 83 (2.8) | 99 (2.5) |
a) According to classification by the International Colaborative Effort (ICE) method.
b) Differences in the total sample due to missing data.
Avoidable infant death distribution occurred with greater frequency in the neonatal period (69.7%). In relation to individual characteristics, males (57%) and brown ethnicity/skin color (53.6%) were predominant. Cesarean delivery (52.6%) stood out as the most frequent type of child delivery among these deaths and the majority of deaths occurred in the under 2,500 gram weight range (63.8%) (Table 1).
With regard to infant death preventability rates, out of the 78 municipalities of Espírito Santo state, we found that João Neiva had the lowest rate (4.40 avoidable deaths/1,000 live births), while Jerome Monteiro had the highest rate (20.10 avoidable deaths/1,000 live births).
The crude mean avoidable death rate was 9.68/1,000 live births. However, the rate reduced to 8.96/1,000 live births, when corrected using the smoothing methods (Table 2).
Table 2 - Descriptive statistics of crude and estimated avoidable infant death rates per 1,000 live births, Espírito Santo, 2006-2013
| Crude ratea | LEBayesb | GEBayesc | |
|---|---|---|---|
| Average | 9.68 | 9.52 | 8.96 |
| Median | 8.94 | 9.36 | 8.90 |
| Standard-deviation | 2.63 | 1.20 | 0.44 |
| Minimum | 4.43 | 7.04 | 7.98 |
| Maximum | 20.10 | 12.27 | 10.16 |
a) Crude avoidable infant death rate/1,000 live births.
b) LEBayes: Local Empirical Bayesian estimator - average incidence found in municipal neighborhoods, using a spatial effect.
c) GEBayes: Global Empirical Bayesian estimator - Weighted average between the crude rate for the specific location and the overall rate of the region.
Among the 78 municipalities forming Espírito Santo state, we found that the rate for 19 of them was less than 8 avoidable deaths/1,000 live births. In contrast, 21 municipalities had crude avoidable death rates of between 11.00 and 20.10 avoidable deaths/1,000 live births (Figure 1A).
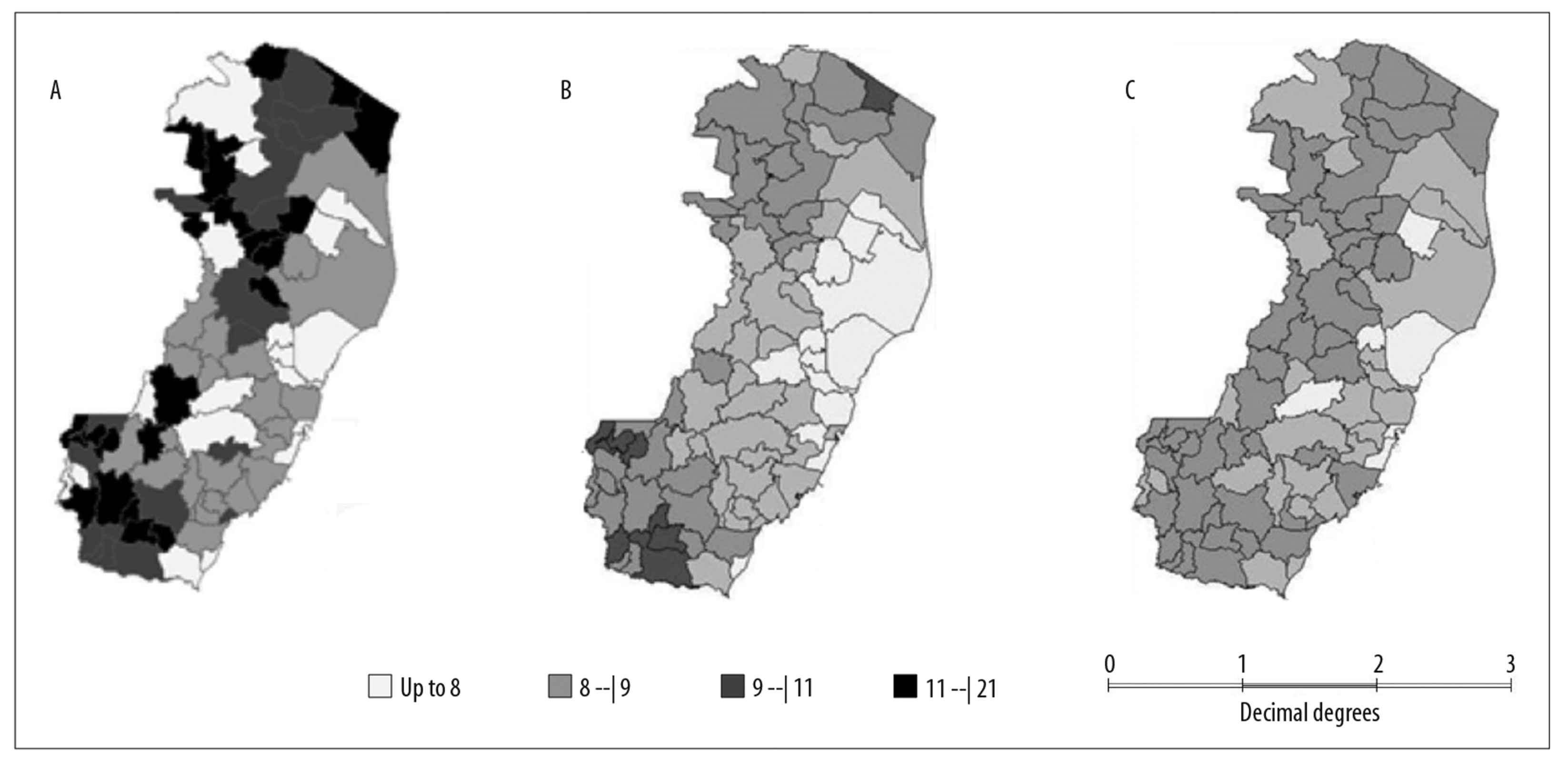
Legend:
A = Gross avoidable death rate.
B = Local Empirical Bayesian Estimator (LEBayes).
C = Global Empirical Bayesian Estimator (GEBayes).
Figure 1 - Distribution of avoidable infant death rates, per 1,000 live birth, Espírito Santo, 2006-2013
Crude rates were found to have smoothed after LEBayes calculation, indicating that the effect of random fluctuations had been smoothed. Following smoothing, only nine of the municipalities that previously had rates of between 11.00 and 20.10 avoidable deaths/1,000 live births continued in this range (Figure 1B). GEBayes was found to follow the same pattern, although it reduced the effect of random fluctuations even more, so that none of the municipalities continued to have rates between 11.00 and 20.10 avoidable deaths/1,000 live births (Figure 1C).
Figure 2 shows the dispersion graphs for the spatial smoothing methods. Discrepant values were found between avoidable death rates in some municipalities. Using LEBayes, the rates for the municipalities of João Neiva, Vila Pavão and Dores do Rio Preto reduced. In contrast, the rates increased in the municipalities of Atílio Vivacqua and Jeronimo Monteiro when using both LEBayes and GEBayes. In both figures, municipality dispersion can be seen in relation to the regression line.
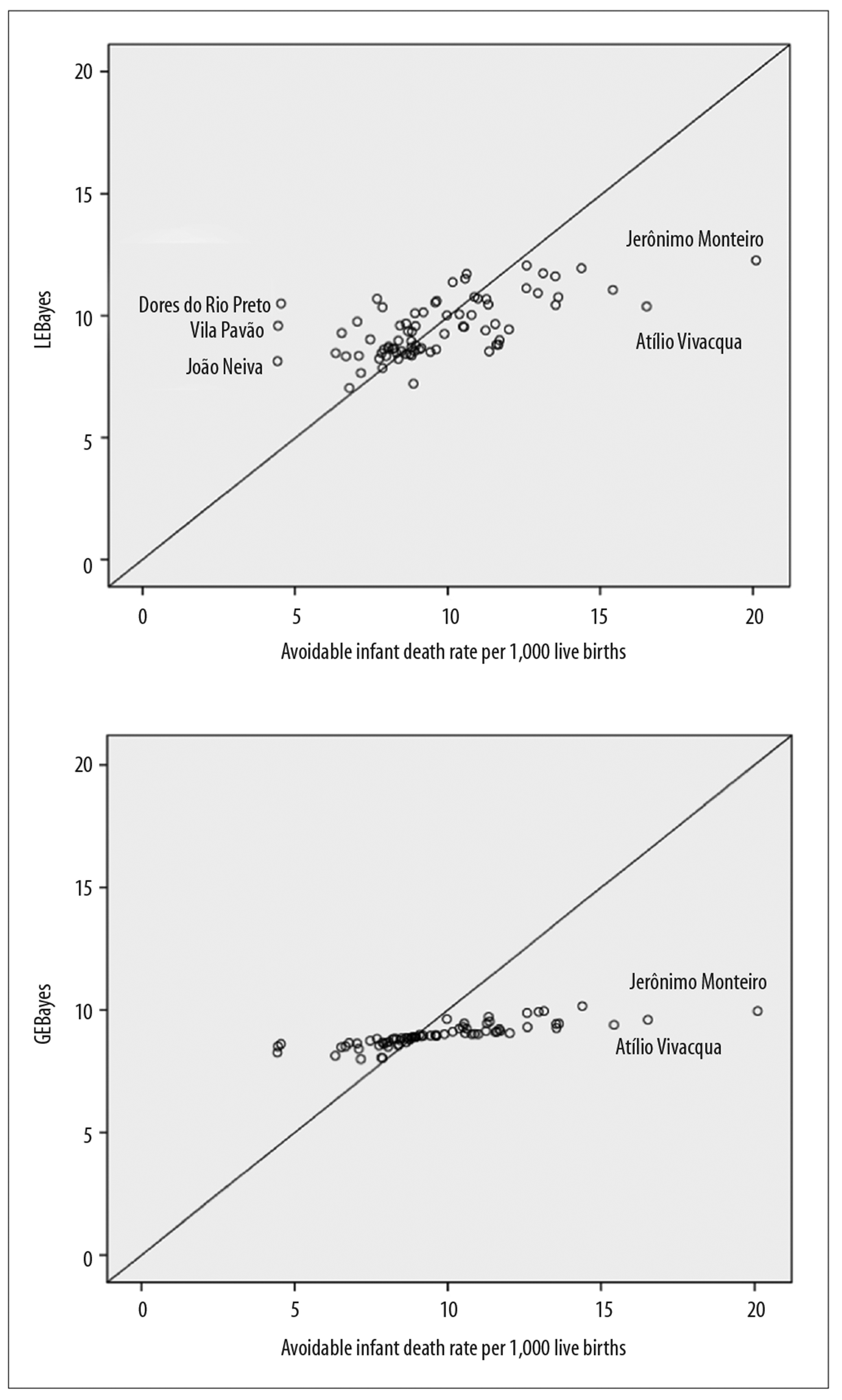
Figure 2 - Dispersion graph of crude avoidable infant death rates corrected by Local Empirical Bayesian Estimator (LEBayes) and by Global Empirical Bayesian Estimator (GEBayes), Espírito Santo, 2006-2013
In addition, spatial autocorrelation calculated using the Local Moran Index (LISA) was 0.197 (p = 0.02), thus indicating the existence of significant spatial correlation between avoidable deaths, although the correlation for Espírito Santo state as a whole was weak. However, this method found a geographic conglomeration of municipalities in the central region of the state, including the municipalities of Aracruz, Ibiraçu, Santa Teresa, with a significance level lower than 0.10%; whereas in São Roque do Canaã, Santa Leopoldina and Afonso Claudio, the significance level was less than 5% in the spatial correlation. Another conglomeration of municipalities stood out southern region of the state, involving the municipalities of Mimoso do Sul, Muqui and Cachoeiro do Itapemirim (p<0.001) and Alegre (p< 0.05).
Discussion
The analysis of the spatial distribution of avoidable infant deaths occurring in Espírito Santo from 2006 to 2013, showed that the majority of the state’s municipalities (75%) had avoidable infant mortality rates of less than 12/1,000 live births. The distribution of these rates at the local level predominated in the southern region of the state, similarly to what occurred with global distribution although the latter had less intensity in geographic space.
Studies conducted in the Southern19 and Northeastern20 regions of Brazil also found high percentages of avoidable infant deaths - 76.4% and 76%, respectively. This reinforces the extent to which avoidable deaths still remain high in Brazil, although their distribution differs according to the region of the country.
It is important to emphasize that avoidable infant deaths result from shortcomings in health services or health care, and can be understood as events that should not occur, given the technologies available for health care. As such, they are referred to as sentinel events, since they are important for evaluating the quality of maternal and child health care.5
This study initially found an average crude coefficient of 9.68 avoidable deaths/1,000 live births. However, after the smoothing methods (GEBayes), this coefficient became 8.96 for avoidable deaths/1,000 live births, ranging between 7.98/1,000 live births to 10.16/1,000 live births, in the period analyzed. For Brazil as a whole, Boing and Boing21 found an average of 11.28 avoidable deaths/1,000 live births. In turn, Nascimento et al.20 identified a mean coefficient of 10.30/1,000 live births, although this was in relation to avoidable neonatal mortality.
It is noteworthy that the coefficient smoothing used in this study enabled more reliable maps to be produced, since it is a process that reduces the influence of random fluctuation of measurements22 and allows better estimation of avoidable infant death coefficients. As a consequence, it also enables identification of high-risk areas for the occurrence of these deaths.
As such, mapping of avoidable infant deaths showed that areas further from urban city centers and with greater lack of services had the highest rates of avoidable mortality. This could possibly indicate imbalance between availability of health services and investments in them. When analyzing geographic access to childbirth facilities in Brazilian municipalities, Almeida and Szwarcwald23 identified that the greater the geographic distance from hospitalization for childbirth, the greater the infant mortality coefficients.
Despite expansion of primary care and increased coverage of prenatal care in remote areas, this phenomenon suggests an unequal distribution of health services in Espírito Santo, even though this geographic inequality is not excessively discrepant. Therefore, the distance of these areas in relation to health services, which are concentrated in the metropolitan region of Vitória, especially high complexity services, points to possible deficiencies in services specialized in the immediate care of the newborn, this being a fundamental element for survival of children younger than 1 year old. This fact corroborates with previous studies conducted in other Brazilian states, which pointed to intraregional inequality as evidenced by the large flow of pregnant women to municipalities located in urban areas with better levels of socioeconomic development.24,25,26
This scenario is worrying, given that in Brazil there is a large proportion of health establishments without the minimum required equipment or specialized professionals for providing emergency care for perinatal women and the newborn.24 This may further increase infant death rates. A study of death preventability classification conducted in Espírito Santo found that a large proportion of avoidable infant deaths occurred due to causes related to immaturity,12 which may be related to failures in obstetric management and/or deficiencies in care for newborns in the state’s Neonatal Intensive Care Units.
Avoidable death rates remain high throughout Brazil. This may be related to the high frequency of avoidable neonatal deaths, which in turn are responsible for the continuing high infant mortality coefficients, given its relationship with conditions during pregnancy and childbirth.
Despite the limitations inherent to this study, especially those related to the detailing of causes of death, the results presented here underline that deaths from avoidable causes are occurring above all owing to low quality health care provided to women and their babies during the prenatal, labor, birth and puerperium periods, given that the ICE classification takes into account causes of death resulting from these periods.12
This study also identified significant spatial correlation between avoidable deaths, although correlation was weak in the context of the state as a whole. This indicates that neighboring regions tend to have rates that are more similar in relation to each other when compared to those of more distant areas, as well as sharing similar demographic and socioeconomic characteristics.27 It is known that the infant mortality rate is linked to social inequalities and that therefore the most vulnerable populations have greater difficulty in accessing health services.
The influence of social and organizational characteristics of the context determines the occurrence of avoidable infant deaths. When analyzing spatial distribution of infant mortality in Espírito Santo, Lapa et al.28 found that socioeconomic status and sewage disposal are factors inherent to the risk of dying. As such, the infant mortality rate is strongly linked to social inequalities, i.e., it is the most vulnerable populations who have greater difficulty in accessing health services.1,21,25,29 However, when avoidable death rates are analyzed, the refined methods used only indicate deaths that could be prevented through intervention.
In order to understand mortality patterns and distribution in time and space, geographic information systems and spatial location are becoming essential public health tools, especially for the spatial representation of events.30 In this sense, the findings of our study reveal that the incorporation of spatial analysis methods enables detection of risk areas and situations, which could ensure the redirection of public policies and interventions targeting priority population groups.
It should be noted that this study also has some limitations, since the data source has flaws with regard to the filling out of death certificates and this can compromise the results of analysis at the local level. However, this does not invalidate the results obtained given the size of the sample used in the study period. In addition, the time period selected (8 years) was sufficient for the analysis proposed by this study, since infant death in small populations - as is the case of Espírito Santo’s municipalities - is an event which occurs in small proportions and can, therefore, generate great variability when the rates are calculated.17,18
In conclusion, differences were found in the rates of avoidable infant deaths between municipalities of Espírito Santo state. This points to the need to develop adequate monitoring in areas with higher risk of death, as well as to improve the integration of primary care actions and enhance the municipal system model of maternal and child care. In addition, this study leads to reflection on the need to improve the living conditions of the population, given that socioeconomic factors are determinants of the occurrence of child deaths from avoidable causes.
REFERENCES
1. França EB, Lansky S, Rego MAS, Malta DC, França JS, Teixeira R, et al. Principais causas da mortalidade na infância no Brasil, em 1990 e 2015: estimativas do estudo de Carga Global de Doença. Rev Bras Epidemiol [Internet]. 2017 maio [citado 2019 jun 4];20(Supl 1):46-60. Disponível em: Disponível em: http://www.scielo.br/pdf/rbepid/v20s1/1980-5497-rbepid-20-s1-00046.pdf . doi: 10.1590/1980-5497201700050005 [ Links ]
2. Ministério da Saúde (BR). Departamento de Informática do Sistema Único de Saúde (DATASUS). Estatísticas vitais [Internet]. Brasília: Ministério da Saúde; 2018 [citado 2018 set 29]. Disponível em: http://datasus.saude.gov.br/informacoes-de-saude/tabnet/estatisticas-vitais. [ Links ]
3. Instituto Brasileiro de Geografia e Estatística. Censo demográfico 2010: Espírito Santo [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2017 [citado 2017 mar 5]. Disponível em: Disponível em: https://cidades.ibge.gov.br/brasil/es/panorama [ Links ]
4. Leal MC, Szwarcwald CL, Almeida PVB, Aquino EML, Barreto ML, Barros F, et al. Saúde reprodutiva, materna, neonatal e infantil nos 30 anos do Sistema Único de Saúde (SUS). Ciên Saúde Coletiva [Internet]. 2018 jun [citado 2019 jun 4];23(06):1915-28. Disponível em: Disponível em: http://www.scielo.br/pdf/csc/v23n6/1413-8123-csc-23-06-1915.pdf . doi: 10.1590/1413-81232018236.03942018 [ Links ]
5. Rutstein DD, Berenberg W, Chalmers T, Child CG, Fishman AP, Perrin EB. Measuring the quality of medical care, a clinical method. N Engl J Med [Internet]. 1976 Mar [cited 2019 Jun 4];294(11):582-8. Available from: Available from: https://www.nejm.org/doi/full/10.1056/NEJM197603112941104?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dpubmed . doi: 10.1056/NEJM197603112941104 [ Links ]
6. Taucher E. La mortalidad infantil em Chile. Notas Poblac [Internet]. 1979 [citado 2019 jun 4];7(20):35-72. Disponível em: Disponível em: https://repositorio.cepal.org/handle/11362/12617 [ Links ]
7. Wigglesworth JS. Monitoring perinatal mortality: a pathophysiological approach. Lancet [Internet]. 1980 Sep [cited 2019 Jun 4];2(8196):684-6. Available from: Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(80)92717-8/fulltext . doi: 10.1016/S0140-6736(80)92717-8 [ Links ]
8. Keeling JW, MacGillivray I, Golding J, Wigglesworth J, Berry J, Dunn PM. Classification of perinatal death. Arch Dis Chilh [Internet]. 1989 Oct [cited 2019 Jun 4];64(10 spec n):1345-51. Available from: Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1590112/ . doi: 10.1136/adc.64.10_spec_no.1345 [ Links ]
9. Cole S, Hartford RB, Bergsjo P, McCarthy B. International collaborative efforton birth weight, plurality, perinatal and infant mortality: III: a method of grouping underlying causes of infant death to aid international comparisons. Acta Obstet Gynecol Scand [Internet]. 1989 Jan [cited 2019 Jun 4];68(2):113-7. Available from: Available from: https://obgyn.onlinelibrary.wiley.com/doi/10.3109/00016348909009897 . doi: 10.3109/00016348909009897 [ Links ]
10. Ortiz LP. Agrupamento das causas de morte dos menores de um ano segundo critério de evitabilidade das doenças [Internet]. São Paulo: Fundação SEADE; 2000 [citado 2019 jun 4]. 18 p. Disponível em: Disponível em: http://www.saude.mg.gov.br/images/documentos/Agrupamento%20das%20Causas%20de%20Morte%20dos%20Menores%20de%20Um%20Ano%20Segundo%20Criterio%20de%20Evitabilidade%20das%20Doencas.pdf [ Links ]
11. Malta DC, Duarte EC, Almeida MF, Dias MAS, Morais Neto OL, Moura L, et al. Lista de causas de mortes evitáveis por intervenções do Sistema Único de Saúde do Brasil. Epidemiol Serv Saúde [Internet]. 2007 out-dez [citado 2019 jun 4];16(4):233-4. Disponível em: Disponível em: http://scielo.iec.gov.br/pdf/ess/v16n4/v16n4a02.pdf [ Links ]
12. Dias BAS, SantosNetoET, Andrade MAC. Classificações de evitabilidade dos óbitos infantis: diferentes métodos, diferentes repercussões? Cad Saúde Pública [Internet]. 2017 [citado 2019 jun 4];33(5):e00125916. Disponível em: Disponível em: http://www.scielo.br/pdf/csp/v33n5/1678-4464-csp-33-05-e00125916.pdf . doi: 10.1590/0102-311x00125916 [ Links ]
13. Lansky S, França E, Leal MC. Mortalidade perinatal e evitabilidade: revisão da literatura. Rev Saúde Pública [Internet]. 2002 dez [citado 2019 jun 4];36(6):759-72. Disponível em: Disponível em: http://www.scielo.br/pdf/rsp/v36n6/13534.pdf . doi: 10.1590/S0034-89102002000700017 [ Links ]
14. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Secretaria de Atenção à Saúde. Manual de vigilância do óbito infantil e fetal e do Comitê de Prevenção do Óbito Infantil e Fetal [Internet]. 2. ed. Brasília: Ministério da Saúde ; 2009 [citado 2019 jun 4]. 96 p. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/manual_obito_infantil_fetal_2ed.pdf [ Links ]
15. Bezerra FilhoJG, Pontes LR, Miná DD, Barreto ML. Infant mortality and sociodemographic conditions in Ceará, Brazil, 1991 and 2000. Rev Saúde Pública [Internet]. 2007 Dec [cited 2019 Jun 4];41(6):1023-31. Available from: Available from: http://www.scielo.br/pdf/rsp/v41n6/6060.pdf . doi: 10.1590/S0034-89102007000600018 [ Links ]
16. Oliveira GS, Lima MCBM, Lyra CO, Oliveira AGRC, Ferreira MAF. Desigualdade espacial da mortalidade neonatal no Brasil: 2006-2010. Ciên Saúde Coletiva [Internet]. 2013 [citado 2019 jun 4];18(8):2431-41. Disponível em: Disponível em: http://www.scielo.br/pdf/csc/v18n8/28.pdf . doi: 10.1590/S1413-81232013000800028 [ Links ]
17. Bailey TC, Gatrell AC. Interactive spatial data analysis. Essex: Longman; 1995. [ Links ]
18. Anselin L. Local indicators of spatial association- LISA. Geogra Anal [Internet]. 1995 Apr [cited 2019 Jun 4];27(2):93-115. Available from: Available from: https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1538-4632.1995.tb00338.x . doi: 10.1111/j.1538-4632.1995.tb00338.x [ Links ]
19. Santos IS, Menezes AM, Mota DM, Albernaz EP, Barros AJ, Matijasevich A, et al. Infant mortality in three population-based cohorts in Southern Brazil: trends and differentials. Cad Saúde Pública [Internet]. 2008 [cited 2019 Jun 4];24 Suppl 3:451-60. Available from: Available from: http://www.scielo.br/pdf/csp/v24s3/11.pdf . doi: 10.1590/S0102-311X2008001500011 [ Links ]
20. Nascimento SG, de Oliveira CM, Sposito V, Ferreira DK, do Bonfim CV. Mortalidade infantil por causas evitáveis em uma cidade do Nordeste do Brasil. Rev Bras Enferm [Internet]. 2014 mar-abr [citado 2019 jun 4];67(2):208-12. Disponível em: Disponível em: http://www.scielo.br/pdf/reben/v67n2/0034-7167-reben-67-02-0208.pdf . doi: 10.5935/0034-7167.20140027 [ Links ]
21. Boing AF, Boing AC. Mortalidade infantil por causas evitáveis no Brasil: um estudo ecológico no período 2000-2002. Cad Saúde Pública [Internet]. 2008 fev [citado 2019 jun 4];24(2):447-55. Disponível em: Disponível em: http://www.scielo.br/pdf/csp/v24n2/23.pdf . doi: 10.1590/S0102-311X2008000200024 [ Links ]
22. Melo ECP, Carvalho MS, Travassos C. Distribuição espacial da mortalidade por infarto agudo do miocárdio no Município do Rio de Janeiro, Brasil. Cad Saúde Pública [Internet]. 2006 jun [citado 2019 jun 4];22(6):1225-36. Disponível em: Disponível em: http://www.scielo.br/pdf/csp/v22n6/12.pdf . doi: 10.1590/S0102-311X2006000600012 [ Links ]
23. Almeida WS, Szwarcwald CL. Mortalidade infantil e acesso geográfico ao parto nos municípios brasileiros. Rev Saúde Pública [Internet]. 2012 fev [citado 2019 jun 4];46(1):68-76. Disponível em: Disponível em: http://www.scielo.br/pdf/rsp/v46n1/3106.pdf . doi: 10.1590/S0034-89102012005000003 [ Links ]
24. Bittencourt DAS, Reis LGC, Ramos MM, Rattner D, Rodrigues PL, Neves DCO, et al. Estrutura das maternidades: aspectos relevantes para a qualidade da atenção ao parto e nascimento. Cad Saúde Pública [Internet]. 2014 ago [citado 2019 jun 4];30(Supl 1):S208-19. Disponível em: Disponível em: https://www.scielosp.org/scielo.php?script=sci_arttext&pid=S0102-311X2014000700025 . doi: 10.1590/0102-311X00176913 [ Links ]
25. Nascimento RCS, Costa MCN, Braga JU, Natividade MS. Spatial patterns of preventable perinatal mortality in Salvador, Bahia, Brazil. Rev Saúde Pública [Internet]. 2017 Aug [cited 2019 Jun 4];51:73. Available from: Available from: http://www.scielo.br/pdf/rsp/v51/0034-8910-rsp-S1518-87872017051007076.pdf . doi: 10.11606/s1518-8787.2017051007076 [ Links ]
26. Maranhão AGK, Vasconcelos AMN, Trindade CM, Victora CG, Rabello Neto DL, Porto D, et al. Mortalidade infantil no Brasil: tendências, componentes e causas de morte no período de 2000 a 2010. In: Ministério da Saúde (BR). Departamento de Análise de Situação de Saúde. Secretaria de Vigilância em Saúde. Saúde Brasil 2011: uma análise da situação de saúde e a vigilância da saúde da mulher [Internet]. Brasília: Ministério da Saúde ; 2012 [citado 2019 jun 4]. p. 163-82. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/saude_brasil_2011.pdf [ Links ]
27. Souza GOC, Torres HG. O estudo da metrópole e o uso de informações georreferenciadas. São Paulo Perspec [Internet]. 2003 jul-dez [citado 2019 jun 4];17(3-4):35-44. Disponível em: Disponível em: http://www.scielo.br/pdf/spp/v17n3-4/a05v1734.pdf . doi: 10.1590/S0102-88392003000300005 [ Links ]
28. Lapa PPA, Honorato T, Reis-Santos B, Sales CMM, Maciel ELN, Bertolde AI. Mortalidade Infantil no estado Espírito Santo: uma análise via modelos Completamente Bayesianos. Rev Bras Pesq Saúde [Internet]. 2014 jan-mar [cited 2019 Jun 4];16(1):99-104. Available from: Available from: http://periodicos.ufes.br/RBPS/article/viewFile/8496/5992 [ Links ]
29. Santos IS, Matijasevich A, Barros AJD, Albernaz EP, Domingues MR, Valle NCJ, et al. Avoidable deaths in the first four years of life among children in the 2004 Pelotas (Brazil) birth cohort study. Cad Saúde Pública [Internet]. 2011 [cited 2019 Jun 4];27(Suppl 2):185-97. Available from: Available from: http://www.scielo.br/pdf/csp/v27s2/07.pdf . doi: 10.1590/S0102-311X2011001400007 [ Links ]
30. Carvalho MS, Santos RS. Análise de dados espaciais em saúde pública: métodos, problemas, perspectivas. Cad Saúde Pública [Internet]. 2005 abr [citado 2019 jun 4];21(2):361-78. Disponível em: Disponível em: http://www.scielo.br/pdf/csp/v21n2/03.pdf . doi: 10.1590/S0102-311X2005000200003 [ Links ]
Received: July 10, 2018; Accepted: May 03, 2019
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
