










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.3 Brasília jun. 2020 Epub 22-Mayo-2020
http://dx.doi.org/10.5123/s1679-49742020000300006
Original article
Cross-sectional study on work and health risk behaviors among school students in a rural area of Rio Grande do Sul State, Brazil, 2010 *
1Universidade Federal de Pelotas, Faculdade de Agronomia Eliseu Maciel, Pelotas, RS, Brazil
2Universidade Federal de Pelotas, Escola Superior de Educação Física, Pelotas, RS, Brazil
3Universidade Federal de Pelotas, Faculdade de Medicina, Pelotas, RS, Brazil
Objective
to evaluate association between work and health risk behaviors among rural schoolchildren.
Methods
this was a cross-sectional study with 5th to 8th grade elementary and middle school students attending municipal schools in Barão do Triunfo, RS, Brazil in 2010; a self-administered questionnaire was used; their work profile was characterized as ‘current workers’, ‘former workers’, and ‘non-workers’; health risk behaviors examined were smoking, alcohol consumption, overweight, and physical inactivity (≤300 minutes per week).
Results
of the 339 participants under 16 years old (89.9%), 82.3% were current workers; their predominant work was domestic services (39.8%), and farming (29.9%); 24.8% of students were overweight, 51.2% were inactive during leisure, 6.6% smoked, and 27.0% had consumed alcohol in the last 30 days; alcohol consumption was higher among workers than non-workers (p=0.02).
Conclusion
eight out of ten schoolchildren worked, most of them as child labor; the most frequent health risk behavior was alcohol consumption.
Key words: Adolescent Behavior; Health; Child Labor; Alcoholic Beverages; Cross-Sectional Studies
Introduction
Globally there are currently 152 million economically active children and adolescents (under 18 years old), including those who work illegally and in the informal sector of the economy.1 Around 70% of children and adolescents involved in child labor worldwide work in the agricultural sector, 17% in the service sector and 12% in industry, as well as one third who do unpaid family activities.1 Poverty, unemployment and belief in work contributing to personal growth are some of the factors that lead families, especially in rural areas,3 to use their children’s labor as a form of income generation.4 It is difficult to distinguish between what is sporadic participation in work activities and what is truly child labor.5 These aspects, among others, make underage labor in rural areas, especially in family farming, a permanent challenge, whether from a legal or a health point of view.3
Brazil is signatory to international agreements on child labor eradication and compliance with the rights of adolescents who work.6 Child labor is work done by individuals under 16 years old, regardless of their occupational category, except in the case of apprentices for whom the minimum age is 14.7 Brazil has a Child and Adolescent Statute to guarantee these rights, as well as government actions to eradicate child labor, minimize health complaints and include these individuals in school and social activities.7
Child labor activities are highly prevalent in Brazil8 and have been associated with important health consequences,5 in particular constant exposure to risk of accidents, development of occupational illnesses, stress, exhaustion9 as well as interference in school life, such as truancy and having to repeat grades.11 Among adolescents and school students who work, tobacco and alcohol use12 are also behaviors of concern and frequently found among those who live in rural areas.13
Despite the relevance of these health risk behaviors, during childhood, adolescence and adult life, few studies are done with rural populations with the aim of investigating the relationship between work activities, child labor and risk behaviors. When an adolescent takes part in a work activity under safe conditions, some positive aspects have stood out as contributing to psychological development, increased self-esteem and learning skills and individual experiences important for socialization. Moreover, authors have reported that urban adolescent workers are more physically active14 and with adequate weight for age when compared to non-working adolescents.15
In rural locations, these activities can be confused with child labor and studies have not assessed activities carried out during adolescents’ free time and which are important for preventing health problems.9 In view of this, the need exists to investigate the relationship between work and health risk behaviors, given the inexistence of studies with these outcomes grouped together.
The objective of this study was to assess association between work and health risk behavior among school students in a rural area.
Methods
This was a school-based cross-sectional study conducted in 2010 in the municipality of Barão do Triunfo, located in the coal mining region of the state of Rio Grande do Sul, Brazil.
The municipality’s economy is based on tobacco farming, followed by cattle rearing, and it has one of the state’s lowest human development indices (HDI=0.61).16 In 2010, Barão do Triunfo had 7,018 inhabitants, 90% of whom lived in the rural area of the municipality, eight municipal schools located in the rural area and two in the urban area.16 As to its adolescent population, 52.9% were male, 50.1% were between 10 and 14 years old and 3.4% did not attend school.17
The study took into consideration all students enrolled in the 5thto 8thgrades, between 10 and 19 years old, distributed among three rural municipal schools offering elementary and middle school education. According to the 2010 school census,16 412 students in this age range were enrolled in the municipal education system and all of them were included in the study.
Following authorization by the City Government, contact was made with the school administrators and the students’ parents. Once their authorization had been obtained, data collection took place between March and September 2010. Identification data held on lists of students by school grade (name, age, grade and contact details) were provided by the Municipal Education Department.
A self-administered instrument was used after having been tested beforehand with a similar sample that was not included in this study. The instrument was used to collect data for a Master’s degree academic project and was divided into blocks of information on sociodemographic details, work, health, diet, physical activity, use of tobacco and alcohol. Data acquisition took place in two stages: (i) questionnaire administration; and (ii) taking measurements. Initially, each classroom was visited at least three times, when the researcher in charge explained the objectives of the study and administered the questionnaire. This involved explaining the objectives of the study and giving guidance on how to answer the instrument. Confidentiality of the information provided by the participants was ensured; on average it took 40 minutes to answer the questionnaire. The outcomes of interest were health risk behaviors (use of tobacco, use of alcoholic beverages, overweight and physical inactivity during leisure time), and the main exposure variable, i.e. work profile.
With regard to tobacco and alcohol consumption, we used the questions adopted by the instrument designed by the Brazilian Psychotropic Drug Information Center: students were asked whether during the last month they had smoked cigarettes (filter, straw etc., even if only one or two puffs) and whether they had consumed alcoholic beverages (e.g. rum, beer, whisky, vodka, wine etc., even if only one or two sips). For both behaviors, a positive answer was considered to be when the student had consumed the substance in the last 30 days, regardless of the number of cigarettes and regardless of the number of measures of alcoholic beverage consumed.17
Following this, weight and height were measured, to assess excess weight: overweight and obesity, as a health risk behavior. Digital Plenna™ scales (up to 150kg – 100g precision) were used to measure weight; and a portable Sanny™ stadiometer (up to 210cm – 1mm precision) was used to measure standing height. The measurements were taken at the schools, in private, with students wearing light clothes, barefoot and in an upright position. These measurements were taken twice by teachers (they had 8 hours prior training); and were repeated when the same student had a difference of more than 10% between the two measurements. Quality control was performed on 10% of measurements. Excess weight was calculated according to the body mass index (BMI), classified taking ≥85% as the parameter, according to age and sex.18
Level of physical activity during leisure time was assessed by asking about activities done during the seven days prior to the questionnaire being administered, excluding physical activity at school and physical activities relating to occupation, domestic chores and going from one place to another. Questions validated by Bastos et al. (2008)19 captured the frequency and duration of each physical activity performed (e.g.: swimming, playing football, basketball etc.). A cut-off point of 300 minutes or less a week was used to classify students as physically inactive.
Work profile, which was the main exposure variable, was defined as any regular work activity, whether paid or not, whether at home or not, reported by the adolescents.2 This definition included helping with domestic activities (housekeeping for parents or other families; looking after younger siblings or other children) as well as formal paid employment and informal work activities – e.g. farming and/or cattle raising activities, at home or away from home. Child labor was considered to be when adolescents under 16 years old reported working or doing any kind of work activity in the last 30 days, including domestic chores, caring for children, looking after animals and doing farming work.7 Former workers were considered to be those who had worked at some time during their lifetime but had not been working in the last 30 days; non-workers were those who had never worked in their lifetime; and current workers were those who had worked in the last 30 days. Two categories of current work (yes; no) were used for the purpose of data analysis.
The questionnaire answered by the students enabled their social and demographic characteristics, health self-assessment, work characteristics and behaviors putting their own health at risk to be investigated. Firstly, we will describe the sociodemographic characteristics and the form of self-assessment of health investigated:
age (in years: 10-13; 14-15; 16 or over);
sex (male; female);
race/skin color (white; non-white); and
self-assessment of health (obtained by asking the question How do you rate your health? with the following answer options: excellent; very good; good; regular or poor).
With regard to the work characteristics of current workers, they were asked:
age when began working (in years: up to 11; 11-12; 13 or over);
place of work activity (at home; away from home; both);
type of work activity (domestic chores/caring for siblings; farming/cattle raising services; other activities);
number of hours worked a day (up to 4; 5-8; 9 or more);
number of days worked a week (1-5; 6-7); and
payment in money (yes; no).
The health risk behaviors assessed were:
tobacco consumption in the last month (yes; no);
alcohol consumption in the last month (yes; no);
excess weight (yes; no); and
weekly physical inactivity in leisure time (yes; no).
As the study was conducted at the schools for logistical reasons, before it started an easy to understand self-administered questionnaire was sent to all parents/legal guardians containing questions about monthly family income (in minimum wages) and parental schooling (in complete years of study). The Free and Informed Consent form was attached to the questionnaire sent to parents/legal guardians.
The data were input twice using Epi Info 6.0 for data error correction using the Validate command. Prevalence rates and respective confidence intervals were calculated for work and health risk behaviors, according to exposure, using State version 11.0 with a 0.05 significance level. Following this, the chi-square test was used to check for work prevalence rate differences (never, former, current) between the risk behavior subgroups. Additional analyses were performed considering two work categories: current work (yes; no), for which Poisson regression with estimated robust variance was used to assess association between health risk behaviors; and current work adjusted for the ‘sex’ and ‘age’ variables.
The adolescents took part in the study after giving verbal consent and parental authorization given by their signing the Free and Informed Consent form. The study was authorized by the local government authority and approved by the Human Research Ethics Committee of the Federal University of Pelotas Physical Education Higher Education School (CEP/ESEF/UFPel): Protocol No. 068, dated November 27th2009. Following CEP/ESEF/UFPel authorization, a meeting was held with the head teachers of the three municipal schools, when each of them signed a document authorizing data collection to be started at their respective teaching institution.
Results
Of the 412 students eligible to take part in the study, 377 were interviewed and 375 had their anthropometric data collected, totaling 9% losses (adolescents absent from the classroom at the time data was collected) and refusals. Taking total participants, 60.8% were between 10 and 13 years old, 53.0% were male and 54.4% were of White race/skin color (data not shown in tables). Excess weight accounted for 24.8%, 51.2% were inactive during leisure time, 6.6% had smoked and 27.0% had consumed alcohol in the 30 days prior to the interview (data not shown in tables).
With regard to work, 82.1% (95%CI 77.0;86.0) were current workers, 9.6% (95%CI 7.0;13.0) were former workers and 8.3% (95%CI 6.0;12.0) were non-workers. Among those interviewed, 339 (89.9%) were under 16 years old and 82.3% of these were current workers (data not shown in tables). There was only a slight difference between work percentages by age and sex. There were no statistically significant differences with regard to race/skin color: in the case of students of White race/skin color, 10.2% did not work, 82.5% did work and 7.3% had worked previously; in the case of non-Whites, 8.8% did not work, 81.8% did work and 9.4% had worked previously. Among students who assessed their health as being excellent, 20.3% did not work, 70.3% did work and 9.5% had worked previously, while among those who reported their health as being regular or poor, 4.9% did not work, 82.7% did work and 12.4% had worked previously (p<0.001) ( Table 1 ).
Table 1 – Description of the work profile of rural area adolescents (n=377) according to social, demographic and health variables, Barão do Triunfo, Rio Grande do Sul, 2010
| Variables | Worker | p-valuea | ||
|---|---|---|---|---|
|
| ||||
| Current | Former | |||
|
| ||||
| No % | Yes % | Yes % | ||
| Work profile | 8.3 | 82.1 | 9.6 | |
| Age (in years) | 0.740 | |||
| 10-13 | 10.0 | 80.8 | 9.2 | |
| 14-15 | 9.1 | 85.4 | 5.5 | |
| ≥16 | 8.3 | 80.6 | 11.1 | |
| Sex | 0.631 | |||
| Male | 9.6 | 80.8 | 9.6 | |
| Female | 9.7 | 83.5 | 6.8 | |
| Race/skin color | 0.707 | |||
| White | 10.2 | 82.5 | 7.3 | |
| Non-White | 8.8 | 81.8 | 9.4 | |
| Self-assessment of healthb | <0.001 | |||
| Excellent | 20.3 | 70.3 | 9.5 | |
| Very good | 7.9 | 88.1 | 4,0 | |
| Good | 5.4 | 90.1 | 4.5 | |
| Regular/poor | 4.9 | 82.7 | 12.4 | |
a) Chi-square test for heterogeneity.
b) n=342.
Table 2 describes work characteristics of the young respondents classified as current workers. Almost half of them (45.4%) had started working when they were between 11 and 12 years old, and the majority worked at home (87.2%). The most frequent types of activity were domestic services/looking after siblings (41.6%) and farming/cattle rearing activities (42.1%). With regard to workload, 23.6% reported working nine or more hours a day and 56.5% reported working six or seven days a week. Approximately 68.0% reported receiving some degree of payment in money for their work.
Table 2 – Profile of rural area adolescent workers (n=310), according to variables related to work activity characteristics, Barão do Triunfo, Rio Grande do Sul, 2010
| Independent variables | n | % |
|---|---|---|
| Age (in years) when began working | ||
| <11 | 145 | 38.5 |
| 11-12 | 171 | 45.4 |
| ≥13 | 61 | 16.2 |
| Place of work activity | ||
| At home | 286 | 87.2 |
| Away from home | 32 | 9.8 |
| Both | 10 | 3.0 |
| Type of work activity | ||
| Domestic services/caring for siblings | 140 | 41.6 |
| Farming/cattle rearing services | 142 | 42.1 |
| Other activities | 55 | 16.3 |
| Number of hours worked per day | ||
| ≤4 | 165 | 43.8 |
| 5-8 | 123 | 32.6 |
| ≥9 | 89 | 23.6 |
| Number of days worked per week | ||
| 1-5 | 164 | 43.5 |
| 6-7 | 213 | 56.5 |
| Payment in money | ||
| No | 106 | 31.6 |
| Yes | 229 | 68.4 |
With regard to health risk behaviors, percentage tobacco consumption was similar between the three work profile groups, differently to alcohol consumption which was reported by 29.5% of current workers, 12.9% of former workers and 17.7% of non-workers (p=0.06). The prevalence rates of excess weight and physical inactivity did not differ significantly between each other by work profile ( Table 3 ).
Table 3 – Health risk behaviors according to rural adolescent work profile (n=377), crude and adjusted analysis, Barão do Triunfo, Rio Grande do Sul, 2010
| Health risk behaviors | Non-worker | Current worker | Former worker | p-valuea | Current work Crude analysis | Current work Adjusted analysisd | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||||||
| (%) | (%) | (%) | PRb | 95%CIc | p-valuea | PRb | 95%CIc | p-valuea | ||||
| Tobacco consumption in the last 30 days | 0.725 | 0.462 | 0.722 | |||||||||
| Yes | 6.3 | 7.0 | 3.2 | 1.06 | 0.91;1.25 | 1.02 | 0.59;1.44 | |||||
| No | 93.8 | 93.1 | 96.8 | 1.00 | 0.78;1.09 | 1.00 | 0.29;1.38 | |||||
| Alcohol consumption in the last 30 days | 0.056 | 0.007 | 0.661 | |||||||||
| Yes | 17.7 | 29.5 | 12.9 | 1.13 | 1.03;1.24 | 1.04 | 0.81;1.33 | |||||
| No | 82.3 | 70.5 | 87.1 | 1.00 | 0.75;1.02 | 1.00 | 0.55;1.10 | |||||
| Excess weighte | 0.381 | 0.675 | 0.748 | |||||||||
| Yes | 33.3 | 24.3 | 19.3 | 0.84 | 0.73;0.98 | 0.64 | 0.56;0.72 | |||||
| No | 66.7 | 75.7 | 80.7 | 1.00 | 0.87;1.09 | 1.00 | 0.73;1.24 | |||||
| Weekly physical inactivity in leisure time | 0.256 | 0.690 | 0.8113 | |||||||||
| Yes | 58.3 | 52.0 | 38.7 | 0.82 | 0.77;0.88 | 0.64 | 0.55;0.75 | |||||
| Não | 41.7 | 48.0 | 61.3 | 1.00 | 0.89;1.08 | 1.00 | 0.78;1.22 | |||||
a) Chi-square test.
b) PR: prevalence ratio.
c) 95%CI: 95% confidence interval.
e) Two values unknown.
d) Poisson regression – adjustment for age and sex.
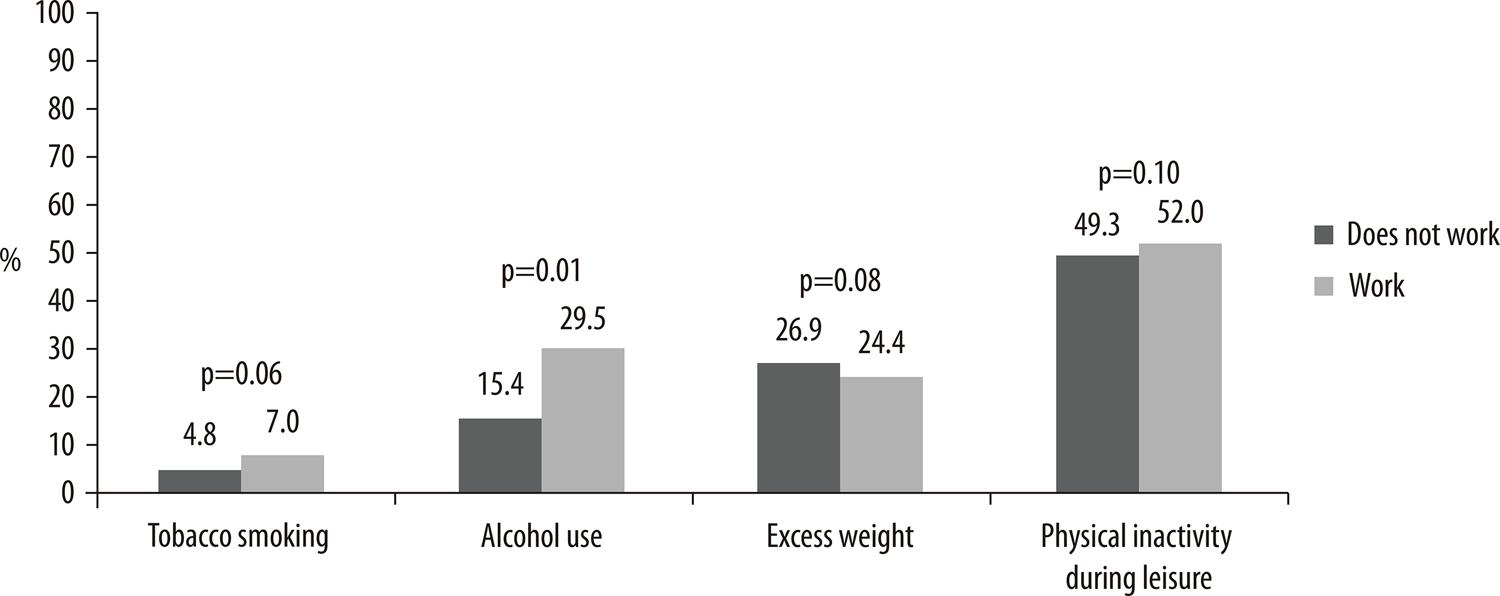
In view of the low number of young respondent in the former work (n=31) and non-work (n=36) categories, we analyzed risk factors comparing current workers with all non-workers at the time of the study (former workers and non-workers). Figure 1 shows that alcoholic beverage consumption was higher among current workers (29.5%), when compared to non-workers (15.4%) (p=0.01). This association remained even after adjusting for students’ age and sex, and for family income and parental schooling (data not shown in tables). Absence of association between excess weight, physical inactivity during leisure time and tobacco consumption in the last 30 days, and current work, found in the previous analyses was also found in this additional analysis.
Discussion
Prevalence of work among the population studied was high: eight out of every ten school students (10-16 years old) reported doing work activities, and the majority of the tasks they did were characterized as child labor. Self-assessment of health reported by the adolescents as being excellent or regular/poor differed between the work profiles. With regard to risk behaviors, consumption of alcoholic beverages was associated with working. It must be emphasized that child labor causes exposure to risk and harm both in the present and in the future, and this is not taken into account by families or local government managers.
Among adolescents heard by the National School Health Survey (PeNSE) conducted in 2015, the majority of those who worked were precisely those who self-reported their health status as poor compared to non-workers in the crude analysis. This finding lost its power in the adjusted analysis,20 similarly to the findings of our study. A recent systematic literature review found that child labor continues to be negatively associated with the physical and psychological health of children involved in it.21 Studies also report that rural areas account for the highest percentage of child labor with outcomes that have greater impact on health1 Alcoholic beverage intake in the last month was found to be higher among current school student workers compared to their non-worker peers in the municipality. It is noteworthy that alcohol use in adolescence can have diverse negative impacts on health: depression, suicidal behavior, car accidents, alcohol dependence in adult life, among others.22
Some sociocultural factors may explain, albeit partially, the association found. The possibility of school students who work feeling more autonomous and closer to the adult world, for instance, may reflect a local cultural norm in which consuming drinks containing alcohol is valued.3 In Barão do Triunfo, alcoholic beverage consumption is constantly encouraged in moments of integration and leisure (such as religious feasts and nighttime dances) among children, adolescents and adults, despite restrictions existing on sales of alcohol to minors which, it must be said, are not duly enforced.Although this study did not intend to assess where alcohol was consumed, the high participation of children and adolescents in these events and constant encouragement to drink may be a factor triggering the result we found, especially among those who work, many of whom can afford to pay for it. Motivations such as curiosity, the quest for pleasure, liveliness, reduced shyness, anxiety (resulting from working conditions or the early commitment to working), acceptance by friends and socialization norms associated with work and the adult world22 can encourage alcohol use. Alongside this is the historical cultural influence of immigration: the local population is predominantly of Italian and German origin, whose ethnic/cultural identities are associated, respectively, with the habit of consuming wine and beer.
The behavior found corroborates the results of the 1stNational Survey of Alcohol Consumption Patterns in the Brazilian Population, with regard to comparison between adolescents (14-19 year-olds) living in Brazilian urban and rural areas. Madruga et al.23 found that prevalence of alcohol use or dependence was similar between adolescents in both areas. The main determining factor of this behavior is not the area in which they live but rather the broader context in which students are placed.
In urban areas alcohol intake is encouraged by the presence of advertising in many different places;24 in rural areas, apart from advertising, other components and players influence alcohol consumption, with similar results. However, the consequences of this behavior during the lifetime of people who live in rural areas can be more negative, given their lower access to a series of health, social support and education resources, compared to the availability of these resources in urban areas. In developed countries, binge drinking and risky alcohol intake is more frequent among rural youth than among urban youth.25
Contrary to the expected, tobacco use was not found to be associated with work profile. Despite school student workers reporting greater tobacco use than non-workers, statistical difference was not confirmed. Nevertheless, the prevalence rates found were similar to those found in adolescents who took part in the PeNSE/2015 Survey (5.6%).26 Another study, involving a cohort of adolescents, demonstrated a strong relationship between working and tobacco use.27 In Barão do Triunfo, many farmers are tobacco growers, so that child and adolescent farm workers have direct contact with the substance or know a lot about how it is grown and harvested. Frequent contact can encourage use, despite the existence of regulatory measures on tobacco advertising and sales.13
Excess weight and physical activity during leisure time were not found to be associated with work profile. A literature review did not find a relationship between working and nutritional status among young people. However, studies with workers in non-sedentary sectors (e.g. the farming or building sectors) have indicated association between child labor and reduced height and weight, in the same direction and magnitude.28 Prevalence of physical inactivity during leisure time among young Brazilians is generally high,26 as a result of barriers existing and reported by adolescents themselves, such as lack of company, time, money and/or preference for other activities.27 Lack of specific public facilities in rural areas for doing physical activities may have influenced the finding of this study, which was similar to findings regarding school students in other regions of the country.29
It is appropriate to mention that in the phase of life assessed in this study, workload may have modified endocrine factors related to weight gain and, in turn, due to physical effort working may have prevented accumulation of abdominal fat. However, work activities that require physical exertion generally lead to more calories being burnt and weight increase as the years go by.30
Some limitations inherent to the study, such as its cross-sectional design, prevent assessment of temporality in the associations found. In addition, the time when the behaviors began was not investigated, nor whether alcohol and tobacco consumption was of high risk to health. Despite losses and refusals accounting for less than 10%, it is possible that those adolescents who were absent from school were working and this would characterize selection bias. This study did not examine other aspects of child labor, in particular children and adolescents involved in illicit activities, such as prostitution and drug trafficking. These activities, which are much more dangerous, could be determinants for those children and adolescents not being at school.
Furthermore, the study’s sample size is small and not very heterogeneous, although it does represent the totality of the municipality’s school students. This prevented health risk behaviors from being stratified by sex in the analyses. Nevertheless, this study is one of the few on this theme and we did not find Brazilian studies relating rural child and adolescent labor to the health risk behaviors observed here. Some studies we consulted relate one, two or three of these behaviors to adolescent work activities, the majority focusing on urban and not rural populations.
In conclusion, prevalence of adolescent school student workers was high in Barão do Triunfo, the majority being characterized as child/adolescent labor. Domestic and farming services were predominant and the most prevalent health risk among current workers was alcoholic beverage intake in the last 30 days. These findings reinforce the need to broaden the scope of public policies aimed at eradicating child/adolescent labor and promoting the health of young school students, especially these living in rural areas. Joint actions developed jointly with families, government, civil society and the third sector are fundamental for eradicating child labor and improving the working and health conditions of young people, based on broader policies or policies better adapted to the social, environmental and cultural issues of each specific place or population.
REFERENCES
1. International Labour Organization (ILO). Global estimates of child labour: Results and trends, 2012-2016 Internet . 2017. Available from: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---dcomm/documents/publication/wcms_575499.pdf%0Ahttps://www.ilo.org/global/publications/books/WCMS_575499/lang--en/index.htm [ Links ]
2. Facchini LA. Trabalho infantil em Pelotas : perfil ocupacional e contribuição à economia Child labor in Pelotas : occupational characteristics and contribution to the economy. Ciências de Saúde Coletiva Internet 20003;8(4):953–61. Available from: http://www.scielo.br/pdf/csc/v8n4/a17v8n4.pdf [ Links ]
3. Radfar A, Asgharzadeh SAA, Quesada F, Filip I. Challenges and perspectives of child labor. Ind Psychiatry J 2018;27(1):17–20. [ Links ]
4. Marin JOB. O Agronegócio e o problema do trabalho infantil. Rev Sociol e Polit 2010;18(35):189–206. [ Links ]
5. Fassa AG, Facchini LA, Dall’agnol MM, Christiani DC. Child labor and health: Problems and perspectives. Int J Occup Environ Health 2000;6(1):55–62. [ Links ]
6. Presidência da República B. Decreto n. 6.481, 12 de junho de 2008. Regulamenta os artigos 3°, alínea “d”, e 4° da Convenção 182 da Organização Internacional do Trabalho (OIT) que trata da proibição das piores formas de trabalho infantil e ação imediata para sua eliminação, aprovada . 2008. [ Links ]
7. Presidência da República B. Lei no 8.069; de 13 de julho de 1990. Dispõe sobre o Estatuto da Criança e do Adolescente e dá outras providências. 2019. [ Links ]
8. Brasil. Pesquisa Nacional por Amostra de Domicílios : síntese de indicadores 2014 / IBGE, Coordenação de Trabalho e Rendimento Internet . 2015. Available from: http://biblioteca.ibge.gov.br/visualizacao/livros/liv94935.pdf [ Links ]
9. Wright S, Marlenga B, Lee BC. Childhood agricultural injuries: An update for clinicians. Curr Probl Pediatr Adolesc Health Care Internet 2013;43(2):20–44. Available from: http://dx.doi.org/10.1016/j.cppeds.2012.08.002 [ Links ]
10. Rauscher K, Runyan C. Adolescent occupational fatalities in north carolina (1990-2008): An investigation of child labor and osha violations and enforcement. New Solut 2013;22(4):473–88. [ Links ]
11. Sousa OMCG de, Alberto M de FP. Early work and children’s and adolescents’ schooling process. Psicol em Estud 2008;13(4):713–22. [ Links ]
12. Souza DPO de, Areco KN, Silveira Filho DX da. Álcool e alcoolismo entre adolescentes da rede estadual de ensino de Cuiabá, Mato Grosso TT - Alcohol and alcoholism among Brazilian adolescent public-school students. Rev Saude Publica Internet 2005;39(4):585–92. [ Links ]
13. Maldonado RM, Pedrão LJ, Castillo MMA, García KSL, Rodríguez NNO. Auto-estima, auto-eficácia percebida, consumo de tabaco e álcool entre estudantes do ensino fundamental, das áreas urbana e rural, de monterrey, Nuevo León, México. Rev Lat Am Enfermagem 2008;16(spe):614–20. [ Links ]
14. De Rezende LFM, Azeredo CM, Canella DS, Claro RM, De Castro IRR, Levy RB, et al. Sociodemographic and behavioral factors associated with physical activity in Brazilian adolescents. BMC Public Health 2014;14(1):1–11. [ Links ]
15. Shoman AE, Mostafa NS, Musslem AA. Nutritional status and parasitic infestation among working children in a village in Egypt: A comparative study. J Egypt Public Health Assoc 2015;90(2):80–4. [ Links ]
16. Instituto Nacional de Pesquisas e Estudos Anísio Teixeira I. Censo Escolar 2010. 2010;2010:1–42. [ Links ]
17. Carlini EL de A, Noto AR, Carlini CM de A, Locatelli DP, Abeid LR, Amato T de C, et al. VI Levantamento Nacional sobre o Consumo de Drogas Psicotrópicas entre Estudantes do Ensino Fundamental e Médio das Redes Publica e Privada de Ensino nas 27 Capitais Brasileiras. 2010. [ Links ]
18. Must A, Dallal GE, Dietz WH. Reference data for obesity: 85th and 95th percentiles of body mass index (wt/ht2) and triceps skinfold thickness. Am J Clin Nutr 1991;53(4):839–46. [ Links ]
19. Bastos JP, Araújo CLP, Hallal PC. Prevalence of insufficient physical activity and associated factors in Brazilian adolescents. J Phys Act Heal 2008;5(6):777–94. [ Links ]
20. Malta DC, De Oliveira MM, Machado IE, Prado RR, Stopa SR, Crespo CD, et al. Characteristics associated to a poor selfrated health in Brazilian adolescents, National Adolescent School-based Health Survey, 2015. Rev Bras Epidemiol 2018;21(Suppl 1). [ Links ]
21. Ibrahim A, Abdalla SM, Jafer M, Abdelgadir J, De Vries N. Child labor and health: A systematic literature review of the impacts of child labor on child’s health in low- and middle-income countries. J Public Heal (United Kingdom) 2019;41(1):18–26. [ Links ]
22. Leeman RF, Hoff RA, Krishnan-Sarin S, Patock-Peckham JA, Potenza MN. Impulsivity, Sensation-Seeking and Part-Time Job Status in Relation to Substance Use and Gambling in Adolescents. J Adolesc Heal 2014;54(4):460–6. [ Links ]
23. Madruga CS, Laranjeira R, Caetano R, Pinsky I, Zaleski M, Ferri CP. Use of licit and illicit substances among adolescents in Brazil - A national survey. Addict Behav Internet 2012;37(10):1171–5. Available from: http://dx.doi.org/10.1016/j.addbeh.2012.05.008 [ Links ]
24. Faria R, Vendrame A, Silva R, Pinsky I. Association between alcohol advertising and beer drinking among adolescents. Rev Saude Publica 2011;45(3):441–7. [ Links ]
25. Legleye S, Janssen E, Spilka S, Le Nézet O, Chau N, Beck F. Opposite social gradient for alcohol use and misuse among French adolescents. Int J Drug Policy 2013;24(4):359–66. [ Links ]
26. Brasil. Ministério da Saúde. Pesquisa nacional de saúde do escolar : 2015. Internet . 2016. Available from: https://biblioteca.ibge.gov.br/visualizacao/livros/liv97870.pdf [ Links ]
27. Dias DF, Loch MR, Ronque ERV. Perceived barriers to leisure-time physical activity and associated factors in adolescents. Cienc e Saude Coletiva 2015;20(11):3339–50. [ Links ]
28. Aransiola TJ, Justus M. Child labor hazard on mental health: Evidence from Brazil. J Ment Health Policy Econ 2018;21(2):49–58. [ Links ]
29. Figueiredo VC, Szklo AS, Costa LC, Kuschnir MCC, Da Silva TLN, Bloch KV, et al. ERICA: Smoking prevalence in Brazilian adolescents. Rev Saude Publica 2016;50(supl 1):1s-10s. [ Links ]
30. Yamada Y, Kameda M, Noborisaka Y, Suzuki H, Honda M, Yamada S. Excessive fatigue and weight gain among cleanroom workers after changing from an 8-hour to a 12-hour shift. Scand J Work Environ Heal 2001;27(5):318–26. [ Links ]
*This article was derived from the Master’s Degree dissertation entitled ‘Association between health risk behaviors of rural area adolescent students and their parents and siblings’, defended by Chirle de Oliveira Raphaelli at the Federal University of Pelotas Physical Education Higher Education School Postgraduate Physical Education Program in 2011.
Received: August 20, 2019; Accepted: March 23, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
