










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.3 Brasília jun. 2020 Epub 25-Maio-2020
http://dx.doi.org/10.5123/s1679-49742020000300008
Original article
Evolution of indicators and service capacity at the beginning of the COVID-19 epidemic in Northeast Brazil, 2020
1Universidade Federal do Piauí, Colégio Técnico de Teresina, Teresina, PI, Brazil
2Universidade Federal do Piauí, Departamento de Enfermagem, Floriano, PI, Brazil
3Universidade Federal do Piauí, Centro de Inteligência em Agravos Tropicais Emergentes e Negligenciados, Teresina, PI, Brazil
Objective
to describe the evolution of indicators and capacity for health care in the initial phase of the COVID-19 epidemic in the Northeast region of Brazil.
Methods
this was a descriptive study based on COVID-19 case epidemiological bulletins released by the Ministry of Health up until April 1st, 2020. The incidence rate, lethality and number of cumulative daily cases were calculated.
Results
1,005 confirmed cases of COVID-19 were identified, most of them in Ceará and Bahia states. The incidence rate was 1.8/100,000 inhabitants and lethality was 2.7%. Ceará was the state with the highest number of cases, with 29.6 new cases per day on average. Average intensive care bed availability in the Northeast region (1.04/10,000 inhab.) was below the national average (2.8/10,000 inhab.).
Conclusion
the indicators suggest that COVID-19 impact is heterogeneous and signal the challenges for health systems in the Northeast Region.
Key words: Coronavirus; Coronavirus Infections; Pandemics; Health Status Indicators; Epidemiology, Descriptive
Introduction
In December 2019, China identified an outbreak of an acute respiratory syndrome among workers at a food and live animal market in Wuhan, caused by a new coronavirus (SARS-CoV-2). This virus belongs to the Coronaviridae family and causes the respiratory disease called COVID-19.1 The impacts of this disease began to be perceived in the health sector and on the global economy in early 2020.
SARS-CoV-2 has high transmissibility, which occurs through person-to-person contact and via fomites, and may remain active on surfaces for more than 24 hours.2 The acute respiratory syndrome it causes ranges from mild cases (around 80%) to very severe cases with respiratory insufficiency (5% to 10%). Lethality is also variable, depending on age group and associated clinical conditions.3 SARS-CoV-2 spread rapidly, affecting more than 100 countries on all five continents, leading the World Health Organization (WHO) to declare COVID-19 to be a pandemic on March 11th2020.1
In Brazil, according to the Ministry of Health, 5,717 COVID-19 cases and 201 deaths had been confirmed as at March 31st.5 The country’s Northeast region concentrated 875 (15.3%) of these cases. It was the region with the second highest number of cases after the Southeast region.
Considering how novel coronavirus has spread rapidly throughout Brazil, the importance of continual epidemiological monitoring for containing the epidemic, the need to plan health care for the population and the economic, environmental and social peculiarities of the Northeast region, knowledge is needed about the evolution of the epidemic and initial health care capacity in this region, so as to generate information capable of informing the best strategies for facing the epidemic.
The objective of this article was to describe the indicators and capacity for health care in the initial phase of the COVID-19 epidemic in the Northeast region of Brazil.
Methods
This was a descriptive study to accompany COVID-19 cases in Northeast Brazil based on epidemiological bulletins.
The Northeast region states account for a population of approximately 53 million inhabitants, according to the Brazilian Institute of Geography and Statistics (IBGE), over an area of 1,554,257km2. It is Brazil’s second most populous region. The ethnic/skin color composition of the region’s population is 62.5% brown; 29.2%, white; 7.8% black; and 0.5% indigenous.6 Between 2009 and 2017, hospital bed availability per 100,000 inhabitants decreased by 8.2%, while intensive care unit (ICU) bed availability increased by 73.6% and there was an increase in the number of large-scale hospitals available via the Brazilian National Health System (SUS). With regard to the legal nature of hospitals, between 2012 and 2017 there was a reduction in the number of private and non-profit hospitals outsourced to SUS and an increase in public administration hospital establishments. Between the beginning and the end of the same period, total hospitalizations decreased by 10.7%.7
We analyzed records of cases occurring in people resident in the nine states that comprise Northeastern Brazil, namely: Alagoas, Bahia, Ceará, Maranhão, Paraíba, Pernambuco, Piauí, Rio Grande do Norte and Sergipe.
The variables analyzed were: number of confirmed cases, number of deaths, number of hospital beds and number of ICU beds.
The study was conducted using data recorded between March 6thand April 1stand retrieved from the Brazil Coronavirus Panel (available at: https://covid.saude.gov.br/), which shows on-line monitoring of COVID-19 cases in Brazil, providing information on new cases and deaths by region, state, day and epidemiological week.8 Data on hospital bed capacity, including ICU bed capacity, were retrieved from the National Health Establishment Registry. Data on resident population were retrieved from the IBGE website and the website of the SUS Information Technology Department (DATASUS), taking the population projection for Brazil as a whole and its Federative Units by sex and age for the period 2000-2030.
Based on the absolute number of confirmed COVID-19 cases and deaths, we calculated incidence (number of confirmed cases divided by resident population and multiplied by 100,000 inhabitants), lethality (number of COVID-19 deaths divided by total confirmed cases and multiplied by 100) and daily cumulative index (DCI) (confirmed cases divided by the number of days between the first reported case and April 1st2020).
Excel for Windows 2016 was used to calculate incidence, lethality, DCI, hospital bed capacity and also to produce graphs. Average case numbers and maximum and minimum values were also calculated.
The study did not need to be submitted for approval by a Research Ethics Committee as public domain data with no identification of participants were used.
Results
Between March 6thand April 1st2020, 1,005 COVID-19 cases were confirmed in the Northeast region. The first case was recorded on March 6thin the state of Bahia and cases increased continually with effect from then. Of the total number of cases reported in the study period, 27 (2.7%) died, with the first death being registered on March 25thin the state of Pernambuco ( Figure 1 ).
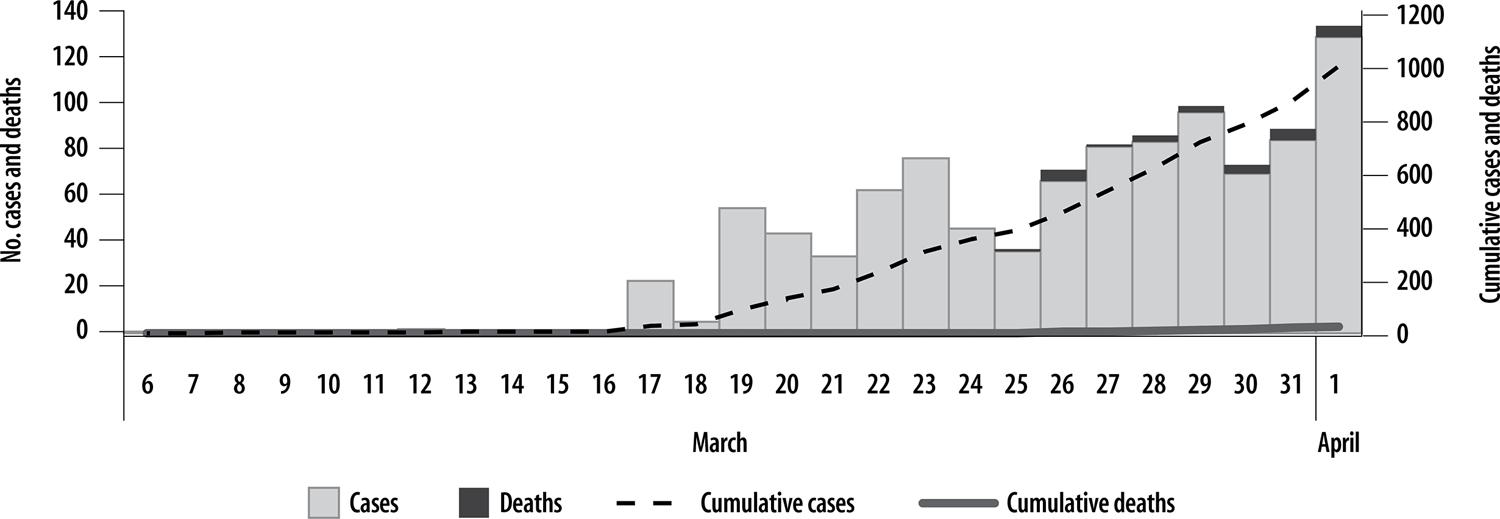
Source: Brazilian Ministry of Health. Coronavirus Panel. Access on: 2020 Apr 02.
Figure 1 – Evolution of COVID-19 cases and deaths in the Northeast region, Brazil (N=1,005), from March 6th to April 1st 2020
The states of Ceará (41.1%) and Bahia (24.4%) concentrated more than 60% of cases reported in the Northeast region. The number of deaths was highest in Ceará and Pernambuco. The overall incidence rate was 1.8/100,000 inhab., but was higher in the states of Ceará (4.9), Rio Grande do Norte (2.6) and Bahia (1.7). Overall lethality was 2.7%, although lethality stands out in the state of Piauí (22.2%), followed by Pernambuco (8.4%) and Alagoas (5.6%). On average, Ceará was the state that most reported cases in the Northeast region, with 30 cases per day (minimum: 1 case; maximum: 54 cases) since the emergence of the first case in that state ( Table 1 ).
Table 1 – COVID-19 indicators by Northeast region states, Brazil, March 6th to April 1st 2020
| State | Resident population | Confirmed cases | Deaths | Lethality (%) | Incidence (100,000 inhab.) | DCIa | Days since first confirmed case |
|---|---|---|---|---|---|---|---|
| Ceará | 9,132,078 | 444 | 8 | 1,8 | 4,9 | 29,6 | 15 |
| Bahia | 14,873,064 | 246 | 2 | 0,8 | 1,7 | 9,5 | 26 |
| Pernambuco | 9,557,071 | 95 | 8 | 8,4 | 1,0 | 4,8 | 20 |
| Rio Grande do Norte | 3,506,853 | 92 | 2 | 2,2 | 2,6 | 4,8 | 19 |
| Maranhão | 7,075,181 | 52 | 1 | 1,9 | 0,7 | 4,7 | 11 |
| Paraíba | 4,018,127 | 20 | 1 | 5,0 | 0,5 | 1,5 | 13 |
| Sergipe | 2,298,696 | 20 | - | - | 0,9 | 1,2 | 17 |
| Alagoas | 3,337,357 | 18 | 1 | 5,6 | 0,5 | 0,8 | 24 |
| Piauí | 3,273,227 | 18 | 4 | 22,2 | 0,5 | 1,5 | 12 |
| Total | 57,071,654 | 1.005 | 27 | 2,7 | 1,8 | 38,7 | 26 |
Source: Brazilian Ministry of Health. Coronavirus Panel. Access on: 2020 Apr 02.
a) DCI: daily cumulative index (cumulative cases/number of days between 1stconfirmed case and April 1st2020).
Cumulative cases in the Northeast region and in the states with highest reported COVID-19 cases are shown in Figure 2 . Exponential growth as the days go by can be seen on a larger scale in the states of Ceará (444) and Bahia (246), followed by the states of Pernambuco (95) and Rio Grande do Norte (92). Ceará had the highest index (4.9/100,000 inhab.).
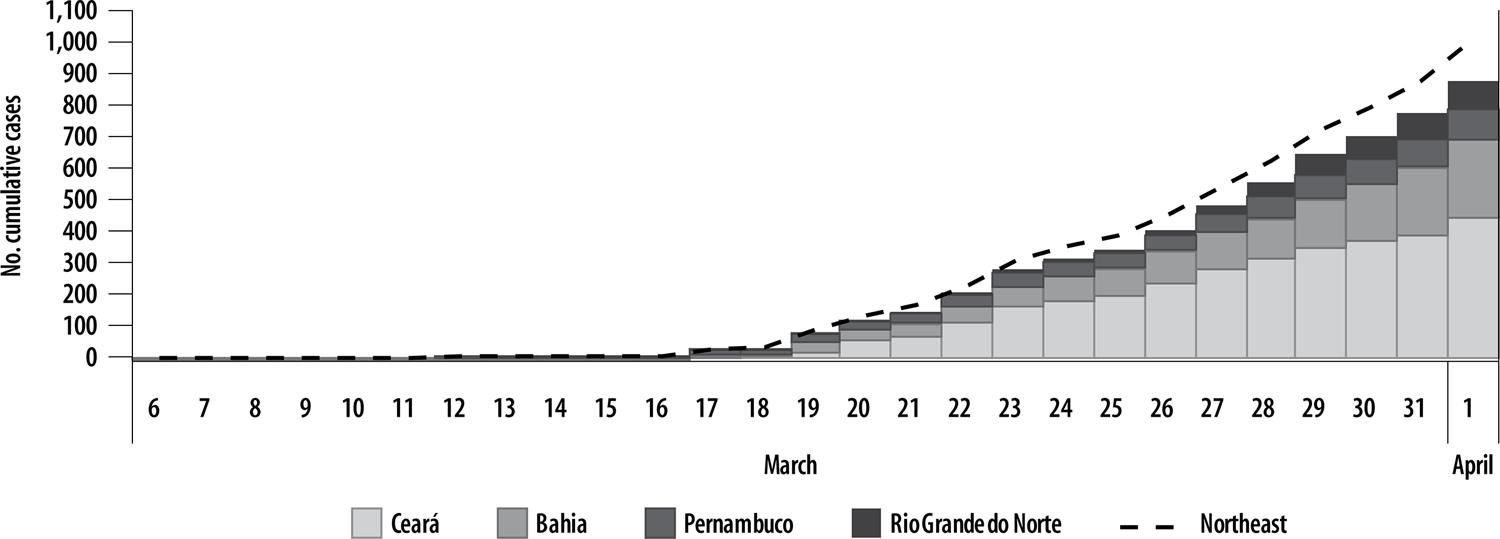
Source: Brazilian Ministry of Health. Coronavirus Panel. Access on: 2020 Apr 02.
Figure 2 – Evolution of cumulative COVID-19 cases in the Northeast region and states with highest occurrence, March 6th to April 1st 2020
The ICU bed ratio per number of inhabitants is shown in Table 2 . The ratio was less than 1 in the majority of the states. Only Pernambuco, Rio Grande do Norte and Paraíba had better distribution in the ICU bed per resident population.
Table 2 – Distribution of intensive care units (ICU) beds in the Northeast region states, March 6th to April 1st 2020
| State | Resident population | ICU beds | Total ICU bed ratiob | |
|---|---|---|---|---|
|
| ||||
| Total beds | SUSabeds | |||
| Ceará | 9,132,078 | 802 | 430 | 0.88 |
| Bahia | 14,873,064 | 1,478 | 774 | 0.99 |
| Pernambuco | 9,557,071 | 1,408 | 755 | 1.47 |
| Rio Grande do Norte | 3,506,853 | 431 | 211 | 1.23 |
| Maranhão | 7,075,181 | 572 | 303 | 0.81 |
| Paraíba | 4,018,127 | 454 | 290 | 1.13 |
| Sergipe | 2,298,696 | 241 | 146 | 1.05 |
| Alagoas | 3,337,357 | 299 | 176 | 0.90 |
| Piauí | 3,273,227 | 277 | 140 | 0.85 |
| Total | 57,071,654 | 5,962 | 3,225 | 1.04 |
Source: Brazilian Ministry of Health. Coronavirus Panel. Access on: 2020 Apr 02.
a) SUS: Brazilian National Health System
b) Per 10,000 inhabitants
Discussion
The results show that the initial evolution of the COVID-19 epidemic occurred in distinct ways in the states of the Northeast region. During the study period, more than 1,000 COVID-19 cases were confirmed in the Northeast. The epidemic began in Bahia and the first death was reported in Pernambuco. It must be highlighted that the region does not have sufficient structure to withstand the epidemic, as will be seen bellow.
In Brazil, the Northeast is the region with the second highest number of confirmed COVID-19 cases. Standing out in particular are the states of Ceará, Bahia, Pernambuco and Rio Grande do Norte. The Northeastern states, and nearly all their capital cities, are home to the main tourist destinations that attract visitors from all over Brazil and from other countries. The flow of tourists to this region in the high season, including the Christmas, New Year and Carnival holiday periods, may have contributed to the introduction of SARS-Cov-2 and its subsequent dissemination. Although the first COVID-19 cases were recorded with effect from March, it is probable that contamination occurred at least 14 days before this, coinciding with the large flow of tourists in airports, coach stations and places with large gatherings of people typical of Carnival.
Large-scale novel coronavirus transmission in Brazil will occur in the next months (with its peak in April or May), when a large part of the population living in large urban centers will be exposed to the virus.9 However, due to the country’s continental dimensions and climatic diversity (temperate, subtropical and equatorial areas), distinct patterns of viral seasonality in the country’s different regions can be identified.11
Although lethality found for cases in the Northeast region as a whole is lower than the average estimated by WHO, namely 3.4%,1 the majority of the Northeastern states recorded lethality above the Brazilian average (5.4%), principally in the states of Piauí and Pernambuco. This suggests lack of adequate capacity to provide health care to initial cases, whether this be due to shortcomings with regard to suspected cases, case reporting, laboratory diagnosis or equipment for timely intensive care; furthermore, testing coverage is low.
Only 153,961 tests investigating severe acute respiratory syndrome (SARS) had been performed in Brazil as at April 7th2020, with the aim of identifying SARS-CoV-2, influenza virus, syncytial virus and other respiratory viruses. Of the tests performed, 62,985 then underwent specific investigation for SARS-CoV-2, and 13,717 results were positive. Coronavirus tests began to be performed in Brazil on February 16thin public and private laboratories.12 Among confirmed COVID-19 cases, 5% to 10% will progress to respiratory insufficiency and will therefore need hospital care.13
As at April 1st2020, Brazil had 2.80 ICU beds specifically for COVID-19 hospitalizations per 10,000 inhab., this ratio being lower than that found in countries such as the United Kingdom, Italy and France.14 However, most of these beds are concentrated in the Southeast region of the country. Availability of ICU beds in the Northeast region (1.04/10,000 inhab.) was below the average ratio and the number of beds needs to be increased. Availability of ICU beds and mechanical ventilators needed for severe cases hospitalized as a result of novel coronavirus infection is of clear concern, as is the availability of specific diagnosis tests for early detection of the virus and prevention of subsequent transmission.10
In the face of this new reality, the MoH created the National Contingency Plan for Human Infection by Novel Coronavirus, to meet the demand in the face of a possible epidemic and define the level of response and corresponding command structure to be set up at each response level. As such, the MoH recommends that the Municipal and State Health Departments and Federal Government Health Services, as well as public and private health services, agencies and companies, use the plan as a reference for preparing their own individual contingency plans and response measures.3 Following the recommendation, all the Brazilian states prepared their plans which had the following elements in common: classification of emergency on three response levels (1-alert; 2-imminent danger; and 3-public health emergency), whereby each level is to be established based on assessment of the type of COVID-19 risk and its impact on public health, including recommendations for surveillance, laboratory support, infection control, risk communication and management.3
By the beginning of April 2020, Ceará had the highest number of registered cases. This fact may be related to investment and increased COVID-19 rapid testing in Fortaleza, the state capital, and in the interior of the state.15 In addition, Ceará is a tourist destination and is visited by thousands of people from a variety of places. The state had 110 basic isolation beds in hospital units, 93 of which were SUS beds, spread over 53 health establishments. It also had 1,475 mechanical ventilators, of which 1,337 were in use, available in 145 health establishments.16 As at April 1st2020, the number of beds was sufficient to meet the demand arising from severe cases. However, if the number of confirmed daily cases continues to rise in the same proportion, the health system will not be capable of meeting the population’s needs in a short space of time.
Bahia, the state with the highest number of confirmed cases, had three hospitals with coronavirus services, 190 clinical beds and ICU 161 beds, with capacity to include a further 200 clinical beds and 83 ICU beds.17 In addition, the state government requested law court authorization to temporarily open two more hospitals, with an estimated additional 139 clinical beds and 80 ICU beds. Two further hospitals are planned to be opened in the interior region of the state, one in the city of Lauro de Freitas with 100 clinical beds, and the other in Feira de Santana with 40 ICU beds. Two more health establishments in the state will be adapted for tents or new beds to be assembled, totaling a further 200 clinical beds.18 In view of the increase in the number of cases, the state will really need to fulfill these proposals.
The states of Pernambuco and Rio Grande do Norte have the same DCI, although the population of Rio Grande do Norte is only slightly more than a third of the population of Pernambuco. During the period analyzed, the number of confirmed cases in Pernambuco remained stable. In Pernambuco, the referral units for suspected COVID-19 cases will be defined as the response levels are reviewed. As such, on level 1, three hospitals will provide care to adults, children and pregnant women. Level 2 is characterized by an increase of 10 ICU beds. On Level 3, the referral services will be expanded to include a further three hospitals and the number of clinical and ICU beds will be increased in the hospitals. Since the beginning of the epidemic, the state has been reorganizing its health service structure to meet the population’s needs.19 With effect from the occurrence of the first COVID-19 cases in Pernambuco, the state government has made 353 additional hospital beds available (113 ICU beds and 220 clinical beds), and intends to increase even more the number of beds. In support of the referral units, health service managers have confirmed the use of a maternity hospital with 120 beds, 40 of which are ICU beds, as well as the purchase of a hospital in the state capital which will provide 230 beds, of which 100 are ICU beds.20
As at the beginning of April 2020, the state of Rio Grande do Norte had two referral hospitals and a further 11 Public State Hospitals had been prepared to care for COVID-19 cases and to be used as referral hospitals as well. This means that 1,229 clinical beds and 76 ICU beds will be made available. A further 47 ICU beds were to be brought into operation. All health services in the state had been sensitized and prepared to provide initial care to people suspected of having COVID-19.21
The state of Maranhão has the fifth largest number of cases. Health services have been organized so that suspected cases can receive care at primary health care centers, emergency care centers, mixed centers, as well as public and private hospitals. Severe cases will be referred to hospitals with capacity to provide care to cases of severe respiratory infections, in accordance with standard precaution measures. Two state-level emergency care centers have been designated as preferential walk-in services for suspected cases. The state has two referral hospitals and one standby hospital for severe adult and child cases.22
The states of Paraíba and Sergipe had the same number of diagnosed cases, despite the population of Paraíba being much larger than that of Sergipe. The Paraíba health care network is comprised of 1,441 Family Health teams, 17 emergency care centers and 32 state-managed hospitals and two federal hospitals. It has two referral hospitals for suspected cases, one of which specializes in child care.23
In the state of Sergipe, suspected cases are detected by screening at health services, both in the state capital and the interior region of the state. Mild cases are to be monitored by Primary Health Care involving home and social isolation precaution measures. Severe cases are to be referred to one of three hospitals available for isolation and treatment as per the state hospital admission control system. In addition, non-severe cases requiring hospitalization identified in health services other than hospitals and/or which are not able to admit them, will be sent to a referral hospital by the Urgent Care Admission Control System.24
The states of Alagoas and Piauí had the same number of confirmed cases and similar resident populations. In Alagoas, mild cases will be attended to by Primary Health Care services, which cover 81.42% of the state’s population. The state has 265 ICU beds registered, of which almost 70% are SUS beds, as well as 56 pediatric ICU beds. Severe cases will be attended to by 12 Emergency Care Centers located in nine municipalities. This is not enough to meet possible emergency demands due to COVID-19; as such, the State Health Department is in the process of making available a further 100 adult and pediatric ICU beds.25
Piauí stands out as the state with the lowest number of confirmed cases and highest lethality in the Northeast region. There are no official data about the exact number of tests performed to diagnose COVID-19 in the state. However, there is reason to believe that there are not sufficient diagnosis test kits in relation to the size of the population, given that the Federal Government has only donated 7,260 rapid tests and 4,180 RT-PCR tests to the state of Piauí.13 As such, the high lethality rate may not be reflecting the true situation of the epidemic in the state. The Piauí State Health Department has been mobilized in the sense of developing prevention, control and care actions, with Primary Health Care services and/or hospital care services as the entry point for patients. There is one state-level referral hospital for COVID-19. If the MOH declares imminent risk and WHO declares an international health emergency, the state will adapt to expand hospital services to the regional hospitals in its 11 health territories, with a further 14 standby or walk-in hospitals and referral hospitals.26
At the beginning of the epidemic, the MOH announced that it was arranging a procurement process in order to allocate 1,000 additional beds in referral hospitals indicated by the states for possible COVID-19 cases. It was also announced that a notice to tender had been published for the purchase of personal protective equipment for health workers – such as surgical masks, face protectors, head caps, N95 masks and gloves –, as well as other supplies.10
It should be noted that all measures adopted are to be based on the best available evidence publicized by renowned institutions and professionals in the area.27 Coronavirus transmission reduction in China occurred mainly through the adoption of three essential measures: protecting health workers with personal protective equipment; identifying symptomatic individuals, by testing and providing test results rapidly; and isolating conformed cases, as well as identifying contacts and imposing quarantine or social distancing.28
Scientific evidence currently available is still insufficient to enlighten all aspects of COVID-19 in Northeast Brazil, as well as in other regions of the country and the world, and this is a limitation of this study. The data presented here refer to the initial period of the epidemic in this region, and continuous monitoring is needed in order to obtain more information and better characterization of the natural history of the disease and the health system’s capacity to cope.
In conclusion, the indicators analyzed suggest heterogeneity in the characterization and evolution of the first COVID-19 cases in the Northeast Brazilian states and make evident the insufficiency of hospital beds for containing the epidemic. Although the indicators provide important input for health management, efforts need to be directed to increasing the capacity of epidemiological surveillance and health care delivery, principally with regard to timely diagnosis and adequate treatment. Moreover, we highlight the importance of providing personal protective equipment to all health workers, and raising the awareness of society as to adopting prevention measures, especially social distancing.
REFERENCES
1. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde - SAPS. Protocolo de manejo clínico do coronavírus (covid-19) na atenção primária à saúde [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 mar 28]. 40 p. Disponível em: https://www.unasus.gov.br/especial/covid19/pdf/37 [ Links ]
2. Ministério da Saúde (BR). Manejo de corpos no contexto do novo coronavírus: COVID-19 [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 abr 01]. 16 p. Disponível em: https://www.saude.gov.br/images/pdf/2020/marco/25/manejo-corpos-coronavirus-versao1-25mar20-rev5.pdf [ Links ]
3. Ministério da Saúde (BR). Fundação Oswaldo Cruz. Plano de contingência da Fiocruz diante da pandemia da doença pelo SARS-CoV-2 (Covid-19) [Internet]. Brasília: Fundação Oswaldo Cruz; 2020 [citado 2020 abr 1]. 8 p. Disponível em: https://portal.fiocruz.br/sites/portal.fiocruz.br/files/documentos/plano_de_contingencia_corona_final_2020-03-13_v1.pdf [ Links ]
4. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med [Internet]. 2020 Apr [cited 2020 May 6];382:1708-20. Available from: https://doi.org/10.1056/NEJMoa2002032 [ Links ]
5. Lima-Costa MF, Barreto SM. Types of epidemiologic studies: basic concepts and uses in the area of aging. Epidemiol Serv Saúde [Internet]. 2003 dez [citado 2020 maio 6];12(4):189-201. Disponível em: http://dx.doi.org/10.5123/S1679-49742003000400003 [ Links ]
6. Instituto Brasileiro de Geografia e Estatística - IBGE. Pesquisa nacional por amostra de domicílios contínua - PNAD Contínua [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2020 [citado2020 abr 12]. Disponível em: https://www.ibge.gov.br/estatisticas/sociais/educacao/9171-pesquisa-nacional-por-amostra-de-domicilios-continua-mensal.html?edicao=19757&t=destaques [ Links ]
7. Ministério da Saúde (BR). Fundação Oswaldo Cruz. Projeto Avaliação do Desempenho do Sistema de Saúde (PROADESS). Boletim informativo: monitoramento da assistência hospitalar no Brasil (2009-2017) [Internet]. Brasília: Projeto Avaliação do Desempenho do Sistema de Saúde; 2019 [citado 2020 abr 29]. 26 p. Disponível em: https://www.proadess.icict.fiocruz.br/Boletim_4_PROADESS_Monitoramento%20da%20assistencia%20hospitalar_errata_1403.pdf [ Links ]
8. Ministério da Saúde (BR). Painel coronavírus [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 abr 1]. Disponível em: https://covid.saude.gov.br/ [ Links ]
9. Ministério da Saúde (BR). Centro de Operações de Emergências em Saúde Pública | COE-COVID-19. Plano de contingência nacional para infecção humana pelo novo coronavírus COVID-19 [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 abr 2]. 24 p. Disponível em: https://portalarquivos2.saude.gov.br/images/pdf/2020/fevereiro/13/plano-contingencia-coronavirus-COVID19.pdf [ Links ]
10. Croda JHR, Garcia LP. Respuesta inmediata de la vigilancia en salud a la epidemia de COVID-19. Epidemiol Serv Saúde [Internet]. 2020 mar [citado 2020 abr 6];29(1):e2020002. Disponível em: https://doi.org/10.5123/s1679-49742020000100021 [ Links ]
11. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Portaria MS/GM nº 116, de 11 de fevereiro de 2009. Regulamenta a coleta de dados, fluxo e periodicidade de envio das informações sobre óbitos e nascidos vivos para os Sistemas de Informações em Saúde sob gestão da Secretaria de Vigilância em Saúde [Internet]. Diário Oficial da União, Brasília (DF), 2009 fev 11 [citado 2020 abr 1]. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/svs/2009/prt0116_11_02_2009.html [ Links ]
12. Ministério da Saúde (BR). Painel de casos de doença pelo coronavírus 2019 (COVID-19) no Brasil pelo Ministério da Saúde [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 abr 11]. Disponível em: https://covid.saude.gov.br/ [ Links ]
13. Ministério da Saúde (BR). Saúde já distribuiu quase 1 milhão de testes para coronavírus [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 abr 11]. Disponível em: https://www.saude.gov.br/noticias/agencia-saude/46707-saude-ja-distribuiu-quase-1-milhao-de-testes-para-coronavirus [ Links ]
14. Ministério da Saúde (BR). Doença pelo coronavírus 2019. Bol Epidemiol [Internet]. 2020 abr [citado 2020 abr 10];8:1-41. Disponível em: https://www.saude.gov.br/images/pdf/2020/April/09/be-covid-08-final.pdf [ Links ]
15. Secretaria de Saúde do Estado do Ceará. Secretaria da Saúde do Ceará anuncia novas estratégias para o combate à doença [Internet]. Fortaleza: Secretaria de Saúde do Estado do Ceará; 2020 [citado 2020 abr 10]. Disponível em: https://www.saude.ce.gov.br/2020/04/06/secretario-da-saude-do-ceara-anuncia-novas-estrategias-para-o-combate-a-doenca__trashed-2/ [ Links ]
16. Secretaria de Saúde do Estado do Ceará. Plano estadual de contingência para resposta às emergências em saúde pública: novo coronavírus (2019-nCoV) [Internet]. Fortaleza: Secretaria de Saúde do Estado do Ceará; 2020 [citado 2020 abr 10]. 70 p. Disponível em: https://www.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-CEAR---EM-REVIS--O.pdf [ Links ]
17. Secretaria de Saúde do Estado da Bahia. Plano estadual de contingências para enfrentamento do novo coronavírus - 2019-n CoV [Internet]. Salvador: Secretaria de Saúde do Estado da Bahia; 2020 [citado 2020 abr 2]. 16 p. Disponível em: https://portalarquivos.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-BAHIA-EM-REVIS--O.pdf [ Links ]
18. Secretaria de Saúde do Estado da Bahia. Entenda o planejamento do Governo do Estado para atender os baianos em caso de contaminação por coronavírus [Internet]. Salvador: Secretaria de Saúde do Estado da Bahia; 2020 [citado 2020 abr 1]. Disponível em: http://www.saude.ba.gov.br/2020/03/27/entenda-o-planejamento-do-governo-do-estado-para-atender-os-baianos-em-caso-de-contaminacao-por-coronavirus/ [ Links ]
19. Secretaria de Saúde do Estado de Pernambuco. Plano de contingência para infecção humana pelo novo coronavírus (2019-nCoV) [Internet]. Recife: Secretaria de Saúde do Estado de Pernambuco; 2020 [citado 2020 abr 10]. Disponível em: https://www.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-PERNAMBUCO-EM-REVIS--O.pdf [ Links ]
20. Secretaria de Saúde do Estado de Pernambuco. Pernambuco contra a COVID-19: medidas governamentais [Internet]. Recife: Secretaria de Saúde do Estado de Pernambuco; 2020 [citado 2020 abr 10]. Disponível em: https://www.pecontracoronavirus.pe.gov.br/ [ Links ]
21. Secretaria de Saúde do Estado do Rio Grande do Norte. Plano de contingência estadual para infecção humana pelo novo coronavírus 2019-nCoV [Internet]. Natal: Secretaria de Saúde do Estado do Rio Grande do Norte; 2020 [citado 2020 abr 10]. 20 p. Disponível em: https://www.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-RIO-GRANDE-DO-NORTE-EM-REVIS--O.pdf [ Links ]
22. Secretaria de Saúde do Estado do Maranhão. Plano de contingência para o 2019-nCov no Maranhão [Internet]. São Luís: Secretaria de Saúde do Estado do Maranhão; 2020 [citado 2020 abr 10]. Disponível em: https://saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-MARANH--O-EM-REVIS--O.pdf [ Links ]
23. Secretaria de Saúde do Estado da Paraíba. Plano de contingência estadual para infecção humana pelo novo coronavírus (2019- nCoV) [Internet]. João Pessoa: . Secretaria de Saúde do Estado da Paraíba; 2020 [citado 2020 abr 11]. 40 p. Disponível em: https://portalarquivos2.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-PARAIBA-EM-REVIS--O.pdf [ Links ]
24. Secretaria de Saúde do Estado de Sergipe. Plano de contingência estadual para infecção humana pelo novo coronavírus 2019-nCoV [Internet]. Aracaju: Secretaria de Saúde do Estado de Sergipe; 2020 [citado 2020 abr 11]. 47 p. Disponível em: https://www.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-SERGIPE-EM-REVIS--O.pdf [ Links ]
25. Secretaria de Saúde do Estado de Alagoas. Plano de contingência estadual para infecção humana pelo novo coronavírus 2019-nCoV [Internet]. Maceió: Secretaria de Saúde do Estado de Alagoas; 2020 [citado 2020 abr 11]. 21 p. Disponível em: https://www.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-ALAGOAS-EM-REVIS--O.pdf [ Links ]
26. Secretaria de Saúde do Estado do Piauí. Plano estadual de contingência para enfretamento da infecção humana pelo coronavírus (2019-nCov) do Estado do Piauí [Internet]. Teresina: Secretaria de Saúde do Estado do Piauí; 2020 [citado 2020 abr 11]. 33 p. Disponível em: https://portalarquivos.saude.gov.br/images/pdf/2020/fevereiro/13/PLANO-DE-CONTINGENCIA-novo-coronavirus-PIAUI-EM-REVIS--O.pdf [ Links ]
27. Silva AAM. Sobre a possibilidade de interrupção da epidemia pelo coronavírus (COVID-19) com base nas melhores evidências científicas disponíveis. Rev Bras Epidemiol [Internet]. 2020 mar [citado 2020 maio 6];23:e200021. Disponível em: https://doi.org/10.1590/1980-549720200021 [ Links ]
28. World Health Organization - WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) [Internet]. Geneva: World Health Organization; 2020 [citado 2020 abr 10]. 40 p. Disponível em: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf [ Links ]
Associate editor: Bárbara Reis Santos – orcid.org/0000-0001-6952-0352
Received: April 24, 2020; Accepted: May 05, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
