










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.3 Brasília jun. 2020 Epub 15-Jun-2020
http://dx.doi.org/10.5123/s1679-49742020000300015
Original article
Food consumption and multimorbidity among non-institutionalized elderly people in Pelotas, 2014: a cross-sectional study *
1Universidade Federal de Pelotas, Faculdade de Nutrição, Pelotas, RS, Brazil
2Universidade Federal de Pelotas, Programa de Pós-Graduação em Epidemiologia, Pelotas, RS, Brazil
3Universidade Católica de Pelotas, Programa de Pós-Graduação em Saúde e Comportamento, Pelotas, RS, Brazil
4Secretaria Municipal de Saúde, Prefeitura Municipal de Pelotas, Pelotas, RS, Brazil
Methods
this was a cross-sectional study of elderly people aged 60 years or older in Pelotas, RS, Brazil, 2014; food consumption was assessed using an abridged Food Frequency Questionnaire; diet quality according to the diet quality index (DQI-E) and scores given to food items; multimorbidity (≥5 diseases) was self-reported; Poisson Regression was used to obtain crude and adjusted prevalence ratios and 95% confidence intervals.
Results
1,426 elderly people were included; men who consumed wholefoods (1 to 6 days) were more likely to have multimorbity (PR=1.64 95%CI 1.21;2.23]); those who ate meat at least weekly were less likely to have multimorbity (PRmen=0.68 95%C I0.51;0.92]; PRwomen=0.70 95%CI 0.61;0.81); no association was found between DQI-E and multimorbidity.
Conclusion
although consumption of most foods was not associated with multimorbidity, the results have produced reflections about dietary habits that are pertinent for discussion by health service managers
Key words: Food Consumption; Chronic Disease; Elderly; Cross-Sectional Studie
Introduction
Aging is characterized by a dynamic and progressive process of morphological, functional, biochemical and psychological changes. Among these changes, progressive loss of ability to adapt to the environment leads to greater vulnerability and occurrence of diseases, such as chronic non-communicable diseases (NCDs).1
Simultaneous occurrence of NCDs in the same person, known as multimorbidity, has become relevant due to population aging, increased NCD prevalence and the importance of modifiable associated factors, such as food intake.2 However, it is not clear whether the occurrence of one disease influences the appears of others (comorbidities), or whether all morbidities are a clinical expression of the aging process.4 As such, only the number of coexisting diseases has been considered when diagnosing multimorbidity.5
According to the World Health Organization (WHO), presence of multimorbidity is more frequent among individuals who are 60 years old or more6 and is related to the development of nutritional shortages or excesses.7 As such, it is essential to assess and monitor elderly people’s eating habits in relation to overall health diagnosis and comorbidity incidence,3 given that a healthy diet is one of the main determinants of healthy aging and, therefore, is capable of prolonging survival and providing better quality of life.9
When taking into consideration the health status of each individual, it is known that there are characteristics inherent to the aging process that hinder good diet, such as dysphagia, xerostomia, tooth loss, functional disability and depression.10 These changes can cause reduced consumption of some types of food such as meat, fruit, raw greens and vegetables, resulting in inadequate intake of fibers, vitamins and minerals13 and, consequently, a poorer diet.
The objective of this study was to analyze association between diet quality and occurrence of multimorbidity among community non-institutionalized elderly people living in the urban area of the city of Pelotas, state of Rio Grande do Sul (RS), Brazil, in 2014.
Methods
This was a cross-sectional population-based study with a representative sample of elderly people living in the urban area of Pelotas, RS, a municipality with 365,696 inhabitants.14 The municipality’s gross domestic product (GDP) is estimated to be BRL 17,353.15 per capita; and its human development index (HDI-M) is 0.739.14 In 2010, 14% of the population of Pelotas was elderly: 46,099 individuals aged 60 or over.14 The data used is this study were provided by the Guided Master’s Degree Consortium for Valuing Care of the Elderly (‘COMO VAI?’ study), conducted between January and August 2014.
Elderly people living in the urban area of Pelotas were eligible to take part. Institutionalized elderly people were excluded (i.e. those who were hospitalized, living in long-stay institutions or imprisoned) and those who had mental or cognitive disability preventing them from answering the questionnaire in the absence of a family member or carer. Elderly people undergoing enteral or parenteral nutrition were also excluded. The interviews were conducted at the homes of the elderly, by interviewers trained in standard anthropometric measurement, using notebooks to record the information collected.
The sample size calculated for the ‘COMO VAI?’ study estimated that 1,649 elderly people would need to be interviewed, plus a further 10% to compensate for possible refusals and losses. The sample size was estimated for 50% outcome prevalence (corresponding to maximum variability), a 95% confidence interval, a sample error of four percentage points and a 1.5 design effect. After adding 10% for losses and refusals, it was estimated that at least 990 elderly people would need to be studied.
The sampling process took place in two stages. Firstly, taking the Brazilian Institute of Geography and Statistics (IBGE) map for 2012,14 the 488 census tracts in the urban area of Pelotas were listed, ordered according to the average income of each inhabitant. The second stage of the sampling process consisted of selecting the households. The total number of households in the municipality (107,152), divided by the defined number of census tracts, following a systematic strategy, resulted in a quotient of 806 households. One hundred and thirty-three census tracts were systematically selected with 31 households per tract, enabling identification of 12 elderly people in each tract (based on an estimate of 0.4 elderly people per household), resulting in 4,123 households to be visited.
Presence of multimorbidity (outcome) was assessed based on self-reported medical diagnosis during lifetime of five or more of the following health problems: arterial hypertension, diabetes, heart problems, heart failure, asthma, bronchitis, emphysema, arthritis, Parkinson’s disease, kidney failure, hypercholesterolemia, convulsions, stomach ulcer, osteoporosis, urinary incontinence, constipation, fecal incontinence, depression, glaucoma, deafness, difficulty in swallowing, insomnia, fainting, rhinitis, difficulty in speaking, stroke, mental disorders and cancer. Multimorbidity was defined as the presence of five or more diseases, based on a study already conducted with the same target population as this study.15 It should be noted that multimorbidity assessment worldwide is not uniform and that currently use of a list of at least 12 diseases is recommended for this assessment.1
Nutritional status was also assessed based on body mass index (BMI), whereby overweight and obesity were considered to be components of multimorbidity and were defined as ≥25kg/m2and ≥30kg/m2, respectively.16 Weight was measured using TANITA UM-080 scales, with capacity for 150kg and 100g precision. Knee height was measured using an Indaiá wooden stadiometer for children, with maximum measurement of 100cm and 0.1cm precision; using the equation suggested by Chumlea17 (method most recommended for the elderly) to estimate the height of each elderly person.18
Information on food consumption in the last seven days was obtained by means of an abridged Food Frequency Questionnaire (FFQ),19 prepared according to recommendations described in the version of the Food Guide for the Brazilian Population in force at the time the study was planned (2013).20 Questions were asked about consumption of the following food items: rice and beans; wholefoods (wholemeal bread, wholemeal biscuits, wholegrain rice or oats); vegetables and greens; fruit; meat; milk and milk products; confectionary, soft drinks and industrialized fruit juice; fried food; conserves, charcuterie and tinned food; frozen food; and fast food. Frequency of consumption of each food item or group was classified into four categories in relation to a one week period: did not eat; ate 1-3 days; ate 4-6 days; ate every day of the week. In the case of frozen food, fast food and meat, the information was dichotomized (did not eat; ate) considering the distribution of the proportion of consumption of the sample itself.
Apart from observing food item or group consumption frequency on its own, the quality of the elderly people’s diet was also assessed using the elderly diet quality index (DQI-E), as described in an earlier publication.19 The score ranged from 0 to 33, whereby a higher score indicated greater frequency of healthier food consumption and lower frequency of unhealthy food consumption. As such, a score varying between 0 and 3 was initially attributed. Each food item considered to be healthy was given a score that increased as consumption increased: did not consume = 0 points; consumed 1-3 days = 1 point; consumed 4-6 days = 2 points; consumed every day of the week = 3 points. Food items considered to be unhealthy were given a score using the same scale, but in reverse order: did not consume = 3 points; consumed 1-3 days = 2 points; consumed 4-6 days = 1 point; consumed every day of the week = 0 point. The total score for all the elderly people assessed using DQI-E was then divided into tertiles, as follows: 1sttertile – low quality, score between 11 and 22 –; 2ndtertile – medium quality, score between 23 and 26 –; and 3rdtertile – high quality, score between 27 and 33. DQI-E was also presented for the total sample and stratified by sex, averages and standard deviations.
The covariables used in the study were:
sex (male; female);
age (in years: 60-69; 70-79; 80 or over);
race/skin color (white; other);
economic classification (A; B; C; D; E);
schooling (in years of study: <8; ≥8);
marital status (married/lives with partner; single/no partner; separated; widowed);
alcohol consumption in the month prior to the interview (yes; no); and
current tobacco smoking (yes; no).
Sex and race/skin color (white; black, brown, yellow or indigenous) were observed and recorded by the interviewers. Economic classification was determined according to the criteria of the Brazilian Survey Companies Association (ABEP),21 by asking questions about consumer goods, whether the household had a domestic employee and head of family schooling level. According to this score, category A is considered to be the wealthiest and, at the other extreme, category E is the poorest. Schooling was self-reported. Alcohol consumption was estimated based on reported consumption of at least one dose of alcoholic beverage in the last 30 days, and smokers were defined as those who smoked at least one cigarette a day during the last 30 days.
The statistical analyses were performed using Stata (14.0). All the variables were described in absolute and relative frequencies, with their respective 95% confidence intervals (95%CI), while DQI-E was presented in averages and standard deviations, as mentioned above.
Pearson’s chi-square test was used to verify the difference between food consumption and presence of multimorbidity, without adjustment for possible confounding factors. Similarly, association between DQI-E tertiles and number of diseases (<2; 2-4; 5-6; 7 or more) was also investigated. In the adjusted analyses prevalence ratios and their respective 95%CIs were obtained using Poisson regression with adjustment for robust variance. The black box analysis model was used with a significance limit of p<0.05. The survey (svy) command was used in the analyses in view of the complex sampling procedure.
The study project was approved by the Federal University of Pelotas Faculty of Medicine Research Ethics Committee (CEP/FAMED/UFPel): Opinion No. 472.357/2013, issued on November 28th2013. Study participants signed a Free and Informed Consent form.
Results
The sampling process located 1,844 elderly people; losses and refusals accounted for 21.3% (n=393), resulting in 1,451 of them being interviewed (78.7%). Statistically, the biggest losses occurred among women (59.3%) and individuals who were 60-69 years old (59.5%). Specifically for this study, we used data on the 1,426 individuals (98.3%) who provided complete information. The majority of the sample was comprised of women (63.0%) and individuals aged between 60 and 69 (52.1%). Excess weight (BMI ≥25.0kg/m2) accounted for 65.6% of males and 68.5% females. Multimorbidity (five or more morbidities) prevalence was 60.0% for the sample as a whole, but higher in women (66.9%) than in men (47.5%) ( Table 1 ), and the most prevalent morbidities were: systemic arterial hypertension (66.7%), dyslipidemia (40.7%), depression (35.7%), constipation (32.0%), deafness (31.3%), urinary incontinence (30.1%) and diabetes (23.5%). 25.3% self-reported medical diagnosis of osteoporosis, 88.5% of whom were women (p<0.001); 41.3% reported diagnosis of arthritis, 79.3% of whom were women (p<0.001).
Table 1 – Elderly people assessed by the ‘COMO VAI?’ study according to demographic, socio-economic, health and lifestyle characteristics, Pelotas, Rio Grande do Sul, 2014
| Characteristics | Total N (%) | Males N (%) | Females N (%) | |||||
|---|---|---|---|---|---|---|---|---|
| Age (in completed years) | ||||||||
|
| ||||||||
| 60-69 | 756 (52.1) | 289 (53.8) | 467 (51.1) | |||||
| 70-79 | 460 (31.7) | 172 (32.0) | 288 (31.5) | |||||
| ≥80 | 230 (15.9) | 175 (14.0) | 155 (17.0) | |||||
| No information | 5 (0.3) | 1 (0.2) | 4 (0.4) | |||||
|
| ||||||||
| Race/skin color | ||||||||
|
| ||||||||
| White | 1.211 (83.4) | 454 (84.6) | 757 (82.8) | |||||
| Other | 236 (16.3) | 82 (15.3) | 154 (16.9) | |||||
| No information | 4(0.3) | 1 (0.2) | 3 (0.3) | |||||
|
| ||||||||
| Schooling (completed years of study) | ||||||||
|
| ||||||||
| None | 196 (13.5) | 58 (10.8) | 138 (15.1) | |||||
| <8 | 782 (53.9) | 316 (58.9) | 466 (51.0) | |||||
| ≥8 | 459 (31.6) | 159 (29.6) | 300 (32.8) | |||||
| No information | 14 (1.0) | 4 (0.7) | 10 (1.1) | |||||
|
| ||||||||
| Economic classa | ||||||||
|
| ||||||||
| A-B | 483 (33.3) | 200 (37.2) | 283 (31.0) | |||||
| C | 720 (49.6) | 248 (46.2) | 472 (51.6) | |||||
| D-E | 169 (11.7) | 60 (11.2) | 109 (11.9) | |||||
| No information | 79 (5.4) | 29 (5.4) | 50 (5.5) | |||||
|
| ||||||||
| Marital status | ||||||||
|
| ||||||||
| Married/lives with partner | 763 (52.6) | 408 (76.0) | 355 (38.8) | |||||
| Single/no partner | 91 (6.3) | 21 (3.9) | 70 (7.7) | |||||
| Separated | 134 (9.2) | 37 (6.9) | 97 (10.6) | |||||
| Widowed | 459 (31.6) | 70 (13.0) | 389 (42.6) | |||||
| No information | 4 (0.3) | 1 (0.2) | 3 (0.3) | |||||
|
| ||||||||
| Nutritional status (BMI)b | ||||||||
|
| ||||||||
| Low weight | 25 (1.7) | 9 (1.7) | 16 (1.8) | |||||
| Normal weight | 360 (24.8) | 140 (26.1) | 220 (24.1) | |||||
| Overweight | 571 (39.4) | 232 (43.2) | 339 (37.0) | |||||
| Obese | 408 (28.1) | 120 (22.4) | 288 (31.5) | |||||
| No information | 87 (6.0) | 36 (6.7) | 51 (5.6) | |||||
|
| ||||||||
| Alcohol consumption | ||||||||
|
| ||||||||
| No | 1,138 (78.4) | 374 (69.6) | 764 (83.6) | |||||
| Yes | 307 (21.2) | 161 (30.0) | 146 (16.0) | |||||
| No information | 6 (0.4) | 2 (0.4) | 4 (0.4) | |||||
|
| ||||||||
| Tobacco smoking | ||||||||
|
| ||||||||
| No | 1,264 (87.1) | 460 (85.7) | 804 (88.0) | |||||
| Yes | 182 (12.5) | 76 (14.2) | 106 (11.6) | |||||
| No information | 5 (0.4) | 1 (0.2) | 4 (0.4) | |||||
|
| ||||||||
| Number of diseases | ||||||||
|
| ||||||||
| 0-4 | 473 (32.6) | 238 (44.3) | 235 (25.7) | |||||
| ≥5 | 866 (60.0) | 255 (47.5) | 611 (66.9) | |||||
| No information | 112 (7.7) | 44 (8.2) | 68 (7.4) | |||||
|
| ||||||||
| DQI-Ec(Mean and SD)d | 24.2 (3.8) | 23.5 (3.8) | 24.6 (3.7) | |||||
|
| ||||||||
| No information | 25 | 7 | 18 | |||||
a) Criterion used based on Brazilian Survey Companies Association (ABEP).(19)
b) BMI: body mass index.
c) DQI-E: elderly diet quality index.
d) SD: standard deviation.
Note: Estimates corrected for sample design effect.
Table 2 shows the description of the participants’ food consumption by sex. Daily consumption of the majority of food items in the healthy food group differed between men and women, except for meat consumption. Only daily frequency of rice and bean consumption was greater among men in relation to women (49.5% and 37.6%, respectively; p<0.001); all the other food items were consumed more daily by women. With regard to the unhealthy food group, men consumed more fried food (2.8%) and conserves/charcuterie/tinned food (4.5%).
Table 2 – Frequency of food consumption in the seven days prior to interviewing elderly community members taking part in the ‘COMO VAI?’ study (n=1,451), Pelotas, Rio Grande do Sul, 2014
| Food consumption | Total N (%) | Males N (%) | Females N (%) | p-valuea |
|---|---|---|---|---|
| Healthy food | ||||
|
| ||||
| Rice and beans | <0.001 | |||
|
| ||||
| Did not eat | 141 (9.7) | 40 (7.5) | 101 (11.0) | |
| 1-3 days | 269 (18.5) | 67 (12.5) | 202 (22.1) | |
| 4-6 days | 418 (28.8) | 160 (29.8) | 258 (28.2) | |
| Every day | 610(42.0) | 266 (49.5) | 344 (37.6) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Vegetables and greens | <0.001 | |||
|
| ||||
| Did not eat | 132 (9.1) | 71 (13.2) | 61 (6.7) | |
| 1-3 days | 491 (33.8) | 179 (33.3) | 312 (34.1) | |
| 4-6 days | 326 (22.5) | 120 (22.4) | 206 (22.5) | |
| Every day | 489 (33.7) | 163 (30.4) | 326 (35.6) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Fruit | 0.001 | |||
|
| ||||
| Did not eat | 97 (6.7) | 44 (8.2) | 53 (5.8) | |
| 1-3 days | 322 (22.2) | 145 (27.0) | 177 (19.4) | |
| 4-6 days | 315 (21.7) | 112 (20.9) | 203 (22.2) | |
| Every day | 704 (48.5) | 232 (43.2) | 472 (51.6) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Milk and milk products | <0.001 | |||
|
| ||||
| Did not eat | 233 (16.1) | 116 (21.6) | 117 (12.8) | |
| 1-3 days | 237 (16.3) | 93 (17.3) | 144 (15.8) | |
| 4-6 days | 189 (13.0) | 62 (11.6) | 127 (13.9) | |
| Every day | 779 (53.7) | 262 (48.8) | 517 (56.6) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Wholefoodsb | <0.001 | |||
|
| ||||
| Did not eat | 907 (63.1) | 373 (69.5) | 534 (58.4) | |
| 1-3 days | 153 (10.6) | 49 (9.1) | 104 (11.4) | |
| 4-6 days | 93 (6.5) | 29 (5.4) | 64 (7.0) | |
| Every day | 285 (19.8) | 82 (15.3) | 203 (22.2) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Meat | 0.302 | |||
|
| ||||
| Did not eat | 14 (1.0) | 6 (1.1) | 8 (0.9) | |
| Ate | 1424 (98.1) | 527 (98.1) | 897 (98.1) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Unhealthy food | ||||
|
| ||||
| Confectionary, soft drinks and industrialized fruit juice | 0.349 | |||
|
| ||||
| Did not eat | 438 (30.2) | 149 (27.8) | 289 (31.6) | |
| 1-3 days | 422 (29.1) | 163 (30.4) | 259 (28.3) | |
| 4-6 days | 161 (11.1) | 57 (10.6) | 104 (11.4) | |
| Every day | 417 (28.7) | 164 (30.5) | 253 (27.7) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Fried food | <0.001 | |||
|
| ||||
| Did not eat | 827 (57.0) | 260 (48.4) | 567 (62.0) | |
| 1-3 days | 545 (37.6) | 231 (43.0) | 314 (34.4) | |
| 4-6 days | 45 (3.1) | 27 (5.0) | 18 (2.0) | |
| Every day | 21 (1.5) | 15 (2.8) | 6 (0.7) | |
| No information | 13 (0.9) | 4 (0.7) | 9 (1.0) | |
|
| ||||
| Conserves, charcuterie and tinned food | <0.001 | |||
|
| ||||
| Did not eat | 915 (63.1) | 300 (55.9) | 615 (67.2) | |
| 1-3 days | 392 (27.0) | 172 (32.0) | 220 (24.1) | |
| 4-6 days | 64 (4.4) | 34 (6.3) | 30 (3.3) | |
| Every day | 55 (3.8) | 24 (4.5) | 31 (3.4) | |
| No information | 25 (1.7) | 7 (1.3) | 18 (2.0) | |
|
| ||||
| Frozen food | 0.318 | |||
|
| ||||
| Did not eat | 1323 (91.2) | 487 (90.7) | 836 (91.5) | |
| Ate | 103 (7.1) | 43 (8.0) | 60 (6.6) | |
| No information | 25 (1.7) | 7 (1.3) | 18 (2.0) | |
|
| ||||
| Fastfood | 0.287 | |||
|
| ||||
| Did not eat | 1344 (92.6) | 495 (92.2) | 849 (94.7) | |
| Ate | 82 (5.7) | 35 (6.5) | 47 (5.3) | |
| No information | 25 (1.7) | 7 (1.3) | 18 (2.0) | |
a) Pearson’s chi-square test, to check food consumption comparison between men and women.
b) Wholefoods were considered to be: wholemeal bread, wholemeal biscuits, wholegrain rice or oats.
Note: N = 1,451; males = 357 and females = 914.
In relation to DQI-E, average score was 24.2 points, with standard deviation (SD) = 3.8 points in the study sample ( Table 1 ). There was no statistically significant association between DQI-E tertiles and number of diseases, both in men (p=0.513) and women (p=0.674) ( Figure 1 ).
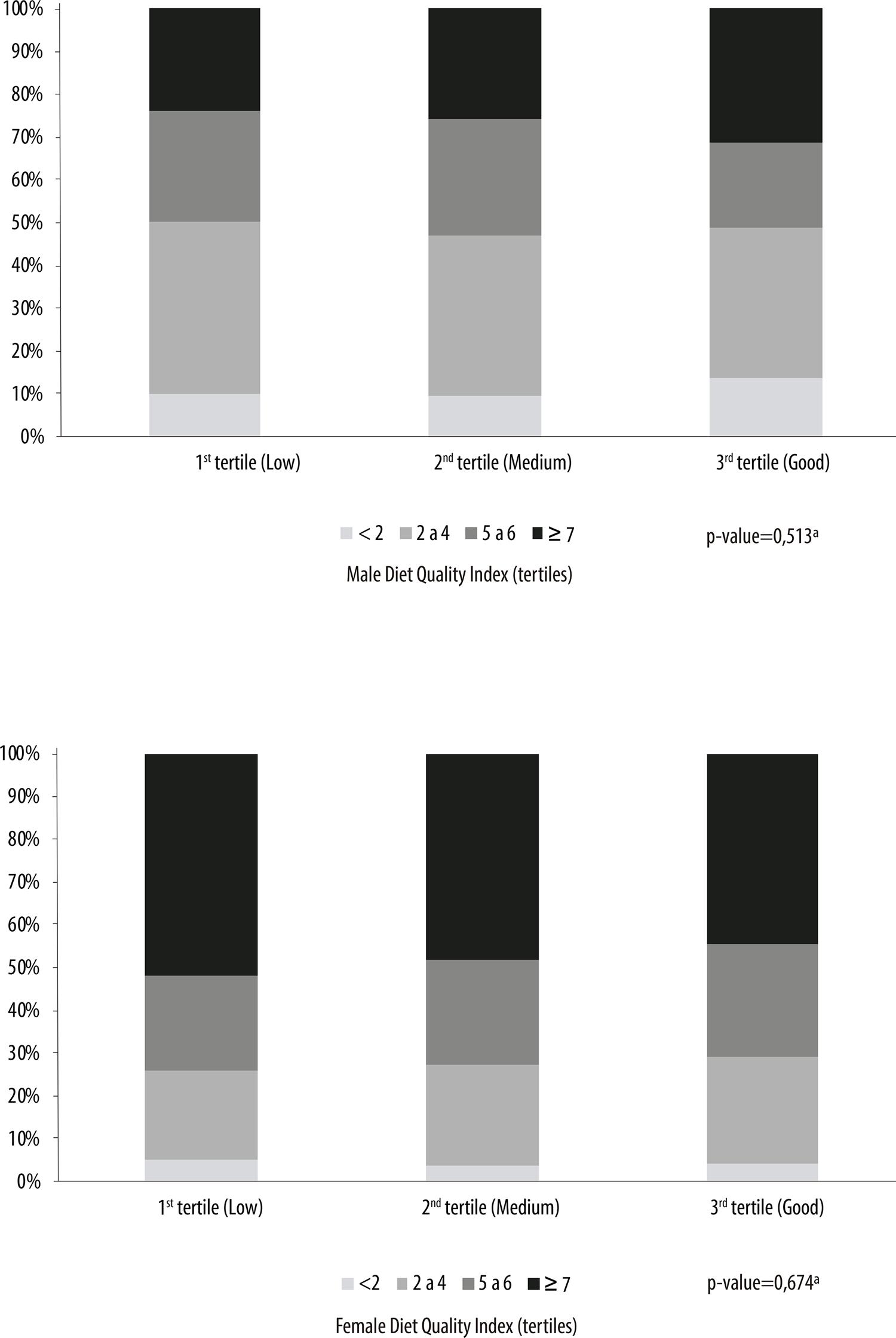
Figure 1 – Number of chronic diseases according to the diet quality index for the elderly (DQI-E), among elderly male and female members participating in the ‘COMO VAI?’ study, Pelotas, Rio Grande do Sul, 2014a) Pearson's chi-square test, to check if the number of diseases between DQI-E tertiles was different.
In Table 3 , only among elderly men, those who reported having consumed wholefoods in the last week (wholemeal bread, wholemeal biscuits, wholegrain rice or oats) on 1-3 days (PR=1.67 95%CI 1.31;2.14) and on 4-6 days (PR=1.64 95%CI 1.21;2.23), had a higher a multimorbidity prevalence ratio. In turn, elderly people who ate meat on at least one day in the week before the interview had less probability of having multimorbidity, whether they were men (PR=0.68 95%CI 0.51;0.92) or women (PR=0.70 95%CI 0.61;0.81).
Table 3 – Adjusted association between presence of multimorbidity (five diseases or more) and healthy food consumption, among elderly community members taking part in the ‘COMO VAI?’ study (n=865), Pelotas, Rio Grande do Sul, 2014
| Food consumption | Males | Females | ||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| N (%) | p-valuea | Adjusted PRb(95%CI) | N (%) | p-valuea | Adjusted PRb(95%CI) | p-valuea | ||
| Rice and beans | ||||||||
|
| ||||||||
| Did not eat | 16 (47.1) | 0.881 | 1.00 | 0.829 | 66 (71.7) | 0.848 | 1.00 | 0.995 |
| 1-3 days | 29 (48.3) | 1.08(0.70;1.68) | 140 (72.5) | 1.01(0.86;1.19) | ||||
| 4-6 days | 80 (53.0) | 1.16(0.80;1.69) | 170 (70.5) | 1.00(0.85;1.17) | ||||
| Every day | 129 (52.2) | 1.17(0.81;1.67) | 235 (73.9) | 1.01(0.87;1.17) | ||||
|
| ||||||||
| Vegetables and greens | ||||||||
|
| ||||||||
| Did not eat | 35 (55.6) | 0.809 | 1.00 | 0.744 | 44 (73.3) | 0.483 | 1.00 | 0.620 |
| 1-3 days | 85 (51.5) | 0.95(0.73;1.23) | 211 (74.0) | 1.04(0.87;1.22) | ||||
| 4-6 days | 55 (48.3) | 0.88(0.53;1.17) | 145 (74.7) | 1.05(0.89;1.25) | ||||
| Every day | 79 (52.7) | 0.99(0.65;1.17) | 211 (69.2) | 0.98(0.83;1.17) | ||||
|
| ||||||||
| Fruit | ||||||||
|
| ||||||||
| Did not eat | 22 (56.4) | 0.625 | 1.00 | 0.390 | 40 (81.6) | 0.318 | 1.00 | 0.428 |
| 1-3 days | 72 (52.6) | 0.85(0.92;1.15) | 116 (71.2) | 0.89(0.76;1.11) | ||||
| 4-6 days | 47 (46.1) | 0.75(0.53;1.06) | 142 (75.1) | 0.95(0.82;1.11) | ||||
| Every day | 113 (52.8) | 0.88(0.65;1.19) | 313 (70.7) | 0.91(0.79;1.05) | ||||
|
| ||||||||
| Milk and milk products | ||||||||
|
| ||||||||
| Did not eat | 58 (52.7) | 0.847 | 1.00 | 0.850 | 83 (75.5) | 0.357 | 1.00 | 0.487 |
| 1-3 days | 41 (47.7) | 1.03(0.77;1.39) | 103 (74.6) | 1.05(0.89;1.20) | ||||
| 1-6 days | 29 (50.0) | 0.99(0.70;1.38) | 92 (76.7) | 1.03(0.89;1.20) | ||||
| Every day | 126 (52.9) | 1.09(0.87;1.36) | 333 (70.0) | 0.97(0.85;1.10) | ||||
|
| ||||||||
| Wholefoodsc | ||||||||
|
| ||||||||
| Did not eat | 166 (47.8) | 0.10 | 1.00 | <0.001 | 360 (72.6) | 0.525 | 1.00 | 0.205 |
| 1-3 days | 29 (70.7) | 1.67(1.31;2.14) | 76 (77.6) | 1.11(0.98;1.25) | ||||
| 4-6 days | 18 (69.2) | 1.64(1.21;2.23) | 38 (67.9) | 0.97(0.81;1.16) | ||||
| Every day | 41 (52.6) | 1.25(0.98;1.59) | 137 (70.6) | 1.02(0.92;1.14) | ||||
|
| ||||||||
| Meat | ||||||||
|
| ||||||||
| Did not eat | 4 (100.0) | 0.070 | 1.00 | 0.013 | 7 (100.0) | 0.103 | 1.00 | <0.001 |
| Ate | 250 (51.2) | 0.68(0.51;0.92) | 604 (99.2) | 0.70(0.61;0.81) | ||||
a) Pearson’s chi-square test to verify whether healthy food consumption was different among elderly people with five diseases or more (multimorbidity).
b) Poisson regression, adjusted for age, race/skin color, schooling, economic classification, marital status, nutritional status, tobacco smoking and alcohol consumption. The statistical analyses took sample design effect into consideration.
c) Wholefoods were considered to be: wholemeal bread, wholemeal biscuits, wholegrain rice or oats.
Notes: N = 865; males = 254 and females = 611.
PR: prevalence ratio.
95%CI: 95% confidence interval.
There was no association between consumption of food considered to be unhealthy and occurrence of multimorbidity ( Table 4 ).
Table 4 – Adjusted association of presence of multimorbidity (five diseases or more) and unhealthy food consumption among elderly community members taking part in the ‘COMO VAI?’ study (n=865), Pelotas, Rio Grande do Sul, 2014
| Food consumption | Males | Females | |||||||
|---|---|---|---|---|---|---|---|---|---|
|
| |||||||||
| N (%) | p-valuea | Adjusted PRb(95%CI) | N (%) | p-valuea | Adjusted PRb(95%CI) | p-valuea | |||
| Confectionary, soft drinks and industrialized fruit juice | |||||||||
|
| |||||||||
| Did not eat | 68 (50.0) | 0.053 | 1.00 | 0.240 | 193 (73.1) | 0.937 | 1.00 | 0.921 | |
| 1-3 days | 89 (58.6) | 1.12 (0.90;1.40) | 174 (71.9) | 0.98(0.88;1.09) | |||||
| 4-6 days | 20 (37.0) | 0.81 (0.55;1.18) | 68 (70.1) | 0.96(0.83;1.11) | |||||
| Every day | 77 (51.3) | 0.69 (0.76;1.21) | 176 (73.0) | 1.01(0.90;1.12) | |||||
|
| |||||||||
| Fried food | |||||||||
|
| |||||||||
| Did not eat | 126 (53.9) | 0.443 | 1.00 | 0.204 | 383 (72.8) | 0.945 | 1.00 | 0.997 | |
| 1-3 days | 105 (48.6) | 0.86(0.71;1.03) | 211 (71.8) | 0.99(0.91;1.09) | |||||
| 4-6 days | 13 (48.2) | 0.81(0.55;1.20) | 13 (72.2) | 0.98(0.74;1.30) | |||||
| Every day | 10 (66.7) | 1.17(0.81;1.69) | 4 (66.7) | 1.04(0.62;1.74) | |||||
|
| |||||||||
| Conserves, charcuterie and tinned food | |||||||||
|
| |||||||||
| Did not eat | 140 (51.1) | 0.994 | 1.00 | 0.866 | 410 (71.4) | 0.492 | 0.209 | ||
| 1-3 days | 81 (51.3) | 0.99(0.82;1.21) | 158 (76.3) | 1.00 | |||||
| 4-6 days | 17 (51.5) | 0.98(0.70;1.36) | 18 (66.7) | 1.10(1.00;1.21) | |||||
| Every day | 13 (54.2) | 1.16(0.70;1.36) | 21 (72.4) | 1.01(0.79;1.30) | |||||
|
| |||||||||
| Frozen food | |||||||||
|
| |||||||||
| Did not eat | 232 (51.8) | 0.307 | 1.00 | 0.975 | 563 (72.2) | 0.257 | 1.00 | 0.329 | |
| Ate | 19 (46.3) | 1.01(0.71;1.43) | 44 (77.2) | 1.08(0.92;1.27) | |||||
|
| |||||||||
| Fastfood | |||||||||
|
| |||||||||
| Did not eat | 235 (51.4) | 0.510 | 1.00 | 0.708 | 580 (73.2) | 0.060 | 1.00 | 0.221 | |
| Ate | 16 (50.0) | 1.07(0.76;1.51) | 27 (60.0) | 0.86(0.67;1.09) | |||||
a) Pearson’s chi-square test to verify whether unhealthy food consumption was different among elderly people with more than five diseases (multimorbidity).
b) Poisson regression with adjustment for robust variance, adjusted for age, race/skin color, schooling, economic classification, marital status, nutritional status, tobacco smoking and alcohol consumption.
Notes: N = 865; males = 254 and females = 611.
PR: prevalence ratio.
95%CI: 95% confidence interval.
Discussion
This study investigated association between food consumption and occurrence of multimorbidity among elderly people in the urban area of Pelotas, RS. With regard to food items considered to be healthy, lower probability of multimorbidity occurring was only found in relation to higher meat consumption and no significant association was found with other food items or groups in this category. On the other hand, the exception with regard to food items considered to be healthy was intake of wholefoods, whereby men in the intermediate consumption groups had greater probability of reporting having had at least five concomitant morbidities in their lifetime.
Although this study did not find significant difference in DQI-E association with the presence of multimorbidity, a population-based study conducted with elderly people in Campinas, SP, in 2008, found better quality diet among those who had three or more chronic diseases, with no difference between men and women.3 In China, between 2002 and 2007, a s tudy aiming to find a relationship between nutrition and NCDs in adult and elderly people, monitored the progress of multimorbidity longitudinally, and concluded that individuals suffering from just one disease consumed more fruit, vegetables and grains (not including rice and wheat) when compared to groups suffering from more diseases.8
Despite a protective relationship having been found between consuming meat and having five or more chronic diseases, studies prove the importance of including meat as part of diet. It has been demonstrated that consuming meat, which is rich in proteins, iron and zinc, contributes significantly to the body’s development and functioning.22 It is however necessary to take care regarding quantity and quality of meat, principally when eating it without removing visible fat,24 as this is possibly harmful to health because it is rich in cholesterol and saturated fatty acids and these are characteristics related to the development of cardiovascular diseases.24
Although this study found association between wholefood consumption and greater risk of multimorbidity occurring in men, wholefood consumption was more frequent among women. Wholefoods have functional properties, contain vitamins and minerals and are rich in fibers that help to prevent several health problems.25 No information was found in the literature to justify why wholefoods would increase the probability of multimorbidity occurring, given that their properties are beneficial for treatment and prevention of a variety of diseases.26 It is possible, however, that individuals with more diseases might decide to consume healthier foods, including wholefoods.
Although in a different cultural context, a study conducted with Iranian adults found inverse association between whole grain consumption and occurrence of NCDs.27 The authors reported that some health risk factors, including dyslipidemia and hypertension, can lead to participants changing their diet and, therefore, confound association between grain consumption and metabolic risks.27 The same may have occurred in our study, so that wholefood intake found among men may not reflect a relationship between this type of food and occurrence of NCDs, but rather a change in behavior in response to multiple diagnoses.
It is also common for eating habits to be maintained following diagnosis of one or more diseases.28 Cembranel et al. found that even after monitoring elderly people in Rio de Janeiro with diagnosis of diabetes mellitus and hypertension for five years, they did not change their eating habits as a measure to assist with treatment of those diseases.28
Absence of inverse association of consumption of some food items recognized as being healthy (as well as the opposite, in the case of unhealthy food) with multimorbidity could be explained – at least in part – by the absence of temporal information in this cross-sectional study, given that a change in food consumption may have occurred once the occurrence of NCDs was identified. This behavior was also mentioned by Fortin et al. in 2010, when they did not identify association between the presence of three or more chronic diseases in adult Canadians (45 years old or more) and not eating the recommended daily amount of fruit and vegetables.29
The positive aspects of this study include the size of the sample in order to meet the objectives proposed and its representativeness, as well as the detailed identification of aspects of elderly people’s lives, investigation of several health problems, methodological rigor and high response rate.
The limitations of this study include information bias due to the use of the Food Frequency Questionnaire (FFQ). Use of the FFQ may imply negative aspects, such as depending on the memory of the participants, given that food consumption referred to the seven days prior to the interview, as well as there being no information about the size of the portions consumed. It may be a case of recall error, whereby it is possible that some consumed food items were not reported and that the results therefore may have been underestimated. It should also be emphasized that the previous seven days may not reflect a habit taking place over a longer period of time; the seven-day recall period was chosen precisely because of the fact of elderly people having reduced memory capacity about food consumption over a longer time period. Elderly people who had difficulty in answering the questionnaire were able to be helped by a carer when answering, also with the aim of reducing the recall time effect.
The possibility of the FFQ causing a classification error should also be taken into consideration, given that consumption was classified categorically and not continuously, in accordance with the assumptions of the former Food Guide (2006), which may not reflect the current context of Brazilian food intake, currently assessed based on the New Food Guide (2014). This new version of the Guide contextualizes food based on the degree of processing and not on types of food.
It should also be highlighted that although the concept of multimorbidity consists of the presence of two or more diseases, this study opted for a different cut-off point (five or more diseases) because of the greater differentiation power of the sample. The same cut-off point was proposed in a study published recently.15
The health problems included in this study were reported by elderly people, which may result in information bias. This may however be minimized by the fact of the questions asking about medical diagnosis30 and approximately 90% of those elderly people having visited a doctor in the last year, thus minimizing possible self-reporting bias.
The lack of an upper limit when scoring food considered to be healthy can also be seen as a limitation, if there was indeed inadequate excessive consumption of these food items. The type of meat consumed was not assessed, so that no further inference could be made about consumption of this type of food. Moreover, the FFQ does not enable assessment of the entire dimension of a person’s diet (other food items, portions, time at which food is consumed, type of food preparation) but rather some consumption “markers”.
There is also a scarcity of national and international studies7 assessing the relationship between multimorbidity and food consumption among elderly people using DQI, thus limiting comparisons with the results of this study. Survivorship bias must also be taken into consideration: the sample was comprised of people who were senior citizens, so that those with severe health problems or a greater number of diseases may have died and, consequently, would not have been included in the sample; they are individuals who, as a consequence of their illnesses, may have taken more care with their food intake.
Finally, some results point to yet another possible bias, namely reverse causality, which limits some associations because it is not possible to observe temporality in the relation between exposure and the study outcome. This bias can hinder understanding with regard to change in consumption of healthy food and being affected by multimorbidity, in particular morbidities capable of asymptomatic progression for a long period of time, this being an effect that is better understood through studies with a longitudinal design. The use of considerably broad categories for the schooling (<8 years; ≥8 years) and tobacco smoking (yes; no) variables may have cause residual confounding. Moreover, performing multiple statistical tests could increase the likelihood of an association having been observed by chance, which could explain the statistical association found only with intermediate wholefood consumption by men in this study.
Studies of this type are important as they point to reflections about current eating habits and their influence on the development and maintenance of non-communicable chronic diseases among the elderly. This study focused on a given moment in time and cross-sectional studies analyzing this relationship are scarce. Encouragement of longitudinal studies is an alternative for a better understanding of the relationship between the occurrence of multimorbidity and food intake habits among the elderly over time. Assessment of functional capacity, access to financial resources, as well as recognition of lifestyle factors that can be changed, represent pertinent information to be taken into consideration by health sectors when examining multimorbidity in this age group. Despite the limitations presented, it must be highlighted that consumption of meat and wholefoods, even though they were found to be protection and risk factors for multimorbidity, respectively, should both be consumed in carefully assessed quantity and quality. Although no association was found between DQI-E and multimorbidity, the results point to the importance of adopting policies aimed at health promotion and the possibility of treating, maintaining and preventing diseases among the elderly population.
REFERENCES
1. World Health Organization - WHO . Non communicable diseases prematurely take 16 million lives annually, WHO urges more action [ Internet ]. Geneva : World Health Organization ; 2015 [ cited 2020 May 13 ]. Available from: http://www.who.int/mediacentre/news/releases/2015/noncommunicable-diseases/en/ [ Links ]
2. Fortin M , Stewart M , Poitras ME , Almirall J , Maddocks H . A systematic review of prevalence studies on multimorbidity: toward a more uniform methodology . Ann Fam Med [ Internet ]. 2012 Mar-Apr [ cited 2020 May 13 ]; 10 ( 2 ): 142 - 51 . Available from: https://doi.org/10.1370/afm.1337 [ Links ]
3. Assumpção DD , Domene SMA , Fisberg RM , Barros MDBA . Qualidade da dieta e fatores associados entre idosos: estudo de base populacional em Campinas, São Paulo, Brasil . Cad Saúde Pública [ Internet ]. 2014 ago [ citado 2020 maio 13 ]; 30 ( 8 ): 1680 - 94 . Disponível em: https://doi.org/10.1590/0102-311X00009113 [ Links ]
4. Hidalgo CA , Blumm , N , Barabási , AL , Christakis NA . A dynamic network approach for the study of human phenotypes . PLoS Comput Biol [ Internet ]. 2009 Apr [ cited 2020 May 13 ]; 5 ( 4 ). Available from: https://doi.org/10.1371/journal.pcbi.1000353 [ Links ]
5. Cheung CL , Nguyen US , AU E , Tan KC , Kung AW . Association of handgrip strength with chronic diseases and multimorbidity: a cross-sectional study . AGE ( Dordr ) [ Internet ]. 2012 Jun [ cited 2020 May 13 ]; 35 ( 3 ): 929 - 41 . Available from: https://doi.org/10.1007/s11357-012-9385-y [ Links ]
6. World Health Organization . Global status report on noncommunicable diseases 2010 [ Internet ]. Geneva : World Health Organization ; 2011 [ cited 2020 May 13 ]. Available from: https://www.who.int/nmh/publications/ncd_report_full_en.pdf [ Links ]
7. Scherer R , Scherer F , Conde SR , Dal Bosco SM . Estado nutricional e prevalência de doenças crônicas em idosos de um município do interior do Rio Grande do Sul . Rev Bras Geriatr Gerontol [ Internet ]. 2013 dez [ citado 2020 maio 13 ]; 16 ( 4 ): 769 - 79 . Disponível em: https://doi.org/10.1590/S1809-98232013000400011 [ Links ]
8. Ruel G , Shi Z , Zhen S , Zuo H , Kroger E , Sirois C , et al . Association between nutrition and the evolution of multimorbidity: the importance of fruits and vegetables and whole grain products . Clin Nutr [ Internet ]. 2014 Jun [ cited 2020 May 13 ]; 33 ( 3 ): 513 - 20 . Available from: https://doi.org/10.1016/j.clnu.2013.07.009 [ Links ]
9. Bernstein M , Muñoz N . Position of the Academy of Nutrition and Dietetics: food and nutrition for older adults: promoting health and wellness . J Acad Nutr Diet [ Internet ]. 2012 Aug [ cited 2020 May 13 ]; 112 ( 8 ): 1255 - 77 . Available from: https://doi.org/10.1016/j.jand.2012.06.015 [ Links ]
10. Baena RC . Muito além dos nutrientes: o papel dos fitoquímicos nos alimentos integrais . Diagn Tratamento [ Internet ]. 2015 mar [ citado 2020 maio 13 ]; 20 ( 1 ): 17 - 21 . Disponível em: http://files.bvs.br/upload/S/1413-9979/2015/v20n1/a4600.pdf [ Links ]
11. Gil-Montoya JA , Mello AL , Barrios R , Gonzalez-Moles MA , Bravo M . Oral health in the elderly patientand its impact on general well-being: a non-systematic review . Clin Interv Aging [ Internet ]. 2015 Feb [ cited 2020 May 13 ]; 10 : 461 - 7 . Available from: https://doi.org/10.2147/CIA.S54630 [ Links ]
12. Gordilho A , Nascimento JS , Silvestre J , Ramos LR , Freire MPA , Espíndola N , et al . Desafios a serem enfrentados no terceiro milênio pelo setor saúde na atenção integral do idoso [ Internet ]. Rio de Janeiro : Universidade do Estado do Rio de Janeiro / Universidade Aberta da Terceira Idade ; 2000 [ citado 2020 maio 13 ]. 90 p. Disponível em: http://www.crde-unati.uerj.br/publicacoes/textos_Unati/unati1.pdf [ Links ]
13. Ministério da Saúde (BR) . Secretaria de Atenção à Saúde . Departamento de Atenção Básica . Obesidade [ Internet ]. Brasília : Ministério da Saúde ; 2006 [ citado 2020 maio 13 ]. ( Cadernos de Atenção Básica, n. 12.) (Série A. Normas e Manuais Técnicos ). 108 p. Disponível em: http://dab.saude.gov.br/portaldab/biblioteca.php?conteudo=publicacoes/cab12 [ Links ]
14. Instituto Brasileiro de Geografia e Estatística - IBGE . Censo demográfico 2010 [ Internet ]. Rio de Janeiro : Instituto Brasileiro de Geografia e Estatística ; 201- [ citado 2018 dez 14 ]. Disponível em: https://ww2.ibge.gov.br/home/estatistica/populacao/censo2010/default.shtm [ Links ]
15. Costa CS , Flores TR , Wendt A , Neves RG , Tomasi E , Cesar J , et al . Inequalities in multimorbidity among elderly: a population-based study in a Brazilian Southern city . Cad Saúde Pública [ Internet ]. 2018 nov [ citado 2020 maio 13 ]; 34 ( 11 ): e00040718 . Disponível em: https://doi.org/10.1590/0102-311x00040718 [ Links ]
16. World Health Organization - WHO . Obesity: preventing and managing the global epidemic [ Internet ]. Geneva : World Health Organization ; 2000 [ cited 2020 May 13 ]. ( WHO Technical Report Series 894 ). 252 p. Available from: https://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/ [ Links ]
17. Chumlea WC , Guo S . Equations for predicting stature in white and black elderly individuals . J Gerontol [ Internet ]. 1992 Nov [ cited 2020 May 13 ]; 47 ( 6 ): 197 - 203 . Available from: https://doi.org/10.1093/geronj/47.6.M197 [ Links ]
18. Closs VE , Feoli VE , Schwanke CHA . Altura do joelho como medida alternativa confiável na avaliação nutricional de idosos . Rev Nutr [ Internet ]. 2015 set [ citado 2020 maio 13 ]; 28 ( 5 ): 475 - 84 . Disponível em: https://doi.org/10.1590/1415-52732015000500002 [ Links ]
19. Gomes AP , Soares ALG , Gonçalves H . Baixa qualidade da dieta de idosos: estudo de base populacional no sul do Brasil . Ciênc Saúde Coletiva [ Internet ]. 2016 nov [ citado 2020 maio 13 ]; 21 ( 11 ): 3417 - 28 . Disponível em: https://doi.org/10.1590/1413-812320152111.17502015 [ Links ]
20. Ministério da Saúde (BR) . Secretaria de Atenção à Saúde . Coordenação-Geral da Política de Alimentação e Nutrição . Guia alimentar para a população brasileira: promovendo a alimentação saudável [ Internet ]. Brasília : Ministério da Saúde ; 2006 [ citado 2020 maio 13 ]. ( Série A. Normas e Manuais Técnicos ). 210 p. Disponível em: http://189.28.128.100/nutricao/docs/geral/guia_alimentar_conteudo.pdf [ Links ]
21. Associação Brasileira de Empresas de Pesquisa - ABEP . Alterações na aplicação do critério Brasil, válidas a partir de 2013 [ Internet ]. São Paulo : Associação Brasileira de Empresas de Pesquisa ; 2013 [ citado 2020 maio 13 ]. Disponível em: http://www.abep.org/novo/Content.aspx?ContentID=835 [ Links ]
22. Mateus K , Santos MR , Cardoso GJ , Souza AT , Kessler JD . A importância e benefícios da carne na alimentação humana . J Sul Brasil Rural [ Internet ]. 2017 jul [ citado 2020 maio 13 ]; 9 ( 195 ): 1 - 4 . Disponível em: http://www.ceo.udesc.br/arquivos/id_submenu/285/rural_195.pdf [ Links ]
23. Malta DC , Stopa SR , Iser BPM , Bernal RTI , Claro RM , Nardi ACF , et al . Fatores de risco e proteção para doenças crônicas por inquérito telefônico nas capitais brasileiras, Vigitel 2014 . Rev Bras Epidemiol [ Internet ]. 2015 dez [ citado 2020 maio 13 ]; 18 ( 2 ): 238 - 55 . Disponível em: https://doi.org/10.1590/1980-5497201500060021 [ Links ]
24. Santos RD , Gagliardi ACM , Xavier HT , Magnoni CD , Cassani R , Lottenberg AMP , et al . I Diretriz sobre o consumo de gorduras e saúde cardiovascular . Arg Bras Cardiol [ Internet ]. 2013 jan [ citado 2020 maio 13 ]; 100 ( 1 Suppl 3 ): 1 - 40 . Disponível em: https://doi.org/10.1590/S0066-782X2013000900001 [ Links ]
25. Lemos Júnior HPL , Lemos ALA . Alimentos integrais . Diagn Tratamento [ Internet ]. 2013 mar [ citado 2020 maio 13 ]; 18 ( 2 ): 72 - 74 . Disponível em: http://files.bvs.br/upload/S/1413-9979/2013/v18n2/a3607.pdf [ Links ]
26. Galdeano MC . Os grãos integrais estão fazendo bem? Portal do Agronegócio [ Internet ]. 2012 nov [ citado 2020 maio 13 ]. Disponível em: https://www.portaldoagronegocio.com.br/artigo/os-graos-integrais-estao-fazendo-bem [ Links ]
27. Esmaillzadeh A , Mirmiran P , Azizi F . Whole-grain consumption and the metabolic syndrome: a favorable association in Tehranian adults . Eur J Clin Nutr [ Internet ]. 2005 Mar [ cited 2020 May 13 ]; 59 ( 3 ): 353 - 62 . Available from: https://doi.org/10.1038/sj.ejcn.1602080 [ Links ]
28. Cembranel F , Oliveira Bernardo C , Ozcariz SGI , D’Orsi E . Impacto do diagnóstico de diabetes e / ou hipertensão em indicadores de consumo alimentar saudável: um estudo longitudinal de idosos . Rev Bras Geriatr Gerontol [ Internet ]. 2017 mar [ citado 2020 maio 13 ]; 20 ( 1 ): 34 - 46 . Disponível em: http://dx.doi.org/10.1590/1981-22562017020.160081 [ Links ]
29. Fortin M , Haggerty J , Almirall J , Bouhali T , Sasseville M , Lemieux M . Lifestyle factors and multimorbidity: a cross sectional study . BMC Public Health [ Internet ]. 2014 Jul [ cited 2020 May 13 ]; 14 : 686 . Available from: https://doi.org/10.1186/1471-2458-14-686 [ Links ]
30. Vellakkal S , Millett C , Basu S , Khan Z , Aitsi-Selmi A , Stuckler D , et al . Are estimates of socioeconomic inequalities in chronic disease artefactually narrowed by self-reported measures of prevalence in low-income and middle-income countries? Findings from the WHO-SAGE survey . J Epidemiol Community Health [ Internet ]. 2015 Dec [ cited 2020 May 13 ]; 69 ( 3 ): 218 - 25 . Available from: https://doi.org/10.1136/jech-2014-204621 [ Links ]
Associated Editors: Lúcia Rolim Santana de Freitas - orcid.org/0000-0003-0080-2858 Vivian Siqueira Santos Gonçalves - orcid.org/0000-0001-6893-8263
*Article derived from a Nutrition Degree course conclusion assignment by Bruna Padilha Pereira, at the Federal University of Pelotas, Pelotas, RS, Brazil. The data used were provided by the Guided Master’s Degree Consortium for Valuing Care of the Elderly (‘COMO VAI?’ study), conducted between January and August 2014, within the Federal University of Pelotas Epidemiology Postgraduate Program. The study received funding from the Coordination for the Improvement of Higher Education Personnel / Ministry of Education, via its Academic Excellence Program (PROEX No. 1,107/2013).
Received: April 04, 2019; Accepted: April 23, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
