










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.4 Brasília 2020 Epub 17-Jul-2020
http://dx.doi.org/10.5123/s1679-49742020000400005
Investigation of public health events of concern
Description of COVID-19 cluster: isolation and testing in asymptomatic individuals as strategies to prevent local dissemination in Mato Grosso state, Brazil, 2020
1Prefeitura Municipal de Tangará da Serra, Tangará da Serra, MT, Brazil
2Secretaria de Estado de Saúde de Mato Grosso, Laboratório Central do Estado de Mato Grosso, Cuiabá, MT, Brazil
3Universidade do Estado de Mato Grosso, Campus de Tangará da Serra, Tangará da Serra, MT, Brazil
4Instituto Oswaldo Cruz, Fundação Oswaldo Cruz, Rio de Janeiro, RJ, Brazil
Objective:
to describe a COVID-19 cluster and the strategies used to contain the virus, in a municipality in the interior region of Mato Grosso state, Brazil.
Methods:
this is a descriptive study of documental records of an epidemiological investigation conducted in April 2020.
Results:
introduction of SARS-CoV-2 in the municipality was identified through a cluster comprised of five people, 4 were symptomatic and 1 was asymptomatic, after the virus was imported by index cases C01 and C02; in addition to household transmission (C03, C04), a physiotherapist (C05) was infected through contact with C02; with the exception of C04, all had an influenza-like symptoms and C02 required hospitalization; as for laboratory tests, all were seroreactive and C01 was RT-PCR positive.
Conclusion:
dissemination of COVID-19 was contained by effective home isolation, an important instrument that should be adopted early by unaffected municipalities to contain virus dissemination, as well as by serological testing that detected infection in asymptomatic patients.
Keywords: Coronavirus; Coronavirus Infections; Epidemiology; Disease Transmission, Infectious; Epidemiology, Descriptive
Introduction
The recent pandemic which began in China caused by the SARS-CoV-2 coronavirus, spread throughout the world and reached Brazil, where a public health emergency of national concern was declared in February.1–2 It is considered to be the most challenging pandemic of modern times; the proportion of COVID-19 cases and deaths has reached alarming levels, with 3,672,238 cases and 254,045 deaths globally3 and 135,106 cases and 9,146 deaths in Brazil as at May 7th 2020.2
This global scenario is due to the high transmissibility4 and high dissemination of the virus, with an estimated basic reproduction number (R0) of between 2.6 and 4.1,5,6 associated with diverse forms of contagion,7 as well as absence of effective medication and vaccines. Introduction of SARS-CoV-2 in new territories occurred initially through imported cases. Its propagation has however been mainly associated with asymptomatic cases,8 possibly because of the difficulty faced by health services in providing mass diagnostic testing and in identifying infected people who transmit the virus during its incubation period. It is known that people can transmit the virus days before the onset of clinical manifestations.9
Within this context and considering that asymptomatic people generally get infected in health and family environments,10 studies published in Germany, Vietnam and China had evidenced asymptomatic transmission of COVID-19 in family clusters.11–13 Apart from difficulty in detecting asymptomatic cases, scarcity of supplies for diagnosis and difficulty in accessing health services have hindered adoption of protective and mitigating measures aimed at early isolation of suspected cases, social distancing and intensification of hygiene habits which contribute to controlling the dissemination of the virus.14
It is appropriate to emphasize that in places with fragile logistics and difficulty in accessing technologies in a timely manner, as is the case of many Brazilian municipalities, the role of health surveillance services becomes fundamental and strategic. Lu et al.15 have affirmed that comprehensive and rigorous epidemiological investigation can assist in identifying asymptomatic cases and contribute to disease control within the catchment areas of these services.
Knowledge of how an infectious agent with high transmissibility rates is introduced into unaffected municipalities is fundamental for determining risks, as well as for assessing the effectiveness of household isolation as a measure to mitigate SARS-CoV-2 dissemination in the Brazilian interior.
In view of this scenario, the aim of this article was to describe a COVID-19 cluster and the strategies used to contain the virus in a municipality in the interior region of Mato Grosso state, Brazil.
Methods
This is a descriptive study of the introduction of SARS-CoV-2 in Tangará da Serra, a municipality in the interior region of Mato Grosso state in March and April 2020.
The municipality is located in the southwest region of Mato Grosso in a Cerrado (savanna) biome area, 240km away from Cuiabá, the state capital. In 2019 the local population was estimated to be 103,750 inhabitants, with population density of 7.37 inhab./km2 and a Human Development Index (HDI) of 0.729. It is the main city in its microregion and serves as a reference for private health care there. It is Mato Grosso's fifth largest city, accounting for some 3% of the state's population.16 It has 211 health establishments, both public and private, registered with the National Health Establishment Registry.17
Public domain data made available daily by Tangará da Serra Municipal Health Department was used, as well as documental records comprised of notification forms and epidemiological investigation reports.
The study variables were comprised of sociodemographic data and data on exposure of infected cases: age (in completed years), sex (female, male), occupation, probable infection situation, date of symptom onset, date of sample collection for laboratory RT-PCR and serology tests, interval between symptoms and RT-PCR collection, interval between RT-PCR collection and access to the result, interval between symptoms and serology. Clinical manifestations were verified (fever, runny nose, headache, cough, sore throat, breathing discomfort, saturation <95%), as well as computerized tomography, hospitalization, ventilation support (no, yes) and case evolution.
The laboratory tests were performed at the Mato Grosso State Central Laboratory, which a state reference service subordinated to the Mato Grosso State Health Department. Combined nasopharyngeal and oropharyngeal swabs were submitted to real-time RT-PCR tests using kits (Charité Protocol: SARS-CoV2 E/P1 - Bio Manguinhos), while serum samples were analyzed using Smart Test Covid-19 Vyttra, batch 2004313, and Bio-activity, batch 9500437, commercial rapid tests, validated by the National Health Surveillance Agency (ANVISA).
The data were systematized on electronic spreadsheets following double data entry and subsequent checking using the Data Compare tool, before being imported into the Statistical Package for the Social Sciences – SPSS version 21.0, for statistical description according to absolute frequency.
All ethical aspects related to research involving human beings were respected in accordance with the Declaration of Helsinki and Brazilian National Health Council Resolution No. 466/2012. This study is part of a matrix project entitled Health Information System, Certification of Submission for Ethical Appraisal – CAAE No. 29208720.1.0000.5166, and was approved by the Mato Grosso State University Research Ethics Committee (Opinion No. 3.903.719), in March 2020. Once household isolation had ended, the subjects, or their legal guardians, signed a Free and Informed Consent form.
Results
The cluster was formed by the first five COVID-19 cases to occur in Tangará da Serra, Mato Grosso, Brazil. It was comprised of index cases C01 (51 years old) and C02 (42 years old); their children C03 (12 years old) and C04 (09 years old); and case C05 (C02's physiotherapist).
The couple C01 and C02 traveled to São Paulo on March 6th 2020 and returned on March 11th 2020. They stayed in the capital of Mato Grosso state, Cuiabá, between March 11th and 13th 2020 before returning to their home. C02 reported that in Cuiabá she had no clinical manifestation and that she was a speaker at a health-related event for 150 people, and that both of them, C01 and C02, had social contact with a health professional who was later diagnosed as having COVID-19.
When they returned to Tangará da Serra on March 13th, the couple C01 and C02 had contact with their children (C03 and C04) and with C02's physiotherapist (case C05), as well as with two female household employees (C06 and C07). On March 17th, C01 and C02 began to show clinical symptoms compatible with COVID-19: C01 had a cough, runny nose, headache and mild dyspnea; while C02 had fever, cough, runny nose and moderate dyspnea. At that time they had not sought medical proof of their condition. On the morning of March 17th, C02 had a session with her physiotherapist (C05) in consulting rooms where other people also consulted until a municipal decree came into force on March 19th 2020 suspending most commercial activities (Figure 1). The physiotherapist remained in social isolation at home with her uncle and aunt C08 and C09.
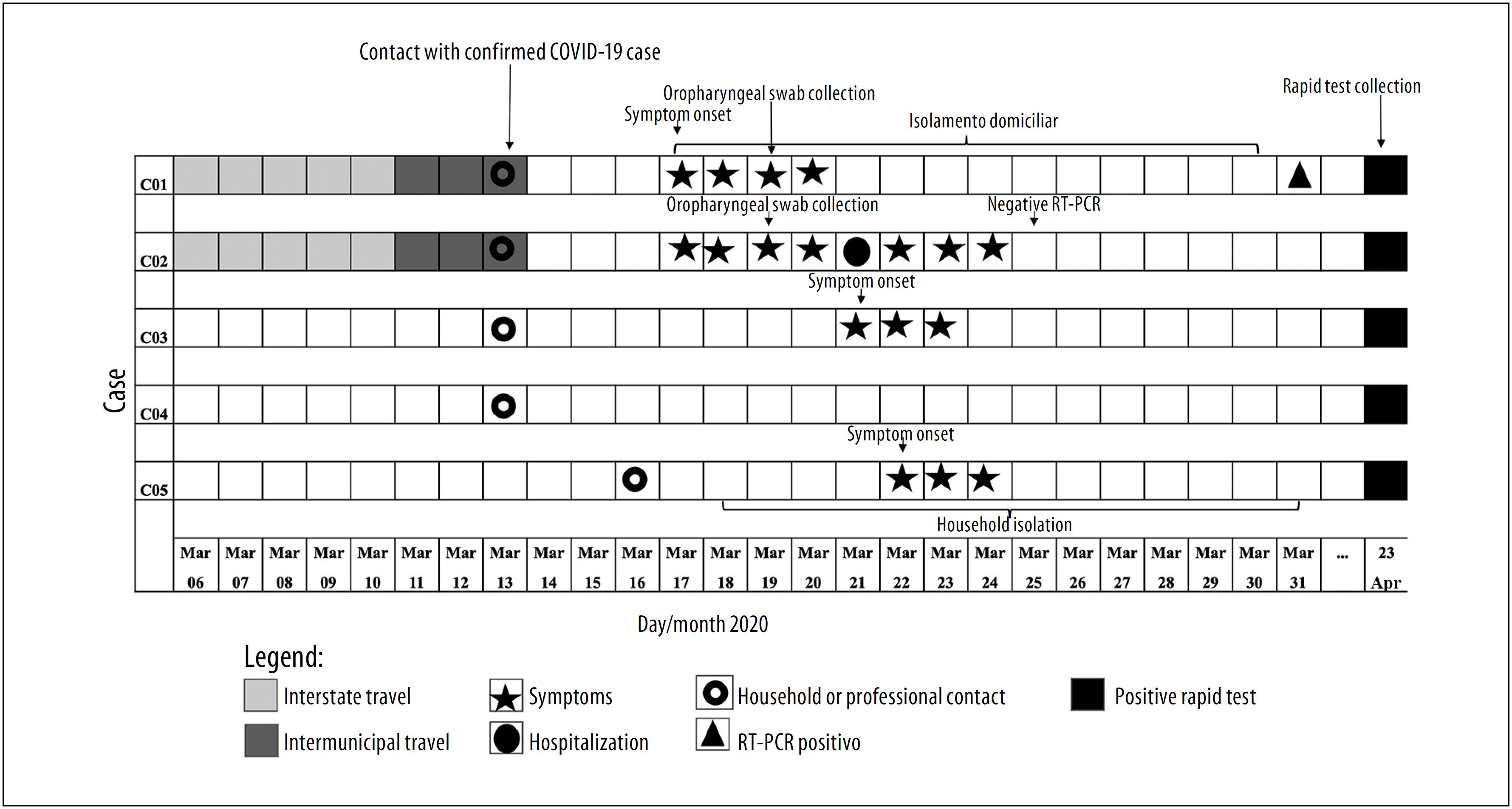
Table 1 shows the cluster's sociodemographic, eidemiological and clinical characteristics of SARS-CoV-2 infection in Tangará da Serra, Mato Grosso, in April 2020.
Table 1 Sociodemographic, epidemiological and clinical characteristics of the COVID-19 family cluster members in Tangará da Serra, Mato Grosso, Brazil, 2020
| Data | Individuals infected by SARS-CoV-2 | ||||
|---|---|---|---|---|---|
| C01 | C02 | C03 | C04 | C05 | |
| Age | 51 years | 42 years | 12 years | 9 years | 35 years |
| Sex | Male | Female | Female | Male | Female |
| Occupation | Agronomist | Dentist | Student | Student | Physiotherapist |
| Probable infection situation | Travel and contact with confirmed case | Travel and contact with confirmed case | Household contact with C01 and C02 | Household contact with C01 and C02 | Professional contact with C02 |
| Interval between symptoms and RT-PCR collection | 2 days | 2 days | N/A | N/A | N/A |
| Interval between collection and access to RT-PCR result | 14 days | 8 days | N/A | N/A | N/A |
| Interval between symptoms and serology test performance | 35 days | 35 days | 32 days | N/A | 31 days |
| Clinical manifestations and evolution | |||||
| Fever | No | Yes | No | No | Yes |
| Runny nose | Yes | Yes | Yes | No | Yes |
| Headache | Yes | No | No | No | Yes |
| Cough | Yes | Yes | Yes | No | Yes |
| Sore throat | Yes | Yes | No | No | No |
| Dyspnea | Yes | Yes | No | No | No |
| Breathing discomfort | No | Yes | No | No | No |
| Saturation <95% | No | Yes | No | No | No |
| Lung CT | N/P | Ground-glass | N/P | N/P | N/P |
| Hospitalization | No | Yes | No | No | No |
| Non-invasive ventilation support | No | Yes | No | No | No |
| Evolution | Cure | Cure | Cure | Cure | Cure |
Legend:
N/A = Not applicable.
N/P = Not performed.
CT = computerized tomography.
On March 17th 2020, after the municipal call center for symptomatic respiratory cases had been informed about their recent journey to the state of São Paulo, C01 and C02 remained in household isolation and were monitored daily by telephone. However, it was only on March 19th that they reported that clinical manifestations had existed since March 17th. C01 and C02 were then referred for medical care, notification and biological sample collection for testing at a private health facility.
On March 21st, C02 had become worse, with breathing difficulties, chest pain and moderate dyspnea, and was taken into hospital. The the computerized tomography (CT) result confirmed the ground-glass pattern. With non-invasive respiratory support, C02 remained in hospital for 24 hours. The result of her rapid influenza test (Alere AG pandemic A/B/A [H1N1], batch 19BOD005A-A) was negative.
On the same day, C03 started with a cough and runny nose, was assessed by a doctor and told to stay at home. A swab specimen was not collected because of the epidemiological criterion requiring travel or contact with a confirmed case, given that at that date the real-time RT-PCR test result was not yet available.
C02 received her negative RT-PCR result on March 25th, but remained in household isolation as C01's result was not available. On that date, C02 spoke with a colleague with whom she had had lunch during the event in Cuiabá on March 12th and her colleague told her she had had a positive RT-PCR result and was recovering after having been hospitalized.
Although C02's real-time RT-PCR test result was negative, C01's swab specimen collected on the second day of clinical manifestations had a positive real-time RT-PCR result. As such, 14 days after the onset of symptoms, on March 31st, with this laboratory confirmation of the case and at the end of C01 and C02's household isolation, it was possible to confirm C02 using the clinical-epidemiological criterion. In addition to contact with C03 and C04, the index cases also informed that they had had contact at home with C06 and C07.
Blood samples of the family members, the physiotherapist and the two other contacts were later submitted to rapid testing (Smart Test Covid-19 Vyttra and Bio-activity COVID-19). All the samples, with the exception of the employees of C01 and C02 and the physiotherapist's contacts, were seroreactive using the two commercial serological tests.
Discussion
COVID-19 emerged in Tangará da Serra, Mato Grosso, as a result of two cases imported from the state of São Paulo, which at that time was considered to be a place where there was community transmission. These index cases infected their two children by household transmission and C02's physiotherapist at a Pilates session. All the cases were confirmed by serology, while only C01's RT-PCR test was positive, evidencing the risk of this test giving a false negative result. All those involved in the cluster remained in household isolation, thus containing the spread of the disease and providing evidence of the mitigating importance of this action.
Descriptions of clusters during the COVID-19 pandemic have been important for understanding the emergence of the disease, principally for identifying asymptomatic cases and their importance in disseminating the diease.11–13 In a study conducted in China, Bai et al.18 showed that the start of a five-member family cluster was triggered by an asymptomatic case who returned from an area where there was community transmission of the disease, as happened in the situation of infection described here. The study by Huang et al.11 highlights that young individuals are responsible for high levels of infection of their contacts, who mostly are family members or people with whom they have professional contact, as happened between C02 and C05 at the physiotherapy session.
Transmission of the virus to children C03 and C04 arose from direct contract and ties of affection between parents and children. The fact that the children began household isolation immediately after their parents’ first symptoms contributed to containing the disease within the household, avoiding it being spread to their school environment, as at that time lessons had not been suspended, as these were the first suspected cases in the municipality. Chen et al.19 indicate that the threat of an emerging disease can influence the population's behavior and that raising its awareness can delay propagation of the disease.
Raising public awareness is important with regard to propagation of communicable diseases. Individual actions, such as paying greater attention to hygiene and avoiding crowds, can reduce disease propagation, as well as assisting with identification and treatment of new cases and facilitating collective responses.20 Moreover, the fact that the two employees stayed away from the household as soon as the symptoms appeared, may have contributed to preventing these domestic service providers from being infected. In addition, the local government recommendations to close commercial outlets and clinics early, as is the case of Municipal Decree No. 122, on March 17th 2020,21 contributed to the start of C05's social isolation, who at that time did not know that C02 had the disease, reinforcing the importance of local government management in controlling the spread of COVID-19.
The beneficial effects of early isolation of suspected cases and social distancing for communicable disease control is well described in the literature, including in the current COVID-19 pandemic.14 This cluster was the first to be reported in the municipality, and was followed by the appearance of two more imported cases. Since then 20 days have gone by with no record of confirmed cases, i.e. suspected cases have been ruled out by laboratory criteria, emphasizing the ability to control imported cases through household isolation and rigorous health surveillance.
An important fact to be highlighted is that the municipality created a telephone call center to answer queries, receive suggestions and complaints in relation to COVID-19, prior to the first recorded cases, and it was through this service that the population reported that C01 and C02 had returned from a journey to a place where there was community transmission. A study conducted in Hong Kong described how the population perceives high risk of illness and thus adopts self-protection and social mobilization measures to control disease.22
The signs and symptoms reported by the cases (fever, cough, runny nose and dyspnea) corroborate international descriptions,23 as do the CT ground-glass findings for C02. A study indicated that CT sensitivity is high (97%), and that ground-glass opacity was detected in 56.4% of Chinese people with COVID-19.24 Furthermore, laboratory testing, even in the absence of fever, is fundamental, and has been reported in situations of cases without fever,25 such as C01, and in pediatric infections, such as C03 and C04.26,27
In relation to laboratory tests for COVID-19 diagnosis, the possibility of false negative results stands out. A Chinese study indicated that RT-PCR sensitivity in oropharyngeal swab samples varied between 30% and 60%, due to collection method limitations and the collection period, among other factors.28 This fact may explain the negative result of the molecular analysis performed on C02. On the other hand, the rapid test analysis conducted by Li et al.29 in individuals with COVID-19, confirmed by RT-PCR and healthy controls, demonstrated 88.7% sensitivity and 90.6% specificity. This was corroborated by a Brazilian study that analyzed the rapid tests available in the country and found them to be efficacious.30 In this study this was important for laboratory confirmation of C02, C03, C04 and C05.
Serological confirmation, although late, of C03, C04 and C05, reinforces the importance of knowledge about asymptomatic cases and the possible transmission dynamics of the disease, which in this report was contained through household isolation. In turn, the evidence of RT-PCR false negative results raises the need for clinical monitoring by a health professional, as well as the need to retest once ample reflection has been given to diagnostic differentials.
The small sample analyzed is a limitation of this study, but its relevance lies in describing the introduction of the disease in municipality in the interior region of Mato Grosso state based on a cluster. Disease dissemination was contained by household isolation, evidencing the importance of this behavior in containing the expansion of COVID-19 and its early adoption by health services in unaffected municipalities.
In this report on a household cluster, evidence was provided that C01 and C02 were the municipality's imported COVID-19 infection index cases, and that there was local transmission to their children (C03 and C04) and to the physiotherapist (C05). The possibility of COVID-19 cases with negative molecular analysis needs to be taken into consideration and, as such, complementing it with serological testing as a diagnosis tool can contribute to elucidating cases and identifying asymptomatic people. Given the serological evidence and the possibility of a positive result, confirmation of C01 using real-time RT-PCR and serological testing as well points to the complementarity of serological tests which, with adequate interpretation, can be strategic instruments for reducing lack of knowledge about viral agents and assist in COVID-19 control and prevention actions.
We suggest that new studies be conducted to gain knowledge of the dynamics of the expansion of infection/disease, taking into consideration the diverse realities in the Brazilian territory.
Referências
1. Wang C, Horby PW, Hayden FG, Gao GF. A novel coronavirus outbreak of global health concern. Lancet [Internet]. 2020 Feb [cited 2020 Apr 30];395(10223):470-3. Available from: https://doi.org/10.1016/s0140-6736(20)30185-9 [ Links ]
2. Ministério da Saúde (BR). Centro de operações de emergência em Saúde Pública – COVID-19. Painel coronavírus [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 jun 30]. Disponível em: https://covid.saude.gov.br [ Links ]
3. World Health Organization - WHO. Coronavirus disease 2019 (COVID-2019) situation report-108 [Internet]. Geneva: World Health Organization; 2020 [cited 2020 May 7]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ [ Links ]
4. Chan JFW, Yuan S, Kok KH, To KKW, Chu H, Yang J, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: a study of a family cluster. Lancet [Internet]. 2020 Jan [cited 2020 Apr 30];395(10223):514-23. Available from: https://doi.org/10.1016/S0140-6736(20)30154-9 [ Links ]
5. Liu Y, Gayle AA, Wilder-Smith A, Rocklöv J. The reproductive number of COVID-19 is higher 279 compared to SARS coronavirus. J Travel Med [Internet]. 2020 Mar [cited 2020 Apr 30];27(2):taaa021. Available from: https://doi.org/10.1093/jtm/taaa021 [ Links ]
6. Nishiura H, Kobayashi T, Miyama T, Suzuki A, Jung S, Hayashi K, et al. Estimation of the 295 asymptomatic ratio of novel coronavirus infections (COVID-19). Int J Infect Dis [Internet]. 2020 May [cited 2020 Apr 30];94:154-5. Available from: https://doi.org/10.1016/j.ijid.2020.03.020 [ Links ]
7. Wang L, Wang Y, Ye D, Liu Q. A review of the 2019 novel coronavirus (COVID-19) based on current evidence. Int J Antim Age [Internet]. 2020 Jun [cited 2020 Apr 30];55(6):105948. Available from: https://doi.org/10.1016/j.ijantimicag.2020.105948 [ Links ]
8. Zhou P, Yang X-L, Wang X-G, Hu B, Zhang L, Zhang W, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature [Internet]. 2020 Mar [cited 2020 Apr 30];579(7798):270-3. Available from: https://doi.org/10.1038/s41586-020-2012-7 [ Links ]
9. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. Internet]. 2020 Mar [cited 2020 Apr 30];395(10229):1054-62. Available from: https://doi.org/10.1016/S0140-6736(20)30566-3 [ Links ]
10. Li C, Ji F, Wang L, Wang L, Hao J, Dai M, et al. Asymptomatic and human-to-human transmission of SARS-CoV-2 in a 2-family cluster, Xuzhou, China. Emerg Infect Dis[Internet]. 2020 Jul [cited 2020 Apr 30];26(7):1626-8. Available from: https://doi.org/10.3201/eid2607.200718 [ Links ]
11. Huang L, Zhang X, Zhang X, Zhijian W, Lingli Z, Jingli Z, et al. Rapid asymptomatic transmission of COVID-19 during the incubation period demonstrating strong infectivity in a cluster of youngsters aged 16-23 years outside Wuhan and characteristics of young patients with COVID-19: a prospective contact-tracing study. J Infect [Internet]. 2020 Jun [cited 2020 Apr 30];80(6):e1-13. Available from: https://doi.org/10.1016/j.jinf.2020.03.006 [ Links ]
12. Rothe C, Schunk M, Sothmann P, Bretzel G, Froeschl G, Wallrauch C, et al. Transmission of 2019-nCoV infection from an asymptomatic contact in Germany. N Engl J Med 2020 [Internet]. 2020 Mar [cited 2020 Apr 30];382(10):970-1. Available from: https://doi.org/10.1056/nejmc2001468 [ Links ]
13. Phan LT, Nguyen TV, Luong QC, Nguyen TV, Nguyen HT, Le HQ, et al. Importation and human-to-human transmission of a novel coronavirus in Vietnam. N Engl J Med [Internet]. 2020 Feb [cited 2020 Apr 30];382(9):872-4. Available from: https://doi.org/10.1056/nejmc2001272 [ Links ]
14. Chinazzi M, Davis JT, Ajelli M, Gioannini C, Litvinova M, Merler S, et al. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science [Internet]. 2020 Apr [cited 2020 Apr 14];368(6489):395-400. Available from: https://doi.org/10.1126/science.aba9757 [ Links ]
15. Lu S, Lin J, Zhang Z, Xiao L, Jiang Z, Chen J, et al. Alert for non-respiratory symptoms of Coronavirus Disease 2019 (COVID-19) patients in epidemic period: a case report of familial cluster with three asymptomatic COVID-19 patients. J Med Virol [Internet]. 2020 Mar [cited 2020 Apr 14]. Available from: https://doi.org/10.1002/jmv.25776 [ Links ]
16. Instituto Brasileiro de Geografia e Estatística - IBGE. IBGE cidades: Tangará da Serra - MT [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2017 [citado 2020 maio 8]. Disponível em: https://www.ibge.gov.br/cidades-e-estados/mt/tangara-da-serra.html [ Links ]
17. Ministério da Saúde (BR). Cadastro Nacional de Estabelecimento de Saúde (CNES). Tabnet: Brasil [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 maio 8]. Disponível em: http://cnes.datasus.gov.br/ [ Links ]
18. Bai Y, Yao L, Wei T, Tian F, Jin D-Y, Chen L, et al. Presumed asymptomatic carrier transmission of COVID-19. JAMA [Internet]. 2020 Feb [cited 2020 Apr 30];323(14):1406-7. Available from: https://doi.org/10.1001/jama.2020.2565 [ Links ]
19. Chen H, Xu C, Paris C, Reeson A, Li X. Social distance and SARS memory: impact on the public awareness of 2019 novel coronavirus (COVID-19) outbreak. medRxiv [Internet]. 2020 Mar [cited 2020 Apr 30]. Available from: https://doi.org/10.1101/2020.03.11.20033688 [ Links ]
20. Bootsma MCJ, Ferguson NM. The effect of public health measures on the 1918 influenza pandemic in U.S. cities. Proc Nat AcadSci U S A [Internet]. 2007 May [cited 2020 Apr 30];104(18):7588-93. Available from: https://doi.org/10.1073/pnas.0611071104 [ Links ]
21. Prefeitura Municipal de Tangará da Serra (MT). Decreto nº 122, de 17 de março de 2020. Altera e complementa as disposições do Decreto nº 119 de 13 de março de 2020, com medidas temporárias e emergenciais de prevenção de contágio pelo coronavírus (COVID-19) e dá outras providências [Internet]. Tangará da Serra: Prefeitura Municipal de Tangará da Serra; 2020 [citado 2020 jun 30]. Disponível em: https://www.tangaradaserra.mt.gov.br/fotos_downloads/38011.pdf [ Links ]
22. Kwok KO, Li KK, Chan HH, Yi YY, Tang A, Wei WI, et al. Community responses during the early phase of the COVID-19 epidemic in Hong Kong: risk perception, information exposure and preventive measures. medRxi [Internet]. 2020 Feb [cited 2020 Apr 30]. Available from: https://doi.org/10.1101/2020.02.26.20028217 [ Links ]
23. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet [Internet]. 2020 Feb [cited 2020 Apr 30];395(10223):497-506. Available from: https://doi.org/10.1016/S0140-6736(20)30183-5 [ Links ]
24. Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, et al. Clinical characteristics of coronavirus 282 disease 2019 in China. N Engl J Med[Internet]. 2020 Apr [cited 2020 Apr 14];382(18):1708-20. Available from: https://doi.org/10.1056/nejmoa2002032 [ Links ]
25. Wu C, Chen X, Cai Y, Xia J, Zhou X, Xu S, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med [Internet]. 2020 Mar [cited 2020 Apr 30]:e200994. Available from: https://dx.doi.org/10.1001%2Fjamainternmed.2020.0994 [ Links ]
26. Li W, Zhou Q, Tang Y, Ren L, Yu X, Li Q, et al. Protocol for the development of a rapid advice guideline for prevention, management and care of children with 2019 novel coronavirus infection. Ann Palliat Med [Internet]. 2020 Feb [cited 2020 Apr 30];apm.2020.02.33. Available from: https://doi.org/10.21037/apm.2020.02.33 [ Links ]
27. Yang C, Li C, Wang S, National Clinical Research Center for Child Health and Disorders and Children's Oncology Committee of Chinese Research Hospital Association. Clinical strategies for treating pediatric cancer during the outbreak of 2019 novel coronavirus infection. Pediatr Blood Cancer [Internet]. 2020 May [cited 2020 Apr 30];67(5):e28248. Available from: https://doi.org/10.1002/pbc.28248 [ Links ]
28. Ai T, Yang Z, Hou H, Zhan C, Chen C, Lv W, et al. Correlation of chest CT and RT-PCR testing in coronavirus disease 2019 (COVID-19) in China: a report of 1014 cases. Radiology [Internet]. 2020 Feb [cited 2020 Apr 30];200642. Available from: https://doi.org/10.1148/radiol.2020200642 [ Links ]
29. Li Z, Yi Y, Luo X, Xiong N, Liu Y, Li S, et al. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J MedVirol [Internet]. 2020 Feb [cited 2020 Apr 30]. Available from: https://doi.org/10.1002/jmv.25727 [ Links ]
30. Castro R, Luz PM, Wakimoto MD, Veloso V, Grinsztejn B, Perazzo H. COVID-19: a meta-analysis of diagnostic test accuracy of commercial assays registered in Brazil. Braz J Infect Dis [Internet]. 2020 Mar-Apr [cited 2020 Apr 30];24(2):180-7. Available from: https://doi.org/10.1016/j.bjid.2020.04.003 [ Links ]
Received: May 05, 2020; Accepted: May 23, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
