










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.5 Brasília 2020 Epub 22-Set-2020
http://dx.doi.org/10.1590/s1679-49742020000500007
ORIGINAL ARTICLE
Factors associated with dental caries in adolescents: a cross-sectional study, São Paulo State, Brazil, 2015*
1Universidade de São Paulo, Faculdade de Saúde Pública, São Paulo, SP, Brazil
2Universidade Estadual de Campinas, Faculdade de Odontologia de Piracicaba, Piracicaba, SP, Brazil
3Universidade de São Paulo, Faculdade de Odontologia, São Paulo, SP, Brazil
Objective:
To analyze association between prevalence and severity of dental caries and demographic, socioeconomic, behavioral and oral health status in adolescents.
Methods:
This was a cross-sectional study with secondary data on 5,558 adolescents examined in the São Paulo State Oral Health Survey in 2015. The zero-inflated negative binomial regression model was used, considering sample weights. Prevalence ratios (PR), ratios of mean (RM) and confidence intervals (CI) were estimated.
Results:
Caries prevalence was 71.7%, and was higher in females (PR=1.09 - 95%CI 1.04;1.15), associated with being behind at school (PR=1.11 - 95%CI 1.03;1.18), dental calculus (PR=1.10 - 95%CI 1.01;1.20) and no access to fluoridated water (PR=1.21 - 95%CI 1.01;1.45).
Conclusion:
Identification of factors associated with dental caries can instruct the programming of health services aimed at controlling the disease.
Keywords: Dental Caries; Adolescents; Oral Health; Socioeconomic Factors, Cross-Sectional Study
Introduction
Dental caries is still the main oral health problem in Brazil, apart from being the most studied oral disease worldwide. It has a multifactorial etiology and has been described as a social disease. Determinants of its prevalence include biological, dietary, behavioral and socioeconomic factors, as well as factors involving access to durable goods and health services.1 National surveys have shown a scenario of decreasing dental caries, principally among school children.2,3 Studies also point to polarization of dental caries, with absence of the disease in one pole and a large number of cases concentrated in a small group of individuals in the other pole. Presence of caries is increasingly moving away from a uniform distribution, reflecting increasing levels of social inequality.4
Reducing oral health inequities is one of the main challenges imposed on public health policy formulators,5 whereby identification of social determinants of oral health is one of the possible ways of overcoming this difficulty.6 Based on information obtained from epidemiological studies of oral diseases, it is possible to see whether prevalence continues to fall or has stabilized, and whether socioeconomic inequality in disease distribution has continued in the most recent period.
Adolescence is an important transition in the evolution of human beings, a time of biological, cognitive, emotional and social changes, marked by increased autonomy, independence in relation to the family and experimentation of new behaviors and experiences.7 In this stage of life in which growth is rapid, there is a great need for calories, along with greater freedom in choosing what to eat, so that the opportunity arises for high consumption of food containing sugar, this being a risk factor for dental caries which, alongside other factors, such as socioeconomic level, behavior and oral hygiene, contributes to the disease setting in and progressing.8
There is evidence that establishing health promotion measures early, such as during intrauterine life, in childhood and adolescence, improves quality of life in adulthood.9 Epidemiological studies of adolescents, for example, enable the impacts of dental caries to be assessed and thus promote better control of this disease through strategies targeting this population.
The objective of this study was to analyze association between caries prevalence and severity and demographic, socioeconomic, behavioral and oral health status factors in adolescents in São Paulo State in 2015.
Method
This study had a cross-sectional design. It was based on secondary data retrieved from an epidemiological oral health survey entitled ‘São Paulo State Oral Health Survey’ conducted in 2015.10 Our study analyzed data collected in 2015 on 5,558 adolescents aged between 15 and 19 years old who lived in São Paulo State.
The state epidemiological survey used probabilistic sampling, by clusters, in two stages, taking into consideration sample weight and design effect in the respective stages of participant selection. The size of the dental caries sample was defined using the sample calculation formula proposed by Silva,11 which considers the mean and standard deviation values of the variable being studied. The detailed calculation can be found in the final report of the state epidemiological survey.10
The examinations were performed by 250 work teams comprised of dental surgeons and auxiliaries, totaling 550 professionals involved. The teams were trained and calibrated in workshops that lasted 16 hours, with the aim of discussing the operationalization of each stage of the work, the attributions of each participant, and ensuring an acceptable degree of uniformity in the procedures. Percentage intra and inter-examiner agreement was checked in order to ascertain the reproducibility of the study. The consensus technique was used and in the final round the Kappa coefficient was calculated, weighted for each examiner, age group and health condition studied, whereby 0.65 was the minimum acceptable limit. Examiners whose Kappa values were lower than 0.65 were not included in the study. The mean inter-examiner Kappa value was 0.82 for dental caries.10
The DMFT index, considered to be the outcome of this study, represents the mean of the total number of decayed, missing and filled permanent teeth in a population group. In the case of just one individual, the DMFT index is the sum of the conditions found in all their teeth. Through this index we obtained prevalence (DMFT=0; absence of caries and DMFT>0; presence of caries) and severity (DMFT scores varying between 0 and 32) of dental caries in the group studied.
The independent variables, considered in order to assess associated factors, were classified into five blocks conceptually organized as follows:
Demographic characteristics (age; gender; race/skin color, self-reported);
Socioeconomic status (household crowding; family income; number of durable goods in the household);
Behavioral status (behind at school);
Oral health status (gum bleeding on probing; dental calculus); and
Access to fluoridated water.
Household crowding was measured as the number of residents per bedroom in the household, categorized into less than two (less crowded households) and two or more (more crowded households). Family income was assessed according to amount categories, expressed in Brazilian Reals (BRL) (in the data collection reference period, one United States dollar corresponded to BRL 3.10). With regard to the number of durable goods in the household, this was informed by means of a standard questionnaire, including items such as refrigerators, radios, televisions etc.
The ‘behind at school’ variable was dichotomous, differentiating adolescents at least one year behind in relation to the number of school years expected for the corresponding age (11 school years for adolescents aged 18 and 19; 10 school years for those aged 17; 9 school years for those aged 16; 8 school years for those aged 15). Adolescents behind at school also included adolescents who, for whatever reason, left formal education before completing high school. This variable has also been incorporated into the overall assessment of the human development index in Brazil.12
Measurement of prevalence of untreated caries, gum bleeding on probing and dental calculus was obtained by means of mouth examination. Access to fluoridated water was also assessed in a dichotomous manner, based on municipalities that did or did not have a fluoridated public water supply.13 Pronounced non-normal DMF distribution, biased to the left, required the use of zero-inflated regression models. Given that this form of presenting the data implies a large concentration of individuals with zero DMFT (free from caries), this justified the choice of the zero-inflated negative binomial regression model in order to obtain greater accuracy in the statistical analysis and exactness of the knowledge generated.
Descriptive statistics were performed. Prevalence ratios (PR) and ratios of mean (RM) were estimated, with their crude values and respective 95% confidence intervals (95%CI).
A zero-inflated negative binomial regression model was used to study association between dental caries distribution and exposure variables of interest. This model was used to calculate PRs in order to identify variables associated with caries prevalence, as well as being used to calculate RMs, in order to indicate factors associated with the number of teeth affected by caries (severity). All the variables of interest were included in the multiple regression model, regardless of fit quality.
The statistical analyses were performed using the Stata version 15.0 computer program (College Station, Texas, USA, 2017), in the survey mode, considering the complex structure of the survey (cluster sampling) and respective sampling weights.
The study project was approved by the São Paulo University Public Health Faculty Research Ethics Committee (CEP/FSP/USP) on May 23rd 2017: Opinion No. 2.078.896; Certificate of Submission for Ethical Appraisal (CAEE) No. 66076517.6.0000.5421.
Results
The DMFT index found among the 15-19-year-old adolescents was 3.76; while caries prevalence was 71.7%. Figure 1 shows the DMFT index distribution and the high concentration of individuals with zero DMFT, i.e. free from caries. Table 1 characterizes the sample.
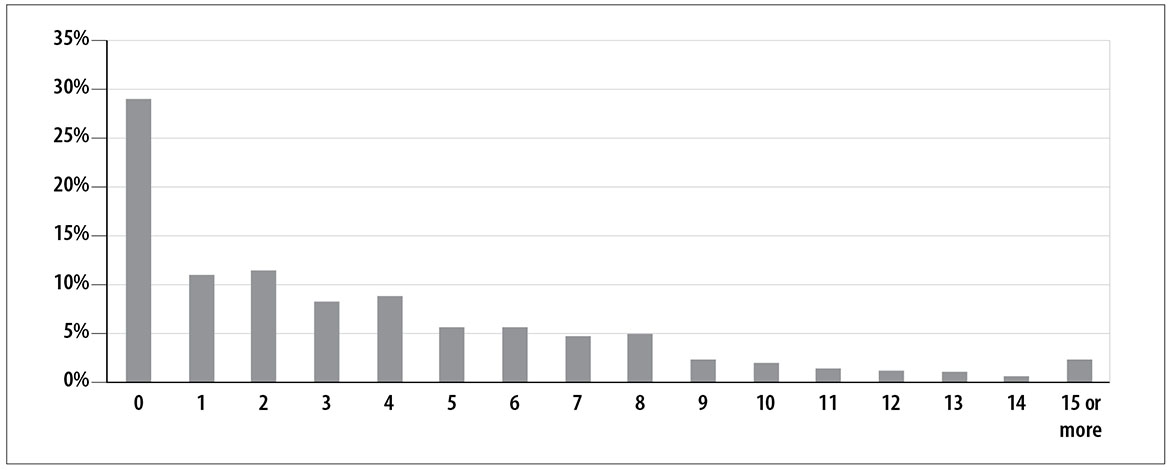
Figure 1 - Percentage distribution of number of decayed, missing and filled teeth (DMFT index) in adolescents (15-19 years old), São Paulo State, 2015
Table 1 - Demographic, socioeconomic, behavioral and tooth brushing quality characteristics in adolescents (15-19 years old), São Paulo State, 2015
| Variables | n | Percentage in the weighted sample | Caries prevalence (%) | DMFTa (95% CI)b |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Gender | ||||
| Male | 2,405 | 43.27 | 67.43 | 3.22 (2.91;3.52) |
| Female | 3,153 | 56.73 | 73.79 | 3.84 (3.45;4.23) |
| Age (years) | ||||
| 15 | 1,546 | 27.81 | 62.03 | 2.76 (2.47;3.05) |
| 16 | 1,081 | 19.45 | 67.41 | 2.99 (2.59;3.40) |
| 17 | 908 | 16.34 | 76.07 | 4.21 (3.64;4.78) |
| 18 | 918 | 16.52 | 73.28 | 3.73 (3.14;4.31) |
| 19 | 1,105 | 19.88 | 76.99 | 4.61 (4.03;5.10) |
| Race/skin color | ||||
| White | 3,357 | 60.41 | 69.09 | 3.38 (3.09;3.67) |
| Black | 412 | 7.42 | 72.63 | 3.65 (3.08;4.22) |
| Yellow | 57 | 1.02 | 80.95 | 6.46 (2.41;10.52) |
| Brown | 1,722 | 30.98 | 74.20 | 3.83 (3.39;4.27) |
| Indigenous | 10 | 0.17 | 55.59 | 2.55 (0.30;4.80) |
| Socioeconomic status | ||||
| Household crowding | ||||
| Up to 2 people | 3,891 | 70.00 | 69.15 | 3.48 (3.17;3.79) |
| 2 or more | 1,667 | 30.00 | 75.45 | 3.78 (3.32;4.24) |
| Family income | ||||
| Up to BRL 1500 | 1,964 | 35.34 | 72.47 | 3.90 (3.54;4.26) |
| BRL 1501 to BRL 2500 | 1,484 | 26.71 | 69.03 | 3.34 (2.90;3.78) |
| BRL 2501 or more | 2,110 | 37.95 | 71.12 | 3.43 (2.94;3.91) |
| Number of durable goods in the household | ||||
| Up to 8 | 3,157 | 56.81 | 73.97 | 3.92 (3.57;4.28) |
| 9 or more | 2,401 | 43.19 | 67.19 | 3.11 (2.75;3.47) |
| Behavioral status | ||||
| Behind at school | ||||
| No | 4,300 | 77.38 | 68.45 | 3.28 (2.96;3.59) |
| Yes | 1,258 | 22.62 | 79.90 | 4.58 (3.88;5.28) |
| Oral health status | ||||
| Gum bleeding on probing | ||||
| No | 3,696 | 66.51 | 69.25 | 3.25 (2.97;3.52) |
| Yes | 1,862 | 33.49 | 74.59 | 4.21 (3.70;4.72) |
| Dental calculus | ||||
| No | 3,810 | 68.55 | 68.16 | 3.25 (2.94;3.56) |
| Yes | 1,748 | 31.45 | 77.31 | 4.27 (3.87;4.67) |
| Access to fluoridated water | ||||
| Yes | 5,478 | 99.40 | 70.95 | 3.55 (3.24;3.86) |
| No | 80 | 0.60 | 85.12 | 7.10 (4.41;9.78) |
| Total | 5,558 | 100.00 | 71.04 | 3.57 (3.26;3.88) |
a) DMFT: number of decayed, missing and filled teeth.
b) 95%CI: 95% confidence interval.
Analysis of non-adjusted associations with dental caries prevalence and severity is shown in Table 2. Females were found to have higher caries prevalence (PR=1.09 - 95%CI 1.04;1.16) and greater caries severity (RM=1.11 - 95%CI 1.01;1.22 [Table 3]), when compared to males. Dental caries prevalence and severity was found to increase as age increased. No statistically significant differences were found in the ‘race/skin color’ variable categories. With regard to socioeconomic status, adolescents who lived in an environment where there was more household crowding had higher dental caries prevalence (PR=1.09 - 95%CI 1.03;1.15), although no difference in caries severity was found among these individuals. Adolescents from households with family income below BRL 1500 had more severe caries, and fewer durable goods in their households was associated with greater dental caries prevalence and severity.
Table 2 - Estimated prevalence ratio and confidence interval values for dental caries, in the crude analysis and in the adjusted zero-inflated negative binomial regression, in adolescents (15-19 years old), São Paulo State, 2015
| Variables | PRa | 95%CIb | p-valuec | PRad | 95%CIb | p-valuec |
|---|---|---|---|---|---|---|
| Demographic characteristics | ||||||
| Gender | ||||||
| Male | 1.00 | 1.00 | ||||
| Female | 1.09 | 1.04;1.16 | <0.001 | 1.09 | 1.04;1.15 | 0.001 |
| Age (years) | ||||||
| 15 | 1.00 | 1.00 | ||||
| 16 | 1.04 | 0.92;1.16 | 0.546 | 1.04 | 0.93;1.16 | 0.457 |
| 17 | 1.17 | 1.06;1.29 | 0.001 | 1.13 | 1.03;1.24 | 0.006 |
| 18 | 1.13 | 1.02;1.24 | 0.014 | 1.09 | 0.99;1.19 | 0.076 |
| 19 | 1.18 | 1.09;1.28 | <0.001 | 1.13 | 1.04;1.22 | 0.003 |
| Race/skin color | ||||||
| White | 1.00 | 1.00 | ||||
| Black | 1.05 | 0.95;1.16 | 0.341 | 1.03 | 0.93;1.14 | 0.611 |
| Yellow | 1.17 | 0.88;1.55 | 0.271 | 1.05 | 0.88;1.25 | 0.488 |
| Brown | 1.07 | 0.99;1.16 | 0.082 | 1.05 | 0.98;1.14 | 0.205 |
| Indigenous | 0.80 | 0.39;1.65 | 0.550 | 0.83 | 0.41;1.66 | 0.596 |
| Socioeconomic status | ||||||
| Household crowding | ||||||
| Up to 2 | 1.00 | 1.00 | ||||
| 2 or more | 1.11 | 1.00;1.23 | 0.002 | 1.07 | 1.00;1.14 | 0.041 |
| Family income | ||||||
| Up to BRL 1500 | 1.00 | 1.00 | ||||
| BRL 1501 to BRL 2500 | 0.95 | 0.88;1.03 | 0.236 | 0.97 | 0.90;1.05 | 0.551 |
| BRL 2501 or more | 0.98 | 0.87;1.11 | 0.760 | 1.00 | 0.90;1.12 | 0.963 |
| Number of durable goods in the household | ||||||
| Up to 8 | 1.00 | 1.00 | ||||
| 9 or more | 0.91 | 0.85; 0.97 | 0.005 | 0.94 | 0.88;0.99 | 0.058 |
| Behavioral status | ||||||
| Behind at school | ||||||
| No | 1.00 | 1.00 | ||||
| Yes | 1.17 | 1.09;1.25 | <0.001 | 1.11 | 1.03;1.18 | 0.004 |
| Oral health status | ||||||
| Gum bleeding on probing | ||||||
| No | 1.00 | 1.00 | ||||
| Yes | 1.08 | 1.00;1.16 | 0.04 | 1.00 | 0.92;1.09 | 0.939 |
| Dental calculus | ||||||
| No | 1.00 | 1.00 | ||||
| Yes | 1.13 | 1.06;1.21 | <0.001 | 1.10 | 1.01;1.20 | 0.025 |
| Access to fluoridated water | ||||||
| Yes | 1.00 | 1.00 | ||||
| No | 1.20 | 0.96;1.49 | <0.001 | 1.21 | 1.01;1.45 | <0.001 |
a) PR: prevalence ratio.
b) 95%CI: 95% confidence interval.
c) Regression coefficient t-test.
d) Adjusted prevalence ratio.
Note: Values adjusted for all the variables in the model.
The behavioral status of being behind at school was associated with greater dental caries prevalence (PR=1.17 - 95%CI 1.09;1.25) and severity (RM=1.23 - 95%CI 1.03;1.47).
With regard to oral health status, bleeding gums were found to be associated with caries severity (RM=1.24 - 95%CI 1.11;1.39), while dental calculus was associated with prevalence (PR=1.13 - 95%CI 1.06;1.21) and severity (RM=1.19 - 95%CI 1.06;1.33). Regarding access to fluoridated water, greater dental caries prevalence and severity were found among those who did not have access: PR=1.20 - 95%CI 0.96;1.49 (for prevalence) and RM=1.77 - 95%CI 1.51;2.08 (for severity).
After adjusting the model (Table 3), dental caries prevalence was found to be greater in females, although greater severity in this group was not significant. With regard to age, there was statistically significant difference in the 17 and 18 year age groups. In relation to socioeconomic status, household crowding was not found to be associated with caries prevalence and severity. However, family income below BRL 1500 was associated with greater severity, while having fewer than 8 durable goods in the household was associated with greater prevalence.
Table 3 - Estimated ratio of mean and confidence interval values for dental caries, in the crude analysis and in the adjusted zero-inflated negative binomial regression, in adolescents (15-19 years old), São Paulo State, 2015
| Variables | RMa | 95%CIb | p-valuec | RMad | 95%CIb | p-valuec |
|---|---|---|---|---|---|---|
| Demographic characteristics | ||||||
| Gender | ||||||
| Male | 1.00 | 1.00 | ||||
| Female | 1.11 | 1.01;1.22 | 0.037 | 1.07 | 0.98;1.18 | 0.138 |
| Age (years) | ||||||
| 15 | 1.00 | 1.00 | ||||
| 16 | 1.06 | 0.94;1.18 | 0.34 | 1.07 | 0.95;1.20 | 0.288 |
| 17 | 1.37 | 1.20;1.55 | <0.001 | 1.29 | 1.16;1.43 | <0.001 |
| 18 | 1.24 | 1.07;1.43 | 0.004 | 1.20 | 1.04;1.39 | 0.012 |
| 19 | 1.49 | 1.34;1.66 | <0.001 | 1.40 | 1.23;1.59 | <0.001 |
| Race/skin color | ||||||
| White | 1.00 | 1.00 | ||||
| Black | 1.03 | 0.89;1.19 | 0.667 | 1.00 | 0.86;1.15 | 0.939 |
| Yellow | 1.74 | 1.19;2.54 | 0.005 | 1.35 | 1.01;1.83 | 0.054 |
| Brown | 1.06 | 0.98;1.16 | 0.139 | 1.04 | 0.95;1.13 | 0.288 |
| Indigenous | 0.92 | 0.64;1.33 | 0.673 | 1.02 | 0.65;1.60 | 0.981 |
| Socioeconomic status | ||||||
| Household crowding | ||||||
| Up to 2 | 1.00 | 1.00 | ||||
| 2 or more | 1.08 | 0.90;1.09 | 0.896 | 1.07 | 0.98;1.17 | 0.765 |
| Family income | ||||||
| Up to BRL 1500 | 1.00 | 1.00 | ||||
| BRL 1501 to BRL 2500 | 0.88 | 0.80;0.98 | 0.016 | 0.91 | 0.82;0.99 | 0.049 |
| BRL 2501 or more | 0.88 | 0.80;0.97 | 0.008 | 0.89 | 0.78;0.99 | 0.054 |
| Number of durable goods in the household | ||||||
| Up to 8 | 1.00 | 1.00 | ||||
| 9 or more | 0.85 | 0.77;0.94 | 0.001 | 0.91 | 0.81;1.02 | 0.136 |
| Behavioral status | ||||||
| Behind at school | ||||||
| No | 1.00 | 1.00 | ||||
| Yes | 1.23 | 1.03;1.47 | 0.020 | 1.07 | 0.92;1.24 | 0.298 |
| Oral health status | ||||||
| Gum bleeding on probing | ||||||
| No | 1.00 | 1.00 | ||||
| Yes | 1.24 | 1.11;1.39 | <0.001 | 1.15 | 1.02;1.30 | 0.018 |
| Dental calculus | ||||||
| No | 1.00 | 1.00 | ||||
| Yes | 1.19 | 1.06;1.33 | 0.004 | 1.04 | 0.91;1.19 | 0.549 |
| Access to fluoridated water | ||||||
| Yes | 1.00 | 1.00 | ||||
| No | 1.77 | 1.51;2.08 | <0.001 | 1.81 | 1.56;2.09 | <0.001 |
a) RM: ratio of mean.
b) 95%CI: 95% confidence interval.
c) Regression coefficient t-test.
d) Adjusted ratio of mean.
Nota: Values adjusted for all the variables in the model.
Being behind at school only remained associated with greater caries prevalence (PR=1.11 - 95%CI 1.03;1.18). With regard to health status, bleeding gums remained associated with caries severity, while dental calculus only remained associated with prevalence. Access to fluoridated water was associated with both dental caries prevalence and severity.
Discussion
The results of this study indicate that the female sex, being older, lower family income, fewer durable goods in the household, being behind at school, oral health status (bleeding gums and dental calculus) and lack of access to fluoridated water were associated with greater dental caries prevalence and/or severity.
Dental caries inequalities among entre adolescents continue to be a reality. The results showed that having lower family income and fewer durable goods in the household were associated with greater dental caries prevalence and severity. A systematic review published in 2018,14 looked for consistent evidence of association between contextual social inequalities and occurrence of dental caries in adolescents, and found articles revealing significant association between contextual socioeconomic factors and caries, demonstrating the importance of these variables in the development of the disease.
A study conducted in Sweden in 2009,15 concluded that socioeconomic factors were associated with dental caries experience in children and adolescents, when used as single factors or combined in an index. Another cohort study published in 2020 and conducted with 1134 12-year-old adolescents in Southern Brazil,16 found that adolescents of lower socioeconomic status and poor schooling contexts had higher rates of dental caries; and that non-White adolescents who had fewer dental appointments, dental plaque and whose parents had little perception of children’s oral health, were also associated with greater dental caries incidence.
Despite this context of inequalities in dental caries distribution, when the results of this study are compared with another study also conducted with adolescents in São Paulo State, in 2002, a falling trend in dental caries among adolescents in this age group can be seen.17
Notwithstanding, the caries burden remains in all age ranges. Dental caries can start at an early age, continue though childhood and adolescence and become more severe in adult life, resulting in tooth loss and consequent deterioration in quality of life.18 This study found statistical difference between the ages analyzed in relation to caries prevalence and severity, thus showing its cumulative effect. Addressing caries in adolescence is therefore important, as it can indicate factors that predict tooth loss in adult life.
A cross-sectional study that analyzed data on adolescents examined during a national oral health epidemiological survey in China in 2016,19 found an annual increase of 3% in dental caries prevalence and an annual DMFT increase of 0.15 between 12 years of age and 14 years of age, thus suggesting an increase in the caries burden as individuals become older.
Dental caries prevalence was higher among females. This finding could be explained by early permanent teeth eruption in girls and, consequently, their greater exposure time to the cariogenic environment.20 According to a systematic review of the social determinants of health and dental caries in Brazil, focusing on the period between 1999 and 2010,21 the studies consulted indicated greater caries occurrence in females; however, only 25% of those associations were statistically significant.
No statistically significant associations were found between race/skin color and dental caries prevalence/severity. This result may possibly be explained by the fact of the socioeconomic variables being strongly associated with dental caries and thus, when adjusted, the weight of social and economic conditions being greater than that of ethnic and racial conditions. On the other hand, other studies have found differences between race/color, whereby Whites had lower dental caries rates than other racial groups.22,23
Level of schooling can affect health by favoring accumulation of knowledge and can influence adoption of healthy habits. As such, the choice of the being ‘behind at school’ variable is justified in this study. Moreover, statistically significant association between level of schooling and greater dental caries prevalence has been demonstrated previously.24
The results of this study showed greater dental caries prevalence and severity among adolescents without access to fluoridated water. Despite the context of declining dental caries and the common use of fluoride toothpaste, the benefits attributed to adding fluoride do not justify this water treatment method being discontinued or even not being scaled up. A population-based study conducted between 2012 and 2014 with Australian children and adolescents,25 found consistent associations between exposure to fluoridated water and dental caries, which remained even when socioeconomic differences were adjusted between the exposure groups, thus supporting the efficacy of continuing with this procedure. Narvai26 also found lower mean caries rates in 11-12-year-old adolescents, when comparing two municipalities in São Paulo State with and without exposure to fluoridated water, even when there was concomitant exposure to fluoride toothpaste, in a scenario of low caries prevalence. Fluoridation of the public water supply has therefore been identified as an environmental variable with the potential to explain the lower magnitude of the DMFT index among people with access to this benefit.
The results of this study pointed to association between bleeding gums and dental caries severity, while dental calculus was associated with greater caries prevalence. This positive association could be explained by the presence of common risk factors, including poor oral hygiene, social and behavioral determinants.27 A 3-year longitudinal study conducted with adolescents revealed that caries had a negative effect on periodontal health.28 Although in terms of etiology, caries and gingivitis are considered mutually independent, presence of sucrose could associate both diseases. Sucrose increases formation of plaque above the gum line, this being a prerequisite for the development of plaque below the gum line which can induce periodontal disease.29 As there are few publications in the literature about association between sucrose, caries and periodontal disease, we suggest that further studies be conducted to elucidate this question.
The limitations of this study include its cross-sectional nature: the information refers to a single moment in time, and does not enable considerations about causality or how much the disease develops over a given period of time.
This study considered access to fluoridation as an individual variable, estimating that all children in municipalities with a fluoridated water supply had access to this benefit. The dichotomous assessment of fluoridation in the municipalities (with fluoridation; without fluoridation), without due control of recommended levels, as this information was not available for analysis, was another limitation of this study. Even before the microbial etiology of dental caries and its strong association with frequent sugar consumption had been proven, fluoride was the first exogenous factor recognized as being important for modifying risk of the disease30 and as such, in view of the acknowledged impact of this measure on dental caries prevention, it is important to include this variable in the statistical model. Moreover, it should be stressed that the sample was representative of the age group studied, thus allowing extrapolation of the study data and ensuring their external validity.
We conclude that inequities in dental caries distribution among adolescents in São Paulo State persist and are a challenge to adopting protection and prevention measures with the aim of improving their oral health status. The study also identified the most relevant factors associated with dental caries prevalence and severity in these young people. The information reported can guide both the planning of health action programs aimed at oral health disease control and improvement, and also approaches targeting common risk factors in order to avoid oral diseases.
REFERENCES
1. Frias AC, Antunes JLF, Junqueira SR, Narvai PC. Determinantes individuais e contextuais da prevalência de cárie dentária não tratada no Brasil. Rev Panam Salud Publica [Internet]. 2007 [citado 2020 jul 6];22(4):279-85. Disponível em: Disponível em: https://scielosp.org/article/rpsp/2007.v22n4/279-285/ [ Links ]
2. Ministério da Saúde (BR). Secretaria de Atenção a Saúde. Departamento de Atenção Básica. Projeto SB Brasil 2003: condições de saúde bucal da população brasileira 2002- 2003: resultados principais [Internet]. Brasília: Ministério da Saúde; 2004 [citado 2020 jul 6]. 51 p. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/condicoes_saude_bucal.pdf [ Links ]
3. Ministério da Saúde (BR). Secretaria de Atenção a Saúde. Departamento de Atenção Básica. Projeto SB Brasil 2010: resultados principais [Internet]. Brasília: Ministério da Saúde ; 2011 [citado 2020 jul 6]. 92 p. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/SBBrasil_2010.pdf [ Links ]
4. Narvai PC, Frazão P, Roncalli AG, Antunes JLF. Cárie dentária no Brasil: declínio, polarização, desigualdade e exclusão social. Rev Panam Salud Publica [Internet]. 2006 [citado 2020 jul 6];19(6):385-93. Disponível em: Disponível em: https://scielosp.org/pdf/rpsp/2006.v19n6/385-393/pt [ Links ]
5. Watt RG. From victim blaming to upstream action: 8. tackling the social determinants of oral health inequalities. Community Dent Oral Epidemiol [Internet]. 2007 Jan [cited 2020 Jul 6];35(1):1-11. Available from: Available from: https://doi.org/10.1111/j.1600-0528.2007.00348.x [ Links ]
6. Williams DM. Global oral health inequalities: the research agenda. Adv Dent Res [Internet]. 2011 May [cited 2020 Jul 6];23(2):198-200. Available from: Available from: https://doi.org/10.1177/0022034511402014 [ Links ]
7. Organização Mundial de Saúde - OMS. Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey [Internet]. Copenhagen: WHO Regional Office for Europe; 2012 [cited 2020 Jul 6]. (Health Policy for Children and Adolescents, No. 6). Available from: Available from: https://www.euro.who.int/en/publications/abstracts/social-determinants-of-health-and-well-being-among-young-people.-health-behaviour-in-school-aged-children-hbsc-study [ Links ]
8. Pitts N, Amaechi B, Niederman R, Acevedo AM, Vianna R, Ganss C, et al. Global oral health inequalities: dental caries task group--research agenda. Adv Dent Res [Internet]. 2011 May [cited 2020 Jul 6];23(2):211-20. Available from: Available from: https://doi.org/10.1177/0022034511402016 [ Links ]
9. Sawyer SM, Afifi RA, Bearinger LH, Blakemore SJ, Dick B, Ezeh AC, et al. Adolescence: a foundation for future health. Lancet [Internet]. 2012 Apr [cited 2020 Jul 6];379(9826):1630-40. Available from: Available from: https://doi.org/10.1016/s0140-6736(12)60072-5 [ Links ]
10. Secretaria do Estado de São Paulo. Universidade Estadual de Campinas. SB São Paulo 2015: pesquisa estadual de saúde bucal - relatório final [Internet]. Piracicaba: Unicamp; 2016 [citado 2020 jul 6]. 64 p. Disponível em: Disponível em: https://pesquisa.bvsalud.org/ses/resource/pt/ses-33751 [ Links ]
11. Silva NN. Amostragem probabilística. São Paulo: EDUSP; 1998. 124 p. [ Links ]
12. Programa das Nações Unidas para o Desenvolvimento - PNUD. Instituto de Pesquisa Econômica Aplicada. Relatório do desenvolvimento humano no Brasil [Internet]. Brasília: Fundação João Pinheiro; 2003 [citado 2020 jul 6]. Disponível em: Disponível em: https://www.br.undp.org/content/brazil/pt/home/library/idh/relatorios-de-desenvolvimento-humano/relatorio-do-desenvolvimento-humano-20003.html [ Links ]
13. Instituto Brasileiro de Geografia e Estatística - IBGE. Coordenação de População e Indicadores Sociais. Pesquisa nacional de saneamento básico 2008 [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2010 [citado 2020 jul 6]. Disponível em: Disponível em: https://www.ibge.gov.br/estatisticas/multidominio/meio-ambiente/9073-pesquisa-nacional-de-saneamento-basico.html?=&t=sobre [ Links ]
14. Nóbrega J, Dantas E, Ferreira-Filho JC, Limão N, Rodrigues-de-Melo AC, Protásio AP, et al. Contextual social inequities and occurrence of dental caries in adolescents: a systematic review. Oral Health Prev Dent [Internet]. 2017 [cited 2020 Jul 6];15(4):329-36. Available from: Available from: https://doi.org/10.3290/j.ohpd.a38744 [ Links ]
15. Kramer AC, Petzold M, Hakeberg M, Östberg AL. Multiple socioeconomic factors and dental caries in swedish children and adolescents. Caries Res [Internet]. 2018 [cited 2020 Jul 6];52(1-2):42-50. Available from: Available from: https://doi.org/10.1159/000481411 [ Links ]
16. Ortiz AS, Tomazoni F, Knorst JK, Ardenghi TM. Influence of socioeconomic inequalities on levels of dental caries in adolescents: a cohort study. Int J Paediatr Dent [Internet]. 2020 Jan [cited 2020 Jul 6];30(1):42-9. Available from: Available from: https://doi.org/10.1111/ipd.12572 [ Links ]
17. Gushi LL, Soares MC, Forni TIB, Vieira V, Wada RS, Sousa MLR. Cárie dentária em adolescentes de 15 a 19 anos de idade no Estado de São Paulo, Brasil, 2002. Cad Saúde Pública [Internet]. 2005 set-out [citado 2020 jul 6];21(5):1383-91. Disponível em: Disponível em: https://doi.org/10.1590/S0102-311X2005000500010 [ Links ]
18. Peres MA, Peres KG, Demarco FF. Saúde bucal no ciclo vital - acúmulos de risco ao longo da vida. In: Antunes JLF, Peres MA. Epidemiologia da saúde bucal. 2. ed. São Paulo: Santos; 2015. parte 2, cap. 2, p. 420. [ Links ]
19. Hu J, Jiang W, Lin X, Zhu H, Zhou N, Chen Y, et al. Dental caries status and caries risk factors in students ages 12-14 years in Zhejiang, China. Med Sci Monit [Internet]. 2018 Jun [cited 2020 Jul 6];24:3670-8. Available from: Available from: https://doi.org/10.12659/msm.907325 [ Links ]
20. Lukacs JR, Largaespada LL. Explaining sex differences in dental caries prevalence: saliva, hormones, and “life-history” etiologies. Am J Hum Biol [Internet]. 2006 Jul-Aug [cited 2020 Jul 6];18(4):540-55. Available from: Available from: https://doi.org/10.1002/ajhb.20530 [ Links ]
21. Boing AF, Bastos JL, Peres KG, Antunes JLF, Peres MA. Social determinants of health and dental caries in Brazil: a systematic review of the literature between 1999 and 2010. Rev Bras Epidemiol [Internet]. 2014 [cited 2020 Jul 6];17 Suppl 2:102-15. Available from: Available from: https://doi.org/10.1590/1809-4503201400060009 [ Links ]
22. Antunes JLF, Pegoretti T, Andrade FP, Junqueira SR, Frazão P, Narvai PC. Ethnic disparities in the prevalence of dental caries and restorative dental treatment in Brazilian children. Int Dent J [Internet]. 2003 Feb [cited 2020 Jul 6];53(1):7-12. Available from: Available from: https://doi.org/10.1111/j.1875-595x.2003.tb00649.x [ Links ]
23. Drummond AM, Ferreira EF, Gomes VE, Marcenes W. Inequality of experience of dental caries between different ethnic groups of brazilians aged 15 to 19 years. PLoS One [Internet]. 2015 Dec [cited 2020 Jul 6];10(12):e0145553. Available from: Available from: https://dx.doi.org/10.1371%2Fjournal.pone.0145553 [ Links ]
24. Boing AF, Kovaleski DF, Antunes JLF. Medidas de condições socioeconômicas em estudos epidemiológicos de saúde bucal. In: Antunes JLF, Peres MA. Epidemiologia da saúde bucal. Rio de Janeiro: Guanabara Koogan; 2006. cap. 1, parte 2, p. 235-48. [ Links ]
25. Spencer AJ, Do LG, Ha DH. Contemporary evidence on the effectiveness of water fluoridation in the prevention of childhood caries. Community Dent Oral Epidemiol [Internet]. 2018 Aug [cited 2020 Jul 6];46(4):407-15. Available from: Available from: https://doi.org/10.1111/cdoe.12384 [ Links ]
26. Cruz MGB, Narvai PC. Caries and fluoridated water in two Brazilian municipalities with low prevalence of the disease. Rev Saúde Pública [Internet]. 2018 Apr [cited 2020 Jul 6];52:28. Available from: Available from: https://doi.org/10.11606/s1518-8787.2018052016330 [ Links ]
27. Durand R, Roufegarinejad A, Chandad F, Rompré PH, Voyer R, Michalowicz BS, et al. Dental caries are positively associated with periodontal disease severity. Clin Oral Investig [Internet]. 2019 Jan [cited 2020 Jul 6];23(10):3811-9. Available from: Available from: https://doi.org/10.1007/s00784-019-02810-6 [ Links ]
28. Albandar JM, Buischi YA, Axelsson P. Caries lesions and dental restorations as predisposing factors in the progression of periodontal diseases in adolescents. A 3-year longitudinal study. J Periodontol [Internet]. 1995 Apr [cited 2020 Jul 6];66(4):249-54. Available from : Available from : https://doi.org/10.1902/jop.1995.66.4.249 [ Links ]
29. Rebelo MAB. Estudo in situ da composição bioquímica da placa dental em função da frequência diária do uso de sacarose [dissertação]. Piracicaba (SP): Universidade Estadual de Campinas, Faculdade de Odontologia de Piracicaba ; 1994. Disponível em: http://repositorio.unicamp.br/jspui/handle/REPOSIP/289287 [ Links ]
30. Antunes JLF, Narvai PC. Políticas de saúde bucal no Brasil e seu impacto sobre as desigualdades em saúde. Rev Saúde Pública [Internet]. 2010 abr [citado 2020 jul 6];44(2):360-5. Disponível em: Disponível em: https://doi.org/10.1590/S0034-89102010005000002 [ Links ]
*Article derived from the Ph.D. thesis entitled ‘Fators associated with dental caries and dental impact on the everyday activities of 15-19-year-old adolescentes, São Paulo State, 2015’, defended by Lívia Litsue Gushi Corrêa at the University of São Paulo Public Health Faculty Epidemiology Postgraduate Program (FSP/USP) in 2019.
Received: January 08, 2020; Accepted: June 10, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
