










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.5 Brasília 2020 Epub 30-Oct-2020
http://dx.doi.org/10.1590/s1679-49742020000500016
Original article
Addressing chronic noncommunicable diseases in primary health care in Goiás, Brazil: a descriptive study, 2012 and 20141
1Universidade Federal de Goiás, Instituto de Patologia Tropical e Saúde Pública, Goiânia, GO, Brazil.
Objective:
To compare primary health care (PHC) actions taken to care for chronic non-communicable diseases (NCDs) in the state of Goiás, Brazil, between 2012 and 2014.
Methods:
This was a descriptive study using secondary data from the National Program for Improving Primary Care Access and Quality (PMAQ-AB). The proportions of teams performing actions to address NCDs were compared between PMAQ-AB cycles I and II using the McNemar test for paired samples.
Results:
Seventeen of the 20 variables studied showed a proportional increase between the two cycles: from 16.0% to 32.1% of teams that practiced all care management actions, from 21.5% to 35.2% of those that practiced all health promotion actions and from 22.2% to 39.8% of teams that practiced all activities at school.
Keywords: Primary Health Care; Chronic Disease; Health Evaluation; Epidemiology, Descriptive
Introduction
Primary Health Care (PHC), the preferential point of entry to the Brazilian National Health System (SUS), has drawn the attention of the debate on the work process aimed at addressing chronic noncommunicable diseases (NCDs). So far, PHC, which has the Family Health Strategy as its main model of action, is not able to provide comprehensive and continuing care capable of countering the heavy burden that NCDs represent for Brazil.1
NCDs affect all nations and social classes, with the majority of deaths attributed to them being concentrated in middle and low-class populations.2 This group of diseases accounted for 73.4% of total deaths worldwide in 2017.3
In Brazil, NCDs accounted for 75.0% of total deaths in 2015 and their main groups of causes were: diseases of the circulatory system; cancer; chronic respiratory disease; and diabetes.4 These four groups share the main risk factors for chronic diseases: inadequate diet; tobacco smoking; physical inactivity; and abusive alcohol consumption.5
The high burden of NCDs deaths in Brazil is the result of the demographic transition the country has gone though, as well accelerated aging arising from reduced fertility/birth rates and reduced mortality in all age groups. In 2010, there were 19.6 million Brazilians aged 60 or over. It is estimated that this age group will account for approximately 41.5 million in 2030.6
A noteworthy initiative to reduce the NCDs burden in Brazil is the ‘Strategic action plan to address chronic noncommunicable diseases in Brazil, 2011-2022’. This plan prioritizes the development of public policies on health promotion, prevention and comprehensive care, aimed at controlling NCDs and their risk factors. The guidelines proposed involve PHC as an important strategy for producing comprehensive and continuing care.7
Within this context, the National Program for Improving Primary Care Access and Quality (PMAQ-AB), initiated in 2011, linked the funding of PHC teams to health management and health care quality standards.8 PMAQ-AB has four stages: (i) adherence and agreement setting, (ii) development, (iii) external evaluation and (iv) agreement resetting. The program’s external evaluation instruments contain questions covering several different parameters, related to Primary Health Care Center infrastructure and Family Health team work processes.1, 8 Several of these questions refer to NCDs-related actions.
Some studies1, 9-11 have used PMAQ-AB to evaluate actions to address NCDs, but none of them have characterized activities undertaken in the state of Goiás. In order to fill this gap, the objective of this study was to compare PHC actions taken to care for NCDs in the state of Goiás, Brazil, between 2012 and 2014.
Methods
This was a descriptive study comparing data from PMAQ-AB cycle I (2012) and cycle II (2013/2014) in Goiás, a state in the Midwest region of Brazil. Goiás covers an area of 340,111.376km2 and in 2017 had an estimated population of 6,779,000 inhabitants, distributed over 246 municipalities and estimated population density of 19.9 inhab./km2. Also in 2017, 39.0% of the population of Goiás was 40 years old or more, whereas in 2000 this proportion was 25.3%. In order to organize the health system in accordance with the principal of Health regionalization within the state, Goiás is divided into 18 Health Regions, has 1409 Family Health teams and 65.3% of its population is covered by PHC.12
PMAQ-AB external evaluation uses standardized instruments built with the purpose of covering all dimensions of PHC. This study analyzed data from Module II of the PMAQ-AB data collection instrument. This data was gathered by means of interviews given by university-qualified Family Health professionals about the team work process. In order to enable comparison between the two moments, we only selected Family Health teams that took part in both PMAQ-AB cycles. The database is available on the Ministry of Health Primary Health Care Secretariat website (https://aps.saude.gov.br/ape/esus).
We selected variables related to addressing chronic diseases and health promotion. In order to enable comparison between the two cycles, only variables used in both cycles were included. They were divided into three dimensions: health promotion; care management; and activities at schools. Figure 1 shows the dimensions defined for this study, their variables and the contents of each of them.
Figure 1 Variables selected from National Program for Improving Primary Care Access and Quality instruments related to addressing chronic noncommunicable diseases, Goiás, 2012 and 2014
| Dimension | Variable | Content of the variable |
|---|---|---|
| Care management | Attending to spontaneous demand | Proportion of teams attending to spontaneous demand. |
| Assessment of risk and vulnerability at initial care | Proportion of teams carrying out assessment of risk and vulnerability at initial care for service users. | |
| Training for assessment and classification of risk and vulnerability | Proportion of teams carrying patient embracement and trained to assess and classify their risk and vulnerability. | |
| Repeat prescription without having to have an appointment | Proportion of teams issuing repeat prescriptions for patients under continuous care/programs such as hypertension and diabetes, without having to have an appointment. | |
| Time slots allotted for receiving and showing test results | Proportion of teams that allot time slots in the appointment book or at a convenient time for health professionals so that patients can receive and be shown their test results. | |
| Time slots allotted for post-consultation queries | Proportion of teams that allot time slots in the appointment book or at a convenient time for health professionals so that patients can make post-consultation queries or show how their situation has progressed. | |
| All care management actions | Proportion of teams carrying out all care management actions. | |
| Health promotion | Support with self-care of chronic diseases | Proportion of teams carrying out health education and health promotion actions in group activities with the aim of supporting self-care of chronic diseases. |
| Actions aimed at women | Proportion of teams carrying out health education and health promotion actions aimed at women (cervical and breast cancer). | |
| Actions aimed at men | Proportion of teams carrying out health education and health promotion actions aimed at men. | |
| Actions aimed at the elderly | Proportion of teams carrying out health education and health promotion actions aimed at the elderly. | |
| Actions aimed at healthy eating | Proportion of teams carrying out health education and health promotion actions aimed at healthy eating. | |
| Encouragement of bodily practices and physical activity | Proportion of teams that encourage and arrange bodily practices or physical activity at the primary health care center and/or in its catchment area. | |
| All health promotion actions | Proportion of teams carrying out all health promotion actions. | |
| Activity at schools | Carries out activity at schools | Proportion of teams carrying out activities at schools. |
| Early detection of arterial hypertension | Proportion of teams carrying out early detection of arterial hypertension. | |
| Nutritional assessment | Proportion of teams carrying out nutritional assessment. | |
| Food security and healthy eating promotion actions | Proportion of teams carrying out food security and healthy eating promotion actions. | |
| Promotion of bodily practices and physical activity at schools | Proportion of teams promoting bodily practices and physical activity at schools. | |
| All activity actions at schools | Proportion of teams carrying out all activity actions at schools. |
Bodily practice and physical activity actions were treated separately on the collection instrument but were assessed together in this study and defined as ‘bodily practices and/or physical activity’.
In addition to the variables selected from data instrument questions, three further variables were created estimating the proportion of the teams that carried out all the actions provided for each dimension: all care management actions; all health promotion actions; and all activity actions at schools.
For the purpose of data analysis, the proportions of each variable of each cycle were estimated. McNemar’s test for paired samples was used when comparing proportions between the PMAQ-AB cycles. Critical values were considered to be those with a p-value less than 0.05 (5% significant level). The IBM SPSS Statistics computer program, version 22.0, was used to tabulate the data and to perform statistical analysis.
The PMAQ-AB study project was analyzed and approved by the Federal University of Goiás Research Ethics Committee, as per Protocol No. 487.055/2013, issued on December 2nd 2013, in accordance with National Health Council Resolution No. 466, dated October 12th 2012.
Results
A total of 677 teams answered the PMAQ-AB cycle I questionnaire, 29 of which did not take part in cycle II. In cycle II, a total of 1180 teams answered the Module II questionnaire, 532 of which had not taken part in cycle I. As such, we compared the questionnaires answered by 648 teams in both cycles (Figure 2).
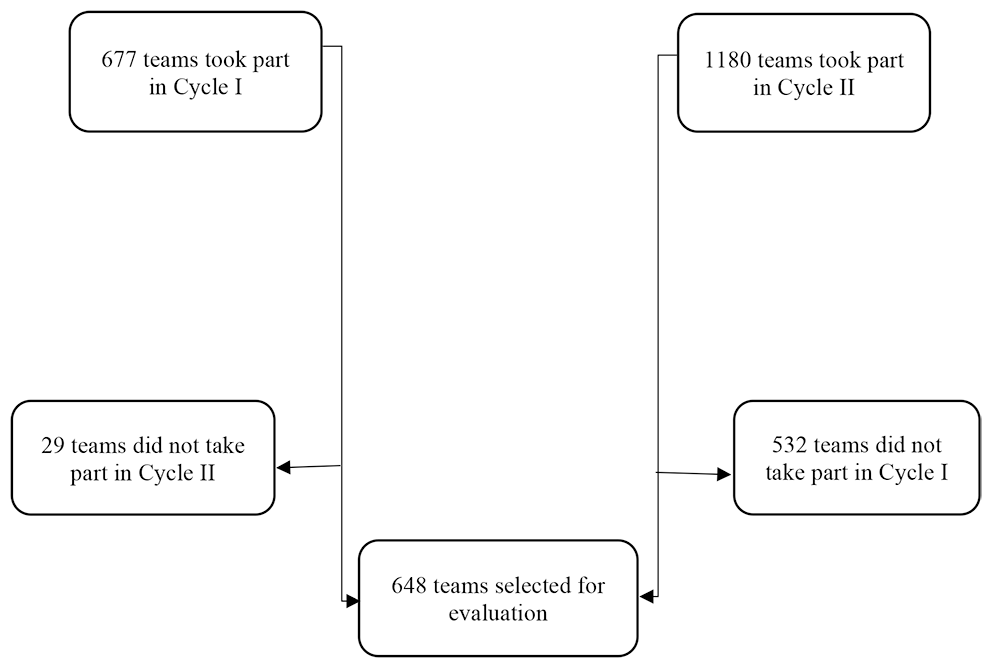
Figure 2 Selection of Family Health teams that took part in cycles I and II of the National Program for Improving Primary Care Access and Quality, Goiás, 2012 and 2014
All six actions relating to the care management dimension increased significantly in the state of Goiás (Table 1). Standing out in particular were the ‘attending to spontaneous demand’ and ‘assessment of risk and vulnerability at initial care’ variables, with an increase above 30 per cent between cycle I and cycle II.
Table 1 Proportion of Family Health teams carrying out care management actions, Goiás, 2012 and 2014
| Care management: Actions | n=648% (95%CIa) | ||
|---|---|---|---|
| Cycle | p-valorb | ||
| I | II | ||
| Attending to spontaneous demand | 65,6 (61,9;69,1) | 96,9 (95,3;98,0) | <0,001 |
| Assessment of risk and vulnerability at initial care | 55,7 (51,9;59,5) | 90,4 (87,9;92,5) | <0,001 |
| Training for assessment and classification of risk and vulnerability | 33,0 (29,5;36,7) | 62,2 (58,4;65,8) | <0,001 |
| Repeat prescription without having to have an appointment | 73,1 (69,6;76,4) | 84,9 (81,9;87,4) | <0,001 |
| Reserving time slots to receive and show test results | 50,3 (46,5;54,2) | 66,8 (63,1;70,3) | <0,001 |
| Reserving time slots for post-consultation queries | 47,8 (44,0;51,7) | 60,8 (57,0;64,5) | <0,001 |
| All care management actions | 16,0 (13,4;19,1) | 32,1 (28,6;35,8) | <0,001 |
a) 95%CI: 95% confidence interval.
b) McNemar’s test.
With regard to the health promotion dimension (Table 2), there was a significant increase in the following variables: ‘support with self-care of chronic diseases’ (from 55.1 to 68.5%), ‘actions aimed at men’ (from 36.7 to 61.7%), ‘bodily practices and/or physical activity’ (from 67.6 to 78.4%) and ‘all health promotion actions’ (from 21.5 to 35.2%) (Table 2).
Table 2 Proportion of Family Health teams carrying out health promotion actions, Goiás, 2012 and 2014
| Health promotion: Actions | n=648% (95%CIa) | ||
|---|---|---|---|
| Cycle | p-valorb | ||
| I | II | ||
| Support with self-care of chronic diseases | 55,1 (51,2;58,9) | 68,5 (64,9;72,0) | <0,001 |
| Actions aimed at women | 78,7(75,4;83,7) | 80,9 (77,7;83,7) | 0,35 |
| Actions aimed at men | 36,7 (33,1;40,5) | 61,7 (57,9;65,4) | <0,001 |
| Actions aimed at the elderly | 77,9 (75,6;80,1) | 81,2 (78,0;84,0) | 0,17 |
| Actions aimed at healthy eating | 73,9 (70,4;77,2) | 77,6 (74,3;80,7) | 0,12 |
| Bodily practices and/or physical activity | 67,6 (63,9;71,1) | 78,4 (75,1;81,4) | <0,001 |
| All health promotion actions | 21,5 (18,5;24,8) | 35,2 (31,6;38,9) | <0,001 |
a) 95%CI: 95% confidence interval.
b) McNemar’s test.
The actions relating to the activities at school dimension had a significant increase for all the variables analyzed (Table 3). In particular, the ‘early detection of arterial hypertension’, ‘nutritional assessment’ and ‘food security and healthy eating promotion actions’ variables had increases greater than 20 per cent.
Table 3 Proportion of Family Health teams carrying out all actions of the activity at schools, Goiás, 2012 and 2014
| Activity at schools: Actions | n=648 % (95%CIa) | ||
|---|---|---|---|
| Cycle | p-valorb | ||
| I | II | ||
| Carries out activity at schools | 77,2 (73,8;80,2) | 88,9 (86,2;91,1) | <0,001 |
| Early detection of arterial hypertension | 37,7 (34,0;41,5) | 59,6 (55,7;63,3) | <0,001 |
| Nutritional assessment | 47,5 (43,7;51,4) | 74,7 (71,2;77,9) | <0,001 |
| Food security and healthy eating promotion actions | 55,1 (51,2;58,9) | 75,8 (72,3;78,9) | <0,001 |
| Promotion of bodily practices and physical activity at schools | 35,3 (31,8;39,1) | 54,0 (50,2;57,8) | <0,001 |
| All activity actions at schools | 22,2 (19,2;25,6) | 39,8 (36,1;43,6) | <0,001 |
| Todas as ações de promoção da saúde | 21,5 (18,5;24,8) | 35,2 (31,6;38,9) | <0,001 |
a) 95%CI: 95% confidence interval.
b) McNemar’s test.
No variable/action had a statistically significant reduction in the period that elapsed between PMAQ-AB cycle I and cycle II (Tables 1, 2 and 3).
Discussion
The results of the study demonstrate that PHC actions addressing NCDs in Goiás were strengthened in the period of time that elapsed between the two moments of the study. There was an increase in practicing 17 of the 20 actions studied and there was no decrease in any of them. All the actions of the ‘activities at school’ and ‘care management’ dimensions increased in the period studied. There was also an increase in promoting chronic disease self-care, actions aimed at men and promotion of bodily practices and/or physical activity among health service users.
The increase in the practicing of patient embracement and assessment of risk and vulnerability actions is compatible with that found for the Northern region of Brazil.9 Patient embracement should be carried out by a multi-professional team, with the purpose of listening to the service user and identifying their needs so that care is as individualized as possible.13-14 Based on adequate health professional training, patient embracement with risk classification can be carried out in parallel to programmed actions, increasing linkage and improving access to services.9, 14
The prevalence rates of actions aimed at women and at promoting healthy eating found by this study are compatible with those identified for the Midwest region. The divergences found for the other promotion actions may be related to differences between the states the comprise the region, as well as to the methodology used to select the teams assessed.1 Values lower than those found for Goiás in relation to healthy eating, physical activity and actions aimed at women were found by a primary health care study in Spain.15 However, the authors of the Spanish study only assessed community activities, whereas PMAQ-AB does not specify whether the actions assessed are community or individual.
Most of the prevention and health promotion interventions aimed at addressing NCDs seek to promote the reduction of risk factors.16 Studies reveal the existence of diverse obstacles to PHC health promotion actions, such as low health professional qualification and low service user adherence.17-18 Generally speaking, actions relating to NCDs continue to be centered on the biomedical model characterized by a medical consultation culminating in a prescription.16 Specific group activities for NCDs are rare and, when they do exist, they are generally based on the transmission of knowledge of traditional methods without follow-up centered on the service user.18
The prevalence of self-care promotion we found is compatible with that found for the Midwest region10 and for the state of Amazonas.11 Supported self-care is one of the main elements of models aimed at NCDs care.19 Health services should investigate as much as possible the specific needs of each individual, encouraging and empowering them for self-care and promoting their own health.20-21 One way to facilitate this form of care is by using social media. The growing popular use of online tools to seek information means that social media are an excellent means of communication between patients and Health professionals.21
The increase in actions aimed at men revealed by the study is similar to results found in the literature10, 22 and may be related to the National Policy on Men’s Comprehensive Health Care. The objective of this policy, which came into force in 2009, is to address risk factors and improve access to men’s health services23 and as such there is a need to invest in health professional training and to provide actions that respect male biological and cultural particularities. Specific strategies, such as household visits at alternative times of the day and extended health center opening hours, can contribute to closer male linkage with PHC.22-23
The promotion of bodily practices and physical activity found in Goiás was greater than that found for Brazil as a whole and for the country’s Midwest region.10, 24 This difference may be related to the fact of this study having grouped together the data on bodily practices and physical activity, whereas other studies have presented these data separately. The increase in promotion of physical activity between the two PMAQ-AB cycles may be a reflection of the strategic action plan to address NCDs, in particular its encouragement of facilities providing sports activities supervised by professionals qualified by the Health Fitness Center Program.25
The increase in Family Health teams in Goiás that carry out activities at schools is similar to that found for the Midwest region as a whole,26 and is probably associated with the implementation of the Health At School Program. This program was created in 2007 and implemented health assessment and promotion actions in schools in accordance with its main strategy of ensuring articulation between each school and each Family Health team in the same catchment area.26 Articulation between schools and Family Health teams can be confirmed by the results of the National School Student Survey,27 and which were corroborated by this study which found that the majority of students attend schools that carry out actions jointly with Family Health teams. The National School Student Survey showed that students have inadequate diets and practice insufficient physical activity,27 highlighting the need to prioritize actions to promote healthy eating and bodily practices at schools as one of the responsibilities of PHC. Implementation of this type of action needs to be articulated between Health services and Education services, which is not always easy or straightforward. Lack of planning between the services responsible leads to health care concentrated on acute conditions.28
Using the PMAQ-AB database as a study source has limitations. The questions related to health promotion did not specify what ‘promotion’ is considered to be and, in addition, it was not possible to confirm that all the actions assessed had in fact been carried out.
The criteria for selecting the teams also results in limitations for generalization of the results. The teams assessed were not selected using probabilistic sampling, thus hindering extrapolation of the results and comparison with other studies. As the main objective of the study was to assess improvement in provision of actions between the two cycles, we only selected teams that took part in both cycles and this reduced the number of teams assessed to just over 50% of the state’s Family Health teams.
Another limitation with regard to being able to perform an adequate temporal comparison was the difference between the evaluation instruments used in cycle I and cycle II. Several questions were modified between cycle I and cycle II so that their sense became altered; other questions used in cycle I were excluded from cycle II, such as the specific questions about care for people with systemic arterial hypertension and diabetes, so that these questions were not selected for assessment. To the extent that the number of comparable variables was reduced, our assessment became less comprehensive.
The results of this study provide evidence of important progress in PHC addressing NCDs in Goiás between the two PMAQ-AB cycles. Notwithstanding, efforts are required in order for all activities relating to NCDs are carried out by all multi-professional teams, both in the Family Health Strategy and in primary health care in general.
We recommend that the data collection instrument be adapted for future PMAQ-AB evaluations, with the aim of including variables capable of characterizing more completely the essential elements of a care model for chronic noncommunicable diseases that is coherent with the national and international literature.
REFERENCES
1. Medina MG, Aquino R, Vilasbôas ALQ, Mota E, Júnior EPP, Luz LA, et al. Promoção da saúde e prevenção de doenças crônicas: o que fazem as equipes de Saúde da Família? Saúde Debate [Internet]. 2014 out [citado 2019 mar 07];38(n spe):69-82. Disponível em: https://doi.org/10.5935/0103-1104.2014S006 [ Links ]
2. Martinez R, Loyd-Sherlock P, Soliz P, Ebrahim S, Vega E, Ordunez P. Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990-2017: a population-based study. Lancet Global Health [Internet]. 2020 Apr [cited 2020 May 18];8(4):E511-23. Available from: https://doi.org/10.1016/S2214-109X(20)30035-8 [ Links ]
3. GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex-specific mortality for 282 causes of death in 195 countries and territories, 1980-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet [Internet]. 2018 Nov [cited 2019 Feb 5];392(10159):1736-88. Available from: https://doi.org/10.1016/S0140-6736(18)32203-7 [ Links ]
4. Malta DC, Moura L, Prado RR, Escalante JC, Schmidt MI, Duncan BB. Mortalidade por doenças crônicas não transmissíveis no Brasil e suas regiões, 2000 a 2011. Epidemiol Serv Saúde [Internet]. 2014 out-dez [citado 2019 mar 31];23(4):599-608. Disponível em: https://doi.org/10.5123/S1679-49742014000400002 [ Links ]
5. Malta DC, Felisbino-Mendes MS, Machado IE, Passos VMA, Abreu DMX, Ishitani LH, et al. Fatores de risco relacionados à carga global de doença do Brasil e Unidades Federadas, 2015. Rev Bras Epidemiol [Internet]. 2017 dez [citado 2019 mar 20];20(Suppl 1):217-32. Disponível em: https://doi.org/10.1590/1980-5497201700050018 [ Links ]
6. Borges GM, Campos MB, Castro Silva LG. Transição da estrutura etária no Brasil: oportunidades e desafios para a sociedade nas próximas décadas. In: Ervatti LR, Borges GM, Jardim AP, organizadores. Mudança demográfica no Brasil no início do século XXI: subsídios para projeções da população [Internet]. Rio de Janeiro: IBGE; 2015 [citado 2020 set 16]. p. 138-151. Disponível em: https://biblioteca.ibge.gov.br/visualizacao/livros/liv93322.pdf [ Links ]
7. Malta DC, Morais Neto OL, Silva Junior, JB. Apresentação do plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis no Brasil, 2011 a 2022. Epidemiol Serv Saúde [Internet]. 2011 out-dez [citado 2019 fev 28];20(4):425-38. Disponível em: http://dx.doi.org/10.5123/S1679-49742011000400002 [ Links ]
8. Pinto HA, Sousa ANA, Ferla AA. O Programa Nacional de Melhoria do Acesso e da Qualidade da Atenção Básica: várias faces de uma política inovadora. Saúde Debate [Internet]. 2014 out [citado 2019 mar 7];38(n esp):358-72. Disponível em: http://dx.doi.org/10.5935/0103-1104.2014S027 [ Links ]
9. Garnelo L, Lima JG, Rocha ESC, Herkrath FJ. Acesso e cobertura da Atenção Primária à Saúde para populações rurais e urbanas na região norte do Brasil. Saúde Debate [Internet]. 2018 set [citado 2020 mar 1];42(n esp1):81-99. Disponível em: http://dx.doi.org/10.1590/0103-11042018s106 [ Links ]
10. Teixeira MB, Casanova A, Oliveira CCM, Ensgtrom EM, Bodstein RCA. Avaliação das práticas de promoção da saúde: um olhar das equipes participantes do Programa Nacional de Melhoria do Acesso e da Qualidade da Atenção Básica. Saúde Debate [Internet]. 2014 out [citado 2019 abr 01];38(n esp):52-68. Disponível em: https://doi.org/10.5935/0103-1104.2014S005 [ Links ]
11. Garnelo L, Cristina R, Parente P, Soares E, Rocha C. Organização do cuidado às condições crônicas por equipes de Saúde da Família na Amazônia. Saúde Debate [Internet]. 2014 out [citado 2019 mar 21];38(n esp):158-72. Disponível em: https://doi.org/10.5935/0103-1104.2014S012 [ Links ]
12. Governo do Estado de Goiás. Secretaria de Estado de Gestão e Planejamento. Instituto Mauro Borges de Estatísticas e Estudos Socioeconômicos - IMB. Goiás em dados: 2017 [Internet]. Goiânia: IMB; 2018 [citado 2020 set 26]. 113 p. Disponível em: http://www.imb.go.gov.br/index.php?option=com_content&view=article&id=85:goi%C3%A1s-em-dados-2017&catid=19&Itemid=151 [ Links ]
13. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Política Nacional de Humanização. HumanizaSUS: documento-base para gestores e trabalhadores do SUS [Internet]. 4. ed. Brasília: Ministério da Saúde; 2010 [citado 2020 set 16]. 72 p. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/humanizasus_documento_gestores_trabalhadores_sus.pdf [ Links ]
14. Camelo MS, Lima LR, Volpe CRG, Santos WS, Rehem TCMSB. Acolhimento na atenção primária à saúde na ótica de enfermeiros. Acta Paul Enferm [Internet]. 2016 ago [citado 2019 mar 2];29(4):463-8. Disponível em: https://doi.org/10.1590/1982-0194201600063 [ Links ]
15. March S, Jordán M, Matilde MG, Isabel BA, Carmen B, Elizalde Soto L, et al. ¿Qué hacemos en el barrio? Descripción de las actividades comunitarias de promoción de la salud en atención primaria: proyecto frAC. Gac Sanit [Internet]. 2014 jul-ago [citado 2020 mar 4];28(4):267-73. Disponible en: http://dx.doi.org/10.1016/j.gaceta.2014.01.009 [ Links ]
16. Silva LS, Cotta RMM, Rosa COB. Estratégias de promoção da saúde e prevenção primária para enfrentamento das doenças crônicas: revisão sistemática. Rev Panam Salud Publica [Internet]. 2013 [citado 2020 set 10];34(5):343-50. Disponível em: https://scielosp.org/article/rpsp/2013.v34n5/343-350/pt/ [ Links ]
17. Salci MA, Meirelles BHS, Silva DMGV. Atenção primária às pessoas com diabetes mellitus na perspectiva do modelo de atenção às condições crônicas. Rev Latino-Am Enfermagem [Internet]. 2017 mar [citado 2019 abr 7];25:e2882. Disponível em: https://doi.org/10.1590/1518-8345.1474.2882 [ Links ]
18. Silocchi C, Junges JR. Equipes de atenção primária: dificuldades no cuidado de pessoas com doenças crônicas não transmissíveis. Trab Educ Saúde [Internet]. 2017 mar [citado 2019 mar 15];15(2);599-615. Disponível em: https://doi.org/10.1590/1981-7746-sol00056 [ Links ]
19. Mendes EV. O cuidado das condições crônicas na atenção primária à saúde: o imperativo da consolidação da estratégia da Saúde da Família [Internet]. Brasília: Organização Pan-Americana da Saúde; 2012 [citado 2020 set 16]. 512 p. Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/cuidado_condicoes_atencao_primaria_saude.pdf [ Links ]
20. Conceição AP, Santos MA, Santos B, Cruz DALM. Autocuidado de pacientes com insuficiência cardíaca. Rev Latino-Am Enfermagem [Internet]. 2015 jul-ago [citado 2019 jan 31];23(4):578-86. Disponível em: https://doi.org/10.1590/0104-1169.0288.2591 [ Links ]
21. De Angelis G, Wells GA, Davies B, King J, Shallwani SM, McEwan J, et al. The use of social media among health professionals to facilitate chronic disease self-management with their patients: a systematic review. Digital Health [Internet]. 2018 May [cited 2019 Feb 12];4. Available from: https://doi.org/10.1177/2055207618771416 [ Links ]
22. Moura EC, Santos W, Neves ACM, Gomes R, Schwarz E. Atenção à saúde dos homens no âmbito da Estratégia Saúde da Família. Ciênc Saúde Coletiva [Internet]. 2014 fev [citado 2019 mar 07];19(2):429-38. Disponível em: https://doi.org/10.1590/1413-81232014192.05802013 [ Links ]
23. Brasil. Ministério da Saúde. Portaria GM/MS nº 1.944, de 27 de agosto de 2009. Institui no âmbito do Sistema Único de Saúde (SUS) a Política Nacional de Atenção Integral à Saúde do Homem [Internet]. Diário Oficial da União, Brasília (DF), 2009 ago 28 [citado 2019 fev 27];Seção I:61. Disponível em: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2009/prt1944_27_08_2009.html [ Links ]
24. Ramos LR, Malta DC, Gomes GAO, Bracco MM, Florindo AA, Mielke GI, et al. Prevalence of health promotion programs in primary health care units in Brazil. Rev Saúde Pública [Internet]. 2014 Oct [cited 2019 Feb 19];48(5):837-44. Available from: https://doi.org/10.1590/S0034-8910.2014048005249 [ Links ]
25. Machado MFAS, Gubert FA, Meyer APGFV, Sampaio YPCC, Dias MSA, Almeida AMB, et al. Programa saúde na escola: estratégia promotora de saúde na atenção básica no Brasil. J Hum Growth Dev [Internet]. 2015 [citado 2019 mar 1];25(3);307-12. Disponível em: http://dx.doi.org/10.7322/jhgd.96709 [ Links ]
26. Brasil. Presidência da República. Decreto nº 6.286, de 5 de dezembro de 2007. Institui o Programa Saúde na Escola - PSE, e dá outras providências [Internet]. Diário Oficial da União, Brasília (DF), 2007 dez 06 [citado 2019 fev 25]. Disponível em: http://www.planalto.gov.br/ccivil_03/_ato2007-2010/2007/decreto/d6286.htm [ Links ]
27. Instituto Brasileiro de Geografia e Estatística - IBGE. Pesquisa nacional de saúde do escolar 2015 [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2016 [citado 2020 set 16]. Disponível em: https://biblioteca.ibge.gov.br/visualizacao/livros/liv97870.pdf [ Links ]
28. Brasil EGM, Silva RM, Silva MRF, Rodrigues DP, Queiroz MVO. Promoção da saúde de adolescentes e Programa Saúde na Escola: complexidade na articulação saúde e educação. Rev Esc Enferm USP [Internet]. 2017 dez [citado 2019 fev 07];51:e03276. Disponível em: https://doi.org/10.1590/s1980-220x2016039303276 [ Links ]
Received: April 13, 2020; Accepted: August 17, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
