










Services on Demand
Journal

Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Curriculum ScienTI
Curriculum ScienTI Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO
Related links
-
 Similars in
SciELO
Similars in
SciELO
Share

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
Print version ISSN 1679-4974On-line version ISSN 2237-9622
Epidemiol. Serv. Saúde vol.29 no.5 Brasília 2020 Epub Sep 28, 2020
http://dx.doi.org/10.1590/s1679-49742020000500004
Profile of National Health Databases
National Health Survey 2019: history, methods and perspectives
1Ministério da Saúde, Departamento de Análise em Saúde e Vigilância de Doenças não Transmissíveis, Brasília, DF, Brazil
2Fundação Instituto Oswaldo Cruz, Instituto de Comunicação e Informação Científica e Tecnológica em Saúde, Rio de Janeiro, RJ, Brazil
3Instituto Brasileiro de Geografia e Estatística, Diretoria de Pesquisas, Rio de Janeiro, RJ, Brazil
This article presents the history and construction of the National Health Survey (PNS) 2019, a household survey conducted in partnership with the Brazilian Institute of Geography and Statistics. The objective of PNS 2019 was to provide the country with information on the health determinants, conditionants and needs of the Brazilian population. The expected sample was 108,525 households, considering a 20% non-response rate. The questionnaire had three parts, covering: (i) the household; (ii) all residents of the household, focusing on collection of socioeconomic and health information; and (iii) the selected resident (15 years old or more) for whom lifestyles, chronic diseases, violence, among other topics were investigated, as well as their anthropometric measurements (subsample). The information provided by PNS 2019 will serve as a basis for the (re)formulation of health policies, as well as support for existing actions and programs of the Brazilian National Health System.
Keywords: Health Surveys; Cross-Sectional Studies; Methodology; Sample Size; Population Characteristics; Brazil
Introduction
Health surveys are essential for evaluating health systems from the perspective of service users. They are important tools for understanding the real needs of the population – living and health conditions –, indispensable for planning, creating and/or enhancing health programs and policies.1,2
One of the main objectives of health surveys is to provide health information which, for the most part, is not recorded on health information systems. The insufficiency of these systems in terms of meeting the needs of public health service management emphasizes the importance of collecting primary data by means of population-based health surveys.1,3
Preferably conducted with constant periodicity, surveys enable information to be consolidated as a population reference base when defining surveillance and monitoring of morbidities and their risk and protective factors. Another characteristic of these surveys is the possibility of analyzing the information collected from the viewpoint of health inequalities, thus guiding policies with the aim of achieving greater equity in access to health.4,5
In high-income countries health surveys have been conducted since the 1960s, whereas in middle and low-income countries this practice is more recent. In Brazil, the first health survey was conducted in 1974, in the city of Ribeirão Preto, SP, and was about reported mortality and use of health services.6 That first initiative gave rise to diverse discussions about methodology and encouraged subsequent projects, such as the National Survey of Family Expenses conducted in 1974 and 1975.7,8 Subsequently, other surveys were conducted, such as the Family Budget Surveys, surveys in the area of diet and reproductive health, such as the National Health and Nutrition Survey in 1989, and the National Demography and Health Survey which began in 1986 and was conducted again in 1996 and 2006 (Figure 1).7,8
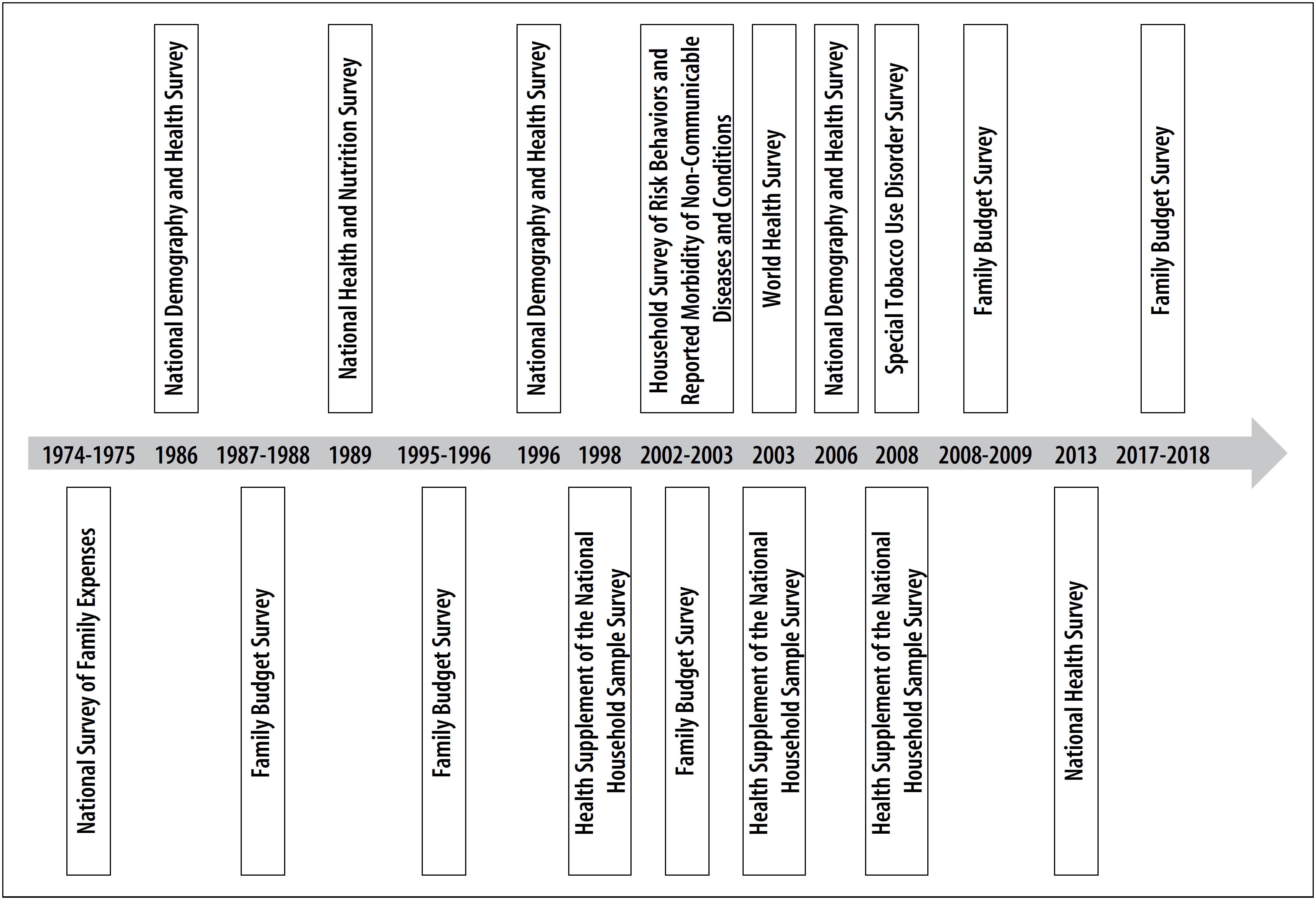
With regard to Health itself, it is fitting to mention Ministry of Health support in funding the Health Supplements of the National Household Sample Survey (PNAD), in 1998, 2003 and 2008.7,8 The Supplements enabled comparisons over time, as well as monitoring of indicators of health service access and use, health expenditure and morbidities;9 other themes were incorporated each time the supplements were conducted, such as chronic noncommunicable disease risk and protective factors, traffic accidents and violence, use of medication and Family Health Strategy coverage.9
Despite the initiatives mentioned above having contributed considerably to increased understanding and monitoring of health indicators, and given the growing use of survey methodology by the Brazilian scientific community, the need exists to expand the capacity to gather information and analyze results. In view of this, consideration was given to the opportuneness of developing a nationwide health survey so as to meet Ministry of Health demands and priorities.
National Health Survey
In 2003, the Thematic Committee on Population-Based Information recommended that a population-based national health survey should be conducted to evaluate health conditions, health service access and use and health expenditure, surveillance of noncommunicable diseases and conditions and their determinants, as well as issues relating to social inequalities with regard to health. On that occasion, the Thematic Committee highlighted the importance of budgeting resources on a regular basis to ensure the sustainability of such a comprehensive and relevant survey.10
Later, in 2007, at a seminar held by the Brazilian Collective Health Association (Associação Brasileira de Saúde Coletiva - ABRASCO) about health surveys, a national survey process became a key issue once more and it was recommended that a working group be set up to plan and carry it out. In 2009, the Ministry of Health issued an ordinance which created a Steering Committee to prepare guidelines for managing the National Health Survey (PNS).11 In 2011 the Ministry updated the ordinance and included the following of its Secretariats in the organization of the survey: Health Surveillance, Executive, Health Care; Strategic and Participative Management, Science, Technology and Strategic Supplies; along with the Oswaldo Cruz Institute Foundation (Fiocruz).12
The first edition of the PNS began in the field in 2013, with the purpose of expanding the thematic investigation of the PNAD Health Supplements. The PNS questionnaire included, comprehensively, modules on health service access and use and health insurance coverage, these being the main themes investigated by the PNAD, and enabled the accompaniment of the five-year series of their indicators over the period 1998-2013. Moreover, differently to the Health Supplements, the PNS was included in the Integrated Household Survey System of the Brazilian Institute of Geography and Statistics (IBGE), independently from the PNAD Contínua survey, having its own design and having been prepared especially to collect health data. It was defined that the PNS would be conducted every five years.
Data collection by means of interviews took place between August 2013 and February 2014. Conducted by IBGE, it involved more than 1,000 of that institution's technical staff who collected data in 1,600 Brazilian municipalities. In all, four reports were released and, together with the databases, they were made available on the IBGE website and have been used in diverse technical and scientific publications.13–16
When the PNS reports were released in 2014 and 2015, the Ministry of Health soon expressed interest in conducting a second edition, so as to enable monitoring of the evolution of the PNS health indicators regarding the situation investigated previously, as well as the subsequent response of the Brazilian National Health System (SUS) towards meeting the population's needs.
In April 2017, the Ministry published the ordinance that created the Steering Committee of the second edition of the PNS, with the participation of the following Secretariats: Health Surveillance, whereby its Department of Noncommunicable Disease Health and Surveillance Analysis was responsible for coordinating the survey; Science, Technology and Strategic Supplies; Executive; Health Care; Strategic and Participative Management; Health Work and Education Management; Special Indigenous Health; and Fiocruz.17
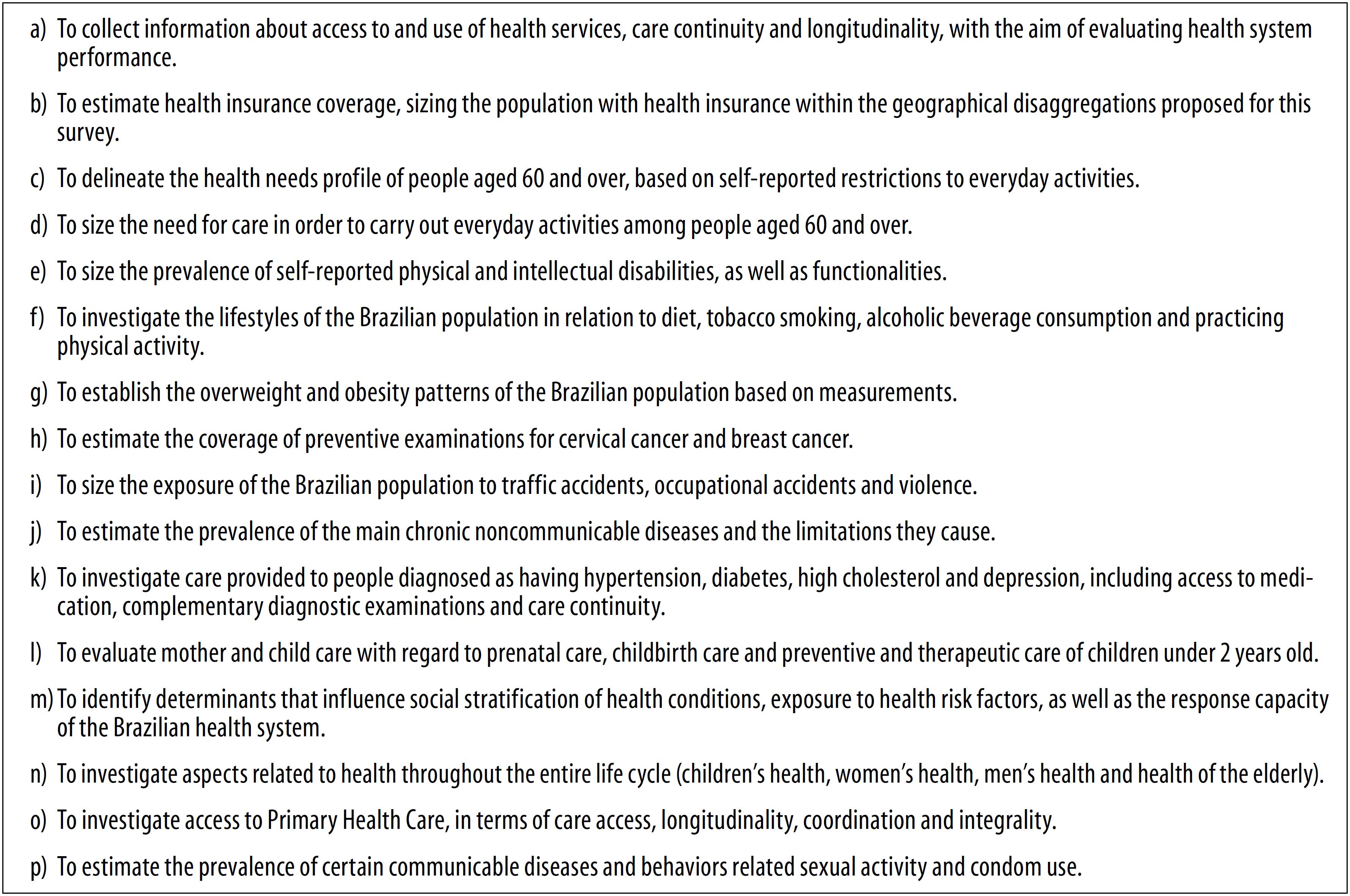
The main objective of PNS 2019 was to provide the country with information on the health determinants, conditionants and needs of the Brazilian population, enabling consistent measures to be established, capable of assisting the formulation of public policies and achieving greater health intervention effectiveness. The specific objectives of PNS 2019 are described in Figure 2.
Methods
The PNS 2019 is a population-based survey that is representative of Brazil and of the population resident in private households on Brazilian territory. Through the survey it was possible to estimate data for urban and rural areas, by the country's five macro-regions, its Federative Units, state capitals and metropolitan regions. The PNS was planned to be conducted every five years. Due to issues related to its design and execution, its second edition, initially planned for 2018, was conducted in 2019.
Participants
The target population of the PNS is comprised of individuals aged 15 years old or over, resident in permanent private dwellings, i.e. built for the exclusive purpose of habitation. The survey sample excluded households located in special census tracts or those scarcely populated, such as indigenous clusters, barracks, military bases, lodgings, campsites, waterborne vessels, penitentiaries, penal colonies, prisons, jails, long-stay institutions for the elderly, comprehensive care facilities for children and adolescents, convents, hospitals, settlement project farming communities and quilombola clusters.
Sampling plan and data analysis
The PNS sample originated from a main sample, comprised of a set of units of areas selected in a register, so as to be able to form subsample selections for diverse different surveys planned for the Integrated Household Survey System of the Brazilian Institute of Geography and Statistics (SIPD/IBGE), such as the National Household Sample Survey (PNAD) and the Family Budget Survey (POF). These units are conceived of as primary sampling units (PSU), within the sample planning of surveys that use the main sample, which is the case of the PNS.
The sampling strategy consisted of (i) a three-stage conglomerate plan, with PSU stratification (in this case, census tracts or sets of tracts) and selection of PSUs for the main sample, with probability proportional to size, defined by the number of permanent private dwellings, and (ii) selection for the PNS sample, also with proportional probability.
The second stage consisted of selecting households from the National Register of Addresses for Statistical Purposes, taking the most recent version of the Register (updated in order to conduct the PNAD Contínua 2019 survey) prior to the conclusion of this stage of the sampling plan, by means of simple random sampling. Following this, one resident aged 15 years old or over from each household was randomly selected, based on the list of household residents obtained at the time of the household interview. In order to set the sample size with the level of accuracy desired for the estimates, some of the PNS 2013 indicators were taken into consideration, such as chronic noncommunicable disease data (diabetes, hypertension, depression), violence, use of health services, having health insurance, tobacco use disorder, practice of physical activities and alcohol consumption, among other indicators. The final sample size is shown in Table 1.
Table 1 Planned sample size of the National Health Survey (PNS), by domains of interest, Brazil, macro-regions and Federative Units, 2019
| Macro-regions and Federative Units | PSUsa in the main sample | PNS sample size | |||||
|---|---|---|---|---|---|---|---|
| Planned number of PSUsa | Number of PSUsa following allocation | Number of planned households selected | Number of households selected following allocation | Expected number of households with interviews conducted (20% non-response) | |||
| Brazil | 15,096 | 7,968 | 8,036 | 107,628 | 108,525 | 86,820 | |
| North | 1,896 | 1,362 | 1,370 | 21,636 | 21,762 | 17,410 | |
| Rondônia | 264 | 174 | 177 | 2,610 | 2,655 | 2,124 | |
| Acre | 276 | 193 | 193 | 2,895 | 2,895 | 2,316 | |
| Amazonas | 360 | 263 | 263 | 3,945 | 3,945 | 3,156 | |
| Roraima | 156 | 156 | 156 | 2,808 | 2,808 | 2,246 | |
| Pará | 504 | 330 | 333 | 4,950 | 4,995 | 3,996 | |
| Amapá | 108 | 108 | 108 | 1,944 | 1,944 | 1,555 | |
| Tocantins | 228 | 138 | 140 | 2,484 | 2,520 | 2,016 | |
| Northeast | 4,908 | 2,810 | 2,840 | 37,104 | 37,503 | 30,002 | |
| Maranhão | 900 | 476 | 482 | 5,712 | 5,784 | 4,627 | |
| Piauí | 324 | 204 | 207 | 3,060 | 3,105 | 2,484 | |
| Ceará | 780 | 476 | 482 | 5,712 | 5,784 | 4,627 | |
| Rio Grande do Norte | 300 | 235 | 237 | 3,525 | 3,555 | 2,844 | |
| Paraíba | 384 | 240 | 245 | 3,600 | 3,675 | 2,940 | |
| Pernambuco | 600 | 374 | 380 | 4,488 | 4,560 | 3,648 | |
| Alagoas | 564 | 251 | 251 | 3,765 | 3,765 | 3,012 | |
| Sergipe | 288 | 198 | 201 | 2,970 | 3,015 | 2,412 | |
| Bahia | 768 | 356 | 355 | 4,272 | 4,260 | 3,408 | |
| Southeast | 4,092 | 1,874 | 1,901 | 23,328 | 23,655 | 18,924 | |
| Minas Gerais | 1,104 | 488 | 495 | 5,856 | 5,940 | 4,752 | |
| Espírito Santo | 600 | 280 | 281 | 4,200 | 4,215 | 3,372 | |
| Rio de Janeiro | 1,164 | 508 | 512 | 6,096 | 6,144 | 4,915 | |
| São Paulo | 1,224 | 598 | 613 | 7,176 | 7,356 | 5,885 | |
| South | 2,664 | 1,090 | 1,090 | 13,080 | 13,080 | 10,464 | |
| Paraná | 828 | 373 | 374 | 4,476 | 4,488 | 3,590 | |
| Santa Catarina | 948 | 355 | 356 | 4,260 | 4,272 | 3,418 | |
| Rio Grande do Sul | 888 | 362 | 360 | 4,344 | 4,320 | 3,456 | |
| Midwest | 1,536 | 832 | 835 | 12,480 | 12,525 | 10,020 | |
| Mato Grosso do Sul | 336 | 222 | 225 | 3,330 | 3,375 | 2,700 | |
| Mato Grosso | 396 | 194 | 193 | 2,910 | 2,895 | 2,316 | |
| Goiás | 528 | 223 | 223 | 3,345 | 3,345 | 2,676 | |
| Federal District | 276 | 193 | 194 | 2,895 | 2,910 | 2,328 | |
a)PSU: primary sampling unit.
In order to define the PSU sample size (md), the number of households selected in each PSU was set and then the size of the sample of households was divided by this number: 12, 15 or 18, depending on the domain – population subgroups, for which separate estimates are planned:
where nACd corresponds to the sample size according to domain-conglomerated sampling.
This difference was due to the PSU sample size being limited by the main sample.
Owing to the complex sampling design and distinct selection probabilities, in order to analyze the PNS data, expansion factors or sample weighting need to be defined, both for the selected households and the selected household residents. The final weighting applied is a product of the inverse of the selection probability expressions of each stage of the sampling plan, which includes correction for non-responses and adjustments to total populations.
Samples that originate conglomerate surveys should be analyzed using statistical analysis programs that have packages for complex data, i.e. which have a logarithm capable of taking into consideration the effects of stratification and conglomeration on indicator estimates and their measurements of accuracy.
As such, when the analysis is performed, three variables need to be taken into consideration in order for the data to be representative of the population for which estimates are intended to be obtained. The three variables are: PSU, stratum and weighting.
Making the PNS 2019 database available is the responsibility of the IBGE, and it can be accessed on the PNS page of the institution's website. A dictionary of variables is also made available together with the database which enables these three variables to be identified. Moreover, distinct weightings are prepared for analysis of all the residents in a household and for analysis of the selected resident. Use of each weighting depends on the dataset which is intended to be analyzed, as well as on the section of the questionnaire to which the data belongs.
Questionnaire
Several meetings were held to review the PNS 2019 questionnaire, with the presence of specialists and representatives of Ministry of Health technical areas. Following this, there was a discussion stage with the IBGE, with the aim of enhancing question flow and the semantics of the questionnaire.
Some blocks of questions were altered in the second edition and others were included. Answer options with low response percentages in 2013, i.e. those that had a high coefficient of variation (above 30%), to the extent of not achieving the accuracy desired, were excluded from the second edition when appropriate. Overall, most of the questionnaire was comparable with the 2013 edition. An important change was made with regard to data collection: the PNS 2013 was directed towards people aged 18 years old or over, while the 2019 edition selected people aged 15 or over for interviewing (with the exception of three thematic blocks).
The final questionnaire was divided into three sections:
-
Household questionnaire
Questions on information about the household and questions about household visits made by endemic disease workers and the Family Health team. This part of the questionnaire was answered by the resident identified as being the head of the household.
-
Questionnaire for all residents in the household
General information was collected on all residents in the household. This information was given by a resident age 18 or over who answered on behalf of the rest (proxy). Questions were asked about: level of schooling; information about occupation; household income; physical and/or intellectual disability; health insurance coverage; health service access and use; the health of individuals age 60 or over; and the health of children under 2 years old.
-
Questionnaire for the selected resident
This block of questions was aimed at one selected resident, aged 15 or over. Information was obtained about work and social support characteristics, perception of state of health, accidents, lifestyles, chronic noncommunicable diseases, women's health, prenatal care, oral health, paternity and male partner prenatal care, in relation to people aged 15 or over; questions about violence, communicable diseases, sexual activity, work relations and conditions, and medical care, were only answered by those aged 18 or over. Figure 3 shows the questionnaire modules contained in the 2013 and 2019 PNS versions.
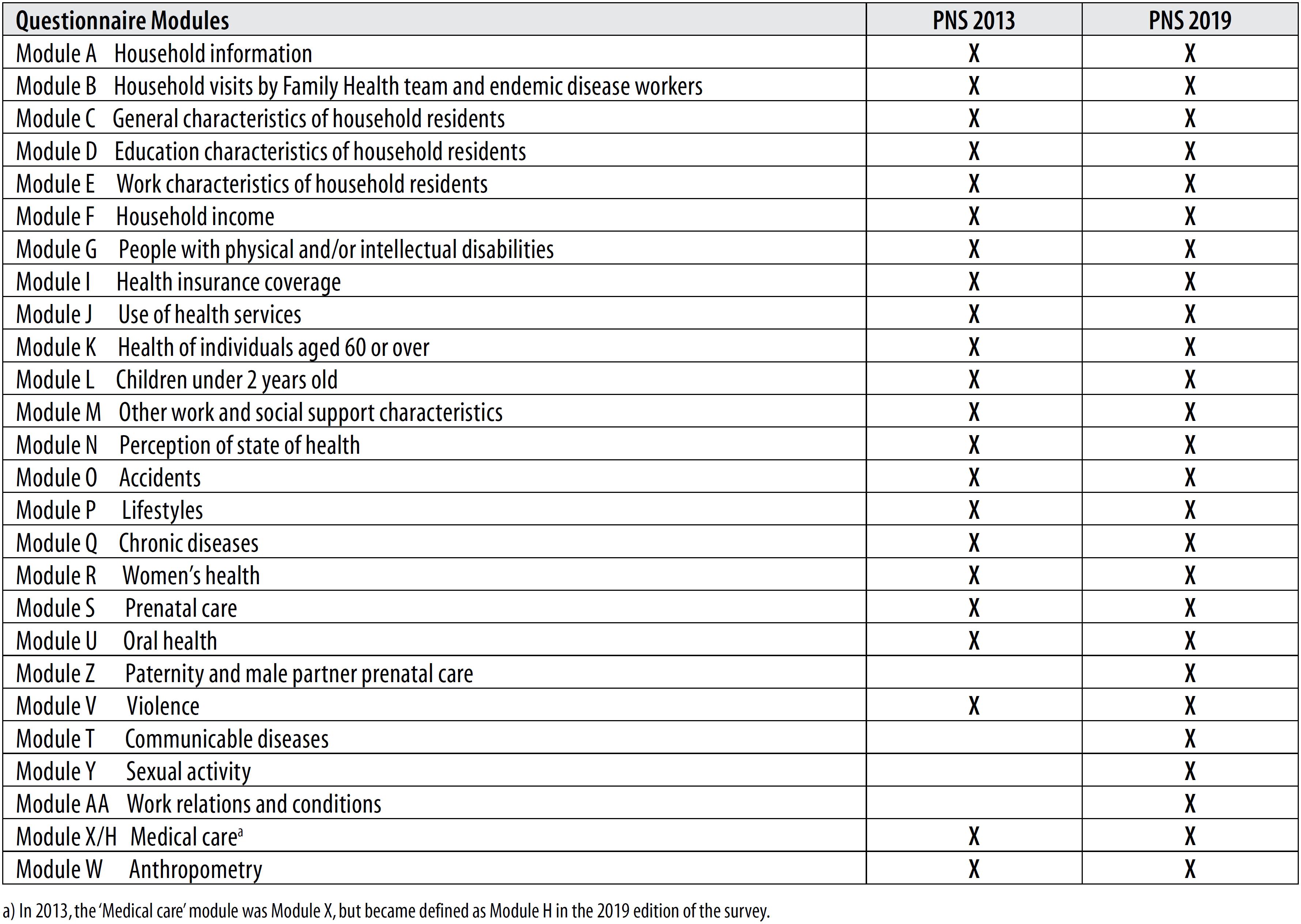
Figure 3 Description of the National Health Survey (PNS) questionnaire modules, Brazil, 2013 and 2019
Finally, the PNS 2019 collection instrument was submitted to a pretest with small samples of individuals. This process was conducted and developed by those responsible for the PNS at the state-level IBGE units. Furthermore, the new questions added to the PNS 2019 underwent a validation process, i.e. a cognitive test, conducted in a community of low socioeconomic status in the city of Rio de Janeiro, RJ. The objective of this test was to assess understanding of each question to be asked of interviewees, in order to obtain the true perception of the instruments and the need to make adjustments if deemed necessary.
Data collection
Data collection organization and field work coordination were done by the IBGE and involved data collection agents (interviewers), supervisors (data collection supervision and collection agent management) and coordinators (responsible for the survey at a given state-level or central IBGE unit) from among IBGE personnel.
Training of coordinators and all other people involved was comprised of two stages: first of all, the state-level IBGE unit coordinators were trained at a workshop held in the city of Bento Gonçalves, RS. When the workshop participants returned to their units they passed on the contents of the training to the supervisors and data collection agents. During the data collection process, the field teams (coordinators, supervisors and collection agents) took part in simultaneous training with the possibility of making queries online.
The interviews were conducted using mobile data collection devices (MDCD), programmed to “jump” questionnaire items and to perform critical analysis of the variables. When arriving at the selected household, first of all the collection agent spoke to the head of the household or other household resident. The agent explained the objectives to the household residents, the data collection procedure and the importance of their participation in the survey. At this time a list was made of all individuals resident in the household, regardless of whether they agreed or not to take part in the survey.
Following this, the resident who would provide the information for the household questionnaire and the questionnaire about all those resident in the household was identified, and a resident age 15 years old or over was randomly selected to answer the individual interview. The interviews were scheduled for the most convenient time for the household residents. Two or more visits were planned to be made to each household.
The PNS 2019 data was collected between August 2019 and March 2020.
Anthropometric measurements
With regard to collection of anthropometric data, only the weight and height of the selected subsample of residents aged 15 or over were measured. Weighing scales, portable stadiometers and gauges, as well as anthropometric tape measures, were used to collect these data.
Anthropometric data collection training was developed in partnership with Fiocruz and the University of São Paulo Public Health Faculty Population Nutrition Assessment Laboratory. It was also part of the training provided to coordinators and supervisors at the state-level IBGE units.
This training stressed the importance of daily calibration of the instruments in order to obtain accurate measurements. In addition to face-to-face training, the entire IBGE field work team also received instructional material (manuals and videos) about how to proceed with instrument organization and calibration involving straightforward techniques such as calibrating weighing scales using PET bottles filled with water as an easy way of checking.
With regard to measuring weight and height, the data collection agents were trained on how to approach household residents, how to set up the equipment and take measurements. When measuring height, the collection agents were instructed to ask interviewees to take off their shoes, any heavy clothing and hair accessories, to stand up straight with their heels and legs together and their head upright looking straight ahead. When measuring weight, the collection agents were instructed to ask interviewees to stand with their feet centered on the scales looking straight ahead.
Ethical aspects
The data collection team was trained to understand that the aim of the survey was to investigate by means of the questions asked and the measurements taken. Data collection agents and field coordinators were prepared in order to answer questions about the survey procedures.
The PNS ensured the confidentiality of the identification and personal data of participants, household residents and interviewees. Informed consent was obtained in two stages directly on the MDCD. In the first stage, i.e. the interview about the household, consent was obtained before the information given by the household informant (proxy) was collected. Following this, a household resident aged 15 years old or over was selected for the individual interview and, if they agreed, consent was obtained both for the interview and for anthropometric measurements to be taken.
Respondents aged 15 to 17 years old did not answer the questions contained in the ‘Violence’, ‘Communicable diseases’, ‘Sexual activity’, ‘Work relations and conditions’ and ‘Medical care’ modules.
The National Health Survey 2019 project was submitted to the National Research Ethics Committee/National Health Council and approved as per Opinion No. 3.529.376, issued on August 23rd 2019.
Final considerations
The PNS 2019 is another step forward with health investigations in Brazil. It is extremely important to ensure continuity of health indicator monitoring, and to translate these indicators into policies or actions to enhance the SUS.
The first edition of the PNS expanded and furthered investigation into health issues that had been taking place nationally, mainly through the PNAD Health Supplements. As it has been an independent survey right from the beginning, i.e. it was designed with the purpose of collecting health information, the PNS estimates indicators of interest with the desired accuracy. It is important to emphasize here the comparability between the indicators of the two editions of the survey, enabling monitoring of possible changes in estimates over the period between the two surveys.
As in 2013, the PNS 2019 kept the commitment to provide continuity to the periodical investigation of the themes of health service access and use, as well as health insurance coverage in Brazil, as begun in 1998 through the PNAD Health Supplement. As such, national progress and challenges in this area have been accompanied for more than 20 years. Consequently, the PNS 2019 not only provides continuity to the investigation of these themes; it accompanies, over time, aspects covered by the Health Supplement samples. Therefore, given that the data collected by the two editions of the survey can be compared, it is possible to monitor the evolution of the indicators.
The importance of going into greater depth with regard to questions of reported morbidity must be noted, more than just estimating prevalence among the population, but rather investigating recommendations for behavioral measures that directly influence people's health, as well as access to medication and regular use of health services to monitor an illness. The possibility of monitoring such data, at different times, enables knowledge of the magnitude of a disease or health condition, the profile of behaviors adopted by the affected population, which is paramount in informing the (re)planning of health priorities and actions.7,10 In this sense, when the Strategic Action Plan for Addressing Chronic Noncommunicable Diseases (NCD) in Brazil 2011-2022,18 one of the main guiding instruments for NCD surveillance in the country, was published in 2011, the actions it planned included the 2013 and 2019 editions of the PNS. The Strategic Action Plan brings together qualified tools for supporting NCD monitoring.
A differential of the PNS 2019 was the change to the age range of the household resident selected for interview. This change was made because of the need to collect valid data for monitoring the indicators established by the Sustainable Development Goals (SDG).19 Notwithstanding, the indicators that will be presented in official IBGE and Ministry of Health publications will relate to the population aged 18 years old or over, with the aim of enabling comparison between survey editions. Indicators of relevance for the SDGs will also be presented for the population aged 15 years old or over.
Standing out among the new modules incorporated into the PNS 2019 are (i) ‘Communicable diseases’, with reference to presence of persistent coughing, numb skin blemishes, Chagas’ disease and sexually transmitted infections, (ii) ‘Sexual activity’, investigating sexual initiation, condom use and access, (iii) ‘Medical care’, focusing on Primary Health Care access and quality, and (iv) ‘Paternity and male partner prenatal care’, which addresses issues of prenatal monitoring of male partners20 with the aim of being an entry point for men to access primary care. All these themes were requested by Ministry of Health technical areas.
The ‘Violence’ module was also reformulated in the PNS 2019, in order to investigate, separately, psychological, physical and sexual violence, as well as the need to use health services because of violence considered to be more severe. The theme of violence is considered to be complex and sensitive,21 and in order to ensure the privacy of the interviewee, the option was taken for them to answer these questions themselves directly on the MDCD. If the interviewee did not feel comfortable using the MDCD or if they had difficulty in reading the questions directly on the MDCD, the interviewer would ask the questions. In these situations, the interviewer made a note on the MDCD that the privacy of the interview had not been guaranteed and that the answers may possibly have been given in front of another person. Apart from the ‘Violence’ module, two other modules were also answered directly by the interviewee: ‘Communicable diseases’ and ‘Sexual activity’.
The PNS 2019 collected information on weight and height as a subsample. Despite the reduced number of anthropometric measurements in relation to the 2013 edition of the survey, the data obtained by the PNS 2019 will enable monitoring of overweight and obesity in Brazil (in both urban and rural areas) as well as in the country's macro-regions. Other surveys, such as the Non-Communicable Disease Risk and Protective Factors Surveillance Telephone Survey System22 (VIGITEL), also investigate the same data, although these are reported by interviewees themselves. The PNS estimates, measured with calibrated anthropometric equipment, are considered to be gold standard. As such, taking these measurements becomes essential in large household surveys.
The PNS is one of the main instruments used by the Ministry of Health to respond to/monitor global indicators, including those of the SDGs,19 those of the Global Action Plan for the Prevention and Control of NCDs 2013-202023 and those of the Strategic Action Plan for Addressing Chronic Noncommunicable Diseases (NCD) in Brazil 2011-2022.18 Moreover, the PNS is the gold standard for Brazilian health surveys because it is the country's largest, most complete and comprehensive health survey. Other surveys, such as the VIGITEL survey,22 use PNS estimates to valid the findings of their monitoring activities. As such, the 2019 edition of the PNS will also enable a new evaluation of the quality of the VIGITEL survey, the main annual health survey conducted by the Ministry of Health, used to monitor health risk factors among the Brazilian population.
Apart from the classic limitations of studies with a cross-sectional design – not determining causality, or excluding street dwellers and people in asylums, for instance –, a limitation of the PNS is that it does not estimate data for geographic areas smaller than the municipal areas of the state capitals. A further limitation is that data on part of the themes investigated by the PNS (the questionnaire about the household and the questionnaire about all the household residents) is collected from just one household resident who answers on behalf of him/herself and also on behalf of all the other residents in the household (proxy). With regard to the resident selected, only in the case of their not being able to answer because of physical or mental health reasons was another resident asked to answer instead. However, studies conducted based on other health surveys have demonstrated good agreement and reproducibility between information collected by means of a proxy and information provided by the people represented by the proxy.24,25
The intention is to publish the PNS 2019 results in official IBGE reports – in partnership with the Ministry of Health –, together with descriptive analyses of indicators already selected; as well as through production and publication of scientific material. The PNS 2019 results are also expected to be available on a data platform/panel, with the possibility of performing simple tabulations, as well as on the IBGE website databases, for more complex analyses.
Conducting a health survey of the amplitude of the National Health Survey 2019 represents progress for Brazilian Public Health. The information obtained through the Survey will serve to inform future actions and policies of the Brazilian National Health System (SUS), as well as to support monitoring and evaluation of existing health programs and services.
Referências
1. Cesar CLG, Goldbaum M. Usos de serviços de saúde. In: Cesar CLG, Carandina L, Alves MCGP, Azevedo MB, Goldbaum M. Saúde e condição de vida em São Paulo: inquérito multicêntrico de saúde no Estado de São Paulo: ISA-SP. São Paulo: Faculdade de Saúde Pública da USP; 2005. p. 185-98. [ Links ]
2. Travassos CMR, Viacava F, Laguardia J. Os suplementos saúde na pesquisa nacional por amostra de domicílios (PNAD) no Brasil. Rev Bras Epidemiol [Internet]. 2008 [citado 2020 ago 17];11 Supl 1:98-112. Disponível em: https://doi.org/10.1590/S1415-790X2008000500010 [ Links ]
3. Szwarcwald CL, Malta DC, Pereira CA, Vieira MLFP, Conde WL et al. Pesquisa Nacional de Saúde no Brasil: concepção e metodologia da aplicação. Ciênc Saúde Coletiva [Internet]. 2014 fev [citado 2020 ago 14];19(2):333-42. Disponível em: https://doi.org/10.1590/1413-81232014192.14072012 [ Links ]
4. Barreto ML. Desigualdades em saúde: uma perspectiva global. Ciênc Saúde Coletiva [Internet]. 2017 jul [citado 2020 jago 14];22(7):2097-108. Disponível em: https://doi.org/10.1590/1413-81232017227.02742017 [ Links ]
5. Szwarcwald CL, Souza-Júnior PBR, Damacena GN. Socioeconomic inequalities in the use of outpatient services in Brazil according to health care need: evidence from the World Health Survey. BMC Health Serv Res [Internet]. 2010 [cited 2020 Aug 14];10:217. Available from: https://doi.org/10.1186/1472-6963-10-217 [ Links ]
6. Carvalheiro JR. Investigação epidemiológica e entrevistas domiciliarias. Rev Saúde Pública [Internet]. 1981 out [citado 2020 ago 14];15(5):543-50. Disponível em: https://doi.org/10.1590/S0034-89101981000500007 [ Links ]
7. Barros MBA. Inquéritos domiciliares de saúde: potencialidades e desafios. Rev Bras Epidemiol [Internet] 2008 maio [citado 2020 ago 14];11(supl1):6-19. Disponível em: https://doi.org/10.1590/S1415-790X2008000500002 [ Links ]
8. Viacava F, Dachs N, Travassos C. Os inquéritos domiciliares e o sistema Nacional de Informações em Saúde. Ciênc Saúde Coletiva [Internet]. 2006 dez [citado 2020 ago 14];11(4):863-9. Disponível em: https://doi.org/10.1590/S1413-81232006000400002 [ Links ]
9. Viacava F. Dez anos de informação sobre acesso e uso de serviços de sáude. Cad Saude Pública [Internet]. 2010 dez [citado 2020 ago 14];26(12):2210-1. Disponível em: https://doi.org/10.1590/S0102-311X2010001200001 [ Links ]
10. Malta DC, Leal MC, Costa MFL, Morais-Neto OL. Inquéritos nacionais de saúde: experiência acumulada e proposta para o inquérito de saúde brasileiro. Rev Bras Epidemiol [Internet]. 2008 maio [citado 2020 ago 14];11(suppl 1):159-67. Disponível em: https://doi.org/10.1590/S1415-790X2008000500017 [ Links ]
11. Brasil. Ministério da Saúde. Portaria MS/GM nº 1.811, de 12 de agosto de 2009. Institui, no âmbito do Ministério da Saúde, Comitê Gestor com a finalidade de planejar e coordenar a criação do Inquérito Nacional de Saúde – INS [Internet]. Diário Oficial da União, Brasília (DF), 2009 ago 12 [citado 2020 mar 27]. Disponível em: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2009/prt1811_12_08_2009.html [ Links ]
12. Brasil. Ministério da Saúde. Portaria MS/GMnº 2.350, de 5 de outubro de 2011. Institui, no âmbito no Ministério da Saúde, o Comitê Gestor da Pesquisa Nacional de Saúde (PNS) [Internet]. Diário Oficial da União, Brasília (DF), 2011 out 6 [citado 2020 abr 12];Seção 1:58 Disponível em: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt2350_05_10_2011.html [ Links ]
13. Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional de Saúde 2013: percepção do estado de saúde, estilos de vida e doenças crônicas [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2014 [citado 2020 fev 22]. 180 p. Disponível em: https://biblioteca.ibge.gov.br/visualizacao/livros/liv91110.pdf [ Links ]
14. Instituto Brasileiro de Geografia e Estatística - IBGE. Pesquisa Nacional de Saúde 2013: acesso e utilização dos serviços de saúde, acidentes e violências [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2015 [citado 2020 fev 22]. 98 p. Disponível em: https://biblioteca.ibge.gov.br/visualizacao/livros/liv94074.pdf [ Links ]
15. Instituto Brasileiro de Geografia e Estatística - IBGE. Pesquisa Nacional de Saúde 2013: ciclos de vida [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2015 [citado 2020 fev 22]. 85 p. Disponível em: https://biblioteca.ibge.gov.br/visualizacao/livros/liv94522.pdf [ Links ]
16. Instituto Brasileiro de Geografia e Estatística - IBGE. Pesquisa Nacional de Saúde 2013: indicadores de saúde e mercado de trabalho [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2016 [citado 2020 fev 22]. 66 p. Disponível em: https://biblioteca.ibge.gov.br/visualizacao/livros/liv97329.pdf [ Links ]
17. Brasil. Ministério da Saúde. Portaria MS/GM nº 1.002, de 13 de abril de 2017. Institui, no âmbito no Ministério da Saúde, o Comitê Gestor da Pesquisa Nacional de Saúde 2018 – PNS/2018 [Internet]. Diário Oficial da União, Brasília (DF), 2017 abr 13 [citado 2020 abr 09];Seção 1:30. Disponível em: https://bvsms.saude.gov.br/bvs/saudelegis/gm/2017/prt1002_17_04_2017.html [ Links ]
18. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância de Doenças e Agravos Não Transmissíveis e Promoção da Saúde. Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis (DCNT) no Brasil 2011-2022 [Internet]. Brasília: Ministério da Saúde; 2011 [citado 2020 ago 14]. 160 p. Disponível em: https://bvsms.saude.gov.br/bvs/publicacoes/plano_acoes_enfrent_dcnt_2011.pdf [ Links ]
19. Organização das Nações Unidas - ONU. Objetivos de desenvolvimento sustentável [Internet]. [S.l]: Organização das Nações Unidas; 2017 [citado 2020 abr 13]. Disponível em: https://nacoesunidas.org/pos2015/agenda2030/ [ Links ]
20. Ministério da Saúde (BR). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. Coordenação Nacional de Saúde do Homem. Guia do pré-natal do parceiro para profissionais de saúde [Internet]. Brasília: Ministério da Saúde; 2016 [citado 2020 ago 14]. 55 p. Disponível em: https://portalarquivos2.saude.gov.br/images/pdf/2016/agosto/11/guia_PreNatal.pdf [ Links ]
21. Schraiber LB, d’Oliveira AFPL, Couto MT. Violência e saúde: contribuições teóricas, metodológicas e éticas de estudas da violência contra a mulher. Cad Saúde Pública [Internet]. 2009 [citado 2020 ago 14];25 Sup 2:S205-16. Disponível em: https://doi.org/10.1590/S0102-311X2009001400003 [ Links ]
22. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Análise em Saúde e Vigilância de Doenças Não Transmissíveis. Vigitel Brasil 2019: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico [Internet]. Brasília: Ministério da Saúde; 2020 [citado 2020 ago 14]. 137 p. Disponível em: http://www.crn1.org.br/wp-content/uploads/2020/04/vigitel-brasil-2019-vigilancia-fatores-risco.pdf?x53725 [ Links ]
23. Organização Mundial da Saúde - OMS. Plano de ações globais para prevenção e controle das DCNT 2013-2020 [Internet]. Genebra: Organização Mundial da Saúde; 2013 [citado 2020 ago 14]. Disponível em: https://apps.who.int/iris/bitstream/handle/10665/94384/9789241506236_eng.pdf;jsessionid=A5E572CA1D2F8DE7F416EAAFDF6065D1?sequence=1 [ Links ]
24. Jardim R, Barreto SM, Giatti L. Confiabilidade das informações obtidas de informante secundário em inquéritos de saúde. Cad Saúde Pública [Internet]. 2010 [citado 2020 ago 14];26(8):1537-48. Disponível em: https://doi.org/10.1590/S0102-311X2010000800008 [ Links ]
25. Santana VS, Almeida Filho N, Rocha CO, Matos AS. Confiabilidade e viés do informante secundário na pesquisa epidemiológica: análise de questionário para triagem de transtornos mentais. Rev Saúde Pública [Internet]. 1997 dez [citado 2020 ago 14];31(6):556-65. Disponível em: https://doi.org/10.1590/S0034-89101997000700003 [ Links ]
Received: May 18, 2020; Accepted: July 09, 2020
 This content is licensed under a Creative Commons Attribution 4.0 International License.
This content is licensed under a Creative Commons Attribution 4.0 International License.
