










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.1 Brasília 2021 Epub 22-Dez-2020
http://dx.doi.org/10.1590/s1679-49742021000100025
Original article
Lockdown-type containment measures for COVID-19 prevention and control: a descriptive ecological study with data from South Africa, Germany, Brazil, Spain, United States, Italy and New Zealand, February - August 2020
1Universidade Federal de Pelotas, Faculdade de Medicina, Pelotas, RS, Brazil
2Universidade Federal de Pelotas, Faculdade de Agronomia, Pelotas, RS, Brazil
Objective
To describe lockdown-type containment measures and COVID-19 incidence in South Africa, Germany, Brazil, Spain, United States, Italy and New Zealand.
Methods
This is a descriptive ecological study with data on daily incidence of confirmed COVID-19 cases from February 22 to August 31 2020, as well as information on lockdown measures implemented by the governments of each country.
Results
Daily COVID-19 incidence (cases per 1 million inhabitants) decreased within three weeks after lockdown started in the countries that implemented it: South Africa (3.7 to 1.7), Germany (37.5 to 33.7) Spain (176.3 to 82.0), Italy (92.0 to 52.1) and New Zealand (7.5 to 1.7). As for Brazil and the United States, which did not implement lockdown, there was no considerable decrease.
Conclusion
After lockdown implementation, there was a considerable decrease in the number of confirmed cases.
Key words: Coronavirus Infections; Social Distance; Incidence; Pandemics; Disease Prevention
Introduction
On December 31st 2019, 27 cases of pneumonia of unknown etiology were identified in Wuhan, capital of Hubei Province, China.1 In January 2020, analysis of lower respiratory tract samples identified the novel severe acute respiratory syndrome coronavirus (SARS-CoV-2) as being the causative agent of the cluster found.2The disease was named COVID-19 by the World Health Organization (WHO).
The first case outside China was confirmed in Bangkok, Thailand, on January 13th 2020.3 On January 30th 2020, WHO declared the COVID-19 outbreak to be a Public Health Emergency of International Concern, warning as to the high risk infection in countries with vulnerable health systems.4 At that time, however, the Emergency Committee believed that the spread of COVID-19 could be interrupted by early detection, isolation, immediate treatment and implementation of a robust contact tracing system.5 WHO finally declared the outbreak to be a pandemic on March 11th 2020.6
By August 21st 2020, a total of 21,294,845 confirmed COVID-19 cases and 761,779 COVID-19 deaths had been registered, in 216 countries, areas or territories.7 Regions in Asia and Europe became epicenters of the pandemic, and the growth and rapid spread of infection on a global scale led to the 24,257,989 cases registered as at August 28th 2020.8
Unfortunately, there has not been a standardized global response for addressing the pandemic. Each country has addressed the crisis according to its possibilities, knowledge and hypotheses raised by their epidemiological surveillance services10 Considering that there is no effective treatment and no vaccine available, implementation of several non-pharmaceutical interventions, including containment measures, have shown themselves to be the best alternatives available for avoiding infection and controlling the spread of the virus.11
As a consequence of their different responses, the virus spread at different speeds in the countries: some have had relative success in controlling transmission, while others have not, despite the containment measures adopted.
This study sought to describe lockdown-type containment measures and COVID-19 incidence in seven different countries: South Africa, Germany, Brazil, Spain, United States, Italy and New Zealand.
Methods
A descriptive ecological study was conducted on COVID-19 incidence, information about lockdown type containment measures implemented by the governments of the seven countries studied and their effects on daily incidence of confirmed cases between February 22nd and August 31st 2020.
The majority of the countries included in the study – Germany, Spain, United States, Italy and New Zealand – are high-income countries. South Africa and Brazil, considered to be emerging countries, are classified as being upper-middle-income countries.12 South Africa is located in the far south of the African continent and has 59,308,690 inhabitants,13 70% of whom are Black.14 The populations of the European countries of Germany, Spain and Italy are 83,783,942, 46,754,778 and 60,461,826 inhabitants, respectively.13 The populations of Brazil, in South America, and the United States, in North America, are 212,559,417 and 331,002,651 inhab.,13 respectively, both characterized by large-scale immigration from diverse parts of the world. New Zealand, in Oceania, has 4,822,233 inhabitants.13
Information on the containment measures used by the governments of each of these countries to prevent COVID-19 was retrieved from the Assessment Capacities Project (ACAPS) website. ACAPS has described the measures taken by each country and the date on which they were implemented based on a compilation of publications in the main communication media or official websites of the respective governments. ACAPS has divided these measures into five categories: (i) movement restrictions; (ii) Public Health measures; (iii) governance and socioeconomic measures; (iv) social distancing; and (v) lockdown (Figure 1).15

Lockdown can be classified as total or partial confinement. Total confinement is defined as ‘total suspension of non-essential activities with restriction of people’s movements’16 with only crucial services in operation, such as health and food supply, for instance. In the case of partial lockdown, some non-essential services may operate, under rigorous surveillance measures.
Daily COVID-19 incidence information was retrieved from the European Center for Disease Prevention and Control;17 when this was not available, information was taken from the WHO daily report on COVID-19.18 The size of each country’s population was taken from United Nations Organization (UNO) estimates for 2020.13
Each country’s relative frequency was described by taking the daily incidence rate, calculated by dividing the daily number of confirmed COVID-19 cases for each country by its total population and multiplying by 1,000,000 (cases per 1 million inhabitants). The data were analyzed using Microsoft Excel version 2016.
Results
South Africa’s first COVID-19 case was recorded on March 6th 2020. It experienced a progressive increase in cases and on March 27th, now with 918 recorded cases, it decreed its first total lockdown, which was expected to end by April 16th (Figure 2 and Table 1). On April 9th, however, this initial deadline was extended to April 30th. On the day of the first decree (March 27th), the national incidence rate was 3.7/1 million inhab.; four days into lockdown it had fallen to 1.7/1 million inhab. and stayed below the rate reported on the date lockdown came into force until April 17th. After this date, incidence increased, despite the social distancing measure having been kept in force, and by April 30th it had reached 6.0/1 million inhab. Nevertheless, with effect from May 1st, relaxation for total lockdown was planned, with a gradual return to economic activities. From then on, there was a gradual increase in cases and by May 24th the national rate had reached 20.4/1 million inhab.; a week later, on May 31st, the rate was 29.1/1 million inhab. confirmed cases, while the country continued to reestablish economic activities. In June, the containment measures to which the reestablishment of activities were subject were relaxed and, as a consequence, the incidence rate had increased to 103.4 cases per 1 million inhab. by June 30th. In July case incidence continued high and distancing and hygiene protocols were maintained, in addition to awareness campaigns. In August, cases fell continuously and by August 31st the incidence rate was 40.2/1 million inhab.
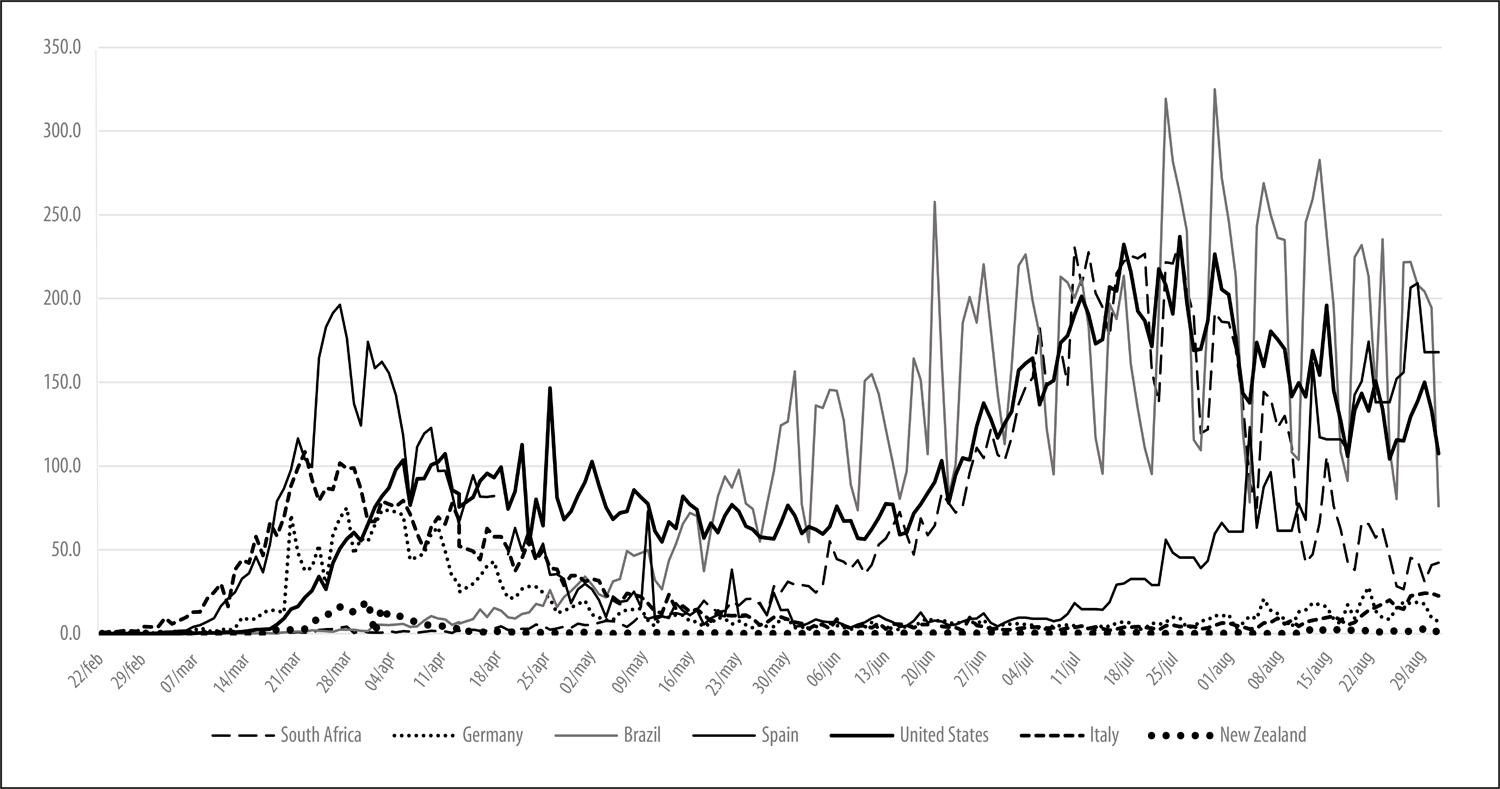
Figure 2 – Daily incidence of confirmed COVID-19 cases (per 1 million inhabitants) in South Africa, Germany, Brazil, Spain, United States, Italy and New Zealand, February 22nd – August 31st 2020
Table 1 – Daily Incidence of confirmed COVID-19 cases (per 1 million inhabitants) with effect from lockdown implementation, by countries studied
| Country | Type of lockdown implemented | Date lockdown implemented | Extent | Incidence rate on lockdown implementation date | Incidence rate 14 days after lockdown implementation | Incidence rate 25 days after lockdown implementation |
|---|---|---|---|---|---|---|
| South Africa | Total | 27/03/2020 | Entire country | 3.7 | 1.2 | 2.4 |
| Germany | Partial | 22/03/2020 | Entire country | 37.5 | 70.8 | 34.2 |
| Brazil |
Partial Partial |
08/04/2020a 16/05/2020b |
Some cities Some cities |
7.8 72.0 |
11.8 126.7 |
23.4 151.0 |
| Spain |
Total Partial Total |
13/03/2020 16/03/2020 28/03/2020 |
Some cities Entire country Entire country |
32.7 36.5 176.3 |
196.4 124.3 97.3 |
111.4 97.0 49.4 |
| United States | Partial | – | – | – | – | – |
| Italy |
Partial Partial Total |
08/03/2020c 20/03/2020 23/03/2020 |
Some cities Entire country Entire country |
20.6 88.0 92.0 |
108.4 77.2 71.4 |
79.1 52.2 62.6 |
| New Zealand |
Total |
23/03/2020 |
Entire country |
7.5 |
8.1 |
0.4 |
a) Date on which partial lockdown was decreed in the country’s largest city, São Paulo, SP.
b) Date on which partial lockdown was decreed in the following cities: São Luis, MA; Fortaleza, CE; Recife, PE; Rio de Janeiro, RJ; and São Paulo, SP.
c) Date on which partial lockdown was decreed in northern regions of Italy (Lombardy and Veneto).
Germany recorded its first case on January 28th. Social distancing measures were recommended there with effect from March 10th, when 1139 cases had been recorded. On March 22nd (incidence rate = 37.5/1 million inhab.), partial lockdown was established for the entire country and expected to last until April 15th (Figure 2 and Table 1). Once lockdown had been established, the incidence rate began to fall and as at April 25th it had fallen to around 26.0/1 million inhab. Notwithstanding the reduction in confirmed cases, the partial lockdown was extended until May 3rd. It was only on May 30th, when the incidence rate had fallen to 8.8/1 million inhab., that religious ceremonies, fitness centers and open-air sports began to be allowed again. On June 24th (incidence rate = 7.0/1 million inhab.), partial lockdown was decreed in two districts of North Rhine-Westphalia, following a COVID-19 outbreak, until July 6th (incidence rate = 2.6/1 million inhab.). After that date, the highest incidence rate was recorded on August 21st (27.8/1 million inhab.), but no new measures were reported.
Brazil recorded its first COVID-19 case on February 26th. On April 15th, with 25,262 confirmed cases, the Federal Supreme Court ruled that the country’s states, Federal District and municipalities were allowed to make their own decisions as to implementation of social distancing measures.19 The federal administration undertook few actions, while implementation of different social distancing measures varied between the states and in terms of dates.20 On April 8th, when the incidence rate was 7.8/1 million inhab., Brazil decided to restrict domestic travel, suspend international flights and close its borders (Figure 2 and Table 1).
Once businesses began to reopen, which each place defined as it saw fit, using facemasks became obligatory in commercial establishments, public transport and essential services in almost all the country’s municipalities. Even so, the incidence rate increased progressively from 17.6 on April 25th to 97.9/1 million inhab. on May 24th. On June 19th, when the incidence rate had reached 107.1/1 million inhab., guidelines were published on measures for social distancing, respiratory etiquette, use of masks, hand sterilization, cleaning instructions and household isolation for suspected and confirmed cases. On July 6th (122.6 cases per 1 million inhabitants), restaurants, bars and beauty salons were allowed to open throughout the country. Nevertheless, this measure was not adopted in some places. No new national measures had been implemented by the end of August, when the average COVID-19 incidence rate reached 190.0/1 million inhab.
Spain’s first case was recorded on February 1st. On March 13th, when the country had recorded 5958 confirmed cases, some places implemented total lockdown (Figure 2 and Table 1). On March 16th, partial lockdown was implemented throughout the entire country. It allowed Spanish citizens to go out of their homes as long as they complied with basic preventive measures: hand sterilization and use of facemasks. On March 28th (incidence rate = 176.3/1 million inhab.), total lockdown (only essential workplaces open) was imposed nationwide and expected to last until April 9th. On April 4th, when the incidence rate was 142.5/1 million inhab., total lockdown was extended until April 26th. Between April 4th and 12th, the daily incidence rate decreased from 168.3 to 103.3/1 million inhab. (Figure 2). Total lockdown was relaxed on April 13th, when some sectors were allowed to start operating again. On May 25th, the beaches began to reopen and on June 8th (incidence rate = 3.6/1 million inhab.), diverse business establishments and public places were allowed to reopen, although with limited capacity. On June 21st, when the incidence rate was 7.1/1 million inhab., it became obligatory to use masks and comply with hygiene measures. In July and August there was a progressive increase in the incidence rate, reaching 209.2/1 million inhab. on August 28th; no new measures were reported in these months.
The first case in the United States was recorded on January 21st. Local containment measures preceded national directives. Movement restriction and social distancing measures in regions most affected by COVID-19 were recommended by the Federal Government on January 31st and April 10th, when the country recorded 6 and 466,033 cases respectively. On March 26th, with an incidence rate of 42.2/1 million inhab., the Centers for Disease Control and Prevention recommended self-quarantine for New York City transport and delivery workers. Despite the measures adopted, no considerable reduction was seen in the incidence rate over time. On May 6th (incidence rate = 72.0/1 million inhab.), agreement was reached on keeping businesses operating and supermarkets open. Guidance on access to events and gatherings was published on June 12th (incidence rate = 69.1/1 million hab.). The incidence rate remained stable from the beginning of May until mid June, with an average of 69.2/1 million inhab. Despite the continuous increase in incidence with effect from mid June (peak on July 25th: 236.9/1 million inhab.), some household isolation policies were suspended on July 20th. No new containment measures were reported in August and a slight decrease in the incidence rate was seen, with the lowest rate of 104.2/1 million inhab. being reached on August 24th.
Italy recorded its first two cases on January 31st. Social distancing measures and Public Health policies were commended on February 21st, when the country had recorded four cases. Even so, daily incidence increased. On March 8th, when partial lockdown was implemented, the country had 20.6 cases per 1 million inhabitants (Figure 2 and Table 1). On the same day, Lombardy and Veneto were closed off. Incidence continued to rise and on March 20th further restrictions were added to the partial lockdown measures, with inhabitants being obliged to justify any attempt to go out of their homes. On March 23rd, total lockdown was implemented (daily incidence = 92.0/1 million inhab.), totally closing down economic activities and businesses – except essential services. Total lockdown was initially planned to last for 21 days (until April 13th), but was extended until May 3rd. Two weeks after lockdown had been implemented (April 7th), the daily incidence rate had decreased to 59.5/1 million inhab. Once the spread of the virus had been brought under control, on May 4th total lockdown was relaxed.
On May 17th (14.5 cases per 1 million inhabitants), legal directives were established for reopening economic sectors; but Italians were still not allowed to gather in public. On May 21st, norms were defined and publicized for playing sports and, four days later, sports facilities were reopened.
On June 3rd (incidence rate = 5.3/1 million inhab.), movement between the country’s regions was allowed once more and Italy opened its frontiers with other European Union countries. On July 10th (incidence rate = 3.5/1 million inhab.), entry into the country of people from 13 countries considered to be at risk was prohibited. On July 14th (incidence rate = 2.8/1 million inhab.), the extension of the restrictions intended to limit the spread of COVID-19 until July 31st was announced, such as it being obligatory to use facemasks in public and commercial establishments. After these measures were relaxed, in August there was a slight increase, reaching an incidence rate of 24.1/1 million inhab. on August 29th.
New Zealand reported its first case on February 28th. Movement restriction and social distancing measures were adopted on March 13th and 19th, respectively. Total lockdown was implemented on March 23rd and was planned to last for 28 days (April 20th) (Figure 2 and Table 1). On March 31st, eight days after enforcement of total lockdown, the COVID-19 incidence rate reached its peak of 19.7/1 million inhab. (Figure 2). On April 27th, the last day of total lockdown, New Zealand had 0.2 case per 1 million inhabitants. On April 28th, partial lockdown replaced total lockdown.
On May 18th, no new cases were reported and New Zealand announced the reopening of teaching establishments and, on May 29th, allowed gatherings of up to 100 people. The country’s inhabitants were able to return to their routine activities with no restrictions on June 9th when there were still no new confirmed cases. Notwithstanding, the health authorities maintained the recommended basic hygiene measures. In July no new measures were reported and the average incidence rate was 0.2/1 million inhab.
On August 12th, due to new community transmission cases, the Auckland region implemented new measures, such as the restriction of only going out of home for essential activities nearby. In the rest of New Zealand, the measures were not so restrictive and businesses were able to reopen in accordance with Public Health guidelines. In August, the average incidence rate increased to 1.2 case per 1 million inhabitants.
Discussion
The positive effects of lockdown-type containment measures were seen in South Africa, Germany, Spain, Italy and New Zealand, with a reduction in confirmed cases after they were implemented. In Germany, COVID-19 incidence began to decrease one month after lockdown implementation. Cases continued to increase in Brazil and the United States; however, at no time was the decision taken to implement total lockdown in these two countries. In the case of Brazil, the federal government neither adopted nor encouraged the adoption of lockdown measures on the subnational level. Each state implemented partial lockdown, as necessary and according to the orders of their respective governments, with no coordination or control of the health situation in the country as a whole by the federal government.20
Studies suggest that the incubation period may be more than two weeks;21 however, in general, a reduction in COVID-19 incidence was seen 14 days after lockdown was implemented. The measure showed itself to be extremely capable of reducing transmission when taken early when there were still very few confirmed cases. The positive effect of lockdown could be explained by the fact of the measure obliging people to remain in total isolation (assuming they comply with the measure), preventing the virus from spreading from both infected symptomatic and asymptomatic individuals.22 Despite this, it must be noted that the incidence rate decreased in South Africa four days after total lockdown was first decreed, and in Spain seven days after it was decreed. These decreases may not be solely due to lockdown, and may also reflect other containment measures implemented earlier on a national level or in different regions of those countries.
All the countries included in this study, right from when their first COVID-19 cases were confirmed, adopted measures such as suspending lessons at school, limiting gatherings, closing borders, among other measures;16but even so cases continued to increase, so that some, but not all, felt obliged to adopt the lockdown-type containment measure.
Spain and Italy only enforced total lockdown when they reached high daily COVID-19 incidence rates: 183.5/1 million inhab. in Spain and 108.4/1 million inhab. in Italy. Perhaps if these two countries had implemented total lockdown before having so many cases, they could have reduced COVID-19 incidence and achieved control of the disease earlier in their territories. Wilder-Smith et al.23 concluded that early measures are needed in order to contain or, at least, significantly reduce the spread of the virus.
Among the countries studied, the only ones that decreed lockdown when they had few confirmed cases were South Africa and New Zealand. Both implemented total lockdown when they had few daily cases per 1 million inhabitants and reached their highest incidence rate by May 27th, namely 20.9 (South Africa) and 19.7 cases per 1 million inhabitants (New Zealand).
However, South Africa relaxed lockdown on May 1st and incidence began to increase once more. The study conducted by Moris & Schizas in Greece revealed that early adoption of lockdown in response to the COVID-19 pandemic resulted in lower mortality per 1 million inhabitants in a space of 30 days,24 demonstrating that this measure not only has a positive effect on case reduction, but also on the reduction of COVID-19 mortality.
Lack of simultaneous implementation of total lockdown in all affected states or places, whether in Brazil or in the United States, could explain the increase in incidence in these two countries which ultimately decided to close their frontiers, restrict traveling, use of facemasks and other measures; without there being a considerable reduction in confirmed cases despite those measures. In Brazil, increase in cases was even seen in some cities that adopted partial lockdown (social isolation), such as São Paulo, SP. However, it should be noted that compliance with the measure was low, with an average isolation rate of 54%,25 thus hindering achievement of its positive effects. A study conducted using mathematical modeling on the impact of a set of social distancing measures in the metropolitan region of São Paulo, indicates that they could avoid the health system from becoming over burdened and the deaths of almost 90,000 people over the course of the epidemic.26In addition, the combination of social distancing measures – isolation of suspected cases, placing contacts in quarantine and social distancing of the elderly and people at greater risk of severe illness – could reduce by two thirds the peak in the demand for medical care, and reduce deaths by half.27 Sjödin et al. draw attention to the importance of high adherence to community quarantine (strict policy on staying at home) and low density of inhabitants per household, in order to contain an outbreak in a closed-off city. According to those authors, the larger the family and the greater the time that has been spent in public, the longer the quarantine period needed.22
A study conducted in China, aimed at assessing the rigorous lockdown measures implemented there, highlighted their potential for delaying the spread of the virus and, in addition to having found similar results, points to the positive effects of lockdown on reducing COVID-19 case incidence.28Similar results were found in France highlighting the positive effect of lockdown.29
This study has limitations with regard to data searching. Its main source was the ACAPS, an institution that compiles information from the main government communication media and official websites.30 As such, relevant information not identified by ACAPS made have been left out. Another limitation of the study is that it only takes into consideration indicators for countries as a whole, while it is known that there are subnational differences, both in terms of indicators and restriction measures adopted – especially in Brazil and the United States, which are countries of continental dimensions in which measures against the pandemic have not been implemented on a national level. National data do not, therefore, reflect the containment measures adopted in some places. As such, many state and municipal decrees have not been taken into consideration. Moreover, this study does not deal with cultural issues such as customs, education and behaviors, which can modify situations arising from social distancing and isolation and quarantine policies implemented. Finally, the descriptive design of the study does not allow the hypothesis raised to be tested.
When countries such as South Africa, Germany, Spain, Italy and New Zealand implemented lockdown, they had a considerable reduction in daily incidence of cases confirmed by their surveillance systems, despite all the other measures adopted prior to lockdown. It is possible that the lack of national lockdown policies in Brazil and the United States has been a determining factor for daily confirmed cases not having reduced, hence the higher incidence curve and, consequently, the higher number of notified COVID-19 deaths. The findings of this study can contribute to reflections on the policies and measures adopted by governments to prevent and control this type of epidemic. We conclude that prior lockdown implementation is an effective measure for minimizing the impact of COVID-19 on the general population.
REFERENCES
1. Lu H, Stratton CW, Tang YW. Outbreak of pneumonia of unknown etiology in Wuhan, China: the mystery and the miracle. J Med Virol [Internet]. 2020 [cited 2020 Nov 12];92(4):401-2. Available from : https://doi.org/10.1002/jmv.25678 [ Links ]
2. Huang C, Wang Y, Li Z, Ren L, Zhao J, Hu Y, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet [Internet]. 2020 Feb [cited 2020 Nov 12];395(10223);497-506. Available from: https://doi.org/10.1016/s0140-6736(20)30183-5 [ Links ]
3. World Health Organization – WHO. Novel Coronavirus (2019-nCoV): situation report 1. 21 [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Mar 25]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200121-sitrep-1-2019-ncov.pdf [ Links ]
4. World Health Organization - WHO. WHO Director-General's statement on IHR Emergency Committee on Novel Coronavirus [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Nov 12]. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-statement-on-ihr-emergency-committee-on-novel-coronavirus [ Links ]
5. World Health Organization – WHO. Novel Coronavirus (2019-nCoV): situation report - 12 [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Nov 12]. Available from: https://apps.who.int/iris/handle/10665/330777 [ Links ]
6. World Health Organization – WHO. WHO Director-General's opening remarks at the media briefing on COVID-19 - 11 [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Aug 11]. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 [ Links ]
7. World Health Organization - WHO. Weekly operational update on COVID-19 [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Nov 12]. Available from: https://www.who.int/docs/default-source/coronaviruse/weekly-updates/wou-21082020.pdf?sfvrsn=e34ba8f3_2 [ Links ]
8. World Health Organization – WHO. Coronavirus disease 2019 situation report [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Mar 25]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200326-sitrep-66-covid-19.pdf?sfvrsn=9e5b8b48_2 [ Links ]
9. World Health Organization - WHO. Weekly operational update on COVID-19 [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Nov 12]. Available from: https://www.who.int/docs/default-source/coronaviruse/situation-reports/wou-28-august-approved.pdf?sfvrsn=d9e49c20_2 [ Links ]
10. Di Gennaro F, Pizzol D, Marotta C, Antunes M, Racalbuto V, Veronese N, et al. Coronavirus diseases (COVID-19) current status and future perspectives: a narrative review. Int J Environ Res Public Health [Internet]. 2020 Apr [cited 2020 Nov 12];17(8):2690. Available from: https://doi.org/10.3390/ijerph17082690 [ Links ]
11. Adhikari SP, Meng S, Wu YJ, Mao YP, Ye RX, Wang QZ, et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: a scoping review. Infect Dis Poverty [Internet]. 2020 Mar [cited 2020 Nov 12];9:29. Available from: https://dx.doi.org/10.1186%2Fs40249-020-00646-x [ Links ]
12. The World Bank. World Bank Country and lending groups [Internet]. Washington, D.C.: The World Bank; 2020 [cited 2020 Nov 12]. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups [ Links ]
13. Worldmeter. Data based on the latest United Nations population division estimates. Countries in the world by popularion [Internet]. [S.l.]: Worldmeter; 2019 [cited 2020 Nov 12]. Available from: https://www.worldometers.info/world-population/population-by-country/ [ Links ]
14. Republic of South Africa. Statistics South Africa. Mid-year population estimates 2019 [Internet]. Pretoria: Statistics South Africa; 2019 [cited 2020 Nov 12]. Available from: http://www.statssa.gov.za/?s=mid-year+population+estimates&sitem=publicatic [ Links ]
15. The Assessment Capacities Project - ACAPS. Covid19 government measures dataset [Internet]. Geneva: ACAPS; 2020 [cited 2020 Nov 12]. Available from: https://www.acaps.org/covid19-government-measures-dataset [ Links ]
16. Ministério da Saúde (BR). Conselho Nacional de Saúde – CNS. Recomendação nº 036, de 11 de maio de 2020. Recomenda a implementação de medidas de distanciamento social mais restritivo (lockdown), nos municípios com ocorrência acelerada de novos casos de COVID-19 e com taxa de ocupação dos serviços atingido níveis críticos [Internet]. Brasília: Conselho Nacional de Saúde; 2020 [citado 2020 nov 12]. Disponível em: http://conselho.saude.gov.br/recomendacoes-cns/1163-recomendac-a-o-n-036-de-11-de-maio-de-2020 [ Links ]
17. World Health Organization - WHO. Situation reports: Coronavirus disease (COVID-19) weekly epidemiological update and weekly operational update [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Nov 12]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports [ Links ]
18. European Centre for Disease Prevention and Control - ECDC. Download today’s data on the geographic distribution of COVID-19 cases worldwide [Internet]. Solna: ECDC; 2020 [cited 2020 Nov 12]. Available from: https://www.ecdc.europa.eu/en/publications-data/download-todays-data-geographic-distribution-covid-19-cases-worldwide [ Links ]
19. Supremo Tribunal Federal (BR). STF reconhece competência concorrente de estados, DF, municípios e União no combate à Covid-19 [Internet]. Brasília: STF; 2020 [citado 2020 out 13]. Disponível em: https://www.stf.jus.br/portal/cms/verNoticiaDetalhe.asp?idConteudo=441447 [ Links ]
20. Silva LLS, Lima AFR, Polli DA, Razia PFS, Pavão LFA, Cavalcanti MAFH, et al. Medidas de distanciamento social para o enfrentamento da COVID-19 no Brasil: caracterização e análise epidemiológica por estado. Cad Saúde Pública [Internet]. 2020 [citado 2020 nov 12];36(9):e00185020. Disponível em: https://doi.org/10.1590/0102-311X00185020 [ Links ]
21. World Health Organization – WHO. Covid 19 Infection [Internet]. Geneva: World Health Organization; 2020 [cited 2020 Mar 31]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 [ Links ]
22. Sjödin H, Wilder-Smith A, Osman S, Farooq Z, Rocklöv J. Only strict quarantine measures can curb the coronavirus disease (COVID-19) outbreak in Italy, 2020. Euro Surveill [Internet]. 2020 Apr [cited 2020 Nov 12];25(13):2000280. Available from: https://dx.doi.org/10.2807%2F1560-7917.ES.2020.25.13.2000280 [ Links ]
23. Wilder-Smith A, Freedman DO. Isolation, quarantine, social distancing and community containment: pivotal role for old-style public health measures in the novel coronavirus (2019- nCoV) outbreak. J Travel Med [Internet]. 2020 Feb [cited 2020 Nov 12];27(2). Available from: https://doi.org/10.1093/jtm/taaa020 [ Links ]
24. Moris D, Schizas D. Lockdown during COVID-19: the Greek success. In Vivo [Internet]. 2020 Jun [cited 2020 Nov 12];34(3 suppl):1695-9. Available from: https://doi.org/10.21873/invivo.11963 [ Links ]
25. Figueiredo P. Isolamento social na cidade de São Paulo subiu em média 2 pontos percentuais com antecipação de feriados municipais. G1 [Internet]. 2020 maio [citado 2020 ago 11]. Disponível em: https://g1.globo.com/sp/sao-paulo/noticia/2020/05/25/isolamento-social-na-cidade-de-sao-paulo-subiu-em-media-2-pontos-percentuais-com-antecipacao-de-feriados-municipais.ghtml [ Links ]
26. Ganem F, Mendes FM, Oliveira SB, Porto VB, Araujo W, Nakaya H, et al. The impact of early social distancing at COVID-19 Outbreak in the largest Metropolitan Area of Brazil. medRxiv [Internet]. 2020 Apr [cited 2020 Nov 12]. Available from: https://doi.org/10.1101/2020.04.06.20055103 [ Links ]
27. Ferguson N, Laydon D, Nedjati Gilani G, Imai N, Ainslie K, et l. Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand [Internet]. United Kingdom: Imperial College COVID-19 Response Team; 2020 [cited 2020 Nov 12]. Available from: https://doi.org/10.25561/77482 [ Links ]
28. Lau H, Khosrawipour V, Kocbach P, Mikolajczyk A, Schubert J, Bania J, et al. The positive impact of lockdown in Wuhan on containing the COVID-19 outbreak in China. J Travel Med [Internet]. 2020 Mar [cited 2020 Nov 12];27(3):1-7. Available from: https://doi.org/10.1093/jtm/taaa037 [ Links ]
29. Roques L, Klein EK, Papaix J, Sar A, Soubeyrand S. Impact of lockdown on the epidemic dynamics of COVID-19 in France. Front Med [Internet]. 2020 Jun [cited 2020 Nov 12];7:274. Available from: https://dx.doi.org/10.3389%2Ffmed.2020.00274 [ Links ]
30. The Assessment Capacities Project - ACAPS. Taxonomy of government measures [Internet]. Geneva: ACAPS; 2020 [cited 2020 Aug 11]. Available from: https://www.acaps.org/sites/acaps/files/products/files/20201505_acaps_covid19_government_measures_report_update.pdf [ Links ]
Received: July 10, 2020; Accepted: October 27, 2020
 This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
