










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.1 Brasília 2021 Epub 31-Mar-2021
http://dx.doi.org/10.1590/s1679-49742021000100029
Original Article
Street people in Brazil: a descriptive study of their sociodemographic profile and tuberculosis morbidity, 2014-2019
1 Universidade Federal da Bahia, Instituto de Saúde Coletiva, Salvador, BA, Brazil
2 Universidade Federal do Vale do São Francisco, Colegiado de Medicina, Paulo Afonso, BA, Brazil
3 Universidade Estadual de Feira de Santana, Departamento de Saúde, Feira de Santana, BA, Brazil
Objective
To characterize the sociodemographic profile of street people (SP) registered on the Single Register for Social Programs (CadÚnico) as at 2019 and tuberculosis morbidity in this population notified on the Notifiable Health Conditions Information System (Sinan) from 2014 to 2018.
Results
127,536 people registered on CadÚnico and 14,059 with tuberculosis notified on Sinan were included in the study. Higher concentrations of SP were found in the states of the South and Southeast regions. In the two subpopulations analyzed, there was a predominance of male SP (CadÚnico = 86.8%; Sinan = 80.9%), people of Black race/skin color (CadÚnico = 67.5%; Sinan = 64.1%) and with incomplete high school education or less (CadÚnico = 81.9%; Sinan = 60.1%). The high treatment dropout proportion (39.0%) was reflected in the high percentage of reentry and relapse.
Conclusion
Tuberculosis continues to be a serious Public Health problem that aggravates survival conditions on the streets of Brazil.
Keywords: Homeless Persons; Social Vulnerability; Epidemiology, Descriptive; Tuberculosis
Introduction
Street people form a heterogeneous group living in extreme poverty, with fragile or broken family ties, living permanently or temporarily in unconventional dwelling conditions.1
There are many dangers on the streets for this population, such as violence, food insecurity, unavailability of clean drinking water, deprivation of sleep and affection, exposing it to a variety of diseases, health conditions and situations of vulnerability. Scarcity of information on street people is a reality in Brazil and, at the time this article was submitted for publication, they are not expected to be included in the demographic census conducted by the Brazilian Institution of Geography and Statistics.2-4
A study conducted by the Institute of Applied Economic Research, a public foundation linked to the Brazilian Ministry of the Economy, which projected estimates based on information from the Federal Government’s Single Registry for Social Programs (CadÚnico) and from the Unified Social Welfare System, allows it to be presumed that in 2020 there are 221,869 street people in Brazil, mainly in the Southeast region, although also growing considerably in Northern Brazil.5
The National Policy on Street People was brought into force by Federal Decree No. 7053, published on December 23rd 2009.6 Notwithstanding, to date fully guaranteed rights and conditions for the dignified existence and social protection of this population have not been achieved, according to political militants from the National Movement of Street Dwellers. In the field of Health, once it was admitted that there were iniquities in their access to services, the decision was taken to dismember action strategies, such as the ‘Operational plan to implement health actions for street people 2012-2015’, by the (now extinct) Ministry of Health Secretariat for Strategic and Participative Health Management, and the ‘Street Consulting Room’, a project within the National Primary Health Care Policy, coordinated nationally by the Ministry of Health Secretariat for Primary Health Care. Despite these initiatives, street people are still stricken by violence, mental illness, chronic diseases and communicable diseases, the latter including tuberculosis.7-9
Brazil is one of the 22 countries with high tuberculosis endemicity. The World Health Organization estimates that around a quarter of the global population is infected with Mycobacterium tuberculosis and that between 5% and 10% of those infected develop tuberculosis during their lives.3,10
Absence of housing and precarious living conditions are determinant factors of the occurrence of the disease among street people. According to a study conduction in Salvador, BA,11 tuberculosis appears as the third leading cause of illness in this specific group. In the state of São Paulo, a study based on data for the period 2009-2013 estimated tuberculosis magnitude, with particularly high treatment dropout percentages among street people, reaching 57.3%. Incidence of latent tuberculosis infection and active tuberculosis among street people is between 10 and 85 times greater than among the general population.12 For these reasons the National Tuberculosis Program has included street people as a priority population.13
The objective of this study, which was set on making denied human rights visible and presenting data that favor decisions being made to ensure actions provided for in intersectoral public policies, was to characterize (i) the sociodemographic profile of street people registered on CadÚnico in May 2019 and (ii) tuberculosis morbidity among this population reported on the Notifiable Health Conditions Information System (Sinan) between 2014 and 2018.
Methods
This was a descriptive study of all street people recorded on the Information Tabulator of CadÚnico (TABCAD - CadÚnico V7) as at May 2019,14 and of street people with tuberculosis notified on the Sinan (TABNET) system between 2014 and 2018.15
Data recorded on TABCAB as at 2019 were used to define the study population, given that this tabulator does not enable selection by time period. These data were accessed on May 2nd 2019.14 When choosing the population on the Sinan system, we sought to include the time interval having most notified cases. This began in 2014, when the ‘Street People’ category was included on the system, within the ‘Special Populations’ variable - these data were tabulated using TABNET on September 20th 2020.15
The following CadÚnico variables were included:
sex (male; female);
age group (in years: 0-15; 16-24; 25-44; 45-54; 55-64; 65 and over);
race/skin color (white; black; yellow; brown; indigenous; no information);
schooling (according to level of education: no schooling; incomplete elementary education; complete elementary education; incomplete high school education; complete high school education; incomplete or complete higher education; no information);
per capita family income bracket (extreme poverty; poverty; low-income; above 1/2 the minimum wage); and
being a beneficiary of the Bolsa Família Program (yes; no).14
The criterion set by the Citizenship Ministry was used to characterize per capita family income brackets: ‘extreme poverty’ being monthly income per person of up to BRL 89.00; and ‘poverty’ being monthly income per person between BRL 89.01 and BRL 178.00.16
When characterizing tuberculosis cases notified on the Sinan system, we opted to describe the sociodemographic variables equivalent to the variables obtained from the CadÚnico system, with the exception of the ‘per capita family income bracket’ variable which is not recorded on the Sinan form. Given the specificity of TABNET, we used the following age categories for the ‘age group’ variable expressed in years: 0-14; 15-24; 25-34; 35-44; 45-54; 55-64; 65 and over; no information.15 The following variables were also described: ‘entry type’ (new case; reentry; relapse; transfer; post-mortem diagnosis; unknown) and ‘treatment outcome’ (cure; dropout; death; transfer; unknown/blank) of tuberculosis cases among street people in Brasil.15 The following variables were removed when analyzing tuberculosis outcomes among street people: ‘TB-DR’, ‘regimen change’, ‘failure’ and ‘primary dropout’, as their results were below 1.1%. Deaths from other causes were also excluded, given that it was impossible to analyze secondary causes. During the data collection and analysis period, case closures for the year 2019 had not been consolidated on the Sinan system and for this reason these data were not included in the study.15
The OGis program was used to generate maps for comparative analysis of the country’s Federative Units with greater numbers of street people registered on CadÚnico and which also had the largest proportions of confirmed tuberculosis cases among street people. Analysis of street people registered on CadÚnico and on Sinan was based on the absolute number and the proportion (%) of the variables of interest using Excel software.
The study project did not need to be submitted to a Research Ethics Committee since the secondary data used were available to the public by via the information systems.
Results
We identified 127,536 street people registered on CadÚnico in May 2019. As per the map (Figure 1A) showing the distribution of street people by Federative Unit, the greater part of this population as concentrated in Minas Gerais, São Paulo, Rio de Janeiro, Paraná and Rio Grande do Sul, with more than 5,000 street people in each of them. The Federative Units with fewer than 500 street people registered were located in the Northern region: Tocantins, Amapá, Rondônia and Acre.
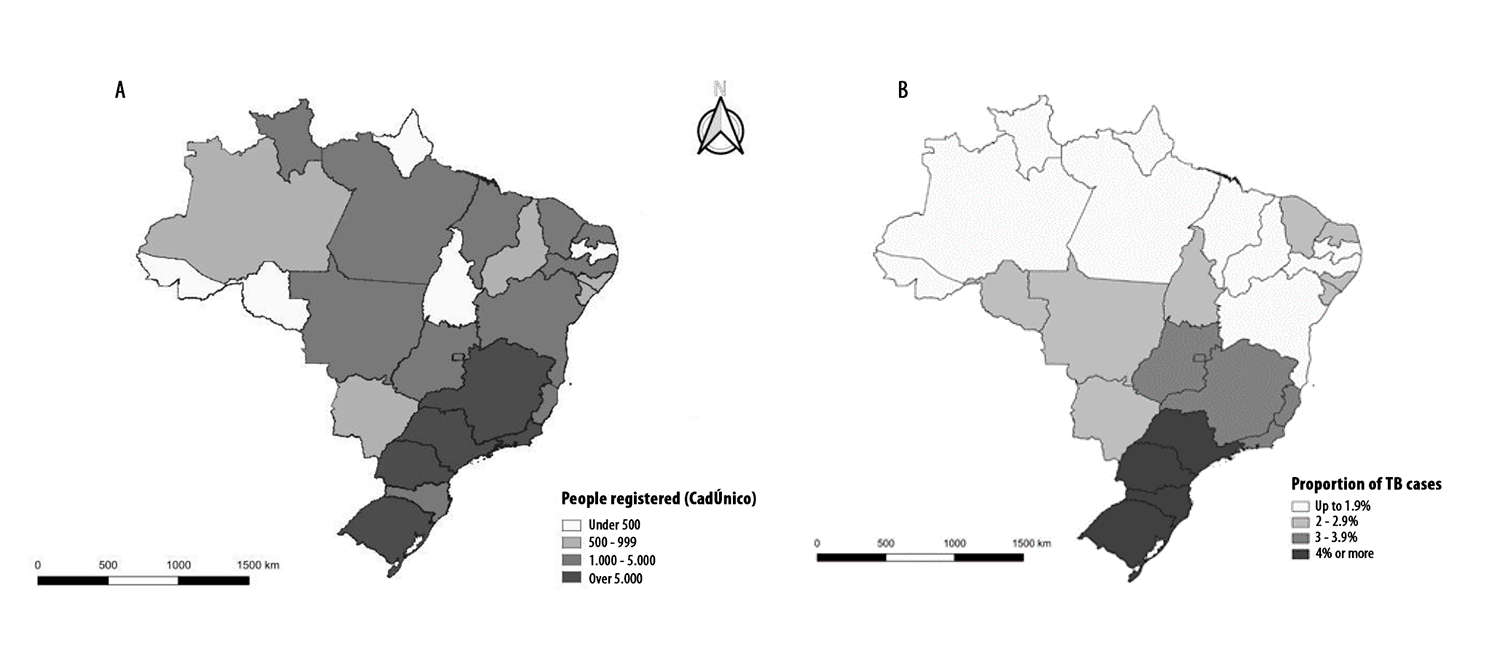
Figure 1 Number of people registered on the Single Registry for Social Programs (CadÚnico) by Federative Unit in May 2019 (A) and proportion of confirmed tuberculosis cases (TB) among street people by Federative Unit between 2014 and 2018 (B)
When analyzing the number of cases of tuberculosis among street people notified on the Sinan system, we identified 14,059 people with tuberculosis between 2014 and 2018. As can be seen in Figure 1B, more than 4% of tuberculosis cases occurred in this population in São Paulo and in the states of the Southern region. It is noteworthy that among the ten states and the Federal District, which had between 1,000 and 5,000 people registered on CadÚnico, only Goiás, Minas Gerais, Rio de Janeiro and Espírito Santo had tuberculosis case proportions of between 3% and 3.9%.
Figure 2 shows the sum total of people notified on the Sinan system according to entry types ‘reentry following dropout’, ‘relapse’, ‘transfer’, ‘post-mortem diagnosis’ as well as records with ‘no information’ on entry type: in all, 6,355 people were notified, accounting for 45.2% of cases notified between 2014 and 2018.
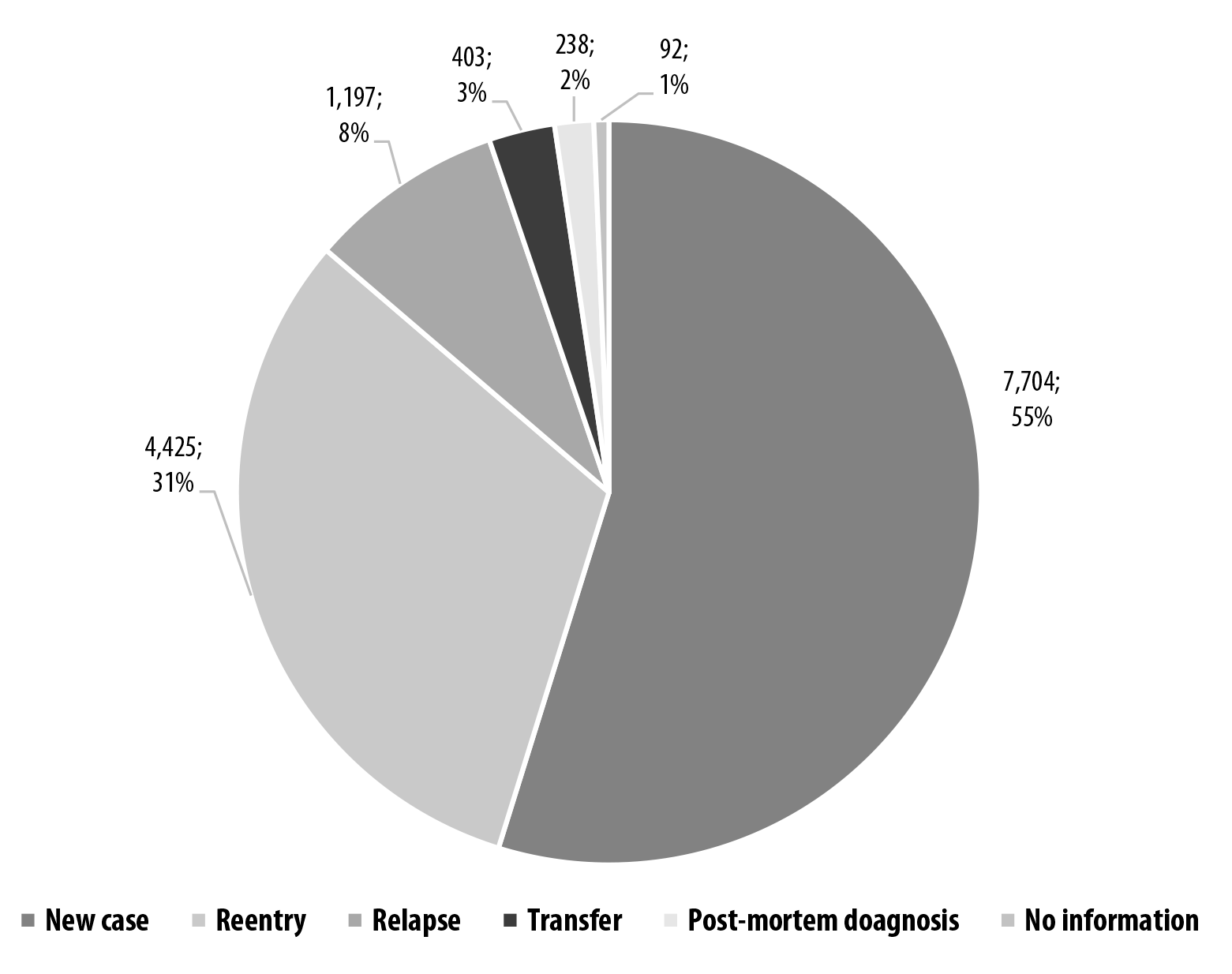
Figure 2 Number and proportion of tuberculosis cases among street people, by entry mode at notification on the Notifiable Health Conditions Information System (Sinan), Brazil, 2014-2018
Of the tuberculosis cases among street people recorded on Sinan (Table 1), 80.9% (11,377) were male and 19.1% (2,682) were female. With regard to age group, 80.7% (11,347) of cases occurred in people between 25 and 54 years old, with greater predominance among individuals in the 35-44 age group (54.2%). In relation to race/skin color, 64.1% (9,003) of cases were Black, i.e. 44.2% (6,209) self-reported their skin color as brown and 19.9% (2,794) as black.
Table 1 Sociodemographic profile of tuberculosis cases (TB) among street people, Brazil, 2014-2018
| Variables | Street people with TB (n=14,059) | |
|---|---|---|
| n | % | |
| Sex | ||
| Male | 11,377 | 80.9 |
| Female | 2,682 | 19.1 |
| Age group (in years) | ||
| ≤14 | 67 | 0.5 |
| 15-24 | 985 | 7.0 |
| 25-34 | 3,719 | 26.5 |
| 35-44 | 4,716 | 33.5 |
| 45-54 | 2,912 | 20.7 |
| 55-64 | 1,288 | 9.2 |
| ≥65 | 359 | 2.6 |
| Race/skin color | ||
| White | 3,733 | 26.5 |
| Black | 2,794 | 19.9 |
| Yellow | 84 | 0.6 |
| Brown | 6,209 | 44.2 |
| Indigenous | 62 | 0.4 |
| No information | 1,177 | 8.4 |
| Schooling | ||
| Illiterate | 715 | 5.1 |
| Incomplete elementary education | 5,881 | 41.8 |
| Complete elementary education | 588 | 4.2 |
| Incomplete high school education | 1,268 | 9.0 |
| Complete high school education | 374 | 2.7 |
| Incomplete or complete higher education | 222 | 1.6 |
| No information | 5,011 | 35.6 |
| Receives government benefit | ||
| Yes | 565 | 4.0 |
| No | 6,489 | 46.2 |
| No information | 7,005 | 49.8 |
With regard to the schooling of street people with tuberculosis notified on Sinan, 46.0% (6,469) had elementary education. In relation to being a beneficiary of government social programs, 46.2% (6,489) did not receive these benefits and only 4.0% (565) did; however, 49.8% (7,005) of street people had no information on this variable (Table 1).
As shown in Table 2, Brazilian street people registered on CadÚnico were comprised of 86.8% (110,732) males and 74.8% (95,394) of individuals in the 25-54 age group. With regard to the ‘race/skin color’ variable, 51.3% (65,454) self-reported themselves as being of brown skin color and 16.2% (20,652) as being of black skin color, totaling 67.5% (86,106) Black people.
Table 2 Sociodemographic profile of street people registered on the Single Registry for Social Programs (CadÚnico), Brazil, May 2019
| Variables | Street people (n=127,536) | |
|---|---|---|
| n | % | |
| Sex | ||
| Male | 110,732 | 86.8 |
| Female | 16,804 | 13.2 |
| Age group (in years) | ||
| ≤15 | 3,347 | 2.6 |
| 16-24 | 7,081 | 5.5 |
| 25-44 | 66,570 | 52.2 |
| 45-54 | 28,824 | 22.6 |
| 55-64 | 16,921 | 13.3 |
| ≥65 | 4,793 | 3.8 |
| Race/skin color | ||
| White | 40,457 | 31.7 |
| Black | 20,652 | 16.2 |
| Yellow | 576 | 0.5 |
| Brown | 65,454 | 51.3 |
| Indigenous | 296 | 0.2 |
| No information | 101 | 0.1 |
| Schooling | ||
| No schooling | 13,859 | 10.9 |
| Incomplete elementary education | 61,779 | 48.4 |
| Complete elementary education | 17,479 | 13.7 |
| Incomplete high school education | 11,354 | 8.9 |
| Complete high school education | 19,781 | 15.5 |
| Incomplete or complete higher education | 1,905 | 1.5 |
| No information | 1,379 | 1.1 |
| Per capita family income bracket | ||
| Extreme poverty | 115,073 | 90.2 |
| Poverty | 2,332 | 1.8 |
| Low income | 2,964 | 2.3 |
| Above 1/2 minimum wage | 7,167 | 5.7 |
| Programa Bolsa Família Beneficiary | ||
| Yes | 96,337 | 75.5 |
| No | 31,199 | 24.5 |
| No information | 7,005 | 49.8 |
The data on schooling, according to level of education, showed that 62.1% (79,258) had elementary education, divided between 48.4% (61,779) with incomplete elementary education and 13.7% (17,479) with complete elementary education. In relation to per capita family income, 90.2% (115,073) of street people fell into the extreme poverty bracket. 5.7% (7,167) had income above half the minimum wage and 75.5% (96,337) were beneficiaries of the Bolsa Família program (Table 2).
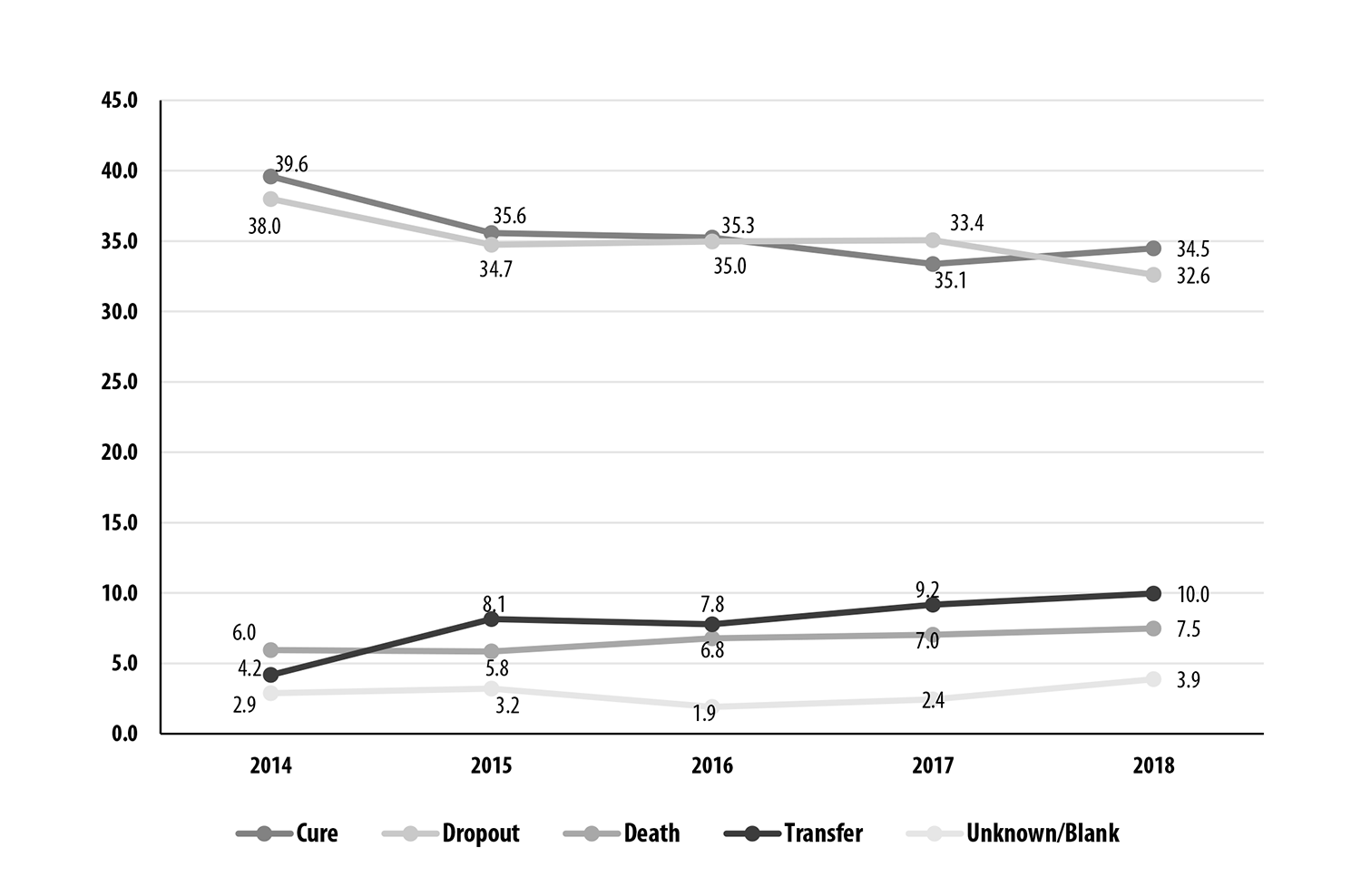
Figure 3 shows treatment outcome percentages for tuberculosis cases among street people in Brazil notified on the Sinan system. Between 2014 and 2018, even with a reduction in treatment dropout estimated at 5.5%, the proportion of individuals who were cured fell by 5.1%, from 39.6% in 2014 to 34.5% in 2018. There was an increase in the ‘unknown/blank’ and ‘transfer’ outcome percentages. Tuberculosis deaths increased over the years studied, from 5.8% to 7.5%. The final year of the period analyzed, 2018, was precisely that which had the highest percentage of deaths, i.e. 7.5% of the total of tuberculosis cases among street people in Brazil.
Discussion
This is the first study conducted in Brazil, on a national level, using sociodemographic data and data on tuberculosis among street people available on information systems. Based on the analysis of all street people registered, the results revealed a concentration of street people and tuberculosis cases among them in the states of Brazil’s Southeastern and Southern regions, in particular the state of Rio Grande do Sul.
The sociodemographic profile of tuberculosis cases among street people, predominantly among males and those of Black race/skin color (black and brown skin color), is similar to the profile of street people registered on CadÚnico. We also identified high percentages of reentry and relapse following treatment dropout, as well as high percentages of the worst outcomes, such as the increase in the proportions of tuberculosis deaths in the period studied.
Street people’s health corresponds to one of the most critical interfaces of the vulnerability of living on the streets, in a context of precarious socioeconomic conditions, difficulty in accessing health services, greater risk of infection, becoming ill and poorer clinical outcomes. Historical, political and sociocultural elements underpin antagonistic relations in Brazilian society, increasingly responsible for social dysregulation of capital, the undermining of social rights and growing health inequities.17 The actions and public policies offered to street people are not free from the influence of prejudiced opinions about people who live on the streets, whose fragility is not recognized or duly understood by society in general and which follows the dominant ideology that “living on the streets is an individual choice”.18
The states of Southeastern and Southern Brazil had the largest concentrations of street people exposed to precarious living conditions and comorbidities. An example of these conditions lies in HIV/AIDS infection, which increases risk of infection and illness due to Mycobacterium tuberculosis. According to a study conducted in Porto Alegre, RS, the percentage of street people with tuberculosis accounted for almost half the total cases in the central area of that state capital city between 2007 and 2011.19
Another study, conducted in the state of São Paulo, identified association between lack of housing and reduced survival time among people with tuberculosis, in particular the economically active age group (20-40 years old), aggravating even more their vulnerability.20 In a scenario in which the number of people surviving on the streets is increasing, due to a variety of factors, such as unemployment and migration, above all in large cities, it is important to consider whether the lower proportions of street people in the remaining states result from shortcomings in tuberculosis surveillance among this population or whether they do indeed reflect the nationwide reality.
The analysis of the Sinan system data highlights high percentages of relapse and reentry regarding tuberculosis treatment among street people. Health professionals in São Paulo City believe that there are difficulties in adhesion to long-term treatment with medication and as well as monitoring the health of people infected with M. tuberculosis, arising from absence of infrastructure, low levels of schooling, poor food intake, unemployment etc.20
Other studies also conducted in the state of São Paulo reveal that 40.5% of street people with tuberculosis dropped out of treatment in 2014, and that approximately 56% had unfavorable outcomes.21 In this study, the high dropout rate is reflected in the high percentage of treatment reentry and relapse.
The majority of tuberculosis cases in the period studied were among males, Black people (those of black and brown skin color), those with low levels of schooling and of economically active age. In the analysis of the information on street people available on CadÚnico, we found that their sociodemographic profile was similar to that of street people with tuberculosis notified on Sinan and, moreover, a per capita family income bracket characterized as extreme poverty.16 Corroborating the profile identified in this study, the 2008 street people census revealed a higher frequency of males, aged between 18 and 54, and predominance of Black race/skin color. That census also revealed a population of street people comprised of workers, with a minority depending on begging for money on the streets as their main source of income, without access to government cash transfer programs, functionally illiterate or having a paid activity.4
The analysis of the sociodemographic factors relating to street people with tuberculosis makes their race/skin color visible, and the majority of them are Black. Other studies conducted in Brazil5,22 demonstrate the relationship between race/skin color and social exclusion. Considering the diverse vulnerabilities to which capitalist society exposes the lower classes, street people in particular are subject to dramas and needs nearly always invisibilized and treated as being natural, corroborating situations already suffered by the Black population over the course of the history of Brazilian society.23
With regard to the Bolsa Família Program, the CadÚnico data indicate than one third of this population receive this benefit. In the study conducted in Salvador, about the receipt of social benefits by people with tuberculosis, it was demonstrated that individuals benefited by social programs were 14.5% more successful in treating tuberculosis infection.24 That analysis, when applied to the vulnerabilities described here, may indicate ways of improving adherence to treatment.
Considering everything that needs to be overcome in order to achieve tuberculosis diagnosis and treatment among street people, the results of this study highlight high percentages of treatment dropout and death. Such high percentages reaffirm the conclusions of studies conducted in Brazil and in European countries about living on the streets being an aggravating factor for tuberculosis treatment failure and increase in deaths.20,25-27
This study has limitations, one of which is the impossibility of calculating tuberculosis incidence among street people: there are no reliable population estimates for them by Federative Unit. Furthermore, it must be borne in mind that the ‘schooling’ and ‘government benefit’ variables on the Sinan form are underrecorded, whereas recording receipt of government benefits on CadÚnico is obligatory.
Among this study`s strong points is the possibility of comparing data on the entire population of street people registered on CadÚnico, nationally, as well as the data on notification of tuberculosis among street people in the last five years. The study also reveals high percentages of negative outcomes (dropout and death) and recurrent cases among this population.
There is a shortage of evidence to enable more in-depth discussion about the relationship between sociodemographic and economic factors and tuberculosis diagnosis, clinical progression and treatment outcome among street people, so that further research, both qualitative and quantitative, is needed to support wide-ranging discussion, greater visibility of the problem and well-informed decisions by those who manage health actions targeting this population.
It falls to the authors of this study to recommend that social welfare and health service networks be strengthened, in partnership with social movements, to meet the needs of street people. Developing social reparation actions enabling access to decent food and housing, as well as promoting citizenship, are both necessary and important.
With regard to the Brazilian National Health System, it is fundamental to eliminate the barriers existing between street people and the services provided by the System, by strengthening Primary Care as an action to increase the potential of early identification of infection and monitored treatment, having directly observed treatment as one of its strategies.13,28
Finally, data on street people available on information systems need to be of good quality, so as to favor decision making about public policies to reduce the invisibility of this population in Brazil. Raising the awareness of the health teams that perform diagnosis and fill in the forms is as essential for quality information as it is for designing effective intersectoral policies, as part of organizing a comprehensive care network for street people’s health.
The results of the study allow us to conclude that tuberculosis continues to be a serious Public Health problem, which makes survival conditions on the streets worse, acting as a marker the violation of street people’s access and right to health in Brazil.
Acknowledgements
To Felipe Nery, for preparing the maps presented in this study.
REFERENCES
1. Brasil. Política Nacional para Inclusão da Pessoa em Situação de Rua [Internet]. Brasília: Ministério do Planejamento, Orçamento e Gestão. Secretaria de Direitos Humanos; 2008. [citado 2019 fev 5]. 25 p. Disponível em: <Disponível em: http://www.mpsp.mp.br/portal/page/portal/cao_civel/acoes_afirmativas/inclusaooutros/aa_diversos/Pol.Nacional-Morad.Rua.pdf >. [ Links ]
2. Brasil. Ministério da Saúde (BR). Secretaria de Gestão Estratégica e Participativa. Departamento de Apoio à Gestão Participativa. Saúde da população em situação de rua: um direito humano. Brasília: Ministério da Saúde; 2014. [ Links ]
3. Brasil. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Boletim epidemiológico sobre população em situação de rua e violência: uma análise das notificações do Brasil de 2015 a 2017. Brasília: Ministério da Saúde ; 2019 jun (50). [ Links ]
4. Brasil. Ministério do Desenvolvimento Social e Combate à Fome (BR). Rua: aprendendo a contar. Pesquisa Nacional sobre a População em Situação de Rua. Brasília: Ministério do Desenvolvimento Social e Combate à Fome; 2009 [ Links ]
5. Natalino, MAC. Estimativa da população em situação de rua no Brasil (setembro de 2012 a março de 2020) [Nota Técnica]. Brasília: Instituto de Pesquisa Econômica Aplicada; 2020. 20 p. [ Links ]
6. Brasil. Casa Civil. Decreto Federal nº 7053, de 23 de dezembro de 2009. Institui a Política Nacional para a População em Situação de Rua e seu Comitê Intersetorial de Acompanhamento e Monitoramento, e dá outras providências. Diário Oficial da República Federativa do Brasil, Brasília (DF), 2009 dez 24; p. 16. [ Links ]
7. Barbosa, J. C. Implementação das políticas públicas voltadas para a população em situação de rua: desafios e aprendizados. Programa de Pós-Graduação em Políticas Públicas e Desenvolvimento, Instituto de Pesquisa Econômica Aplicada. Brasília, 2018. [ Links ]
8. Brasil. Ministério da Saúde (BR). Plano operativo para implementação de ações em saúde da população em situação de rua 2012-2015. Brasília: Ministério da Saúde ; 2012. [ Links ]
9. Brasil. Ministério da Saúde. Portaria nº 2436, de 21 de setembro de 2017. Aprova a Política Nacional de Atenção Básica, estabelecendo a revisão de diretrizes para a organização da Atenção Básica, no âmbito do Sistema Único de Saúde (SUS). Diário Oficial da República Federativa do Brasil , Brasília (DF), 2017. [ Links ]
10. World Health Organization (WHO). Global tuberculosis report. New York: WHO; 2020. Disponível em: <Disponível em: https://www.who.int/publications/i/item/who-consolidated-guidelines-on-tuberculosis-module-1-prevention-tuberculosis-preventive-treatment >. Acesso em: 25 de agosto de 2020. [ Links ]
11. Salvador. Prefeitura Municipal. Relatório da pesquisa sobre a população em situação de rua no município de Salvador-Ba/ Prefeitura Municipal de Salvador. 1. ed. - Salvador: Programa Salvador Cidadania, 2010. 93p. [ Links ]
12. Ranzani OT, Carvalho CR, Waldman EA, Rodrigues LC. The impact of being homeless on the unsuccessful outcome of treatment of pulmonary TB in São Paulo State, Brazil. BMC Med. 2016 mar 23; 14:41. [ Links ]
13. Brasil. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Manual de Recomendações para o Controle da Tuberculose no Brasil. Brasília: Ministério da Saúde ; 2018. [ Links ]
14. Brasil. Ministério da Cidadania (BR). Relatórios de Informações Sociais. Consulta, Seleção e Extração de informações do Cadastro Único - CECAD. Brasília: Ministério da Cidadania; 2020. Disponível em: Disponível em: https://aplicacoes.mds.gov.br/sagi/cecad20/tab_cad.php . Acesso em: 02 de maio de 2019. [ Links ]
15. Brasil. Ministério da Saúde (BR). Informações de saúde (TABNET) [Internet]. Brasília: Ministério da Saúde ; 2016. Disponível em: <Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinannet/cnv/tubercbr.de >. Acesso em 20 de setembro de 2020. [ Links ]
16. Brasil. Ministério da Cidadania (BR). Guia de Cadastramento de Pessoas em Situação de Rua. Brasília: Ministério da Cidadania ; 2020. Disponível em: Disponível em: https://www.mds.gov.br/webarquivos/arquivo/cadastro_unico/_Guia_Cadastramento_de_Pessoas_em_Situacao_de_Rua.pdf . Acesso em: 02 de setembro de 2020. [ Links ]
17. Geolin, George Francisco. Crise do capital, precarização do trabalho e impactos no Serviço Social. Serv. Soc. Soc., São Paulo, n. 118, p. 239-264, Jun 2014. [ Links ]
18. Serafino I, Luz LCX. Políticas para a população adulta em situação de rua: questões para debate. Revista Katálysis, v. 18, n. 1, p. 74-85, 2015. [ Links ]
19. Peruhype, RC et al. Distribuição da tuberculose em Porto Alegre: análise da magnitude e coinfecção tuberculose-HIV. Revista da Escola de Enfermagem da USP, v. 48, n. 6, p. 1035-1043, 2014. [ Links ]
20. Ranzani OT, Rodrigues LC, Bombarda S, Minto CM, Waldman EA, Carvalho CRR. Long-term survival and cause-specific mortality of patients newly diagnosed with tuberculosis in São Paulo state, Brazil, 2010-15: a population-based, longitudinal study. Lancet Infect Dis. 2020;20(1):123-132. doi:10.1016/S1473-3099(19)30518-3 [ Links ]
21. São Paulo (Cidade). Estratégias no enfrentamento da tuberculose na população em situação de rua na cidade de São Paulo. In: Assembleia da Rede de Comitês Tb, 7. 2015, Brasília. Anais: Brasília, 2015. Disponível em: Disponível em: https://drive.google.com/file/d/0B0CE2wqdEaR-Wm1TLTVhQ29FWWc/view . Acesso em: 26 de setembro de 2020. [ Links ]
22. Mattos RM, Ferreira RF. Quem vocês pensam que (elas) são? Representações sobre as pessoas em situação de rua. Psicol Soc. 2004;16(2):47- 58. [ Links ]
23. Silva TD, Natalino M, Pinheiro MB. População em situação de rua em tempos de pandemia: um levantamento de medidas municipais emergenciais [Nota Técnica]. Brasília: Instituto de Pesquisa Econômica Aplicada ; 2020. 26 p. [ Links ]
24. Andrade KVF, Nery JS, Araújo GS, Barreto ML, Pereira SM. Associação entre desfecho do tratamento, características sociodemográficas e benefícios sociais recebidos por indivíduos com tuberculose em Salvador, Bahia, 2014-2016. Epidemiol. Serv. Saúde. 2019; 28(2): e2018220. [ Links ]
25. Nordentoft M, Wandall-Holm N. 10 year follow up study of mortality among users of hostels for homeless people in Copenhagen. BMJ 2003; 327: 81-83. Disponível em: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC164916/pdf/el-gp81.pdf. [ Links ]
26. Beijer U, Wolf A, Fazel S. Prevalence of tuberculosis, hepatitis C virus, and HIV in homeless people: a systematic review and meta-analysis. Lancet Infect Dis 2012;12: 859-70. doi:1473-3099(12)70177-9 [ Links ]
27. Bernard C, Sougakoff W, Fournier A, Larnaudie S, Antoun F, Robert J, Brossier F, Truffot-Pernot C, Jarlier V, Veziris N. Impact of a 14-year screening programme on tuberculosis transmission among the homeless in Paris. Int J Turerc Lung Dis, 2012. 16(5):649-655. [ Links ]
28. Alecrim TFA, Mitano F, Reis AA, Roos CM, Palha PF, Protti-Zanatta ST. Experiência dos profissionais de saúde no cuidado da pessoa com tuberculose em situação de rua. Rev. esc. enferm. USP. 2016; Out 50(5): 808-815. [ Links ]
Received: July 25, 2020; Accepted: November 17, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
