










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.2 Brasília 2021 Epub 08-Abr-2021
http://dx.doi.org/10.1590/s1679-49742021000200010
ORIGINAL ARTICLE
Analysis of vaccination coverage of children under one year old in Roraima, Brazil, 2013-2017*
1Universidade Federal de Roraima, Programa de Pós-Graduação em Ciências da Saúde, Boa Vista, RR, Brazil
Objective:
To analyze vaccination coverage of children under 1 year old in the State of Roraima, Brazil, between 2013 and 2017, and show health professionals’ perception, regarding the barriers that influence the achievement of higher vaccination coverage, 2017.
Methods:
This was a descriptive study that analyzed vaccination coverage for bacillus Calmette-Guérin (BCG), rotavirus, poliomyelitis, yellow fever, pentavalent, meningococcal C conjugate and 10-valent pneumococcal, based on data from immunization information systems. The barriers identified by the professionals were measured by a questionnaire with Likert scale answer options.
Results:
BCG had the highest coverage (146.1%) in 2014; while Rotavirus had the lowest (70.4%) in 2013. Difficulty in accessing the internet was the main barrier (56/100) to better coverage identified by professionals working in the program (100 respondents).
Keywords: Vaccine Coverage; Immunization Programs; Vaccination; Health Services Accessibility; Epidemiology, Descriptive
Introduction
Vaccination is one of the safest and most effective interventions for elimination and control of communicable diseases, as well as being a determinant of reduction in morbidity and mortality, especially among children, who are particularly vulnerable.1 Immunization technology has enabled the eradication of serious diseases, such as smallpox in 1980.2
In Brazil, vaccination is a basic citizenship right. The National Immunization Program (PNI), responsible for organizing and coordinating all vaccination actions, seeks to ensure vaccination for all individuals, regardless of social class and residence location, whether in rural or urban areas.3 The PNI's mission is to control, eradicate and eliminate vaccine-preventable diseases and, therefore, the Ministry of Health has established indicators that support analysis of the program: vaccination coverage; dropout rate; and homogeneity rate.4
Vaccination coverage is comprised of the proportion of the target population that has received the complete vaccination schedule. Through this indicator, individual vulnerability and the risks of acquiring vaccine-preventable diseases are verified. The PNI’s mission will only be fulfilled when adequate vaccination coverage is achieved.5 The dropout rate expresses the acceptance of immunization by the population and, as a Program indicator, applies to vaccines with multi-dose schedules. The homogeneity rate, in turn, estimates the proportion of municipalities with adequate vaccination coverage.6
In recent decades, the PNI has incorporated new information technologies, such as the National Immunization Program Information System (SI-PNI), in addition to expanding the Brazilian vaccine schedule. Currently, the national vaccination schedule for childhood includes 14 immunobiological products - eight of them, vaccines for children under 1 year old, aimed at preventing some 12 diseases.7
The increasing complexity of the PNI has brought challenges, including (i) maintenance of high and homogeneous vaccination coverage, (ii) logistics planning for the production and distribution of immunobiological products, (iii) identification of adverse events after vaccination, (iv) constant quest for information improvement, (v) prevention of the reemergence of diseases that have already been controlled and (vi) training and updating its human resources.8 In view of this complexity, constant analyses of health services are recommended in order for them to achieve a high level of performance in immunization procedures.9.10
In Brazil, the extensive rural and indigenous area, in addition to Venezuelan migrants seeking shelter in the country, are characteristics that can influence PNI performance in the states of the Northern region,4 especially Roraima, where the great challenge is to integrate, accommodate and promote vaccination actions for the thousands of Brazilian citizens and migrants from the neighboring country, and thus keep its entire population protected from vaccine-preventable diseases, thus reducing their vulnerability.11
The difficulties experienced in professional health practice, in view of the reemergence of vaccine-preventable diseases in the state of Roraima, have motivated this study. Its objective was therefore to analyze the vaccination coverage of children under 1 year old in Roraima, between 2013 and 2017, taking into account the perceptions of health professionals and managers working in the immunization program regarding the barriers that influenced achievement of high vaccination coverage in the state in 2017.
Methods
This was a descriptive study, conducted in all 15 municipalities in the state of Roraima, between 2013 and 2017.
According to data from the Brazilian Institute of Geography and Statistics (IBGE), the estimated population of Roraima in 2017 was 522,636 inhabitants, divided into 15 municipalities.12
According to Live Birth Information System (Sinasc) data, between 2013 and 2017, 56,459 children were born alive in the state.13
Data on vaccination coverage, vaccine doses administered and information about health professionals’ and managers’ perception of Roraima immunization program were consulted.
For the analysis of vaccine coverage and vaccine doses administered, data from the Immunization Program Evaluation Information System and from the SI-PNI itself were used regarding vaccine doses administered to all children under 1 year old, born alive between 2013 and 2015.
With regard to analysis of health professionals’ perception, all professionals and managers registered as working in the immunization program between July and August, 2018 were considered eligible.
Data for analysis of vaccination coverage were obtained from the SI-PNI and from the Immunization Program Evaluation Information System. The immunobiological products chosen for the study were bacillus Calmette-Guérin vaccine (BCG), vaccines against human rotavirus, poliomyelitis and yellow fever, pentavalent (DTP/HB/Hib), meningococcal C conjugate and 10-valent pneumococcal. The research variables comprised the following PNI health indicators: vaccination coverage, homogeneity rate and dropout rate.
Vaccination coverage was calculated considering the number of doses administered of a certain vaccine as the numerator, and the estimated size of its target population as the denominator, and multiplying the result by 100. In the population group analyzed, vaccination coverage was considered adequate when it reached values equal to or higher than: 90% for BCG and human rotavirus; 95% for poliomyelitis, pentavalent, meningococcal C conjugate and 10-valent pneumococcal vaccines; and 100% for yellow fever vaccine.
The homogeneity rates were calculated considering the number of municipalities with adequate coverage for a given vaccine as the numerator, and the total number of municipalities in the state as the denominator, and multiplying the result by 100. The homogeneity rate was considered to be adequate if at least 70% of the municipalities met the recommended vaccination target.13
Dropout rates (applied to multi-dose vaccines in children younger than 1 year old) were calculated by dividing the difference between the number of first doses and the number of last doses administered in the vaccination schedule by the total of first doses, and multiplying the result by 100.The dropout rates were considered to be low (<5%), average (≥5% and <10%), and high (≥10%).14
The perception of professionals and managers working in the immunization program was measured by an instrument, which was prepared and presented to the participants in the form of a semi-structured questionnaire, based on a Likert scale, covering aspects related to weaknesses in the SI-PNI implementation process and difficulties faced by the population in adhering to the program. For the analysis of possible barriers to access to vaccine rooms, the questionnaire took as a reference the theoretical model proposed by Ferreira et al.,15 established under the array of dimensions and criteria that influence the population's access to vaccine rooms, classified as follows: organizational access; geographic access; sociocultural access; and economic access.
In order to validate the questionnaire before administering it with the population of interest, the following procedures were performed: definition of its structure, objectives and theoretical model; content validation; and finally, pre-test with ten people with the same characteristics as the target population. Participants were not obliged to answer questions they did not want to, and a space in the questionnaire was provided in order for them to add other variables they considered relevant.
Regarding weaknesses in the SI-PNI implementation process, the questionnaire covered the following variables: lack of qualified professionals; computer installations; difficulty in accessing the Internet; work overload; delay in service; and insufficient number of professionals. The professionals answered according to their perception of each of these items, rated according to four points: 1 - Not very weak; 2 - Weak; 3 - Not weak; 4 - Very weak.
With regard to professionals’ perception about difficulties faced by the population in adhering to the immunization program, the following variables were considered: difficulty accessing service/extensive rural area; vaccine hesitancy; lack of investment in the program; lack of priority given to the program; and lack of financial resources. The professionals answered according to their perception of each of these items, rated according to four points: 1 - None; 2 - Little; 3 - Neither a little, nor a lot; 4 - A lot.
The questionnaire was sent to the e-mail addresses registered with the Roraima State Department of Health for all professionals and managers registered as working in the program between the months of July and August, 2018. In the case of municipalities located up to 134km from the capital Boa Vista, a visit was made to collect data and administer the questionnaire in person.
Data on vaccination coverage, dropout rates and homogeneity rates in Roraima, collected from information systems, were tabulated and interpreted using the descriptive statistics method, and organized in the form of graphs and tables. The information collected about the professionals’ perception, taken from their answers to the questionnaire, were systematized on electronic spreadsheets, then interpreted and analyzed according to the Grounded Theory.
To identify the desirable sample size, the simple sampling method was applied, calculated - for a finite population - by the following formula:
Where:
n = sample size
N = population size
p = proportion of favorable results for the variable in the population
q = proportion of unfavorable results in the population
Zα/2̸ = critical value for desired degree of confidence
E = standard error of the proportion of cases
Thus, the value of 184 and 0.05 significance level were obtained.
The study project was approved by the Human Research Ethics Committee of the Federal University of Roraima (CEP/UFRR) in its Opinion No. 85816518.8.0000.5302, issued on April 5, 2018. Access to the immunization program information systems was authorized by the General Coordination of Health Surveillance of the State of Roraima. The professionals who answered the questionnaire signed a Free and Informed Consent Form.
Results
We were able to collect secondary data from all 15 municipalities of Roraima, regarding the seven vaccines of interest. The questionnaires were sent to 170 e-mail addresses registered on the system, and 70 replies were received. A further 60 professionals were invited to answer the questionnaire in person, and 30 of them agreed to be interviewed. Thus, of the 230 professionals invited to participate, 100 accepted.
BCG vaccination coverage was high for the entire period studied, while human rotavirus vaccine coverage targets were achieved only in 2015 (94.2%) and 2017 (90.9%). The poliomyelitis vaccine coverage target was achieved only in 2015 (106.6%), while the yellow fever vaccine did not reach the vaccine coverage target recommended by the Ministry of Health in any year of the period studied (Table 1).
The highest homogeneity rate was achieved for the 10-valent pneumococcal vaccine in 2016 (80%). On the other hand, the lowest rates of vaccination coverage homogeneity refer to the BCG vaccine throughout the period analyzed (Figure 1).
The highest dropout rates occurred with the poliomyelitis vaccine in 2013 (21.8%) and 2017 (30.2%), followed by the dropout rates for the human rotavirus vaccine in 2013 (18.6%). The lowest dropout rates recorded were for the meningococcal C conjugate vaccine (3.2%) in 2013, 10-valent pneumococcal (5.5%) in 2013 and (5.3%) in 2016, and the poliomyelitis vaccine (5.5%) in 2015; considering the period 2013-2017 as a whole, meningococcal C conjugate vaccine had the state vaccination program’s lowest dropout rate (Figure 2).
Health professionals and managers in all the municipalities of the state of Roraima were asked about their perceptions related to the specificities of the immunization program in the state. Percentage non-response, considering the predicted sample size, was 45.7%. Of the total of 100 professionals and managers who answered the questionnaire, 39 were nurses, 44 vaccinators and 17 managers whose work with immunizations was part of their daily activities. All participants of the survey, a total of 100 professionals, answered all the questions proposed.
The ratings given by the health professionals and managers of the Roraima immunization program who took part in the study were recorded with regard to the factors responsible for the vaccination situation in the state, according to their perception (Table 2). The first situation raised by the questionnaire related to SI-PNI implementation and their answers revealed the greatest weaknesses of this process in their opinion: difficulty in accessing the Internet (56%), insufficient number of professionals (54%) and work overload (48%).
Table 1 - Proportional vaccination coverage per type of vaccine in children under 1 year old and respective targets (%), Roraima, 2013-2017
| Vaccine | 2013 | 2014 | 2015 | 2016 | 2017 | Coverage target |
|---|---|---|---|---|---|---|
| Bacillus Calmette-Guérin | 126.6 | 146.1 | 112.7 | 107.3 | 113.6 | 90.0 |
| Human Rotavirus | 70.4 | 82.4 | 94.2 | 87.8 | 90.9 | 90.0 |
| 10-valent pneumococcal | 80.3 | 80.7 | 89.7 | 101.7 | 97.9 | 95.0 |
| Meningococcal C conjugate | 81.5 | 81.1 | 95.6 | 99.1 | 89.5 | 95.0 |
| Pentavalent | 80.4 | 79.6 | 96.5 | 92.4 | 92.6 | 95.0 |
| Poliomyelitis | 84.3 | 84.7 | 106.6 | 89.2 | 88.9 | 95.0 |
| Yellow fever | 79.8 | 82.8 | 92.3 | 89.1 | 95.2 | 100.0 |
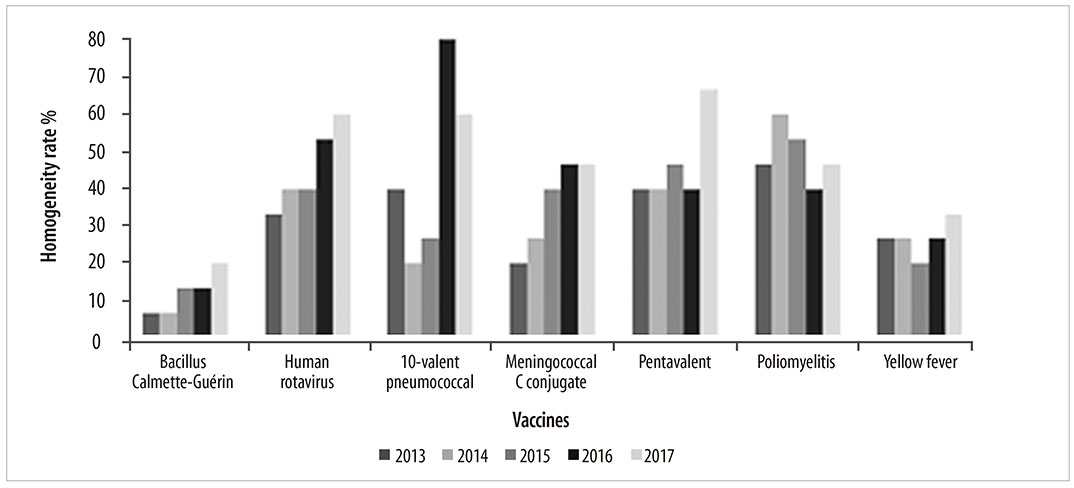
Note: the line indicates the 70% homogeneity rate.
Figure 1 - Vaccine coverage homogeneity rate, by type of vaccine, Roraima, 2013-2017
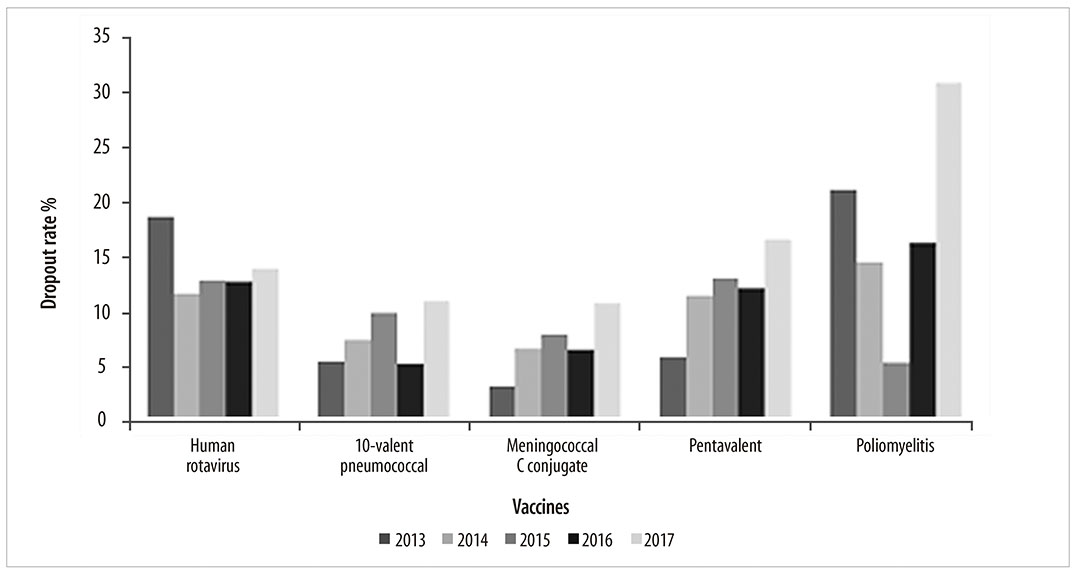
Table 2 - Frequency (%) of Health professionals’ and managers’ perception (N=100) regarding barriers to achieving high vaccination coverage, Roraima, 2017
| Weakness in the SI-PNIa implementation process | Not very weak | Weak | Not weak | Very weak |
|---|---|---|---|---|
| Lack of qualified professionals | 25.0 | 40.0 | 10.0 | 25.0 |
| Computers and their installation | 19.0 | 24.0 | 24.0 | 33.0 |
| Difficulty accessing the internet | 12.0 | 23.0 | 9.0 | 56.0 |
| Work overload | 15.0 | 26.0 | 11.0 | 48.0 |
| Delay in service | 28.0 | 22.0 | 10.0 | 40.0 |
| Insufficient number of professionals | 17.0 | 19.0 | 10.0 | 54.0 |
| Difficulty in the process for adhering to the immunization program | None | Little | Neither a lot, nor a little | A lot |
| Difficulty accessing service/extensive rural area | 16.0 | 37.0 | 25.0 | 22.0 |
| Vaccine hesitancy | 8.0 | 50.0 | 22.0 | 20.0 |
| Lack of investment in the program | 15.0 | 26.0 | 27.0 | 32.0 |
| Lack of priority for the program | 18.0 | 24.0 | 24.0 | 34.0 |
| Lack of financial resources | 18.0 | 26.0 | 24.0 | 32.0 |
a) SI-PNI: National Immunization Program Information System.
The ratings indicated for the factors responsible for population’s difficulty in adhering to the immunization program were similar between the variables (Table 2), although each of them stood out because of the diversity of opinions: for example, 'lack of investment in the program' was perceived as a very strong influence for 32% of participants and of no importance (none) for 15% of participants.
The variable presented as hindering adherence to the immunization program about which the participants’ opinions differed most - ranging from those who perceived its influence to be more intense to those for whom it was less intense - was 'vaccine hesitancy': while 50% of the participants considered it to have little influence, for 22% it had strong influence, while for 8% this variable had no influence on adherence to the vaccination program (Table 2).
Discussion
In general the results of this study indicated vaccination coverage below the targets established by the Ministry of Health. However, some vaccination coverage was far above these targets; while others oscillated to the point of having excellent vaccination coverage one year and a drastic proportional drop the next.
A limitation of this study is inherent to the use of secondary data, subject to possible typing errors, data incompleteness or input pending on immunization information systems - that is, the possibility exists of further data having been input after this study was concluded.
Only one out of every 2.3 questionnaires sent to professionals registered as working in the immunization program was answered. Considering the high turnover of health managers/professionals and the hiring of new vaccinators, it is possible that the electronic addresses registered on the systems were not up to date. Despite the possibility that the low proportion of response influenced the study's ability to represent the target population, the results of this study corroborate those of the national and international literature: barriers to accessing services strongly influence the population’s adherence to disease prevention programs.16 However, if vaccine hesitancy is one of the factors responsible for the drop in vaccination coverage in Brazil, it has low influence on the population’s adherence to the program in Roraima.17
BCG vaccination coverage in the state of Roraima remained high, achieving more than 100% throughout the period studied. This finding is contrary to those for states such as Pará, Maranhão and Bahia, where there was a decrease in the number of people who received this immunobiological. The heterogeneity of vaccination coverage in Brazilian states can be explained by births outside the mother's place of residence.18 In this sense, it is possible that the estimate of the population of children living in Roraima is underestimated, due to the high number of migrants and their possible impact on this study’s findings about vaccination coverage.
In 2015, poliomyelitis vaccine coverage was high. In the following year, on the contrary, it was well below target. Such oscillations may reflect errors in records, lack of data input due to logistical difficulties and even population underestimation or undercounting.19 Nevertheless, the existence of countries where the disease is endemic, such as Afghanistan, Pakistan and Nigeria,20 indicates that the low vaccination coverage observed represents a risk of reemergence of poliomyelitis in Brazil. Therefore, efforts should be made to achieve vaccination targets in the coming years.
In this study, there was a considerable increase in dropout rates for vaccination against poliomyelitis and human rotavirus. The greater the vaccination program credibility, the greater vaccine coverage will tend to be and therefore the dropout rate will decrease.21 The population's access to the vaccination service also interferes with dropout rates, such as geographical barriers - e.g. the extensive rural and indigenous areas - and organizational barriers, both of which are recognized as hindering conditions for the implementation of the new information system, given the difficulty of accessing the Internet in some locations and also in some regions of the country.22
Although vaccine hesitancy does not appear as one of the major causes of non-vaccination in Roraima, this factor is considered to be one of the main causes of the drop in vaccination coverage in Brazil as a whole. This is also a common finding in regions where access to vaccines is guaranteed. This is the case in Europe, where there are no barriers to vaccination related to infrastructure, but rather sociocultural barriers, such as questioning religious or philosophical beliefs or even beliefs contrary to vaccination.23
Lack of supply of immunobiological products, attributed to difficulties with international vaccine delivery and laboratory production capacity, may be responsible for the drop in vaccination coverage in Brazil.23 Despite these problems, in Roraima, there was no association between lack of immunobiological products and the drop in vaccination coverage in the state.
Analyzing vaccination coverage enables the performance of the Roraima immunization program to be verified, as well as gaining knowledge about groups susceptible to acquiring vaccine-preventable diseases. The results of this study showed heterogeneity in vaccination coverage between Roraima’s municipalities, and high dropout rates, especially for vaccination against human rotavirus and poliomyelitis. It was also made evident that barriers to access to vaccination influence the achievement of high vaccination coverage.
REFERENCES
1. Méndez MCR, Barros AJD, Wong KLM, Johnson HL, Pariyo G, Wehrmeister FC, et al. Missed opportunities in full immunization coverage: findings from low- and lower-middle-income countries. Global Health Action [Internet]. 2016 May [cited 2020 Dec 29];9(1):30963. Available from: https://doi.org/10.3402/gha.v9.30963 [ Links ]
2. Hochman G. Vacinação, varíola e uma cultura da imunização no Brasil. Ciênc Saúde Coletiva [Internet]. 2011 fev [citado 2020 dez 29];16(2):375-86. Disponível em: https://doi.org/10.1590/S1413-81232011000200002 [ Links ]
3. Domingues CMAS, Woycicki JR, Rezende KS, Henriques CMP. Programa Nacional de Imunização: a política de introdução de novas vacinas. Rev Eletr Gestão Saúde [Internet]. 2015 out [citado 2020 dez 29];6(supl 4):3250-74. Disponível em: Disponível em: https://periodicos.unb.br/index.php/rgs/article/view/3331 [ Links ]
4. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância Epidemiológica. Programa Nacional de Imunizações (PNI): 40 anos [Internet]. Brasília: Ministério da Saúde; 2013 [citado 2020 dez 29]. 236 p. Disponível em: Disponível em: https://bvsms.saude.gov.br/bvs/publicacoes/programa_nacional_imunizacoes_pni40.pdf [ Links ]
5. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das doenças transmissíveis. Manual de normas e procedimentos para vacinação [Internet]. Brasília: Ministério da Saúde ; 2014 [citado 2020 dez 29]. 176 p. Disponível em: Disponível em: http://bvsms.saude.gov.br/bvs/publicacoes/manual_procedimentos_vacinacao.pdf [ Links ]
6. Silva ABS, Araújo ACM, Santos MCS, Andrade MS, Mendonça RM. Indicadores de Cobertura Vacinal para classificação de risco de doenças imunopreveníveis. Rev Bras Promoç Saúde [Internet], 2019 ago; 32(1):1-11. Disponível em: https://periodicos.unifor.br/RBPS/article/view/9285 [ Links ]
7. Domingues CMAS, Teixeira AMS. Coberturas vacinais e doença imunopreveníveis no Brasil no período 1982-2012: avanços e desafios do programa nacional de imunizações. Epidemiol Serv Saúde [Internet]. 2013 jan-mar [citado 2020 dez 29];22(1):9-27. Disponível em: Disponível em: http://dx.doi.org/10.5123/S1679-49742013000100002 [ Links ]
8. Sato APS. National Immunization Program: computerized system as a tool for new challenges. Rev Saúde Pública [Internet]. 2015 Jul [cited 2020 Dec 29];49:39:1-5. Available from: Available from: https://doi.org/10.1590/S0034-8910.2015049005925 [ Links ]
9. Kagoné M, Yé M, Nébié E, Sie A, Schoeps A, Becher H, et al. Vaccination coverage and factors associated with adherence to the vaccination schedule in young children of a rural area in Burkina Faso. Global Health Action [Internet]. 2017 Nov [cited 2020 Dec 29];10(1):1399749. Available from: Available from: https://doi.org/10.1080/16549716.2017.1399749 [ Links ]
10. Tanaka OY, Tamaki EM. O papel da avaliação nos serviços de saúde para tomada de decisão. Ciênc Saúde Coletiva [Internet]. 2012 [citado 2020 dez 29];17(4):821-8. Available from: Available from: https://doi.org/10.1590/S1413-81232012000400002 [ Links ]
11. Barbosa LA, Sales AFG, Souza ILL. Reflexos da imigração venezuelana na assistência em saúde no maior hospital de Roraima: análise qualitativa. Saúde Soc [Internet]. 2020 jun [citado 2020 dez 29];29(2):1-11. Disponível em: Disponível em: http://dx.doi.org/10.1590/s0104-12902020190730 [ Links ]
12. Instituto Brasileiro de Geografia e Estatística - IBGE. População residente estimativas para o TCU Roraima, 2017 [Internet]. Rio de Janeiro: IBGE; 2017 [citado 2020 dez 29]. Disponível em: Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?ibge/cnv/poptrr.def [ Links ]
13. Ministério da Saúde (BR). Nascidos Vivos - Roraima, 2013 - 2017 [Internet]. Brasília: Ministério da Saúde ; 2017 [citado 2020 dez 29]. Disponível em: Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sinasc/cnv/nvrr.def [ Links ]
14. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Coberturas vacinais no Brasil: período: 2010 - 2014 [Internet]. Brasília: Ministério da Saúde ; 2015 [citado 2020 dez 29]. Disponível em: Disponível em: https://antigo.saude.gov.br/images/pdf/2017/agosto/17/AACOBERTURAS-VACINAIS-NO-BRASIL---2010-2014.pdf [ Links ]
15. Ferreira AV, Oliveira CF, Guimarães EAA, Cavalcante RB, Moraes JT, Oliveira VC. Acesso às salas de vacina na Atenção Primária à Saúde. Rev Eletr Enf [Internet]. 2017 ago [citado 2020 dez 29];19(1):1-11. Disponível em: Disponível em: https://doi.org/10.5216/ree.v19.42468 [ Links ]
16. Figueiredo A, Johnston LG, Smith DMD, Agarval S, Larson H, Jones NS. Forecasted trends in vaccination coverage and correlations with socioeconomic factors: a global time-series analysis over 30 years. Lancet Glob Health [Internet]. 2016 Oct [cited 2020 Dec 29];4(10):726-35. Available from: Available from: https://doi.org/10.1016/S2214-109X(16)30167-X [ Links ]
17. Duarte DC, Oliveira VC, Guimarães EAA, Viegas SMF. Vaccination access in Primary Care from the user's perspective: senses and feelings about healthcare services. Escola Anna Nery [Internet]. 2018 Dec [cited 2020 Dec 29];23(1):1-8. Available from: Available from: https://doi.org/10.1590/2177-9465-ean-2018-0250 [ Links ]
18. Arroyo LH, Ramos ACV, Yamamura M, Weiller TH, Crispim JA, Ramos DC, et al. Áreas com queda da cobertura vacinal para BCG, poliomielite e tríplice viral no Brasil (2006-2016): mapas da heterogeneidade regional. Cad Saúde Pública [Internet]. 2020 [citado 2020 dez 29];36(4). Disponível em: Disponível em: https://doi.org/10.1590/0102-311X00015619 [ Links ]
19. Teixeira AMS, Rocha CMV. Vigilância das coberturas de vacinação: uma metodologia para detecção e intervenção em situações de risco. Epidemiol Serv Saúde [Internet]. 2010 jul-set [citado 2020 dez 29];19(3):217-26. Disponível em: Disponível em: http://dx.doi.org/10.5123/S1679-49742010000300004 [ Links ]
20. Ministério da Saúde (BR). Informe técnico: campanha nacional de vacinação contra a Poliomielite e contra o Sarampo [Internet]. Brasília: Ministério da Saúde ; 2018 [citado 2020 dez 29]. Disponível em: https://www.cevs.rs.gov.br/upload/arquivos/201807/31163732-informe-tecnico-campanha-nacional-de-vacinacao-contra-a-poliomielite-e-o-sarampo-2018.pdf [ Links ]
21. Braz MR, Domingues CMAS, Teixeira AMS, Luna EJA. Classificação de risco de transmissão de doenças imunopreveníveis a partir de indicadores de coberturas vacinais nos municípios brasileiros. Epidemiol Serv Saúde [Internet]. 2016 out-dez [citado 2020 dez 29];25(4):745-54. Disponível em: Disponível em: https://doi.org/10.5123/s1679-49742016000400008 [ Links ]
22. Silva BS, Coelho HV, Cavalcante RB, Oliveira VC, Guimarães EAA. Evaluation study of the National Immunization Program Information System. Rev Bras Enfermagem [Internet]. 2018 Nov [cited 2020 Dec 29];71(1):615-24. Available from: Available from: http://dx.doi.org/10.1590/0034-7167-2017-0601 [ Links ]
23. Sato APS. What is the importance of vaccine hesitancy in the drop of vaccination coverage in Brazil? Rev Saúde Pública [Internet]. 2018 Nov [cited 2020 Dec 29];52(1):1-9. Available from: Available from: https://doi.org/10.11606/s1518-8787.2018052001199 [ Links ]
*Article derived from the Master's degree dissertation entitled 'Situational analysis of the immunization program in the state of Roraima: compliance with the basic vaccination schedule between 2013 and 2017', submitted by Keila Rodrigues da Fonseca to the Health Sciences Postgraduate Program of the Federal University of Roraima in 2019.
Received: April 24, 2020; Accepted: November 09, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
