










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.3 Brasília set. 2021 Epub 11-Ago-2021
http://dx.doi.org/10.1590/s1679-49742021000300024
Original Article
Socio-demographic and clinical factors of leprosy cases associated with the performance of the evaluation of their contacts in Ceará, Brazil, 2008-201910
1Universidade Federal do Ceará, Programa de Pós-Graduação em Saúde Pública, Fortaleza, CE, Brazil
2Universidade Federal da Bahia, Núcleo Epidemiologia e Saúde Coletiva, Vitória da Conquista, BA, Brazil
3Universidade Federal do Rio de Janeiro, Faculdade de Medicina, Rio de Janeiro, RJ, Brazil
4Secretaria da Saúde do Estado do Ceará, Fortaleza, CE, Brazil
5Universidade Federal do Ceará, Departamento de Saúde Comunitária, Fortaleza, CE, Brazil
Objective
To analyze the effect of sociodemographic and clinical characteristics of new leprosy cases as determinants in the performance of the evaluation of their contacts
Methods
This was a cross-sectional study, with a temporal approach to the evaluation indicator of 100% of contacts examined of each new case (NC) registered in the state of Ceará, Brazil, on the Notifiable Diseases Information System (SINAN), in 2008-2019. Logistic regression was used to estimate odds ratio (OR) with 95% confidence intervals (95%CI). The temporal trends were analyzed using joinpoint regression.
Results
23,675 NCs, 65.4% with contacts examined were analyzed. It was less likely to evaluate 100% of the registered contacts when the new cases were multibacillary (OR=1.19 - 95%CI 1.11;1.28) and with examination of contacts as an entry mode (OR=1.71 - 95%CI 1.35;2.18). There was an increasing temporal trend of the indicator (Annual Percentage Change: 2.1 - 95%CI 1.2;3.0).
Conclusion
Distinct dimensions of individual and social vulnerability among new leprosy cases influenced the persistent unsatisfactory performance of the evaluation of contacts.
Keywords: Leprosy; Epidemiology; Surveillance; Contact tracing
Introduction
Living in close contact with leprosy patients without polychemotherapeutic treatment is the main factor associated with higher transmission of Mycobacterium leprae (M. leprae), or Hansen’s bacillus.1,2 Leprosy is a chronic infectious disease, primarily neural. The development of physical disability is considered the central element to understand its physical, social and mental impact, in addition to social stigma, which also represents an important aspect.3 This disease is strongly associated with contexts of high individual, social and programmatic vulnerability.4,5
202,185 new cases were recorded, worldwide, in 2019 (2.74 cases per 100,000 inhabitants) in contexts of increased poverty. In the same year, Brazil reported 27,863 new cases, which corresponds to 13.8% of cases worldwide and 93.1% in the Americas.6 Among the people affected and who had the degree of physical disability (DPD) evaluated, 8.4% (2,351 people) were diagnosed with the maximum degree (2), a condition that limits or even prevents the performance of activities of daily living, including work and social life.7
Based on the recommendations of the World Health Organization (WHO), the Brazilian Ministry of Health has established, as one of the main strategies to reduce the burden of the disease, the development of surveillance of contacts of leprosy cases. Basically, the Ministry of Health recommends that soon after the diagnosis of a new case, the patient’s contacts should undergo a dermato-neurological examination.3,8 Since 2016, the country has extended the scope of contact definition of new leprosy cases, going beyond those of home environment, i.e.: people who live or have resided with the person with leprosy up to five years before treatment.2 Based on this definition, people who take part of the household social network such as, neighbors, colleagues and school friends, were included because they have prolonged close contact with new leprosy cases,2,9,10 in line with the evidence that has been established so far.1
Despite their relevance, these surveillance actions have presented important operational failures, either in coverage (population and individual), or in the quality of actions, related to dermato-neurological examination, immune-prophylaxis and contact tracing, over at least five years, under the responsibility of Primary Health Care (PHC).2,3,11
For the monitoring of these actions, at the municipal level, the Ministry of Health recommends the use of the indicator related to the proportion of contacts examined among the registered cases.2,10 Although relevant regarding the surveillance, this indicator presents limitations related to the monitoring of all dimensions of this process.11 The proportion of contacts examined in Brazil ranged from 74.5% to 81.4% between 2014 and 2019. According to data from the Leprosy Epidemiological Record 2020, the Northeast and North regions of the country presented the lowest coverage of contact evaluation, 79.6% and 78.6% respectively.10
With the publication of the ‘National Leprosy Control Program 2019-2022’, the Ministry of Health has reinforced the importance of the health information and surveillance system for monitoring and evaluating leprosy control, emphasizing household contact surveillance.3,8 The document represents an advance, as it breaks the cycle under the perspective of priority municipalities and begins to recommend differentiated strategies for each location, depending on epidemiological and operational patterns of control, aiming at achieving greater effectiveness of actions in the municipalities.3
The state of Ceará ratified the national recommendations and has established actions according to its reality, in its ‘Integrated Plan of strategic actions to eliminate Leprosy in Ceará, 2019-2022’.12
Taking into consideration the previous perspectives, given the need to improve leprosy contact surveillance as a strategic action for disease control, the objective of this study was to analyze the effect of sociodemographic and clinical characteristics of new leprosy cases as determining and potential factors for differential patterns in the performance of the evaluation of their contacts.
Methods
This was a cross-sectional, population-based study according to the analysis of an indicator related to the surveillance of contacts of new leprosy cases living in the state of Ceará, Brazil, from 2008 to 2019. Sociodemographic and clinical factors related to new cases, potentially associated with the performance of this indicator, were analyzed.
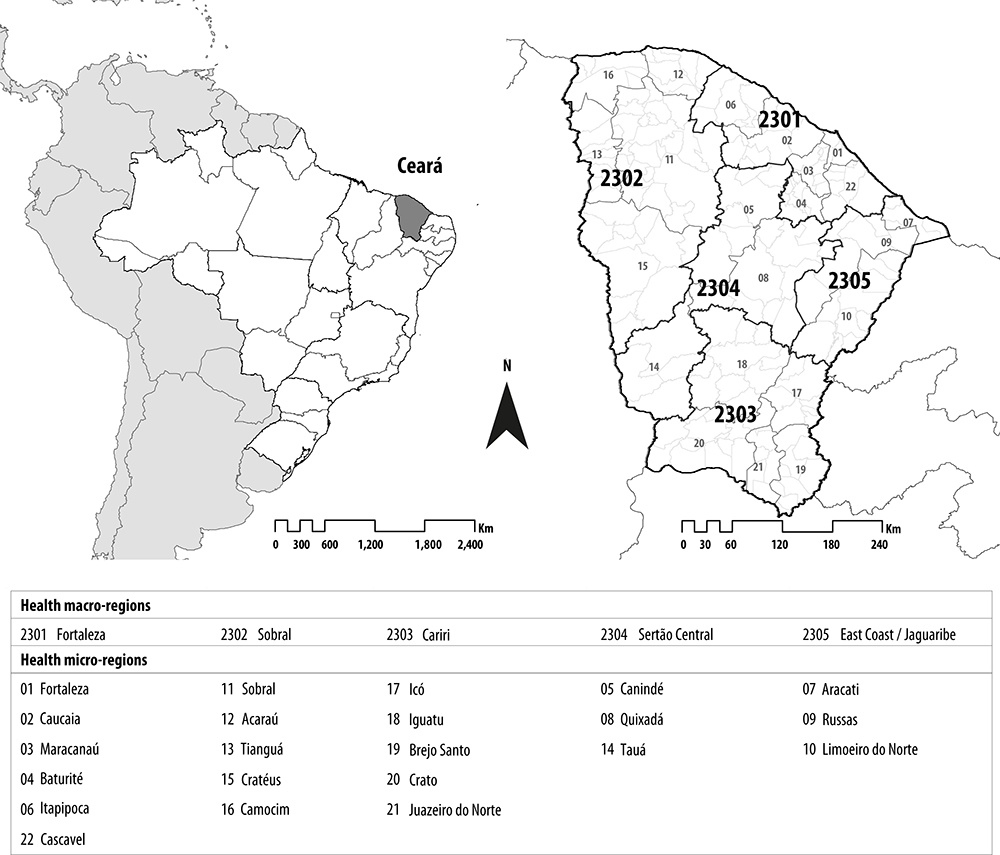
Located in the Northeast region of Brazil, Ceará is divided into 184 municipalities, distributed among five health macro-regions and 22 micro-regions (Figure 1). The population was estimated at 9,132,078 inhabitants in 2019, of which a significant part lived in the rural area (24.9%). Of the state’s total population, 48.7% were male and 4.7% self-reported black race/skin color; in the ‘social inequality’ item, 14.7% were extremely poor, and the illiteracy rate was 28.5% among those aged 18 years or older. Life expectancy at birth in the state was 72.6 years old, and the proportion of elderly people (over 65 years old) was 7.54% of the general population. In 2010, the human development index (HDI) in Ceará was 0.682; and the Gini index, 0.61.13-15
Data were retrieved from the Notifiable Diseases Information System (SINAN), obtained from the Health Surveillance Coordination for the Epidemiological Surveillance Center of the Health Department of the State of Ceará. After excluding the records with exit criteria for diagnostic error, database analysis was performed, considering the variables regarding the fields of contacts examined and registered contacts. The following classification was preliminarily established: (i) new cases with zero registered contact; (ii) new cases with 100% contacts registered and examined; (iii) new cases with a lower number of contacts examined than registered contacts; and (iv) new cases with a higher number of contacts examined than registered contacts. From the proportions generated for each of these categories, its variation was verified over a twelve-year period, in Ceará.
Following this, we started the construction of the indicator related to the proportion of new leprosy cases that had all their contacts (100%) registered, among the cases examined. Therefore, all new cases that had the number of registered contacts lower than or equal to the number of contacts examined, as well as all new cases that had no contact registered (zero: 0) were considered as ‘yes’; and as ‘no’, all those new cases whose number of registered contacts was higher than the number of contacts examined.
The analysis of sociodemographic variables of new leprosy cases included:
- gender (female; male);
- self-reported skin race/color (white; black; Asian; brown; indigenous);
- age group (in years: <15; 15-59; ≥60);
- schooling (no education; elementary school;
- high school; higher education); and
- place of residence (urban; rural; peri-urban).
Among the clinical variables, we considered: operational classification of the disease (paucibacillary case; multibacillary case); the highest degree of physical disability (0; 1; 2); and mode of detection of new cases (referral; spontaneous demand; collective examination; examination of contacts) as an operational variable.
Binary logistic regression analysis was used in order to verify the potential association between independent, sociodemographic and clinical variables of new leprosy cases with the outcome of interest related to the performance of the evaluation of their contacts examined among those registered (100% of contacts examined).
Univariate logistic regression analysis was used to identify the associated factors. The odds ratio (OR) was calculated for each independent variable, with their respective 95% confidence intervals (95%CI). The variables analyzed that were associated with p-value lower than 0.20 in the univariate regression analysis were included in the logistic regression analysis model, using the stepwise method for this selection. The objective of this stage was to investigate the independent effect of these variables, when together, for the non-evaluation of all contacts of new leprosy cases. Variance inflation factor was used to detect the presence of collinearity among the explanatory variables of the model. Variables with evidence of collinearity were excluded from the analysis.
The significance level for inclusion of variables in the final model was 5%, used for all categories of the response variable, evaluating interaction and confusion questions. Crude and adjusted OR estimates and respective 95%CI were performed, and only variables with statistical significance (p-value<0.05) remained in the model.
Poisson regression model by inflection points (Joinpoint) was used to recognize the temporal trend of the contact evaluation indicator, and its possible variation from sociodemographic and clinical characteristics of new leprosy cases. The software Joinpoint Regression Program, version 4.5.0.1 (http://surveillance.cancer.gov/joinpoint/) was used because it provides a line of best fit to a series of data points on logarithmic scale, from the annual trend tests.
For the significance test, the Monte Carlo permutation method was used to search for adjustments based on the best line of each segment. For this, the annual percentage changes (APC) were tested, with respective 95%CI. The result of model inflections defined by the program itself, as a criterion for analysis, allowed a better representation of the temporal trend.
The results obtained demonstrated (i) temporal trend of growth, when the APC values were positive and presented statistical significance (p-value<0.05), (ii) a reduction, when the APC values were negative and with statistical significance, or (iii) the absence of tendency, when the APC value was equal to zero or did not present statistical significance.
Statistical analyses were performed using Stata software, version 11.2 (Stata Statistical Software: Release 11. College Station, TX: StataCorp LP).
This study was based on secondary morbidity data of open access, thus there was no need to submit the project to the evaluation of the Research Ethics Committee (REC).
Results
During the study period, 23,675 new cases of leprosy were reported, of which 65.4% (15,484) had 100% of their registered contacts examined. 25.8% of the new cases had more registered contacts than contacts examined; 3.8% had neither registered contacts, nor contacts examined (Figure 2).
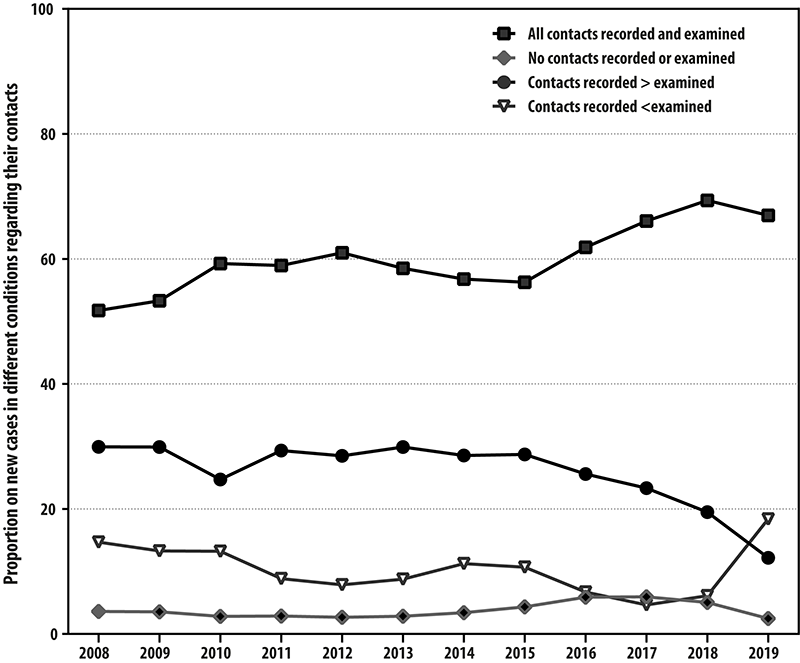
Figure 2 Analysis of consistency and completeness of variables regarding registered contacts related to contacts examined of new leprosy cases, Ceará state, Brazil, 2008-2019
According to the logistic regression analysis, when the leprosy case was male, there was an 18% higher chance (crude OR=1.18 - 95%CI 1.12;1.24) that not all his registered contacts were examined, when compared to leprosy case in females. In the adjusted analysis, there was a higher chance of not evaluating all registered contacts when the new cases were of brown (OR=1.28 - 95%CI 1.18;1.39) or black race/skin color (OR=1.37 - 95%CI 1.19;1.57), when compared to white race/skin color. The age group did not seem to be associated with the non-evaluation of 100% of the contacts, when the leprosy patient was 60 years of age or older. However, there was a factor of ‘protection’ when the patient had a higher education level, that is, having elementary school was associated with an 87% higher probability (OR=0.87 - 95%CI 0.81;0.94) that all contacts were examined, when compared to the same probability for a new case without education. When the new case of leprosy lived in the rural area, there was a 52% higher chance of not having all his or her registered contacts examined. Similarly, having been a new multibacillary case (OR=1.19 - 95%CI 1.11;1.28) and having as an entry mode, the examination of the contacts (OR=1.71 - 95%CI 1.35;2.18) was less likely to have 100% of contacts examined (Table 1).
Table 1 Multivariate analysis of the proportion of new leprosy cases with 100% of contacts examined among those registered in years of the cohort, according to sociodemographic and clinical variables of these new cases, state of Ceará, Brazil, 2008-2019
| Variables | New cases | New cases with 100% of contacts examined | Crude ORa (95%IC)b | Adjusted ORa (95%IC)b | |
|---|---|---|---|---|---|
| Yes (%) | No (%) | ||||
| Total | 23,675 (100.0) | 15,484 (65.4) | 8,191 (34.6) | - | - |
| Sex | |||||
| Female | 10,324 (43.6) | 6,535 (42.2) | 3.789 (46.3) | 1.00 | - |
| Male | 13,348 (56.4) | 8,949 (57.8) | 4.399 (53.7) | 1.18 (1.12;1.24) | - |
| Race/skin color | |||||
| White | 4,414 (18.6) | 2,864 (18.5) | 1,550 (18.9) | 1.00 | |
| Black | 1,767 (7.5) | 1,280 (8.3) | 487 (5.9) | 1.42 (1.26;1.61) | 1.37 (1.19;1.57) |
| Asian | 250 (1.1) | 165 (1.1) | 85 (1.0) | 1.05 (0.80;1.37) | - |
| Brown | 13,643 (57,6) | 9,677 (62.5) | 3,966 (48.4) | 1.32 (1.23;1.42) | 1.28 (1.18;1.39) |
| Indigenous | 67 (0,3) | 46 (0,3) | 21 (0,3) | 1,19 (0,70;1,99) | - |
| Age group (in years) | |||||
| <15 | 1,309 (5.5) | 748 (4.8) | 561 (6.8) | 1.00 | - |
| 15-59 | 15,698 (66.3) | 10,134 (65.4) | 5,564 (67.9) | 1.30 (1.19;1.42) | - |
| ≥60 | 6,668 (28.2) | 4.602 (29.7) | 2,066 (25.2) | 1.57 (1.42;1.74) | - |
| Schooling | |||||
| Illiterate | 2,680 (17.1) | 2,062 (13.3) | 618 (7.5) | 1.00 | |
| Elementary school | 9,785 (62.3) | 6,825 (44.1) | 2,960 (36.1) | 0.69 (0.63;0.76) | 0.87 (0.81;0.94) |
| High school. | 2,710 (17.3) | 1,842 (11.9) | 868 (10.6) | 0.64 (0.56;0.72) | - |
| Higher education | 525 (3.3) | 344 (2.2) | 181 (2.2) | 0.57 (0.47;0.70) | - |
| Place of residence | |||||
| Urban | 18,190 (76.8) | 11,442 (73.9) | 6,748 (82.4) | 1.00 | |
| Rural | 4,253 (18.0) | 3.344 (21.6) | 909 (11.1) | 2.17 (2.00;2.35) | 2.01 (1.81;2.22) |
| Peri-urban | 458 (1.9) | 232 (1.5) | 226 (2.8) | 0.61 (0.50;0.73) | 0.48 (0.38;0.61) |
| Degree of disability | |||||
| Grade 0 | 13,767 (58.1) | 8,.968 (57.9) | 4,799 (58.6) | 1.00 | - |
| Grade 1 | 4,577 (19.3) | 3,133 (20.2) | 1,444 (17.6) | 1.16 (1.08;1.25) | - |
| Grade 2 | 1,703 (7.2) | 1,091 (7.0) | 612 (7.5) | 0.95 (0.86;1.06) | - |
| Operational classification of the disease | |||||
| Paucibacillary | 8,704 (36.8) | 5,512 (35.6) | 3,192 (39.0) | 1.00 | |
| Multibacillary | 14,967 (63.2) | 9,968 (64.4) | 4,999 (61.0) | 1.15 (1.09;1.22) | 1.19 (1.11;1.28) |
| Mode of detection of new cases | |||||
| Referral | 12,755 (53.9) | 7,421 (47.9) | 5,334 (65.1) | 1,00 | |
| Spontaneous demand | 9,181 (38.8) | 6,808 (44.0) | 2,373 (29.0) | 2.06 (1.94;2.19) | 1.55 (1.44;1.66) |
| Collective examination | 441 (1.9) | 286 (1.8) | 155 (1.9) | 1.33 (1.09;1.62) | - |
| Examination of contacts | 582 (2.5) | 430 (2.8) | 152 (1.9) | 2.03 (1.68;2.45) | 1.71 (1.35;2.18) |
a) OR: odds ratio; b) 95%IC: 95% Confidence interval.
Note: The dash ( - ) represents ‘not calculated’.
For joinpoint analysis, the general trend was to increase leprosy cases in which all contacts, among those registered, were examined (VPA=2.1 - 95%CI 1.2;3.0). However, when considering race/skin color, this same trend was only observed in white people (VPA=2.3 - 95%CI 0.2;4.4) and those with high school (VPA=4.5 - 95%CI 2.6;6.5) or higher education (VPA=11.0 - 95%CI 6.2;16.1). Living in the urban area showed an increase (VPA=2.3 - 95%CI 1.5;3.2), while living in the peri-urban area, a reduction (VPA=-7.8 - 95%CI -13.6;-1.7). Regardless of the operational classification of leprosy cases, a trend of a more expressive increase was observed in new multibacillary cases (VPA=2.2 - 95%CI 1.4;2.9). Regarding the mode of entry of new cases, cases diagnosed through the collective examination (VPA=3.1 - 95%CI 1.5;4.7) presented a significant trend of an increasing tendency of evaluations of contacts (Table 2).
Table 2 Temporal trend using joinpoint analysis of the proportion of new leprosy cases with 100% of contacts examined among those recorded in the years of cohort, related to sociodemographic and clinical variables of new leprosy cases, state of Ceará, Brazil, 2008-2019
| Variables | Annual percentage change (95%CI) |
|---|---|
| Total | 2.1a (1.2;3.0) |
| Sex | |
| Female | 2.0a (1.1;2.9) |
| Male | 2.1a (1.2;3.0) |
| Race/skin color | |
| White | 2,3a (0.2;4.4) |
| Black | 1.2 (-0.3;2.8) |
| Asian | 1.9 (-0.4;4.3) |
| Brown | 0.7 (-0.8;2.3) |
| Indigenous | 1.6 (-7.6;11.7) |
| Age group (in years) | |
| <15 | 1.9a (0.4;3.3) |
| 15-59 | 2.1a (1.1;3.1) |
| ≥60 | 1.9a (1.1;2.6) |
| Schooling | |
| Illiterate | 2.0a (0.4;3.6) |
| Elementary school | 1.0 (-1.0;3.1) |
| High school | 4.5a (2.6;6.5) |
| Higher education | 11.0a (6.2;16.1) |
| Place of residence | |
| Urban | 2.3a (1.5;3.2) |
| Rural | 0.7 (-0.8;2.1) |
| Peri-urban | -7.8a (-13.6;-1.7) |
| Degree of disability | |
| Grade 0 | 2.7a (1.8;3.7) |
| Grade 1 | 1.9a (1.0;2.8) |
| Grade 2 | 1.6a (0.5;2.7) |
| Operational classification of the disease | |
| Paucibacillary | 1.9a (0.6;3.2) |
| Multibacillary | 2.2a (1.4;2.9) |
| Mode of detection mode of new cases | |
| Referral | 2,3a (1,0;3,6) |
| Spontaneous demand | 1,5a (0,5;2,4) |
| Collective examination | 3,1a (1,5;4,7) |
| Examination of contacts | 1,6a (0,3;3,0) |
a) Significantly different of 0,0 (p < 0,05).
Discussion
Despite the increased risk of illness among contacts of new leprosy cases, failures have been persistent in the development of surveillance actions in the state of Ceará, in more than one-third of the situations, making it difficult to control the disease. There was an association between specific characteristics of new leprosy cases and the fact that they did not have 100% of their contacts evaluated, highlighting, as determining factors: male gender, having self-referred of brown or black race/skin color, having low level of education, living in the rural area, being a multibacillary case and having been diagnosed through the evaluation of contacts. Although the indicator of surveillance action coverage for each case have shown general trend of increase over the selected 12-year period, the joinpoint analysis did not recognize this same pattern for contacts of new leprosy cases of black or brown race/ skin color, with low level of education and resident in rural areas of Ceará.
The higher probability for non-evaluation of all contacts, when the person with leprosy is male, can reveal sociocultural issues, closely related to the way of experiencing the health-disease-care process. In Brazil, traditional attitudes, practices and values, expressed through sexist or misogynistic behavior, reinforce a cultural structure related to gender inequality, which interferes in the health care process.18 The representation of caring as a female task, as well as failures in the provision of healthcare for men, leave them in a situation of vulnerability. Studies related to leprosy and physical disability point out to a higher individual vulnerability to the occurrence of this association in men and the elderly, similarly, data from the Ministry of Health have shown an increase in the number of cases among male population.4,19 Therefore, in addition to specific actions aimed at leprosy contact tracing among the male population, it is essential to develop health education strategies and promote self-care practices.
In addition to the aspects raised, related to gender, different perspectives on access to healthcare, work, education among others, essential to human life, are strongly influenced by the dimension of race/skin color.20 In a specific way, understanding how much the access to health services is affected in a society with a strong racial bias has been central in this analysis. Understanding the reasons for the low coverage of the evaluation of leprosy contacts of black race/skin color necessarily implies the implementation of strategies to face difficulties in exercising citizenship by these people.20,21 A study conducted in the state of Bahia, aimed at analyzing the coverage of the evaluation of contacts of leprosy cases, pointed out to a critical barrier to access to race/skin color.22 Another study, involving 24,000 people with leprosy throughout Brazil, analyzing only data from individuals up to 15 years of age, showed that children of black race/skin color had a leprosy detection rate 92% higher than those of white race/skin color; the same study observed that this rate was 40% higher when the adult population was included.23 Thus, facing racism in our society and existing inequalities that impact on a greater stigma, lower social participation and less empowerment become a central element in actions aimed at qualifying contact surveillance.24
Another sociodemographic factor associated with the non-evaluation of all contacts of new leprosy cases refers to the variable ‘schooling’, a proxy for socioeconomic status. From the broader perspective of human and social development, the worse the level of education, the greater the context of vulnerability and neglect, maintaining leprosy as a problem that will follow the patient in different stages of life.25 This study indicates that in Ceará, contacts of cases with higher education level are 60% more likely to be evaluated, when compared to those without education. Another study revealed that in general, those cases who went through irregular polychemotherapy for leprosy were among people with lower education.26 Likewise, a study conducted in Vale do Jequitinhonha, state of Minas Gerais, showed that people without education were 82% more likely to present physical disabilities in the diagnosis of leprosy, when compared to those with elementary education, and this probability was even higher when compared to those with high school: OR=4.03; p<0.0001.16
Leprosy is a neglected condition associated with poverty, therefore, there is increased vulnerability, given all dimensions previously presented, when expressed together. In addition to structural reforms aimed at overcoming inequalities and poverty/extreme poverty in the country, it is essential to incorporate new strategies of inclusive health education, contextualized, accessible to different sociodemographic conditions.27
Living in the rural area implied a possible limitation of access to the evaluation of contacts, which may mean, for example, the presence of geographical barriers. Studies that discuss the evaluation of leprosy contacts in the context of rural areas in the country, under different levels of PHC coverage, are limited. The study conducted in the state of Bahia, mentioned before, found an increased tendency in the proportion of contacts examined, with a lower expression when the leprosy case lived in small towns.22,28 Considering that surveillance actions should take place, as a priority, in the context of the performance of PHC teams, and given their satisfactory coverage - and scope - in most small and medium-sized municipalities, it is essential to deepen the analysis of possible factors associated with the unsatisfactory performance of leprosy surveillance actions. It is necessary to understand to what extent the development of these actions is part of the routine of health teams, in the process of monitoring and evaluating leprosy in Ceará. Similarly, it is of strategic importance to understand possible sociocultural aspects capable of interfering in the search or not for health care in rural communities.29
The study revealed an association between the non-evaluation of all contacts of new cases and the operational classification of multibacillary leprosy. From the clinical point of view, new multibacillary cases reveal greater potential of severity of the disease, in addition to a longer time of its evolution without diagnosis.2 Similarly, when the entry of new cases resulted from examination of contacts, it was almost 80% less likely to have their contacts evaluated. A possible consequence of these findings is the persistence of higher risk of infection among household social networks of these cases, increasing the occurrence of overlapping of new cases in the same family as an indicator of increased risk.28
A plan based on the analysis of this territorial context could guide the development of actions related to this reality, in Primary Health Care. Thus, it is suggested to make this a sentinel event, aimed at prioritizing longitudinal surveillance of leprosy contacts, especially those of multibacillary cases and families with recurrent leprosy.28
Limitations are part of studies that use secondary database. In this study, we sought to understand the quality of the information analyzed, by identifying the pattern of variables and indicators related to contacts registered and evaluated over a 12-year period. It is worth highlighting that, on average, almost 4% of new leprosy cases have no contacts registered on a state database. Considering a more in-depth discussion, it is necessary to integrate the perspectives of data surveillance at the local level, for an adequate management of care.30 Keeping database up to date, throughout the treatment of leprosy cases, should be a priority for surveillance, development of actions and care aimed at this population. In addition, temporal analyses reaffirmed the trend of maintenance - or worsening - of some dimensions of vulnerability analyzed, reinforcing the relevance of the results of this research.
Distinct dimensions of individual and social vulnerability of new leprosy cases in the state of Ceará influence the persistent unsatisfactory performance of the evaluation of their contacts. Operational aspects of contact surveillance actions reinforce that leprosy control goes through a process of qualification and development of more contextualized strategies, according to different territories, and also in the Brazilian National Health System, at the local level. The ‘Integrated Plan of Strategic Actions to Eliminate and Control Leprosy in Ceará, 2019-2022’ reaffirms the importance of the qualification and development of actions based on municipal realities.12
The negative impact on disease control confirms that the state of Ceará has had the challenge of qualifying its healthcare network through the development of leprosy surveillance actions; and implementation of strategies aimed at reducing inequalities, in addition to signifying the sociodemographic and clinical characteristics of the population as determining factors of vulnerability to the disease. Leprosy, like other neglected tropical diseases, demands structural changes in its surveillance, to which the ethical commitment of researchers, managers, health professionals and the community should be added, in defense and promotion of Public Health.
Referências
1. Ploemacher T, Faber WR, Menke H, Rutten V, Pieters T. Reservoirs and transmission routes of leprosy: a systematic review. PLoS Negl Trop Dis. 2020;14(4):e0008276. doi: https://doi.org/10.1371/journal.pntd.0008276. [ Links ]
2. Ministério da Saúde (BR). Diretrizes para a vigilância, atenção e eliminação da hanseníase como problema de saúde pública: manual técnico-operacional [Internet]. Brasília, DF: MS; 2016 [acesso 19 nov. 2020]. Disponível em: http://portalarquivos2.saude.gov.br/images/pdf/2016/fevereiro/04/diretrizes-eliminacao-hanseniase-4fev16-web.pdf [ Links ]
3. Ministério da Saúde (BR). Estratégia nacional para enfrentamento da hanseníase 2019-2022 [Internet]. Brasília, DF: MS ; 2020 [acesso 21 nov. 2020]. Disponível em: http://www.aids.gov.br/system/tdf/pub/2016/67207/estrategia_nacional_de_hanseniase_2019-2022_web.pdf?file=1&type=node&id=67207&force=1 [ Links ]
4. Souza EA, Boigny RN, Ferreira AF, Alencar CH, Oliveira MLW, Ramos Jr AN. Vulnerabilidade programática no controle da hanseníase: padrões na perspectiva de gênero no Estado da Bahia, Brasil. Cad Saude Publica 2018;34(1): e00196216. doi: https://doi.org/10.1590/0102-311x00196216. [ Links ]
5. Souza EA, Ferreira AF, Boigny RN, Alencar CH, Heukelbach J, Martins-Melo FR, et al. Leprosy and gender in Brazil: trends in an endemic area of the Northeast region, 2001-2014. Rev Saude Publica. 2018;52:20. https://doi.org/10.11606/S1518-8787.2018052000335. [ Links ]
6. World Health Organization. Global leprosy (hansen disease) update, 2019: time to step-up prevention initiatives. Weekly Epidemiological Record [Internet]. 2020 Sep 4 [citado 2 nov. 2020];95(36):417-40. Disponível em: https://apps.who.int/iris/bitstream/handle/10665/334140/WER9536-eng-fre.pdf?sequence=1&isAllowed=y [ Links ]
7. Secretaria da Saúde do Estado do Ceará. Boletim epidemiológico: Hanseníase [Internet]. Fortaleza: Secretaria da Saúde do Estado do Ceará; 10 jun. 2020 [acesso 21 nov. 2020]. Disponível em: https://www.saude.ce.gov.br/wp-content/uploads/sites/9/2018/06/boletim_hanseniase_10_06_2020_v2.pdf [ Links ]
8. World Health Organization. Global leprosy strategy 2016-2020: accelerating towards a leprosy-free world [Internet]. New Delhi: WHO; 2016 [acesso 22 nov. 2020]. 23 p. Disponível em: http://apps.who.int/iris/bitstream/10665/208824/1/9789290225096_Eng.pdf [ Links ]
9. Ministério da Saúde (BR). Guia prático sobre a hanseníase [Internet]. Brasília, DF: MS ; 2017 [acesso 3 nov. 2020]. Disponível em: https://www.saude.gov.br/images/pdf/2017/novembro/22/Guia-Pratico-de-Hanseniase-WEB.pdf [ Links ]
10. Ministério da Saúde (BR). Hanseníase: 2020. Boletim epidemiológico [Internet]. jan. 2020 [citado 1 nov. 2020]; (n. especial):1-51. Disponível em: https://portalarquivos2.saude.gov.br/images/pdf/2020/janeiro/31/Boletim-hanseniase-2020-web.pdf [ Links ]
11. Romanholo HSB, Souza EA, Ramos Jr AN, Kaiser ACGCB, Silva IO, Brito AL, et al. Vigilância de contatos intradomiciliares de hanseníase: perspectiva do usuário em município hiperendêmico. Rev Bras Enferm. 2018;71(1):163-9. doi: http://dx.doi.org/10.1590/0034-7167-2016-0607. [ Links ]
12. Secretaria de Saúde (CE). Plano integrado de atenção e vigilância para o enfrentamento da hanseníase no Ceará, 2019-2022. Fortaleza: Secretaria Estadual de Saúde do Ceará. 2021 [acesso 5 mar. 2021]. Disponível em: https://www.saude.ce.gov.br/wp-content/uploads/sites/9/2020/12/plano_integrado_atencao_enfrentamento_hanseniase_2019_2022_20211102.pdf [ Links ]
13. Instituto Brasileiro de Geografia e Estatística. Estatística IBGE [Internet]. Brasil em Síntese. 2020 [Acesso em 1 nov. 2020]. Disponível em: https://cidades.ibge.gov.br / [ Links ]
14. Instituto de Pesquisa Econômica Aplicada. Atlas da vulnerabilidade social nos municípios brasileiros [Internet]. Brasília, DF: IPEA; 2015 [acesso 10 nov. 2020]. Disponível em: http://ivs.ipea.gov.br [ Links ]
15. Atlas do desenvolvimento humano no Brasil [Internet]. Perfil municipal Rio de Janeiro, RJ. [local desconhecido]: PNUD; c2013 [acesso 9 nov. 2020]. Disponível em: http://atlasbrasil.org.br/2013 / [ Links ]
16. Lages DS, Kerr BM, Bueno IC, Niitsuma ENA, Lana FCF. A baixa escolaridade está associada ao aumento de incapacidades físicas no diagnóstico de hanseníase no Vale do Jequitinhonha. HU Rev. 2019 jun. 21;44(3):303-9. doi: https://doi.org/10.34019/1982-8047.2018.v44.14035 [ Links ]
17. Moura EGS, Araújo APM, Silva MCR, Cardoso BA, Holanda MC S, Conceição AO, et al. Relação entre a classificação internacional de funcionalidade, incapacidade e saúde (CIF) e a limitação de atividades e restrição à participação de indivíduos com hanseníase. Cad Saude Colet. 2017 set. 28;25(3):355-61. doi: https://doi.org/10.1590/1414-462x201700030336 [ Links ]
18. Oka M, Laurenti C. Entre sexo e gênero: um estudo bibliográfico-exploratório das ciências da saúde. Saude Soc. 2018;27(1):238-51. doi: https://doi.org/10.1590/s0104-12902018170524. [ Links ]
19. Nobre ML. Estratégias para bloquear a transmissão da hanseníase em município hiperendêmico, Mossoró, RN [tese; Internet] -. Rio de Janeiro: Fundação Oswaldo Cruz; 2016 [acesso 1 nov. 2020]. 231 f. Disponível em: https://www.arca.fiocruz.br/handle/icict/18794 [ Links ]
20. Abreu DMX, Lopes ÉAS, Lima AMLD, Santos AF, Rocha HA, Fonseca Sobrinho D et al. Acesso à atenção básica em saúde nas regiões nordeste e sudeste segundo raça/cor [Internet]. Anais do 21. Encontro Nacional de Estudos Populacionais; 2018 [acesso 2 nov. 2020];1-5. 2018. Disponível em: http://www.abep.org.br/publicacoes/index.php/anais/article/download/3198/3059 [ Links ]
21. Almeida SL. Racismo estrutural: Feminismos Plurais [livro eletrônico]. São Paulo: Pólen; 2019. [ Links ]
22. Souza EA, Ferreira AF, Pinto MSAP, Heukelbach J, Oliveira HX, Barbosa JC, et al. Desempenho da vigilância de contatos de casos de hanseníase: uma análise espaço-temporal no Estado da Bahia, Região Nordeste do Brasil. Cad Saude Publica . 2019;35(9): e00209518. doi: http://dx.doi.org/10.1590/0102-311X00209518. [ Links ]
23. Pescarini JM, Williamson E, Nery JS, Ramond A, Ichihara MY, Fiaccone RL, et al. Effect of a conditional cash transfer programme on leprosy treatment adherence and cure in patients from the nationwide 100 Million Brazilian Cohort: a quasi-experimental study. Lancet Infect Dis. 2020;20(5):618-27. doi: https://doi.org/10.1016/S1473-3099(19)30624-3. [ Links ]
24. Carvalho SR, Gastaldo D. Promoção à saúde e empoderamento: uma reflexão a partir das perspectivas crítico-social pós-estruturalista. Cienc Saude Colet. 2008;13(Suppl 2):2029-40. doi: http://dx.doi.org/10.1590/S1413-81232008000900007. [ Links ]
25. Curi AZ, Menezes-Filho NA. A relação entre altura, escolaridade, ocupação e salários no Brasil. Pesqui Planej Econ [Internet]. 2009 [acesso 4 nov. 2020];38(3):414-58. Disponível em: http://www.anpec.org.br/encontro2008/artigos/200807071013530-.pdf [ Links ]
26. Lopes VAS, Rangel EM. Hanseníase e vulnerabilidade social: uma análise do perfil socioeconômico de usuários em tratamento irregular. Saude Debate. 2014;38(103):817-29. doi: http://doi.org/10.0.23.47/0103-1104.20140074. [ Links ]
27. Silva MCD, Paz EPA. Educação em saúde no programa de controle da hanseníase: a vivência da equipe multiprofissional. Esc Anna Nery. 2010;14(2):223-9. doi: https://doi.org/10.1590/S1414-81452010000200003. [ Links ]
28. Boigny RN, Souza EA, Romanholo HSB, Araújo OD, Araújo TME, Carneiro MAG, et al. Persistência da hanseníase em redes de convívio domiciliar: sobreposição de casos e vulnerabilidade em regiões endêmicas no Brasil. Cad Saúde Pública. 2019;35(2): e00105318. http://doi.org/10.1590/0102-311X00105318. [ Links ]
29. Ferreira ILCSN, Ferreira IN, Morraye MA. Os contatos de portadores de hanseníase em Paracatu (MG): perfil, conhecimentos e percepções. Hansenol Int [Internet]. 2012 [acesso 17 maio 2021];37(1):35-44. [ Links ]
30. Viana TCT, Novaes RT, Souza JDD, Pires MC, Souza KCS, Silva MV. Consistência e completitude do SINAN para vigilância do contato familiar de casos de hanseníase em área hiperendêmica de Rondônia, Brasil. Braz J Surg Clin Res [Internet]. 2017 [acesso 17 maio 2021];19(2):1-6. Disponível em: https://www.mastereditora.com.br/periodico/20170706_115041.pdf [ Links ]
Received: September 04, 2020; Accepted: April 12, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
