










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.4 Brasília dic. 2021 Epub 29-Nov-2021
http://dx.doi.org/10.1590/s1679-49742021000400023
Original Article
Repercussions of the COVID-19 epidemic on Brazilian National Health System urgent dental care in Piracicaba, Brazil, 2020
1 Prefeitura do Município de Piracicaba, Secretaria Municipal de Saúde, Piracicaba, SP, Brazil
2 Universidade Estadual de Campinas, Faculdade de Odontologia de Piracicaba, Piracicaba, SP, Brazil
Objective
To evaluate the repercussions of the COVID-19 pandemic on procedures performed by a public urgent dental care service (PUDS).
Methods
This was a cross-sectional study, using data from the PUDS in Piracicaba, SP, Brazil, prior to the pandemic (February-March 2020) and during the pandemic (March-April 2020). Differences in the care profile between the pre-COVID-19 period and the COVID-19 period, according to sex, age and dental procedures were analyzed using Pearson’s Chi-square test. Effect size was also measured using Cramer’s V.
Results
There was a 51% reduction in the number of visits between the pre-COVID-19 period (n=824) and the COVID-19 period (n=404). The percentage of extractions reduced from 14.7% to 8.9%, while the percentage of temporary cavity fillings increased from 22.9% to 33.2%, between the two periods.
Conclusion
The COVID-19 pandemic had repercussions on the amount and pattern of procedures performed at the city’s urgent dental care service.
Keywords: COVID-19; Dental Care; Infection Control, Dental; Surgery, Oral; Brazilian National Health System; Cross-Sectional Studies
Introduction
COVID-19 is a disease caused by the novel coronavirus (SARS-CoV-2), an infectious agent responsible for severe acute respiratory syndrome (SARS).1,2 Emerging in China in December 2019, the COVID-19 outbreak spread rapidly around the world until it was declared a pandemic by the World Health Organization (WHO) on March 11, 2020.3,4
In Brazil, the first case of the disease was diagnosed on February 26, 2020, and community transmission was declared on March 20 of the same year.5 Since then, the Ministry of Health has developed articulated actions and recommendations, aiming to inform the population about the disease and precautions against it, as well as to promote the need for social distancing.
The virus is transmitted mainly by inhalation/ingestion/direct contact of mucous membrane with droplets expelled by an infected individual.3-5 Due to its high fatality rate, COVID-19 has caused considerable changes to the routine of cities and the organization of health services, including dental services.6,7 Dental surgeons are health professionals at greatest risk of contracting the disease in their daily work, due to close contact with the oral cavities of the people they treat.8-10 Studies have shown that many dental procedures produce aerosol particles and droplets contaminated with blood, saliva and other fluids, which carry bacteria and viruses with a high potential for infecting dentists, auxiliary staff and users of health care services.11-14
To protect the health of dental professionals and the population under their care, on March 16, 2020, the Federal Dentistry Council recommended the suspension of dental activities in public health establishments throughout the country that were not proven to be urgent or emergency cases, i.e. activities related to the treatment of pain and infections of oral origin.15 In addition, the Council requested maximum rigor in service provision, concerning the adoption of sterilization and disinfection protocols, in order to minimize the risk of contagion.15 In this sense, the National Health Surveillance Agency (ANVISA) published a technical note reinforcing the recommendation to dental professionals to ensure necessary care regarding the use of personal protective equipment and measures to reduce the spread of aerosol particles.16
Studies worldwide have seen changes in the profile of care in health services, including oral health services, during the COVID-19 pandemic.17,18 In Brazil, studies have found changes in the profile of dental care in public health services, especially its reduction in the pandemic periods.19,20
Despite such evidence, little is known about the immediate repercussion of the pandemic on emergency dental services. In a study they conducted in Beijing, China, Guo et al.18 found that the COVID-19 epidemic influenced the number and types of dental procedures performed in emergency services. However, at the time of writing this publication, there is no knowledge of research on such aspects in public urgent dental services in Brazil.
The objective of this study was to evaluate the repercussion of the COVID-19 pandemic on the procedures performed by a public urgent dental care service.
Methods
This is a cross-sectional study, using secondary data from an urgent dental care service in the municipality of Piracicaba, São Paulo, collected prior to COVID-19 (February-March 2020) and during the pandemic (March-April 2020).
The Piracicaba municipal urgent dental care center, referred to as the urgent dental care service, has two consulting rooms and professionals able to provide urgent care on weekdays, from 7 a.m. to 9 p.m., and on holidays and weekends, from 8 a.m. to 4 p.m. At the urgent dental care service, users are attended to on a first-come, first-served basis, without prior risk assessment.
In 2020, Piracicaba had an estimated population of 404,142 inhabitants.21 In that year, the municipality's Public Health network was comprised of 51 Family Health Strategy centers and 20 primary health care centers, a medical specialty center, two dental specialty centers, four urgent medical care units, an urgent orthopedic and trauma care unit, a polyclinic and two referral hospitals. Within Primary Care provided under the Brazilian National Health System in Piracicaba, public dental care services were available at 30 Family Health Strategy centers and 17 primary health care centers, format I (dental surgeon and auxiliary).
Two periods were defined for analysis of dental care records and procedures, namely a pre-pandemic period (pre-COVID-19) and a second period corresponding to the beginning of the pandemic (COVID-19), according to criteria adopted by Guo et al.18 and adapted to the reality of this study, as follows:
Pre-COVID-19 period - care provided between February 27 and March 11, 2020 (two weeks), when, although there was already communitary transmission of coronavirus infection in Brazil, there were no restrictions on movement in the national territory, nor confirmed cases in Piracicaba.
COVID-19 period (COVID-19) - care provided between March 26 and April 8, 2020 (two weeks), when social distancing had been decreed in São Paulo state, after Brazilian authorities announced the presence of community transmission and cases of the disease had already been confirmed in Piracicaba.
The repercussion of the COVID-19 pandemic on urgent care provision was assessed by means of retrospective analysis of a census sample, on data about all care provided by the urgent dental care service in the periods studied (before and during the pandemic). These data were retrieved on May 14, 2020, using the OLOSTECH program,22 an online public health computer system adopted by the municipality. Through this system, a report is generated with information about the date of the consultation, service user’s name, sex, age, procedure performed and the professional responsible for the procedure. Records not containing the procedure performed were excluded.
The sample size, comprised of 1,228 people cared for at the urgent dental care service, had power of 0.98 (β = 0.02), with a 5% significance level (α = 0.05) for measuring the effect found (Cramer’s V = 0.1356).
The variables assessed were ‘sex’ (female; male), ‘age’ (in completed years, dichotomized by median age into ≤36 years and >36 years), ‘dental procedures’ (medication and orientation; pulp therapy; temporary cavity filling; extraction; other procedures), according to the periods defined (pre-COVID-19 and COVID-19).
Initially, descriptive analyses of the data were performed. Associations between the ‘gender’, ‘age’ and ‘dental procedures’ variables and the pre-COVID-19 and COVID-19 periods were analyzed using Pearson's chi-square test. Effect size was also measured using Cramer’s V.
The analyses were performed using the SAS/STAT 9.4 statistics program [Statistical Analysis System (SAS) Institute Inc. 2013, Version 9.4, Cary, NC, USA].
The study project was approved by the Research Ethics Committee of the Faculdade de Odontologia de Piracicaba, Universidade Estadual de Campinas, as per Certificate of Submission for Ethical Appraisal No. 42980921.0.0000.5418, in accordance with the Declaration of Helsinki.
Results
A total of 1,241 urgent dental care visits took place in the periods under analysis, pre-COVID-19 and COVID-19. Thirteen were excluded for not having a record of the procedure. This left a final sample of 1,228 visits. Among these, 824 (67.1%) related to the pre-COVID-19 period and 404 (32.9%) to the COVID-19 period, corresponding to a 51% reduction (Table 1).
Table 1 Demographic characteristics of individuals who used the urgent dental care service in the pre-COVID-19 period (February-March 2020) and during the COVID-19 pandemic (March-April 2020)
| Demographic characteristics | Period | Total | |
|---|---|---|---|
| Pre-COVID-19 | COVID-19 | ||
| n (%) | n (%) | n (%) | |
| Age (in full years) | |||
| ≤36 | 419 (50.8) | 204 (50.5) | 623 (50.7) |
| >36 | 405 (49.2) | 200 (49.5) | 605 (49.3) |
| p-value | 0.907 | ||
| Sex | |||
| Female | 403 (49.0) | 201 (49.7) | 604 (49.2) |
| Male | 421 (51.0) | 203 (50.3) | 624 (50.8) |
| p-value | 0.780 | ||
| Total | 824 (100.0) | 404 (100.0) | 1,228 (100.0) |
The demographic characteristics of the users attended to at the Urgent Dental Care Service in both the pre-COVID-19 period and the COVID-19 period indicate that there was no statistically significant difference in distribution by service user sex and age in either of the periods (Table 1).
Figure 1 shows the frequency of dental visits according to type of procedure, in both periods. In the pre-COVID-19 period, the main reason for dental visits was medication and guidance (32.6%), followed by pulp therapy (23.5%), temporary cavity filling (22.9%), extraction (14.7%) and other procedures (6.3%). In the COVID-19 period, the main reason for dental consultation was temporary cavity filling (33.2%), followed by medication and guidance (31.4%), pulp therapy (23.3%), extraction (8.9%) and other procedures (3.2%).
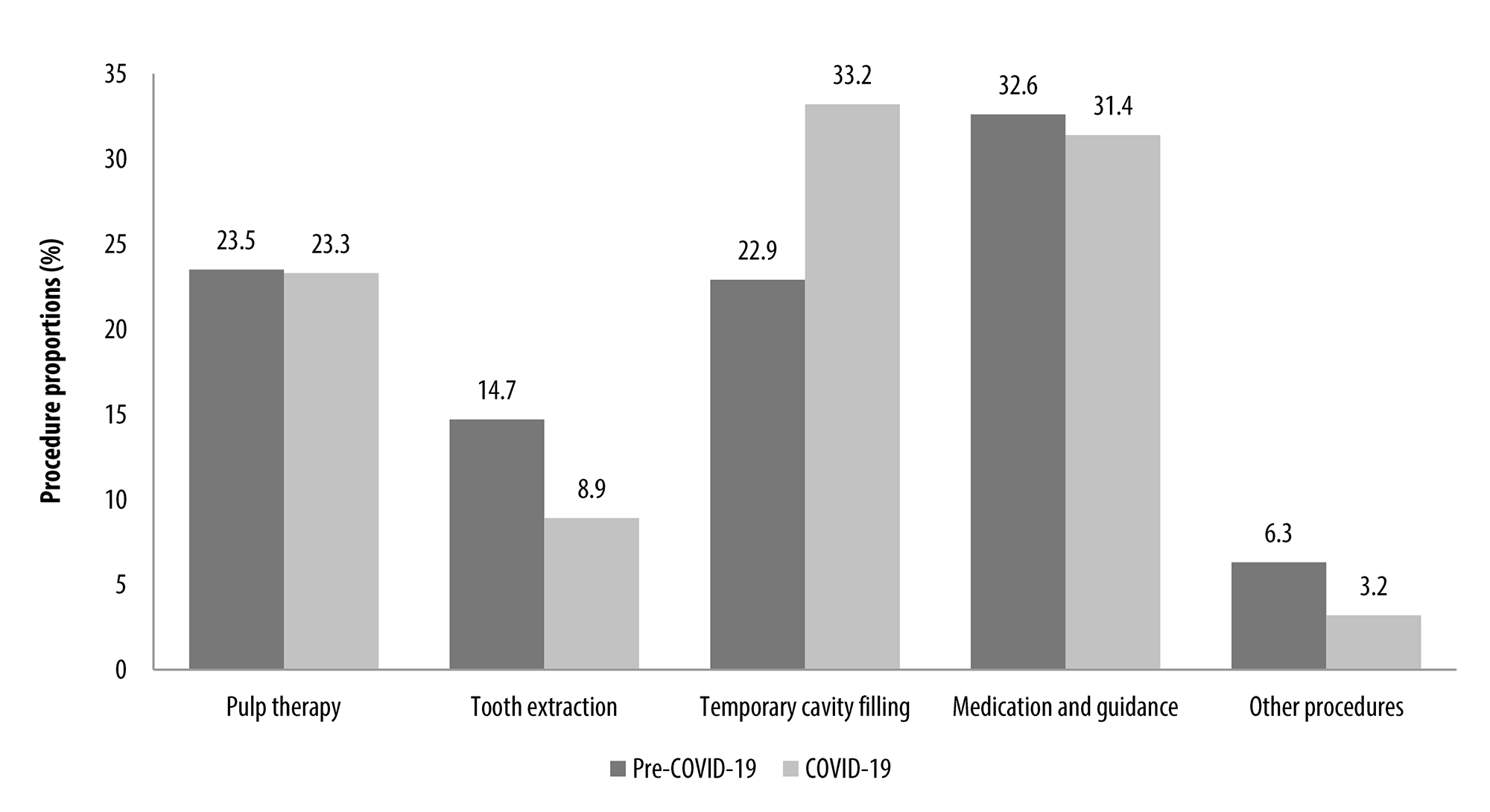
Figure 1 Dental care proportions according to procedure type, in the pre-COVID-19 period (February-March 2020) and during the COVID-19 pandemic (March-April 2020)
There was statistically significant association between type of dental procedure and the period when it was performed, either pre-COVID-19 or COVID-19, with a decrease in the percentage of extractions (from 14.7 to 8.9%) and an increase in the percentage of temporary cavity fillings (from 22.9 to 33.2%) between the pre-COVID-19 and COVID-19 periods.
Discussion
This study assessed the repercussion of COVID-19 on procedures carried out at the Piracicaba Municipal Urgent Dental Care Center, after the decree establishing social distancing in São Paulo state was published. The results indicate a considerable decrease in the number of urgent dental visits, besides changes in the pattern of dental procedures, such as the reduction in the number of tooth extractions with effect from the beginning of the epidemic. This fact, in particular, corroborates the findings of Cunha et al.23 on public dental services throughout the country. They compared data from the Brazilian National Health System Outpatient Information System, between April and June 2019 and during the year 2020, and found a decrease of 88.4% in the total productivity of the services offered by Primary and Specialized Care, as well as an 87% reduction in tooth extractions, as also found by studies conducted in other countries.18
Some hypotheses can be raised to explain the results of the present study. Initially, the population was seen to stay at home and followed the recommendations for social distancing, having only gone out to undertake essential activities, in accordance with health regulations. Moreover, the fear of contracting COVID-19 could have made people reluctant to attend health services, such as hospitals and dental centers, with the intention of preventing the risk of contagion, as demonstrated by several studies.24 It is possible that many toothache problems were temporarily solved with painkillers, since self-medication is widely used in Brazil and mainly involves access to medicines without a prescription issued by a qualified professional being required.25
The most frequent dental procedures performed at the Urgent Dental Care Service in the pre-COVID-19 period were medication and orientation, followed by pulp therapy, indicated due to the presence of acute pain/infection of dental origin. In contrast, in the COVID-19 period, the most frequent procedure was temporary cavity filling, this being less urgent and invasive. These findings differ from the study by Guo et al.,18 conducted in an emergency dental service in Beijing, which found that people preferred to seek those services when they had intense toothache, trauma, cellulitis or dental abscesses during the epidemic.18 It must be taken into consideration that the Beijing study involved users of a dental service located inside a hospital, where there is a greater probability of there being individuals with COVID-19. This fact may have resulted in fear of using that service and, therefore, only those with more severe conditions sought dental care.26 Another hypothesis to be considered, to explain these differences, may be related to the self-medication culture observed in the Brazilian population.25
Visits involving extraction procedures decreased, between the pre-COVID-19 and the COVID-19 periods. As already described, one of the hypotheses for this decrease may be the population's fear of contracting COVID-19 during their care in health services.24 Of equal importance, however, is that health professionals’ fear of contracting COVID-19 for the same reason may have increased in relation to performing more invasive procedures, such as tooth extractions, which may have led to a reduction in these procedures being performed in health services.27 Ahmed et al.28 demonstrated that despite dentists having a high level of knowledge about preventing infection in dental practice, they were anxious and afraid about attending to service users, fearing that they might become infected and transmit the disease to their families.
Although there are studies in Brazil that corroborate changes in the pattern of dental procedures offered by health services in the context of the COVID-19 pandemic, they have not specifically evaluated changes in the pattern of procedures offered in urgent dental care services.19,20 As such, the present study contributes to the literature on the subject, since it was conducted in a different setting and evaluated other variables and associations not investigated in the aforementioned studies.
There are speculations that the demand for dental services may grow exponentially, once the epidemic has been controlled, given the demand held back by the COVID-19 factor.18
On the global scenario, remote health care is one of the alternatives being used by health services to meet the population’s health needs. In Brazil, telemonitoring and teleconsultation are recently regulated forms of remote care that are now in use.29 Additionally, Federal Dentistry Council Resolution No. 228, dated July 16, 2020,30 allows use of technology-mediated teledentistry by the Brazilian National Health system for as long as the state of public calamity decreed by the Federal Government remains in force. These remote forms of care can be important allies, avoiding having to out unnecessarily.
As limitations of the study, we mention the short time interval of the pre-COVID-19 and COVID-19 evaluation periods (two weeks for each), which did not allow investigation of whether the changes in patterns found in that period remained for longer. However, this short study period was selected because following it the service was reorganized, involving an intentional decrease in the availability of urgent care for the population with the aim of reducing the risks of infection for both service users and health workers. However, it is noteworthy that studies such as this are important as they can point out aspects that can contribute to the qualification of health information systems.
We conclude that the COVID-19 epidemic had an immediate impact on the number and pattern of procedures performed at the Piracicaba Municipal Urgent Dental Care Center. We highlight the need for continuous reorganization and adaptation of oral health services, given the rapid changes brought about by COVID-19. Health workers dedicated to these services need to receive training to ensure their individual and collective protection. It is suggested that health service managers act in a coordinated manner to provide support for the new demands generated, and implement comprehensive measures for the prevention and control of oral health problems, as well as facilitating access to elective services for dental treatment in the future.
Referências
1. Gorbalenya AE, Baker SC, Baric RS, de Groot RJ, Drosten C, Gulyaeva AA, et al. Severe acute respiratory syndrome-related coronavirus: the species and its viruses, a statement of the coronavirus study group. bioRxiv. 2020. Now published: Nat Microbiol. 2020;5:536-44. doi: https://doi.org/10.1038/s41564-020-0695-z. [ Links ]
2. Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020 Feb 20;382(8):727-33. doi: https://doi.org/10.1056/NEJMoa2001017. [ Links ]
3. Spagnuolo G, De Vito D, Rengo S, Tatullo M. Covid-19 outbreak: an overview on dentistry. Int J Environ Res Public Health. 2020 Mar 22;17(6):2094. doi: https://doi.org/10.3390/ijerph17062094. [ Links ]
4. Li Q, Guan X, Wu P, Wang X, Zhou L, Tong Y, et al. Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia. N Engl J Med. 2020 Mar 26;382(13):1199-1207. doi: https://doi.org/10.1056/NEJMoa2001316. [ Links ]
5. Ministério da Saúde (BR). Portaria n. 454, de 20 de março de 2020. Declara, em todo o território nacional, o estado de transmissão comunitária do coronavírus (covid-19). D Of Uniao [Internet]. 20 mar. 2020 [acesso 21 out. 2021];2020(55-F):1. Seção 1. Disponível em: https://www.in.gov.br/en/web/dou/-/portaria-n-454-de-20-de-marco-de-2020-249091587 [ Links ]
6. Rache B, Rocha R, Nunes L, Spinola P, Malik AM, Massuda A. Necessidades de infraestrutura do SUS em preparo ao covid-19: leitos de UTI, respiradores e ocupação hospitalar. São Paulo: IEPS; 2020. (Nota técnica n. 3). [ Links ]
7. Ather A, Patel B, Ruparel NB, Diogenes A, Hargreaves KH. Coronavirus disease 19 (covid-19): implications for clinical dental care. J Endod. 2020;46(5):584-95. doi: https://doi.org/10.1016/j.joen.2020.03.008. [ Links ]
8. Valenzuela M. Coronavirus y el consultorio dental. J Oral Res. 2020;2020(Covid-19):14-9. doi: https://doi.org/10.17126/joralres.2020.045. [ Links ]
9. Coulthard P. Dentistry and coronavirus (covid-19), moral decision, making. Br Dent J. 2020;228(7):503-5. doi: https://doi.org/10.1038/s41415-020-1482-1. [ Links ]
10. Gamio L. The workers who face the greatest coronavirus risk. The New York Times [Internet]. 2020 Mar 15 [acesso 15 mar. 2020]. Disponível em: https://www.nytimes.com/interactive/2020/03/15/business/economy/coronavirus-worker-risk.html?action=click&module=Top+Stories &pgtype=Homepage [ Links ]
11. Ge Z-Y, Yang L-M, Xia J-J, Fu X-H, Zhang Y-Z. Possible aerosol transmission of covid-19 and special precautions in dentistry. J Zhejiang Univ Sci B. 2020;21(5):361-8. doi: https://doi.org/10.1631/jzus.B2010010. [ Links ]
12. Burger D. ADA recommending dentists postpone elective procedures. ADANews [Internet]. 2020 Mar 16 [acesso 21 out. 2020]. Disponível em: https://www.ada.org/en/publications/ada-news/2020-archive/march/ada-recommending-dentists-postpone-elective-procedures [ Links ]
13. Tuñas ITC, Silva ET, Santiago SBS, Maia KD, Silva Júnior JO. Doença pelo coronavírus 2019 (covid-19): uma abordagem preventiva para a odontologia. Rev Bras Odontol. 2020;77:e1766. doi: http://doi.org/10.18363/rbo.v77.2020.e1776. [ Links ]
14. Harrel SK, Molinari J. Aerosols and splatter in dentistry: a brief review of the literature and infection control implications. J Am Dent Assoc. 2004;135(4):429-37. doi: http://doi.org/10.14219/jada.archive.2004.0207. [ Links ]
15. Conselho Federal de Odontologia (BR). Ofício n. 477/2020/CFO. Atendimento odontológico: covid-19. Brasília, DF: CFO; 16 de março de 2020. [ Links ]
16. Agência Nacional de Vigilância Sanitária (BR). Nota Técnica n. 4, de 2020. Orientações para serviços de saúde: medidas de prevenção e controle que devem ser adotadas durante a assistência aos casos suspeitos ou confirmados de infecção pelo novo coronavírus (SARS-CoV-2). Brasília, DF, ANVISA; 2020. [ Links ]
17. Yang Y, Zhou Y, Liu X, Tan J. Health services provision of 48 public tertiary dental hospitals during the covid-19 epidemic in China. Clin Oral Investig. 2020;24(5):1861-4. doi: http://doi.org/10.1007/s00784-020-03267-8. [ Links ]
18. Guo H, Zhou Y, Liu X, Tan J. The impact of the covid-19 epidemic on the utilization of emergency dental services. J Dent Sci. 2020;15(4):564-7. doi: http://doi.org/10.1016/j.jds.2020.02.002. [ Links ]
19. Lucena EHG, Freire AR, Freire DEWG, Araújo ECF, Lira GNW, Brito ACM, et al. Offer and use of oral health in primary care before and after the beginning of the covid-19 pandemic in Brazil. Pesqui Bras Odontopediatria Clin Integr. 2020;20(suppl 1):e0139. doi: https://doi.org/10.1590/pboci.2020.163. [ Links ]
20. Santos MBF, Pires ALC, Saporiti JM, Kinalski MA, Marchini L. Impact of covid-19 pandemic on oral health procedures provided by the Brazilian public health system: covid-19 and oral health in Brazil. Health Policy Technol. 2021;10(1):135-42. doi: https://doi.org/10.1016/j.hlpt.2021.02.001. [ Links ]
21. Instituto Brasileiro de Geografia e Estatística. Piracicaba: panorama [Internet]. Brasília, DF: IBGE; 2020 [acesso 21 out. 2020]. Disponível em: https://cidades.ibge.gov.br/brasil/sp/piracicaba/panorama [ Links ]
22. Olostech [homepage]. Jaraguá do Sul (SC): Olostech; 1993 [acesso 21 out. 2020]. Disponível em: http://www.olostech.com [ Links ]
23. Cunha AR, Velasco SRM, Hugo FN, Antunes JLF. The impact of the covid-19 pandemic on the provision of dental procedures performed by the Brazilian unified health system: a syndemic perspective. Rev Bras Epidemiol. 2021 May 26;24:e210028. doi: https://doi.org/10.1590/1980-549720210028. [ Links ]
24. Moraes RR, Correa MB, Queiroz AB, Daneris Â, Lopes JP, Pereira-Cenci T, et al. Covid-19 challenges to dentistry in the new pandemic epicenter: Brazil. PLoS One. 2020 Nov 30;15(11):e0242251. doi: https://doi.org/10.1371/journal.pone.0242251. [ Links ]
25. Arrais PSD, Fernandes MEP, Dal Pizzol TS, Ramos LR, Mengue SS, Luiza VL, et al. Prevalence of self-medication in Brazil and associated factors. Rev Saude Publica. 2016;50(suppl 2):13s. doi: https://doi.org/10.1590/S1518-8787.2016050006117. [ Links ]
26. Medina MG, Giovanella L, Bousquat A, Mendonça MHM, Aquino R. Primary healthcare in times of COVID-19: what to do?. Cad Saude Publica. 2020;36(8):e00149720. doi: http://doi.org/10.1590/0102-311X00149720. [ Links ]
27. Teixeira CFS, Soares CM, Souza EA, Lisboa ES, Pinto ICM, Andrade LR, et al. The health of healthcare professionals coping with the covid-19 pandemic. Cienc Saude Colet. 2020;25(9):3465-74. doi: http://doi.org/10.1590/1413-81232020259.19562020. [ Links ]
28. Ahmed MA, Jouhar R., Ahmed N, Adnan S, Aftab M, Zafar MS, et al. Fear and practice modifications among dentists to combat novel coronavirus disease (covid-19) outbreak. Int J Environ Res Public Health. 2020 Apr 19;17(8):2821. doi: http://doi.org/10.3390/ijerph17082821. [ Links ]
29. Conselho Federal de Odontologia (BR). Resolução CFO-226, de 4 junho de 2020. Dispõe sobre o exercício da odontologia a distância, mediado por tecnologias, e dá outras providências. Brasília, DF: CFO; 4 jun. 2020. [ Links ]
30. Conselho Federal de Odontologia (BR). Resolução CFO-228. Regulamenta o artigo 5º da resolução CFO n. 226/2020. Brasília, DF: CFO; 16 jul 2020. [ Links ]
Received: July 26, 2021; Accepted: September 05, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
