










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.4 Brasília dic. 2021 Epub 29-Nov-2021
http://dx.doi.org/10.1590/s1679-49742021000400024
Original Article
In-hospital case fatality ratio due to COVID-19 in four Brazilian state capitals and its possible temporal relationship with the Gamma variant, 2020-2021
1 Fundação Oswaldo Cruz, Instituto Leônidas e Maria Deane, Manaus, AM, Brazil
2 Universidade do Estado do Amazonas, Escola Superior de Ciências da Saúde, Manaus, AM, Brazil
3 Universidade Federal de Pelotas, Faculdade de Medicina, Pelotas, RS, Brazil
Objective
To describe in-hospital and intensive care unit (ICU) case fatality ratios due to COVID-19 in four Brazilian state capitals, during the months of epidemic peaks and previous months.
Methods
This was an ecological study using monthly data from the Influenza Epidemiological Surveillance Information System, between 2020-2021, in individuals aged 20 years or older. Case fatality ratio and mortality rate were estimated with 95% confidence intervals (95%CI).
Results
In Manaus, the capital city of the state of Amazonas, ICU case fatality ratio among those >59 years old was lower in December/2020 (80.9%; 95%CI 78.4;83.3) and during the peak in January/2021 (79.9%; 95%CI 77.4;82.5), compared to the peak in April/2020 (88.2%; 95%CI 86.1;90.3). In São Paulo, the capital city of the state of São Paulo, Curitiba, the capital city of the state of Paraná, and Porto Alegre, the capital city of the state of Rio Grande do Sul, there was a decrease or stability in ICU and in-hospital case fatality ratio in January/2021, compared to the reference month in 2020.
Conclusion
In January/2021, in-hospital and ICU case fatality ratios decreased or remained stable in the four state capitals, especially in Manaus, and during the epidemic peak with the prevalence of the Gamma variant.
Keywords: Hospital Mortality; Brazil; COVID-19; Severe Acute Respiratory Syndrome; Coronavirus Infections; Ecological Studies
Introduction
As of October 2021, more than 4.9 million deaths due to COVID-19 had occurred worldwide, of which, more than 600,000 only in Brazil.1 More than half of the deaths in the country occurred in the first six months of 2021,1 when community transmission of the Gama variant achieved its highest levels and spread across South America.2
Manaus, the capital city of Amazonas state, was the Brazilian epicenter of the epidemic during its first wave. The city was observed between April and May 2020, and showed rapid and strong dissemination of the Gama variant during the second wave, in January 2021, when about 1,700 people died due to COVID-19 in the first 20 days of the year and at least 40 died due to lack of medical oxygen supply.3
Studies have indicated that variants of concern, such as Gamma,4,5 contribute to a rapid increase in the incidence of COVID-19, which may lead to overwhelmed healthcare system6 and, indirectly, increased case fatality ratio,7,8 given that the number of deaths due to the disease can achieve an exponential pattern. Variants such as Alpha, also with high transmission potential,9 could directly contribute to increased case fatality ratio,10 although this hypothesis has not been widely accepted.11
There are no published studies that have investigated whether there is an association between Gamma variant and higher in-hospital case fatality ratio. Although a recent analysis of the mortality profile, before and after the emergence of the Gamma variant in the state of Amazonas, suggests greater pathogenicity of this variant,12 but its results are still inconclusive.
This study aimed to describe hospital and intensive care unit (ICU) case fatality ratio due to COVID-19, in four Brazilian state capitals, during the months of epidemic peaks and the previous months.
Methods
Study design
This was an ecological study, using data from hospitalizations due to severe acute respiratory syndrome (SARS) caused by the new coronavirus (COVID-19).13 The units of analysis were four Brazilian state capitals.
Study population
The population analyzed was comprised of the aggregates of hospital records for hospitalizations and deaths in four regional metropolises: Manaus (North region), São Paulo (Southeast region), Curitiba (South region) and Porto Alegre (South region).
Manaus was included in the study because it was the most affected capital by the epidemic, both in the first and second waves. There is evidence that the Gama variant spread rapidly in that capital, leading to a new and even more severe collapse of its healthcare system.4 São Paulo, Curitiba and Porto Alegre, which provide some of the best high complexity healthcare services in the country,14 including significant ICU bed availability - compared to the North region, for example - were selected as 'control' because they experienced a decrease or stability related to the incidence of SARS in January 2021, compared to December 2020.15 This pattern of community transmission allowed not only the evaluation of in-hospital case fatality ratio in a scenario of modest advances in the therapy and management of COVID-19 cases, but also to find evidence that the Gama variant did not circulate intensively in those state capitals before February 2021.6,5
Authors' estimates took into consideration individuals aged 20 years or older, given the low COVID-19 mortality rate in those under this age.16 Deaths that occurred in Manaus between January 13 and 16, 2021 were excluded from the study in order to minimize distortions in case fatality ratio estimates: January 13 preceded the crisis of lack of medical oxygen in hospitals in Manaus, and it was the date when 110 victims of COVID-19 died, the highest daily number until then.17 January 14 was the date when the culmination of the crisis of medical oxygen supply took place; and the next two days, the only ones in the historical series with 125 or more deaths per day,17 when many individuals were transferred to other regions in the country, given the chaotic situation in the local healthcare system.
Data sources and measurement
Data were obtained from the Influenza Epidemiological Surveillance Information System (SIVEP-Gripe).13 It is updated weekly and brings together all notifications from health facilities in the country. To minimize coverage and lag problems, data under scrutiny were retrieved more than 160 days after the end of the investigation period, on January 31, 2021.
In Brazil, notification of suspected or confirmed COVID-19 cases is mandatory. It is considered as 'hospitalization due to COVID-19' all hospital records with the final classification of SARS due to COVID-19, which is equivalent to cases with closure records based on laboratory, clinical-epidemiological, clinical or clinical-imaging criteria.13 All records were collected according to the place of residence and date of symptom onset. Demographic data result from estimates developed by the Ministry of Health.
The period from March to August 2020 was defined as the first wave of the epidemic, based on the indicator for incidence rate of SARS per 100,000 inhabitants, according to the date of symptom onset.15 In the time frame for the first wave, the incidence rate of SARS suddenly increased from March to the first half of April when it reached its peak. In May, there was an abrupt drop, followed by sustained stabilization in June and July, forming a kind of “valley” to separate the first from the second wave. August was highlighted by the beginning of the reversal of decrease in the incidence rate of SARS in Manaus.15
The time frame for the second wave, from September onwards, is characterized by a sustained (for more than six weeks in a row) and significant increase in the incidence rate of SARS, reaching its peak in January 2021,15 without returning to the lowest values of the historical series (June and July 2020),
We considered as case fatality indicators (i) the percentage of individuals who died among those hospitalized, in general, here called 'in-hospital case fatality ratio, and (ii) the percentage of those hospitalized in the ICU.
The aggregate data on hospitalization were stratified according to the following variables:
state capital (Manaus; São Paulo; Porto Alegre; Curitiba);
age group (in full years: 20 to 39; 40 to 59; 60 and older); and
periods (monthly aggregation: Mar./2020; Apr./2020; May/2020; Jul./2020; Jan./2021).
The study included two distinct periods. For Manaus, these periods were comprised of two consecutive months and, only one month, for the other state capitals. The first period for Manaus, March and April 2020, represents the highest incidence rate of SARS during the first wave and there is no influence of the Gamma variant;15 the second period, December 2020 and January 2021, represents the highest incidence rate of SARS and strong circulation of the Gamma variant during the second wave.15 For São Paulo, the selected periods were May 2020, the month with the highest incidence rate of SARS that year and there was no influence of the Gamma variant, and January 2021, when the incidence rate of SARS showed signs of decrease, just before a significant increase.15 For Curitiba and Porto Alegre, the first period is related to July 2020 and the second to January 2021, according to the same criteria adopted for São Paulo.15
Data analysis
The calculation of the indicators was performed as follows:
a) In-hospital case fatality ratio
Numerator - number of deaths in hospital due to SARS caused by COVID-19, according to age groups, period, date of symptom onset and place of residence.
Denominator - total number of hospitalizations due to SARS caused by COVID-19, reported, according to age groups, period, date of symptom onset and place of residence.
Multiplication factor: 100
b) ICU case fatality ratio
Numerator - number of deaths reported in ICU due to SARS caused by COVID-19, according to age groups, period, date of symptom onset and place of residence.
Denominator - total number of hospitalizations reported in ICU due to SARS caused by COVID-19, according to age groups, period, date of symptom onset and place of residence.
Multiplication factor: 100
c) Mortality rate due to SARS caused by COVID-19 in Manaus (per 100,000 inhabitants)
Numerator - number of reported deaths due to SARS caused by COVID-19 in Manaus, according to age groups, period and date of symptom onset.
Denominator - corrected population projection for the total number of residents in Manaus, according to age group and for the year 2020.
Multiplication factor: 100,000
d) Standardized mortality ratio due to SARS caused by COVID-19
Numerator - number of reported deaths due to SARS caused by COVID-19 in Manaus, according to age groups, period and date of symptom onset.
Denominator - number of reported deaths due to SARS caused by COVID-19, in Manaus, according to a given age group and date of symptom onset.
Multiplication factor: 100
Case fatality ratio estimates have been presented as percentages, with 95% confidence intervals (95%CI). CIs were estimated based on the percentile bootstrap, with 1,000 replications,18 avoiding negative values and loss of accuracy of interval estimates. Thus, case fatality assessments were performed through inspection of the lower and upper limits of the interval estimates.
To evaluate the evolution of the epidemic in Manaus, taking into consideration the low and irregular performance of notification of new cases in the state of Amazonas,19 mortality rates due to COVID-19 were estimated. These rates sought to correct part of the negative impact of the pandemic on the demographic composition of the local population in 2020,20 as long as the analyses performed included only January 2021. As such, the excess mortality was estimated based on the difference between observed mortality and expected mortality in each age group, according to previously published methods.16 Then, the surplus value was deducted from each of the population estimates of the Ministry of Health, achieving the corrected population estimate.
Mortality rates and standardized mortality ratios were also followed by their respective 95%CI. For the analyses, the R software, version 3.6.1, and RStudio, version 1.2.1335 (http://www.r-project.org) were used.
Results
Manaus, during the first wave of the epidemic, reported 153 deaths due to COVID-19, being March 2020, the date of the symptom onset, and the mortality rate was 10.4 (95%CI 8.9;12.2) per 100,000 inhabitants. In April 2020, there were 1,584 deaths in the capital, according to the date of symptom onset, and the mortality rate was 108.2 (95%CI 103.0;113.6) per 100,000 inhabitants. During the second wave, in Manaus, 1,300 deaths were reported, and the date of symptom onset was December 2020, the mortality rate was 88.8 (95%CI 84.1;93.7) per 100,000 inhabitants. In January 2021, there were 3,148 deaths, according to the date of the symptom onset, and the mortality rate was 214.9 (95%CI 207.6;222.6) per 100,000 inhabitants.
Figure 1 shows that in Manaus, regardless of month and age group, mortality rates were higher in those aged 60 years and older. In the months immediately preceding the collapse that occurred in both April 2020 and January 2021, mortality rates were lower.
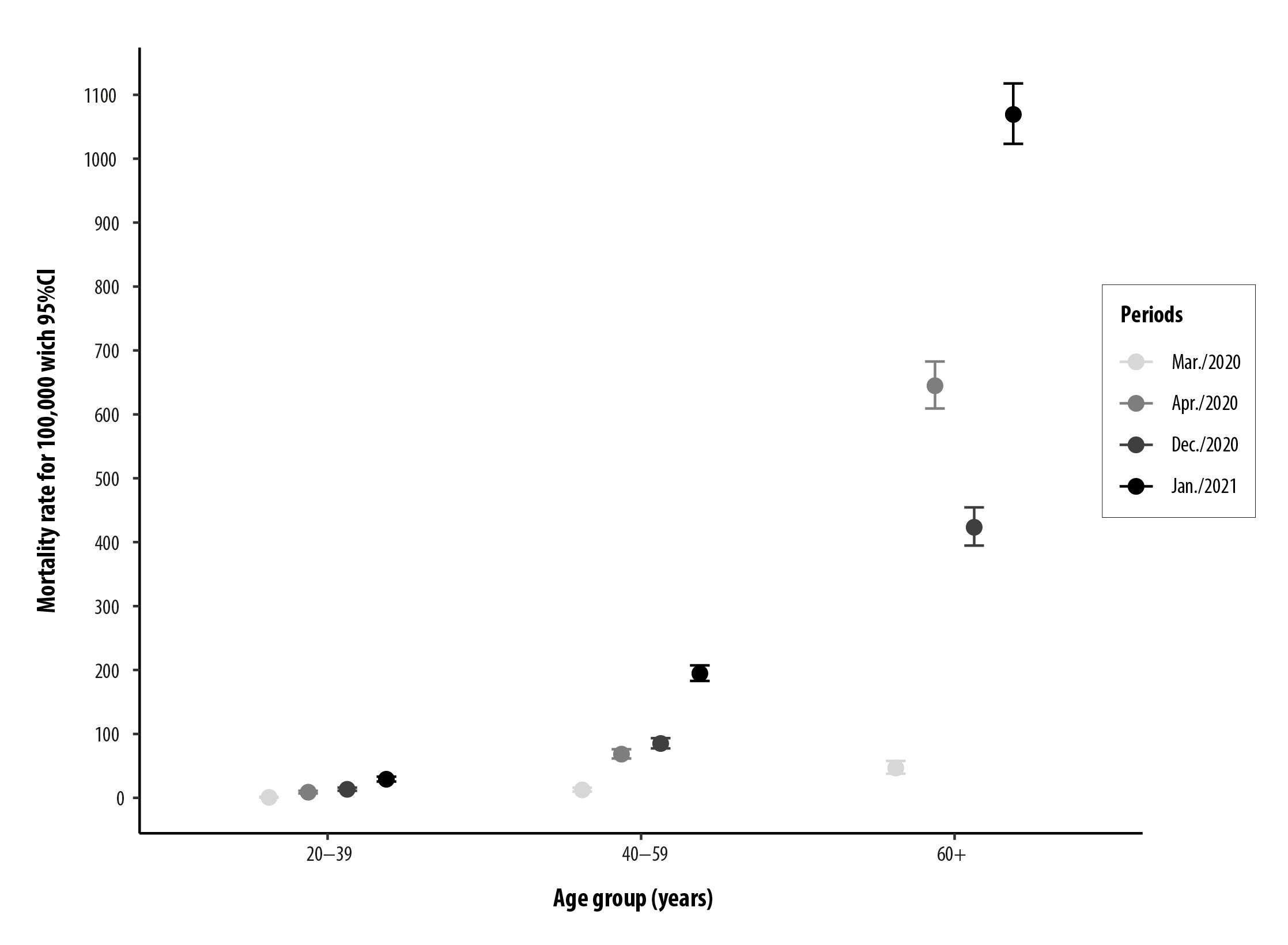
Figure 1 Mortality rate due to COVID-19 with 95% confidence interval (95%CI), according to the month of symptom onset and age group, Manaus, Amazonas, Brazil, 2020-2021
The ratio between total deaths in January 2021 and April 2020 resulted in an excess deaths of 99.0% (95%CI 87.0;111.0) in January 2021.
In-hospital case fatality ratio (Table 1) and ICU case fatality ratio (Table 2) in Manaus, during the months of peaks of mortality in the first and second waves, were similar to individuals aged 20-39 and those aged 40-59 years. Among the elderly - aged 60 years and older - in January 2021 (n=1,534), in-hospital case fatality ratio was lower compared to April 2020 (n=1,104): 62.1% (95%CI 59.1;65.2) and 72.9% (95%CI 70.1;75.7), respectively. ICU case fatality ratio in January 2021 (n=477) was also lower compared to April 2020 (n=456): 78.5% (95%CI 76.0;80.9) and 88.4% (95%CI 86.4;90.4), respectively.
In-hospital case fatality ratio in Manaus was lower during the months preceding the peaks of mortality in the first and second waves, as well as in December 2020 in those aged 60 years and older, when compared to the case fatality ratio in March and April 2020 (Figure 2).
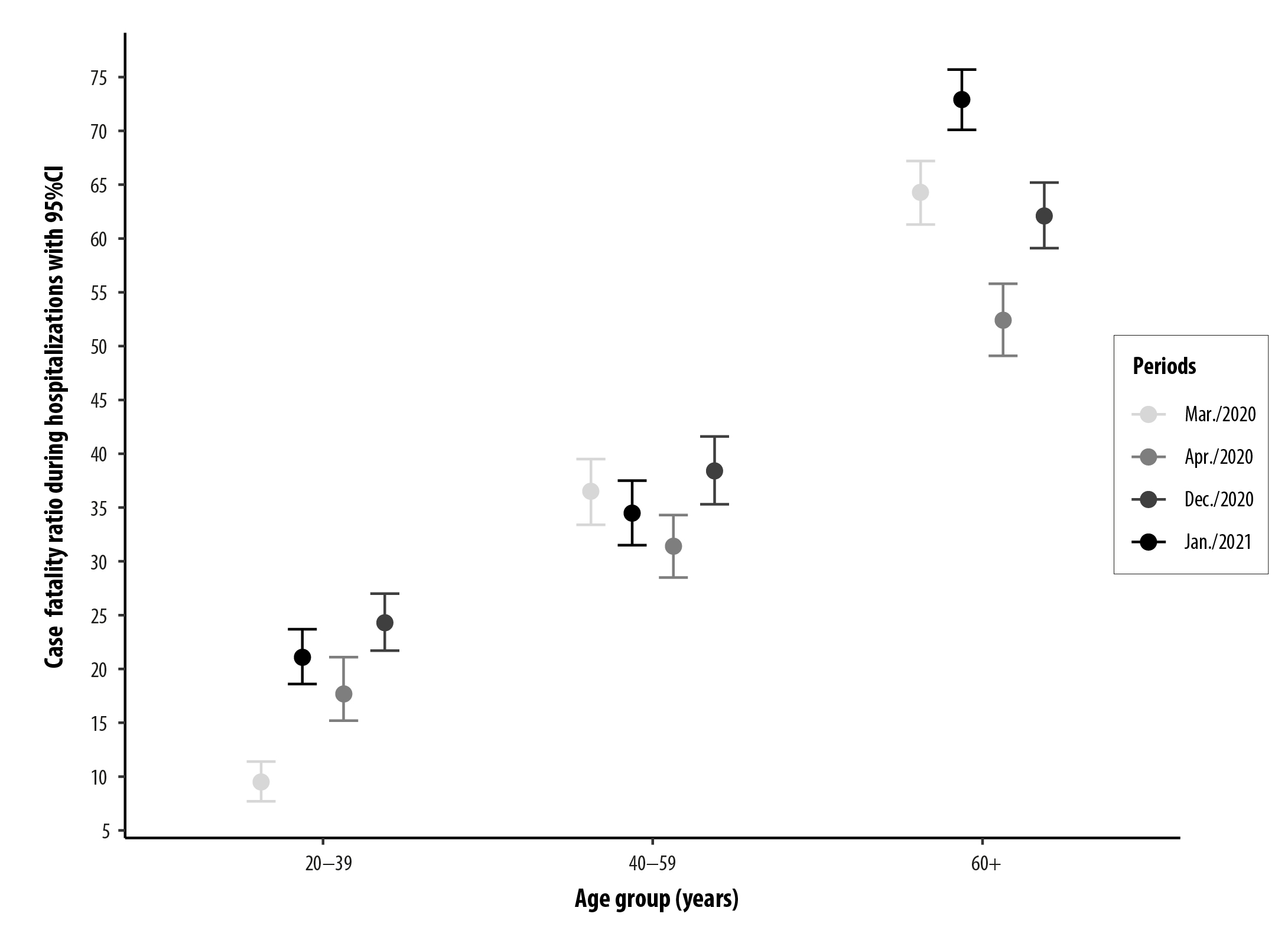
Figure 2 Case fatality ratio during hospitalization with 95% confidence interval (95%CI), according to the month of symptom onset and age group, Manaus, Amazonas, Brazil, 2020-2021
During the months preceding the peaks of mortality, in Manaus, both in the first and second waves, ICU case fatality ratio did not differ among age groups (Figure 3), except for those aged 20-39 years, with case fatality ratio ranging from 45.5% (95%CI 42.4;48.5) in March (n=5) to 56.5% (95%CI 53.3;59.7) in April 2020 (n=39), and from 50.5% (95%CI 47.3;53.7) in December 2020 (n=49) to 57.2% (95%CI 54.1;60.4) in January 2021 (n=107). In those aged 60 years and older, ICU case fatality ratio was lower in January 2021 (79.9%; 95%CI 77.4;82.5), compared to April 2020 (88.2%; 95%CI 86.1;90.3).
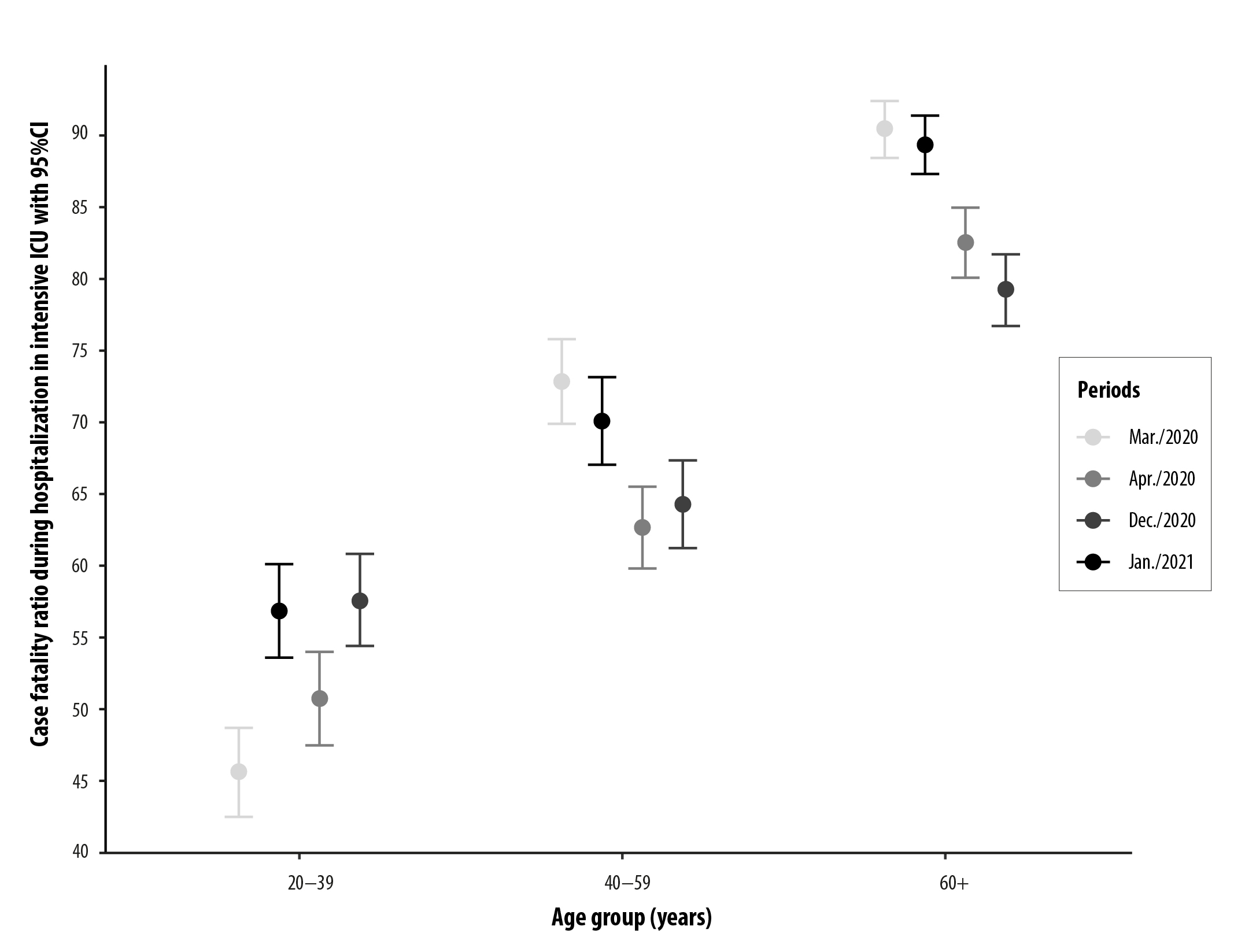
Figure 3 Case fatality ratio during hospitalization in intensive care unit (ICU) with 95% confidence interval (95%CI), according to the month of symptom onset and age group, Manaus, Amazonas, Brazil, 2020-2021
In São Paulo, Porto Alegre and Curitiba, the pattern of in-hospital case fatality ratio was the same as that observed in Manaus (Table 1), with a decrease among those aged 60 years and older in January 2021. In São Paulo, case fatality ratio ranged from 41.0% (95%CI 37.9;44.2) in May 2020 (n=2,804) to 34.5% (95%CI 31.5;37.5) in January 2021 (n=1,430). In Porto Alegre, case fatality ratio ranged from 48.6% (95%CI 45.5;51.7) in July 2020 (n=335) to 42.1% (95%CI 38.9;45.0) in January 2021 (n=207). In Curitiba, case fatality ratio ranged from 43.4% (95%CI 40.3;46.6) in July 2020 (n=400) to 33.4% (95%CI 30.4;36.4) in January 2021 (n=259).
Table 1 Case fatality ratio during hospitalization, according to month of symptom onset and age group, in the Brazilian state capitals Manaus, São Paulo, Porto Alegre and Curitiba, 2020-2021
| Age group (years) | Deaths (n) | Case fatality ratio (95%CI a) | Deaths (n) | Case fatality ratio (95%CI a) |
|---|---|---|---|---|
| Manaus | ||||
| Apr./2020 | Jan./2021 | |||
| 20-39 | 67 | 21.1 (18.6;23.7) | 185 | 24.3 (21.7;27.0) |
| 40-59 | 314 | 34,5 (31.5;37.5) | 825 | 38.4 (35.3;41.6) |
| ≥60 | 1,104 | 72.9 (70.1;75.7) | 1,534 | 62.1 (59.1;65.2) |
| São Paulo | ||||
| May/2020 | Jan./2021 | |||
| 20-39 | 127 | 6.9 (5.3;8.5) | 52 | 6.9 (5.3;8.6) |
| 40-59 | 707 | 15.4 (13.2;17.7) | 314 | 14.0 (11.8;16.2) |
| ≥60 | 2,804 | 41.0 (37.9;44.2) | 1,430 | 34.5 (31.5;37.5) |
| Porto Alegre | ||||
| Jul./2020 | Jan./2021 | |||
| 20-39 | 9 | 7.5 (5.8;9.2) | 3 | 5.6 (4.1;7.0) |
| 40-59 | 42 | 12.9 (10.8;15.1) | 40 | 19.2 (16.7;21.8) |
| ≥60 | 335 | 48.6 (45.5;51.7) | 207 | 42.1 (38.9;45.0) |
| Curitiba | ||||
| Jul./2020 | Jan./2021 | |||
| 20-39 | 16 | 6.7 (5.1;8.2) | 9 | 6.7 (5.1;8.3) |
| 40-59 | 109 | 16.9 (14.6;19.3) | 63 | 13.3 (11.2;15.4) |
| ≥60 | 400 | 43.4 (40.3;46.6) | 259 | 33.4 (30.4;36.4) |
a) 95%CI: 95% confidence interval, based on percentile bootstrap.
In São Paulo, ICU case fatality ratio was lower among the age groups 40-59 and 60 years and older, in January 2021 (Table 2); in Porto Alegre, it was lower among individuals aged 20-39 and higher in those aged 40-59 years. In Curitiba, regardless of age group, the case fatality ratio due to COVID-19 among people in ICU were similar in July 2020 and January 2021.
Table 2 Case fatality ratio during hospitalization in intensive care unit (ICU), according to month of symptom onset and age group, in the Brazilian state capitals Manaus, São Paulo, Porto Alegre and Curitiba, 2020-2021
| Age group (years) | Deaths (n) | Case fatality ratio (95%CI a) | Deaths (n) | Case fatality ratio (95%CI a) |
|---|---|---|---|---|
| Manaus | ||||
| Apr./2020 | Jan./2021 | |||
| 20-39 | 39 | 56.5 (53.4;59.7) | 107 | 57.2 (54.0; 60.4) |
| 40-59 | 169 | 69.5 (66.5;72.5) | 400 | 63.8 (60.0; 66.8) |
| ≥60 | 456 | 88.4 (86.4;90.4) | 477 | 78.5 (76.0; 80.9) |
| São Paulo | ||||
| May/2020 | Jan./2021 | |||
| 20-39 | 87 | 18.8 (16.4;21.3) | 37 | 14.4 (12.3;16.5) |
| 40-59 | 462 | 37.2 (34.1;40.2) | 240 | 29.1 (26.3;31.9) |
| ≥60 | 1,596 | 64.6 (61.6;67.7) | 898 | 53.5 (50.4;56.7) |
| Porto Alegre | ||||
| Jul./2020 | Jan./2021 | |||
| 20-39 | 8 | 40.0 (36.9;43.1) | 2 | 8.3 (6.5;10.2) |
| 40-59 | 35 | 33.7 (30.8;36.5) | 32 | 42.1 (39.0;45.3) |
| ≥60 | 224 | 69.6 (66.8;72.3) | 158 | 66.9 (63.9;70.0) |
| Curitiba | ||||
| Jul./2020 | Jan./2021 | |||
| 20-39 | 12 | 18.2 (15.7;20.6) | 6 | 17.1 (14.8;19.5) |
| 40-59 | 85 | 42.5 (39.4;45.6) | 49 | 47.1 (44.0;50.2) |
| ≥60 | 266 | 66.8 (64.0;69.7) | 152 | 65.8 (62.8;68.8) |
a) 95%CI: 95% Confidence Interval, based on percentile bootstrap.
Discussion
This is the first study aimed at describing hospital and ICU case fatality ratio due to COVID-19, in scenarios with and without circulation of the Gamma variant. The results presented on in-hospital and ICU case fatality ratios in the four metropolises evaluated suggest that the collapse of the healthcare system in Manaus may have determined the increase in mortality rates due to COVID-19, a possible indirect consequence of the strong circulation of the Gamma variant.
In Manaus, the significant difference among the magnitude of mortality rates due to COVID-19 in the months preceding the collapse that occurred in both April 2020 and January 2021 suggests greater uncontrolled community transmission of SARS-CoV-2 in December 2020, probably related to neglect of health measures by decision-makers and the general population, as well as the emergence of the variant of concern, Gamma, associated with increased transmissibility.3,4
In Manaus, the mortality rate was higher in January 2021, and individuals aged 60 years and older were the most affected. This finding corroborates the results of previous studies in the literature on the subject, which also present higher mortality in the elderly.21 The significant increase in the mortality rate in January 2021, compared to April 2020, was more expressive in the age group 40-59 years, compared to the elderly, possibly related to the disproportionate excess mortality among those aged 60 years and older during the first wave. An analysis of the mortality profile, before and after the emergence of the Gamma variant in Amazonas, also found higher mortality rates due to COVID-19 in January 2021, especially in individuals aged 40 to 59 years.12
Among those who presented the first symptoms of the disease in January 2021, mortality was approximately twice higher than that observed in those who presented the first symptoms of COVID-19 in April 2020, showing exponential excess mortality during the second wave, in Manaus.
In the capital city of Amazonas, both in-hospital and ICU case fatality ratios were similar to those aged 20-39 years, in January 2021 and April 2020. However, it could be seen that, although there was no significant difference regarding in-hospital case fatality ratio, the specific estimates in the age groups 20-39 and 40-59 years were higher in January 2021 when compared to those in April 2020, a pattern different from that of ICU case fatality ratio.
It is possible that in Manaus, the pattern of ICU case fatality ratio has not been replicated for the indicator of in-hospital case fatality ratio, given the differences in the rhythm and quantity of open beds in both situations: between December 10, 2020 and January 31, 2021, the number of hospital beds ranged from 32422 to 1,954,17 representing an increase of 500%, while the number of ICU beds ranged from 19322 to 691,17 that is, a smaller increase than that of hospital beds. Therefore, the significant increase in the number of hospital beds in Manaus may have limited not only the quantity of human resources available, but also the quality of care provided, as observed in other contexts.7,8
It is worth noting that, although in-hospital case fatality ratio patterns among the ages of 20-39 and 40-59 years were similar in São Paulo, Porto Alegre and Curitiba, at different times of the epidemic, the percentages tended to be lower in January 2021, in general, which may be related to the lower severity of the epidemic in January 2021, compared to the most critical months of 2020. In addition, in-hospital and ICU case fatality ratios were consistently and significantly lower in those capitals, compared to Manaus, a result possibly related to regional inequalities in access to healthcare, taking into consideration the Brazilian context.14,23
It is worth highlighting the fact that in-hospital case fatality ratio among those aged 60 years and older was lower in January 2021, regardless of the capital evaluated; and especially in Manaus, whose healthcare system had collapsed at that time, under strong pressure from the Gama variant.2-4 The decline in COVID-19 case fatality ratio among the elderly may be associated with greater health care adherence by this age group and/or lower exposure to the virus, given the strong impact of the pandemic on those aged 60 years and older in 2020, a cause of great concern.
In Manaus, ICU case fatality ratio was significantly lower in January 2021, when compared to April 2020, among those aged 60 years and older. In São Paulo, a consistent pattern of significant reduction in ICU case fatality ratio could be seen in January 2021, compared to May 2020. In Porto Alegre and Curitiba, in general, the pattern of ICU case fatality ratio was similar, regardless of the period evaluated.
With regard to Manaus, another fact highlighted in this study is related to both in-hospital and ICU case fatality ratio, where the consistently lower values in the months preceding the collapse that occurred during the first and second waves, suggests, as observed in other contexts, that the tendency of case fatality in individuals hospitalized due to COVID-19 was higher in periods when the healthcare system was overwhelmed or when it collapsed. 7,23-25
Regarding Manaus, both in-hospital and ICU case fatality ratios among those aged 40-59 and 60 years or older were lower in December 2020, when compared to the ratios occurred in March and April 2020, suggesting that case fatality ratio - even with the probable circulation of the Gamma variant since November 2020 and having reached around 52.0% of the samples with genomic sequencing in December 202026 - would tend to be lower during the second wave, if the healthcare system saturation had not been so significant in January 2021, when 85.0% of the samples with genomic sequencing were associated with the Gamma variant.26 This is a valid hypothesis, if we observe the reasonably lower pattern of in-hospital and ICU case fatality ratios in São Paulo, Curitiba and Porto Alegre in January 2021, possibly influenced not only by the reduction in the pressure of community transmission of SARS-COV-2 on health services, but also by the progress related to the therapy and clinical management of severe COVID-19, as observed worldwide.27
As limitations of the study, it is important to highlight its descriptive pattern and the absence of records with information on the etiological diagnosis of COVID-19 attributed to the Gama variant, which would allow a detailed evaluation of case fatality ratio. Data coverage and quality may have been affected, given the pandemic moment, especially in Manaus, where the health system collapsed twice, leading not only to a possible reduction in the number of hospitalizations and deaths due to COVID-19, but also to less reliable records.28 Moreover, each hospitalization record was counted as an independent admission, something that may not be always certain and safe taking into consideration that readmissions are possible, and the frequency of these readmissions is not necessarily constant.
This study has as a strong point the fact of having evaluated in-hospital case fatality ratio in Manaus, during the epidemic phases with and without strong circulation of the Gamma variant, as well as in metropolises little or barely affected by this variant. The exponential pattern of mortality, in December 2020 and January 2021, not only reinforces that the Gamma variant may have begun to circulate in Manaus before December 2020, but also that its rapid dissemination may have indirectly contributed to the increase in mortality due to COVID-19. This result is in line with studies that have showed the increase in mortality associated with overwhelmed healthcare systems in different regions of the world,7,8 as well as recent notes from a panel of experts that make a possible association between the Gama variant and increase in hospital admissions, without confirmation of an increase in the severity of the disease or in risk of mortality.29,30
Taking into consideration the results presented, we suggest that the collapse of the healthcare system in Manaus may have determined the increase in mortality rates due to COVID-19, as a consequence of the strong circulation of the Gama variant, associated with higher transmissibility. It can be concluded that in January 2021, in-hospital and ICU case fatality ratios decreased or remained stable in the four state capitals analyzed, especially in Manaus and during the epidemic peak with the prevalence of the Gama variant.
Referências
1. World Health Organization. WHO coronavirus disease (covid-19) dashboard [Internet]. [Geneva]: WHO; 2021]; [citado 20 out. 2021]. Disponível em: https://covid19.who.int/ [ Links ]
2. Taylor L. Covid-19: Brazil breaks record daily death toll as crisis spreads through South America. BMJ. 2021;373:n930. doi: https://doi.org/10.1136/bmj.n930. [ Links ]
3. Brazilian Society of Tropical Medicine. Manaus: chaotic picture and successive records of infections by the new coronavirus [Internet]. Brasília, DF: BSTM; 2021 [citado 13 jul 2021]. Disponível em: https://www.sbmt.org.br/portal/manaus-cenario-caotico-e-recordes-sucessivos-de-infeccoes-pelo-novo-coronavirus/?locale=en-US&lang=en [ Links ]
4. Naveca FG, Nascimento V, Souza VC, Corado AL, Nascimento F, Silva G, et al. COVID-19 in Amazonas, Brazil, was driven by the persistence of endemic lineages and P.1 emergence. Nat Med. 2021;27(7):1230-8. doi: https://doi.org/10.1038/s41591-021-01378-7. [ Links ]
5. Volz E, Mishra S, Chand M, Barrett JC, Johnson R, Geidelberg L, et al. Assessing transmissibility of SARS-CoV-2 lineage B.1.1.7 in England. Nature. 2021;593(7858):266-9. doi: https://doi.org/10.1038/s41586-021-03470-x. [ Links ]
6. Martins AF, Zavascki AP, Wink PL, Volpato FCZ, Monteiro FL, Rosset C, et al. Detection of SARS-CoV-2 lineage P.1 in patients from a region with exponentially increasing hospitalisation rate, february 2021, Rio Grande do Sul, Southern Brazil. Euro Surveill. 2021;26(12):2100276. doi: https://doi.org/10.2807/1560-7917.ES.2021.26.12.2100276. [ Links ]
7. Olivas-Martínez A, Cárdenas-Fragoso JL, Jiménez JV, Lozano-Cruz OA, Ortiz-Brizuela E, Tovar-Méndez VH, et al. In-hospital mortality from severe COVID-19 in a tertiary care center in Mexico City; causes of death, risk factors and the impact of hospital saturation. PLoS One. 2021;16(2):e0245772. doi: https://doi.org/10.1371/journal.pone.0245772. [ Links ]
8. Rossman H, Meir T, Somer J, Shilo S, Gutman R, Arie AB, et al. Hospital load and increased covid-19 related mortality in Israel. Nat Commun. 2021 Mar 26;12(1):1904. doi: https://doi.org/10.1038/s41467-021-22214-z. [ Links ]
9. Graham MS, Sudre CH, May A, Antonelli M, Murray B, Varsavsky T, et al. Changes in symptomatology, reinfection, and transmissibility associated with the SARS-CoV-2 variant B.1.1.7: an ecological study. Lancet Public Health. 2021;6(5):e355-45. doi: https://doi.org/10.1016/S2468-2667(21)00055-4. [ Links ]
10. Davies NG, Jarvis CI, CMMID COVID-19 Working Group; Edmunds WJ, Jewell NP, Diaz-Ordaz K, et al. Increased mortality in community-tested cases of SARS-CoV-2 lineage B.1.1.7. Nature. 2021;593(7858):270-4. doi: https://doi.org/10.1038/s41586-021-03426-1. [ Links ]
11. Frampton D, Rampling T, Cross A, Bailey H, Heaney J, Byott M, et al. Genomic characteristics and clinical effect of the emergent SARS-CoV-2 B.1.1.7 lineage in London, UK: a whole-genome sequencing and hospital-based cohort study. Lancet Infect Dis. 2021;21(9):1246-56. doi: https://doi.org/10.1016/S1473-3099(21)00170-5. [ Links ]
12. Freitas ARR, Beckedorff OA, Cavalcanti LPG, Siqueira AM, Castro DB, Costa CF, et al. A emergência da nova variante P.1 do SARS-CoV-2 no Amazonas (Brasil) foi temporalmente associada a uma mudança no perfil da mortalidade devido a covid-19, segundo sexo e idade. SciELO Preprints. 26 mar. 2021. doi: https://doi.org/10.1590/SciELOPreprints.2030. [ Links ]
13. Ministério da Saúde (BR). Banco de dados de síndrome respiratória aguda grave: incluindo dados da covid-19 [Internet]. Brasília, DF: MS; 2020 [citado 12 jul 2021]. Disponível em: https://opendatasus.saude.gov.br/dataset/bd-srag-2020 [ Links ]
14. Ranzani OT, Bastos LSL, Gelli JGM, Marchesi JF, Baião F, Hamacher S, et al. Characterisation of the first 250 000 hospital admissions for covid-19 in Brazil: a retrospective analysis of nationwide data. Lancet Respir Med. 2021;9(4):407-18. https://doi.org/10.1016/S2213-2600(20)30560-9. [ Links ]
15. Codeço CT, Cruz OG, Gomes MFC, Villela D, Carvalho LM, Coelho FC, et al. Atualização parcial InfoGripe semana 14 [Internet]. [citado 14 de abril de 2021]. Disponível em: https://gitlab.procc.fiocruz.br/mave/repo/-/tree/master/Boletins%20do%20InfoGripe/Imagens/Capitais [ Links ]
16. Orellana JDY, Marrero L, Horta BL. Excesso de mortes por causas respiratórias em oito metrópoles brasileiras durante os seis primeiros meses da pandemia de covid-19. Cad Saude Publica. 2021;37(5):e00328720. doi: https://doi.org/10.1590/0102-311X00328720. [ Links ]
17. Governo do Estado do Amazonas. Boletim diário covid-19 no Amazonas: 31 janeiro 2021 [Internet]. Manaus, AM: FVS; 2021 [citado 12 jul 2021]. Disponível em: https://www.fvs.am.gov.br/media/publicacao/31_01_21_BOLETIM_DIÁRIO_DE_CASOS_COVID-19.pdf [ Links ]
18. Chernick MR, LaBudde RA. An introduction to bootstrap methods with applications to R. Hoboken, NJ: John Wiley & Sons; 2014. [ Links ]
19. Prado MF, Antunes BBP, Bastos LSL, Peres IT, Silva AAB, Dantas LF, et al. Analysis of covid-19 under-reporting in Brazil. Rev Bras Ter Intensiva. 2020;32(2):224-8. doi: https://doi.org/10.5935/0103-507x.20200030. [ Links ]
20. Castro MC, Gurzenda S, Turra CM, Kim S, Andrasfay T, Goldman N. Reduction in life expectancy in Brazil after covid-19. Nat Med. 2021;27(9):1629-35. doi: https://doi.org/10.1038/s41591-021-01437-z. [ Links ]
21. Mascarello KC, Vieira ACBC, Souza ASS, Marcarini WD, Barauna VG, Maciel ELN. Hospitalização e morte por covid-19 e sua relação com determinantes sociais da saúde e morbidades no Espírito Santo: um estudo transversal. Epidemiol Serv Saude. 2021;30(3):e2020919. doi: https://doi.org/10.1590/S1679-49742021000300004. [ Links ]
22. Governo do Estado do Amazonas. Boletim diário covid-19 no Amazonas: 10 de dezembro de 2020 [Internet]. Manaus, AM: FVS; 2021 [citado 12 jul 2021]. Disponível em: https://www.fvs.am.gov.br/media/publicacao/10_12_20_BOLETIM_DIÁRIO_DE_CASOS_COVID-19_1.pdf [ Links ]
23. Baqui P, Bica I, Marra V, Ercole A, van der Schaar M. Ethnic and regional variations in hospital mortality from covid-19 in Brazil: a cross-sectional observational study. Lancet Glob Health. 2020;8(8):e1018-26. doi: https://doi.org/10.1016/S2214-109X(20)30285-0. [ Links ]
24. Lemos DRQ, D'Angelo SM, Farias LABG, Almeida MM, Gomes RG, Pinto GP, et al. Health system collapse 45 days after the detection of COVID-19 in Ceará, Northeast Brazil: a preliminary analysis. Rev Soc Bras Med Trop. 2020; 53:(e20200354). doi: https://doi.org/10.1590/0037-8682-0354-2020 [ Links ]
25. Chaudhry R, Dranitsaris G, Mubashir T, Bartoszko J, Riazi S. A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on covid-19 mortality and related health outcomes. EClinicalMedicine. 2020;25:100464. doi: https://doi.org/10.1016/j.eclinm.2020.100464. [ Links ]
26. Dejnirattisai W, Zhou D, Supasa P, Liu C, Mentzer AJ, Ginn HM, et al. Antibody evasion by the P.1 strain of SARS-CoV-2. Cell. 2021 May 27;184(11):2939-54. doi: https://doi.org/10.1016/j.cell.2021.03.055.. [ Links ]
27. Finelli L, Gupta V, Petigara T, Yu K, Bauer KA, Puzniak LA. Mortality Among US Patients Hospitalized With SARS-CoV-2 Infection in 2020. JAMA Netw Open. 2021 Apr 1;4(4):e216556. doi: https://doi.org/10.1001/jamanetworkopen.2021.6556. [ Links ]
28. Fernández-Fontelo A, Moriña D, Cabaña A, Arratia A, Puig P. Estimating the real burden of disease under a pandemic situation: the SARS-CoV2 case. PLoS One. 2020 Dec 3;15(12):e0242956. doi: https://doi.org/10.1371/journal.pone.0242956. [ Links ]
29. Funk T, Pharris A, Spiteri G, Bundle N, Melidou A, Carr M, et al. Characteristics of SARS-CoV-2 variants of concern B.1.1.7, B.1.351 or P.1: data from seven EU/EEA countries, weeks 38/2020 to 10/2021. Euro Surveill. 2021;26(16):2100348. doi: https://doi.org/10.2807/1560-7917.ES.2021.26.16.2100348. [ Links ]
30. World Health Organization. Listings of WHO's response to covid-19 [Internet]. Geneva: WHO 2021 [citado 12 jul 2021]. Disponível em: https://www.who.int/news/item/29-06-2020-covidtimeline [ Links ]
Received: July 27, 2021; Accepted: September 30, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
