










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.4 Brasília dez. 2021 Epub 29-Nov-2021
http://dx.doi.org/10.1590/s1679-49742021000400025
Original Article
Evolution of COVID-19 in Santa Catarina, Brazil: state decrees and epidemiological indicators up until August 2020*
1Universidade Federal de Santa Catarina, Curso de Graduação em Medicina, Florianópolis, SC, Brazil
2Universidade Federal de Santa Catarina, Programa de Pós-Graduação em Saúde Coletiva, Florianópolis, SC, Brazil
Objective
To describe the evolution of decrees and indicators related to COVID-19 in Santa Catarina, Brazil, up until August 2020.
Methods
This was an ecological study that analyzed epidemiological indicators and state decrees on social distancing. The decrees were grouped into restriction, maintenance and relaxation. The indicators were mortality, incidence and transmissibility.
Results
179,443 cases and 2,183 deaths were recorded in the period. The incidence rate went from 20.4 cases per 100,000 inhabitants in March to 642.2 in August. Fifteen state decrees were issued. In August, when the highest mortality rate was observed (13.1 per 100,000 inhabitants), it was found that all decree categories, except one, had been relaxed.
Conclusion
The decrees that relaxed social distancing measures were issued early and in disagreement with the epidemiological context in the state.
Keywords: Coronavirus Infections; COVID-19; Mortality; Decrees; Legislation; Epidemiology, Descriptive
Introduction
Brazil’s first COVID-19 case was confirmed in February 2020 and its first COVID-19 death was confirmed in March of the same year.1 In January 2021, Brazil ranked third among the countries with the highest number of confirmed COVID-19 cases and in second place regarding the number of deaths, with 8,638,249 COVID-19 cases and 212,831 COVID-19 deaths.1 Results from a study that retrospectively analyzed all adult individuals hospitalized between Epidemiological Weeks 8 and 33 in 2020 point to high in-hospital COVID-19 mortality in Brazil, even among those under 60 years of age, exacerbated by regional disparities present in the public health system.2
The World Health Organization (WHO) emphasizes that public and social policies play a key role in limiting the transmission of the novel coronavirus and decreasing COVID-19 deaths.3 WHO also highlights the need for regular monitoring of indicators and continuous adjustment of SARS-CoV-2 containment measures, including those for social distancing, in keeping with the level of transmission in each country and region. Health indicators, together with the health system response capacity, should be the basis for adjustment and impact assessment, as well as a guide for future changes.3,4 Social distancing measures, such as closure of schools and shops, travel restrictions, cancellation of mass events, prohibition of crowds, among others, are part of the non- pharmaceutical measures recommended for countries to control the pandemic.5-7
In Brazil, the emergency nature of the pandemic demanded fast, cooperative and supportive action from the different governmental levels. However, the Federal Administration can be seen to have underestimated the pandemic and its effects, making systematic attempts to obstruct the norms promoted by other actors, in particular the National Congress and local governments.8,9 With the regulation of the Federal Law No. 13979, dated February 6, 2020, which, among other provisions, authorized the promotion of emergency measures of social distancing through decrees, state governors and city mayors became protagonists in the production of normative acts related to the COVID-19 pandemic in their territories.10
In Santa Catarina, Brazil’s second most southerly state, according to official data there were 549,579 confirmed cases and 5,988 deaths caused by COVID-19 as at January 2021.11 When compared to the remaining Brazilian states, in November 2020, Santa Catarina stood out with regard to the number of new cases.12 Between March and November 2020, several decrees regulated public measures for COVID-19 prevention and control, including the promotion of social distancing. A study conducted in the municipality of Florianópolis, the state capital, analyzed the relationship between the potential spread of SARS-CoV-2 and the municipal government's decision-making regarding social distancing up until July 14, 2020. The results showed divergence between the distancing measures and the epidemiological indicators at the time of the political decision.13
Considering the impact of the COVID-19 pandemic in Brazil, the considerable regional differences in the country and the high number of cases and deaths in Santa Catarina, it is necessary to evaluate, with a greater degree of detail, the state’s epidemiological context when social distancing measures were implemented, maintained and/or relaxed. This study aimed to describe the evolution of the decrees and indicators related to COVID-19 in the state of Santa Catarina, Brazil, up until August 2020.
Methods
This is an ecological study, conducted in the state of Santa Catarina. The period studied was from the 1st to the 35th Epidemiological Week of 2020, corresponding to the interval between December 29, 2019 and August 29, 2020. Confirmed COVID-19 cases and deaths of people living in the state were analyzed. Cases or deaths were considered to be those with laboratory confirmation of SARS-CoV-2, through molecular biology tests, immunological tests or antigen tests, regardless of signs or symptoms presented.14
The data source used for information on cases and deaths was the Santa Catarina state open data portal,15 retrieved on September 11th 2020. The information on the population resident in Santa Catarina was obtained from the Brazilian National Health System Information Technology Department, considering the population projection estimated for Santa Catarina in 2020. Effective reproduction rate (Rt) estimates were taken from the Rede CoVida panel,16 collected on the first day of each month. Rt is a mathematical metric that indicates how contagious a disease is. It was calculated using the case curve predicted by the mathematical case prediction model.
The following variables characterizing the epidemiological context were analyzed:
number of new cases (by symptom onset date);
number of deaths in the last 24 hours (by date of death);
mortality rate;
incidence rate;
adjusted effective reproduction rate, Rt; and
number of municipalities with cases and number of municipalities with deaths.
The data were described according to calendar months. The incidence and mortality rates were obtained by dividing the number of cases and the number of deaths in the last 24 hours, respectively, by the resident population and multiplying by 100,000. The data were analyzed using Stata software version 14.
The decrees consulted in the study were also identified on the Santa Catarina open data portal,15 and their full contents were retrieved by the Official State Gazette. The Santa Catarina state decrees that regulate matters related to Law No. 13979/2020 were analyzed. The variables analyzed in the different decrees were: number of the decree; date of its publication; date it came into force; and the social distancing measure implemented and its repercussion on the category, in relation to the previous norm. The analysis aimed to evaluate social distancing measures, and nine activity group categories were created. First, social distancing-related activities17 were selected during the analysis of the decrees which allowed greater contact between people - which could be avoided or reduced by restricting such activities. In order to create the categories, we used groupings already existing in the decrees themselves and also similar groupings found in other studies published in the literature,17,18 namely:
on-site teaching - this included all educational levels, from elementary school to university, as well as young and adult education, technical education and public training;
non-essential food and beverage businesses - this included restaurants, bars and other establishments providing non-essential food and beverages;
transport of people - this included air, land or waterborne transport;
hotels - this included hotels, guesthouses or any form of charged accommodation;
product sales businesses - this included non-food and non-essential product sales businesses in general;
essential food businesses - this included supermarkets, markets, grocery stores, bakeries, butchers and fishmongers;
staying in squares and public places - this included public spaces for collective use, such as beaches, parks and squares;
church services - this included gatherings of a religious character and masses; and
crowding - this included any norm on the matter, whether or not specifically described, provided that the term crowding was specifically mentioned.
In turn, the repercussion of the decrees on the category groups was further classified into three categories:
-
(i) Restriction
Repercussion caused by a decree the text of which contained initial restrictive measures for the category or measures with restrictive effects exceeding those in effect prior to the decree. Exceeding effects were considered to be the impact of the measure, and not period in which it was in force.
-
(ii) Maintenance
When a new decree extended restrictive measures put in place by previous decrees for a further period of time and with equal effects.
-
(iii) Relaxation
This was the case of a new decree, when the impact of the restrictions it provided for were perceived to be reduced, compared to the previous decree; or a decree that ends the period in which the previous decree was in force, without adding new restrictions to the category.
Some of the indicators were taken from the COVID-19 Risk Potential Matrix, published by the Santa Catarina State Health Department.19 By combining indicators, this matrix classifies the state’s regions into four levels of risk of infection: moderate, high, severe or very severe.19
Because public domain data was used and there was no identification of the participants, the study design was exempted from appraisal by a Human Research Ethics Committee.
Results
As at the end of Epidemiological Week 35 of 2020, there were 179,443 laboratory-confirmed COVID-19 cases and 2,183 deaths among people living in the state of Santa Catarina. In the period, the highest number of new cases was recorded in July (87,143) while the highest number of deaths was recorded in August (947). The incidence rate went from 20.4 cases per 100,000 inhabitants in March to 1,201.6/100,000 inhabitants in July and 642.2/100,000 inhabitants in August. The highest mortality rate in the period analyzed also occurred in August: 13.1 deaths per 100,000 inhab. (Table 1).
Table 1 COVID-19 indicators by month of occurrence, Santa Catarina, Brazil, up until August 2020
| Month | Casesa | Deathsb | Incidence rate (per 100,000 inhab.) | Mortality rate (per 100,000 inhab.) | Rtc (95%CId) | Municipalities with cases | Municipalities with deaths |
|---|---|---|---|---|---|---|---|
| n | n | n (%) | n (%) | ||||
| February | 30 | - | 0.4 | - | 17 (5.7) | - | |
| March | 1,483 | 5 | 20.4 | 0.1 | 116 (39.3) | 5 (1.6) | |
| April | 2,936 | 49 | 40.5 | 0.7 | 3.0 (0.7;7.8) | 180 (61.0) | 31 (10.5) |
| May | 9,698 | 95 | 133.7 | 1.3 | 1.2 (0.9;1.5) | 244 (82.7) | 57 (19.3) |
| June | 31,576 | 229 | 435.4 | 3.2 | 1.2 (0.9;1.4) | 281 (95.2) | 89 (30.1) |
| July | 87,143 | 858 | 1,201.6 | 11.8 | 1.2 (1.0;1.3) | 295 (100.0) | 162 (54.9) |
| August | 46,577 | 947 | 642.2 | 13.1 | 1.2 (1.0;1.3) | 295 (100.0) | 206 (69.8) |
| Total | 179,443 | 2,183 | 2,474.2 | 30.1 | 295 (100.0) | 295 (100.0) |
a) Number of new cases each month; b) Number of deaths recorded each month; c) Rt: adjusted effective reproduction rate, for the first day of the month; d) 95%CI: 95% confidence interval.
On April 1st, on average an infectious person produced three secondary infections (Rt=3.0). In the months that followed this indicator was 1.2. In August 2020, all the state’s 295 municipalities had reported cases of the disease, while 69.8% of them had reported deaths (Table 1).
In the period studied, 31 state decrees were issued regarding SARS-CoV-2 in Santa Catarina: three by the legislative branch and 28 by the executive branch. Among the 31 decrees examined, 15 dealt with measures for restriction, relaxation or maintenance of social distancing in relation to the activity group categories analyzed.
In March 2020, six decrees were issued, all of which either introduced restrictions or maintained existing restrictions. In April, four decrees were issued, providing seven relaxation measures in the categories analyzed, namely: non-essential food and beverage businesses (two decrees with relaxation measures for this category were issued); and hotels, product sales businesses, staying in squares and public places, church services and crowding (relaxation measures were issued for each of these categories). In June, a decree was issued relaxing measures regarding on-site teaching, transport of people and crowding. The main characteristics of three decrees issued in July and one decree issued in August were, on the one hand, maintenance of the relaxation measures and, on the other hand, restriction measures for municipalities in regions classified as having very severe potential risk according to the COVID-19 Potential Risk Matrix, published by the State Health Department. In August, practically all categories - with the exception of one - were subject to relaxation measures and no decrees imposing restrictive measures were issued (Figure 1).
Figure 1 Description of state decrees related to COVID-19 by date of publication and activity group categories, Santa Catarina, Brazil, up until August 2020
| Decree number | Date | Month published | On-site teaching | Non-essential food and beverage businesses | Transport of people | Hotels | Product sales businesses | Essential food businesses | Staying in squares and public places | Church services | Crowding |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 507 | 16/03 | March | Restriction | - | - | - | - | - | - | - | - |
| 509 | 17/03 | Restriction | Restriction | - | - | - | - | - | - | Restriction | |
| 515 | 17/03 | Maintenance | Restriction | Restriction | Restriction | Restriction | - | - | Restriction | - | |
| 521 | 19/03 | - | - | Restriction | - | - | - | Restriction | - | - | |
| 525 | 23/03 | Maintenance | Maintenance | Maintenance | Maintenance | Maintenance | Restriction | Maintenance | Maintenance | - | |
| 535 | 30/03 | Maintenance | Maintenance | Maintenance | Maintenance | Maintenance | - | - | - | - | |
| 550 | 07/04 | April | Maintenance | Maintenance | Maintenance | Maintenance | Maintenance | - | - | - | - |
| 554 | 11/04 | Maintenance | Relaxation | Maintenance | Relaxation | Maintenance | Maintenance | Maintenance | Maintenance | Restriction | |
| 562 | 17/04 | Maintenance | Maintenance | Maintenance | - | Maintenance | Maintenance | Maintenance | Maintenance | Maintenance | |
| 587 | 30/04 | Maintenance | Relaxation | Maintenance | - | Relaxation | Maintenance | Relaxation | Relaxation | Relaxation | |
| 630 | 01/06 | June | Relaxation | - | Relaxation | - | - | Maintenance | - | - | Relaxation |
| 724 | 17/07 | July | Maintenance | - | Restrictiona | - | - | - | Restrictiona | - | - |
| 740 | 24/07 | - | - | Maintenancea | - | - | - | Maintenancea | - | - | |
| 762 | 31/07 | - | - | Maintenancea | - | - | - | Maintenancea | - | - | |
| 792 | 14/08 | August | - | - | Maintenancea | - | - | - | Maintenancea | - | - |
a) Municipalities in regions with very severe potential risk, according to the COVID-19 Potential Risk Matrix, published by the Santa Catarina State Health Department.
Figure 2 shows the temporal evolution of the number of new COVID-19 cases and that of state decrees related to social distancing measures in Santa Catarina. The first decrees relaxing social distancing measures in the categories analyzed were issued in April. Decrees 554, 587 and 630 were issued between April 11th and June 1st and resulted in relaxation of measures in all the activity group categories analyzed, with the exception of ‘essential food businesses’. In the period between the publication of Decrees 554 and 630, there was an increase of 1,805% in the number of new cases per day. The first decree published after this period established restrictions on activities for municipalities in regions classified as being at extremely high risk, according to the State Health Department’s COVID-19 Potential Risk Matrix (Figure 2).
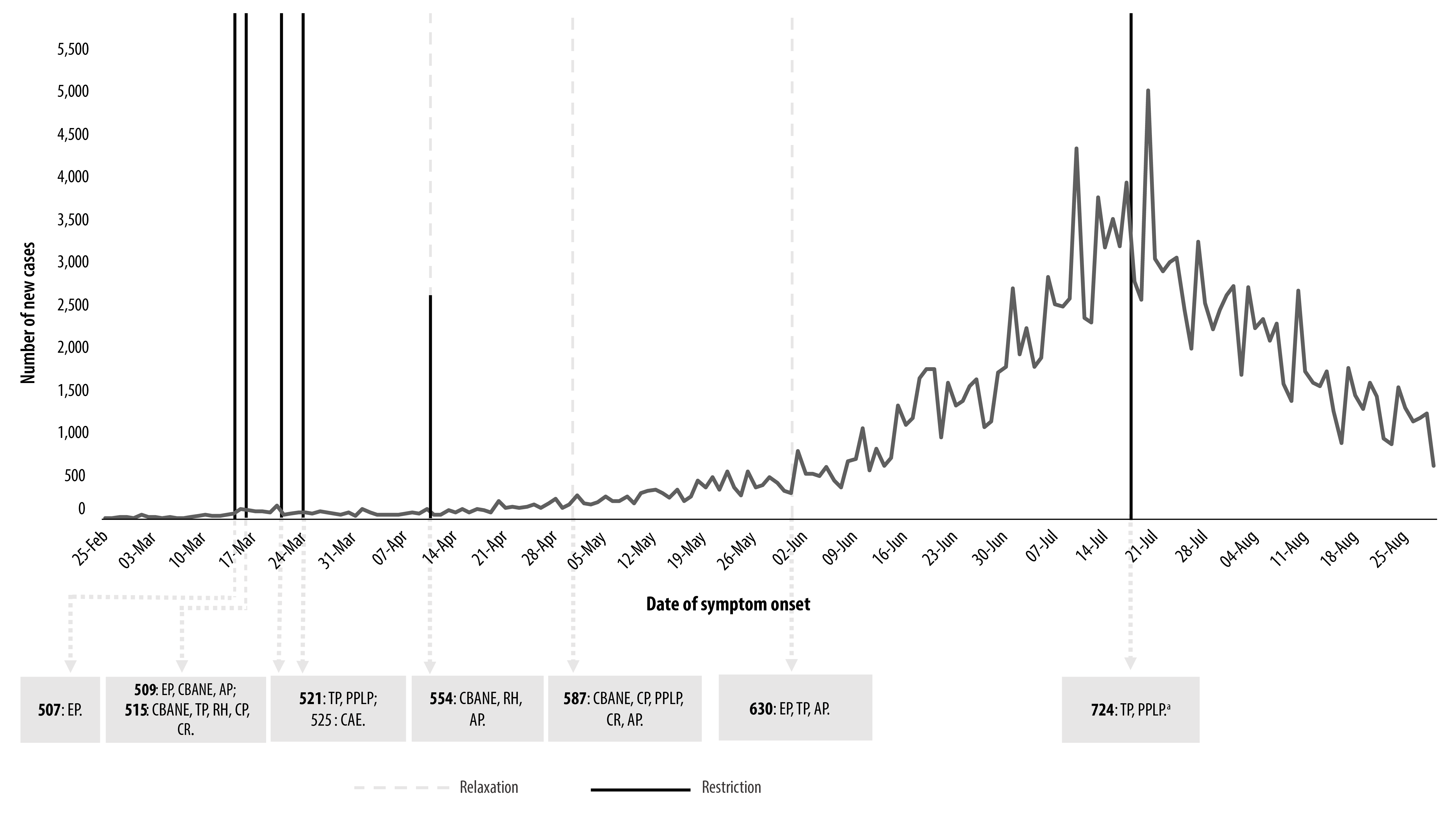
a) Municipalities in regions with very severe potential risk, according to the COVID-19 Potential Risk Matrix, published by the Santa Catarina State Health Department. Legend: EP: on-site teaching; CBANE: non-essential food and beverage businesses; TP: transport of people; RH: hotels; CP: product sales businesses; CAE: essential food businesses; PPLP: staying in squares and public places; CR: church services; AP: crowding.
Figure 2 Temporal evolution of the number of new COVID-19 cases and state decrees related to the disease that relaxed or restricted the activity group categories, Santa Catarina, Brazil, up until August 2020
Figure 3 shows the temporal evolution of the number of COVID-19 deaths in the last 24 hours, accompanied by the series of state decrees related to social distancing measures in Santa Catarina. The first five decrees restricting activities - Decrees 507, 509, 515, 521, and 525 - were published when there were still no recorded deaths due to COVID-19 in the state. In May, June, July and August 2020, in contrast to the growth in the number of deaths, no restrictive decrees were issued - with the exception of State Decree No. 724, dated July 17, 2020, referring only to municipalities in regions classified as being at extremely high risk, according to the Santa Catarina State Health Department COVID-19 Potential Risk Matrix (Figure 3).
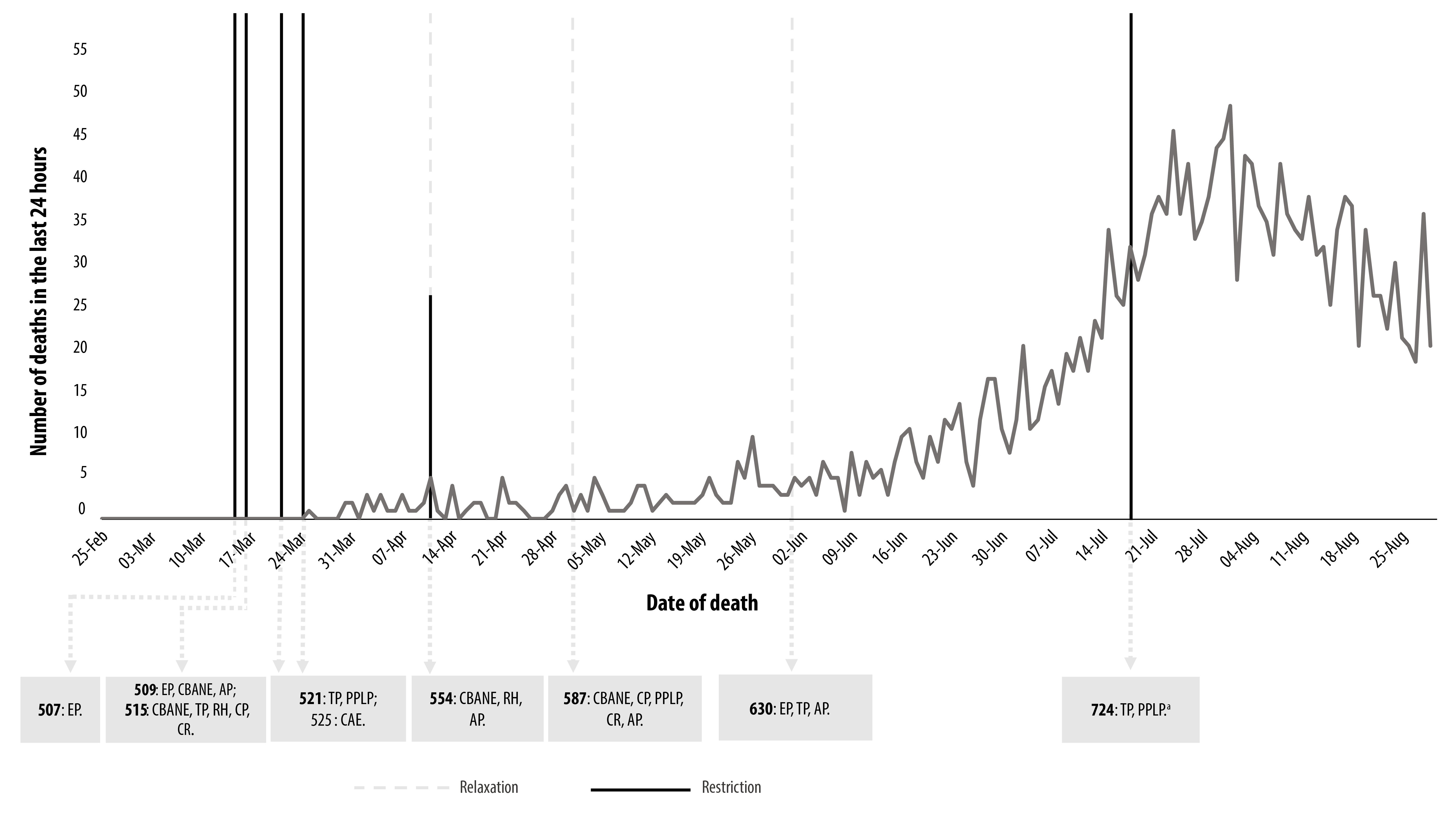
a) Municipalities in regions with very severe potential risk, according to the COVID-19 Potential Risk Matrix, published by the Santa Catarina State Health Department. Legend: EP: on-site teaching; CBANE: non-essential food and beverage businesses; TP: transport of people; RH: hotels; CP: product sales businesses; CAE: essential food businesses; PPLP: staying in squares and public places; CR: church services; AP: crowding.
Figure 3 Temporal evolution of the number of deaths in the last 24 hours and state decrees related to the disease that relaxed or restricted the activity group categories, Santa Catarina, Brazil, up until August 2020
Discussion
Between Epidemiological Weeks 1 and 35 in 2020, COVID-19 incidence and mortality rates increased in the state of Santa Catarina. In that period, the state issued 31 decrees establishing norms on matters related to SARS-CoV-2 and almost half of them had repercussions on social distancing in the categories we analyzed. In August, when the highest mortality rate for the disease was recorded in the state, measures were relaxed for all the categories analyzed, except one.
Mortality rates and incidence rates increased in the state of Santa Catarina in different proportions. Compared to other Brazilian states, Santa Catarina remained among the states with the lowest SARS-CoV-2 mortality rates in the country during the entire period studied.20 A study that described COVID-19 evolution in Brazil up until Epidemiological Week 20 indicated that Santa Catarina had the sixth lowest COVID-19 mortality rate in the country and the ninth lowest incidence rate.21 By the end of Epidemiological Week 35, the state was in 8th position in the number of confirmed COVID-19 cases22 and had the 11th highest rate in the country.20 The adjusted Rt began at 3.0 in April, dropped to 1.2 in May 2020 and remained constant at that rate until the end of the period. These figures are consistent with the national rates found in a South American study, which showed an initial Rt of 3.4 14 days after the first infection in Brazil, and an Rt of 1.2 after 90 days.23
A Brazilian project to ‘Map and analyze legal norms in response to COVID-19 in Brazil’ between January and December 2020, revealed Santa Catarina to be one of the country’s states that produced the highest number of coronavirus-related norms by April 2020.24 However, the greater number of regulations did not necessarily reflect consistency in relation to the epidemiological context of COVID-19 in the state.
In the period studied, nine of the 15 state decrees aimed at regulating social distancing in relation to the categories we studied impacted on restriction or relaxation of the activities undertaken by the category. The first five decrees preceded the first COVID-19 death in the state and had a restrictive character. The first decree went into effect in the 12th Epidemiological Week of 2020, and in just one week, all the categories had been restricted. A Brazilian study on the subject,18 dedicated to characterizing the initial social distancing measures implemented by the states, concluded that in most states social distancing measures were implemented early, considering the phase of the exponential growth curve for COVID-19 cases and deaths. The same study classified the state of Santa Catarina as being in the ‘intermediate’ category, according to the epidemiological moment in time when each state implemented its social distancing measure categories according to the number of confirmed COVID-19 cases.18 Thus, it was noted that the Santa Catarina State Government was quick to establish initial restrictions.
The importance of implementing social distancing measures early in order to contain COVID-19 has been widely discussed in the literature. Using a mathematical model, Lai et al. suggest that social distancing measures could have reduced the number of SARS-CoV-2 cases in China by 95% if they had been applied three weeks earlier than they actually were.6 Another study, this time in the United States, evaluating the effects of social distancing on the COVID-19 mortality rate in that country, suggests that after the first seven days of social distancing measure implementation, mortality rate growth decreases by around 2% per day, highlighting the importance of early implementation of social distancing measures.25
With regard to these measures being obligatory and the effects thereof, a study in the United Kingdom aimed at analyzing the impact of social distancing measures on social isolation rates and the estimated COVID-19 basic reproduction rate (Ro) found a 74% reduction in interpersonal contact and a reduction from 2.6 to 0.62 in the estimated basic reproduction rate.7 The results of a Brazilian study, which aimed to identify some of the potential determinants of levels of social distancing in the country, showed that norms imposing social distancing have more effect than perceived numbers of cases, suggesting that people respond better to norms than to the severity of the pandemic.26
Despite the consolidated importance of drafting and implementing norms regulating social distancing, Brazilian state governors have faced federative crossfire in attempting to legislate on the matter.27 In the period between the publication of state Decrees 521 and 525, the Federal Government enacted Provisional Measure 926 on March 20, 2020,28 which, among other provisions, amended Law No. 13979 enacted on February 6, 2020, with the aim of limiting the power of governors and mayors to issue decrees, giving only the Federal Administration the right to decide on certain restrictions. It should be noted that, at that moment, Law 13979/2020 had been in effect for 14 days, and all the country’s 26 states and its Federal District had already issued decrees regulating it.18 The alteration proposed by Provisional Measure 926/2020 therefore became the object of a law suit filed with the Federal Supreme Court alleging its unconstitutionality (ação direta de inconstitucionalidade - ADI).28 On March 24, 2020, the Federal Supreme Court partly granted the request for an injunction made in ADI 6341, so as to recognize concurrent competency between states, municipalities and the Federal Administration in taking normative and administrative measures to address the novel coronavirus.28 Because of this ruling, state and municipal governments therefore had their constitutional right to legislate on public health ensured.
The timing of the issuing of decrees is as important as their contents in slowing down the number of COVID-19 cases and deaths.6,29 Among the impacts of the decrees issued by the state of Santa Catarina between Epidemiological Week 1 and 35, relaxation measures require special attention, given the time at which they were implemented. Between April 11 and June 1, 2020, three relaxation decrees were issued, concomitantly with 1,804.8% growth in the absolute number of new COVID-19 cases.
Regarding the timing of social distancing measure relaxation, it is considered too early to relax restrictions before an effective reproduction rate (Rt) below 1.0 is reached.30 As such, all the relaxation measures decreed by the state of Santa Catarina, including the issuing of Decrees 554, 587 and 630, occurred early, since the Rt found at those times was 1.2.16 Added to this is the fact that the relaxation of measures in the state took place abruptly, in disagreement with what is recommended in the literature.5,29
New restrictions were established only by the last four decrees issued during the period analyzed; and even then they were only partial restrictions. They applied to the ‘transport of people’ and ‘staying in squares and public places’ categories, and only required social distancing in municipalities in regions considered to be at very severe potential risk. Those decrees were issued between epidemiological weeks 29 and 33, when the state of Santa Catarina faced the worst epidemiological moment of the period evaluated, had the highest number of new COVID-19 cases in the Southern region and reached the fourth highest number of new cases in Brazil, as at Epidemiological Week 31.20
Effectively, between June 1, 2020 and the end of the period studied, total relaxation was found to have occurred in relation to six out of the nine activity categories analyzed, despite the increasing mortality and incidence rates in the state of Santa Catarina. These findings are consistent with the results of other Brazilian studies, which found inadequacies in the relaxation of social distancing measures in the light of epidemiological data.16
This study has potential limitations, inherent to its epidemiological design and the data sources consulted. The choice of using secondary data, both for the identification of COVID-19 cases and COVID-19 deaths, subjects the results to (i) the influence of the availability of tests for laboratory diagnosis in Santa Catarina over the period, (ii) the quality of the filling out of investigation forms and (iii) the comprehensiveness of the health information systems involved in the notification of outpatient and inpatient cases, namely the, e-SUS VE and the Influenza Epidemiological Surveillance systems. In addition, municipal decrees and other forms of legislation were not subject to analysis in this study.
In conclusion, in the state of Santa Catarina there was growth in the number of COVID-19 cases and deaths, as well as in the COVID-19 incidence and mortality rates until Epidemiological Week 35, 2020, accompanied by a rise in the incidence and mortality rates in the period studied. The decrees that relaxed social distancing measures, recommended to contain transmission and reduce COVID-19 morbidity and mortality, were issued early, at odds with the epidemiological context of infection in the state of Santa Catarina.
REFERENCES
1. Johns Hopkins Coronavirus Resource Center. COVID-19 Map [Website]. 2021 [citado em 26 jan 2021]. Disponível em: https://coronavirus.jhu.edu/map.html [ Links ]
2. Ranzani OT, Bastos LSL, Gelli JGM, Marchesi JF, Baião F, Hamacher S, et al. Characterisation of the first 250 000 hospital admissions for COVID-19 in Brazil: a retrospective analysis of nationwide data. Lancet Respiratory Medicine. 2021;15:S2213-2600(20)30560-9. doi: https://doi.org/10.1016/S2213-2600(20)30560-9. [ Links ]
3. World Health Organization. Considerations for implementing and adjusting public health and social measures in the context of COVID-19: interim guidance, 4 November 2020. Geneva: WHO; 2020 [acesso 19 out. 2021]. Disponível em: https://apps.who.int/iris/handle/10665/336374. [ Links ]
4. Viana N. Gestão estadual do SUS: avaliação da transparência. In: Santos AO, Lopes LT, organizadores. Competências e regras [Internet]. Brasília, DF: CONASS; 2021 [acesso 20 out. 2021]. (Coleção covid-19, vol. 3). p. 188-207. Disponível em: https://www.conass.org.br/biblioteca/volume-3-competencias-e-regras/ [ Links ]
5. Organização Pan-Americana de Saúde. Medidas não farmacológicas para a redução da disseminação do vírus. Brasília, DF: OPAS; [2020] [acesso 21 jan. 2021]. Disponível em: https://opascovid.campusvirtualsp.org/covid-19/medidas-nao-farmacologicas-para-reducao-da-disseminacao-do-virus [ Links ]
6. Lai S, Ruktanonchai NW, Zhou L, Prosper O, Luo W, Floyd JR, et al. Effect of non- pharmaceutical interventions to contain covid-19 in China. Nature. 2020;585(7825):410-3. doi: https://doi.org/10.1038/s41586-020-2293-x. [ Links ]
7. Jarvis CI, Van Zandvoort K, Gimma A, Prem K, Klepac P, CMMID COVID-19 working group, et al. Quantifying the impact of physical distance measures on the transmission of covid-19 in the UK. BMC Medicine. 2020;18(1):154. doi: https://doi.org/10.1186/s12916-020-01597-8. [ Links ]
8. Conectas Direitos Humanos. Mapeamento e análises das normas jurídicas de resposta à covid-19 no Brasil. Bol Direitos Pandemia. 20 jan. 2021 [acesso 26 jan. 2021];(10)1-56. Disponível em: https://www.conectas.org/publicacoes/download/boletim-direitos-na-pandemia-no-10 [ Links ]
9. The Lancet. Covid-19 in Brazil: "So what?". Lancet. 2020 May 9;395(10235):1461. doi: https://doi.org/10.1016/S0140-6736(20)31095-3. [ Links ]
10. Terrazas FV. Legislação para o enfrentamento da covid-19: leis e atos administrativos. In: Santos AO, Lopes LT, organizadoras. Competências e regras [Internet]. Brasília, DF: CONASS; 2021 [acesso 20 out. 2021]. (Coleção covid-19, vol. 3). p. 248-268. Disponível em: https://www.conass.org.br/biblioteca/volume-3-competencias-e-regras/ [ Links ]
11. Governo de Santa Catarina. Coronavírus: boletim epidemiológico [Internet]. [Florianópolis, SC]: Secretaria de o Estado da Administração]; 2021 [acesso 20 jan. 2021]. Disponível em: http://www.coronavirus.sc.gov.br/wp-content/uploads/2021/01/boletim-epidemiologico-20-01-2021.pdf [ Links ]
12. Ministério da Saúde (BR). Covid-19 no Brasil: painel [Website]. c2020 [acesso 3 nov. 2020. Disponível em: https://susanalitico.saude.gov.br/extensions/covid-19_html/covid-19_html.html [ Links ]
13. Garcia LP, Traebert J, Boing AC, Santos GFZ, Pedebôs LA, d'Orsi E, et al. O potencial de propagação da covid-19 e a tomada de decisão governamental: uma análise retrospectiva em Florianópolis, Brasil. Rev Bras Epidemiol. 2020;23:e200091. doi: http://doi.org/10.1590/1980-549720200091. [ Links ]
14. Diretoria de Vigilância Epidemiológica de Santa Catarina, Secretaria do Estado de Saúde (SC). Manual de orientações da covid-19: vírus SARS-CoV-2 [Internet]. [Florianópolis, SC]: SES; 2020 [acesso 3 nov. 2020]. Disponível em: https://www.saude.sc.gov.br/coronavirus/arquivos/Manual_23-10-atualizado.pdf [ Links ]
15. Governo do Estado de Santa Catarina (SC). Portal de dados abertos do estado de Santa Catarina [Website]. c2016 [acesso 9 nov. 2020]. Disponível em: http://dados.sc.gov.br [ Links ]
16. Rede Covida Ciência Informação e Solidariedade. Painel [Website]. - Rede CoVida [Internet]. 2020 [citado em 26 jan 2021]. Disponível em: https://painel.redecovida.org/brasil [ Links ]
17. Aquino EML, Silveira IH, Pescarini JM, Aquino R, Souza-Filho JA, Rocha AS, et al. Social distancing measures to control the covid-19 pandemic: potential impacts and challenges in Brazil. Cien Saude Colet. 2020;25(suppl 1):2423-46. doi: https://doi.org/10.1590/1413-81232020256.1.10502020. [ Links ]
18. Silva LLS, Lima AFR, Polli DA, Razia PFS, Pavão LFA, Cavalcanti MAFH, et al. Social distancing measures in the fight against covid-19 in Brazil: description and epidemiological analysis by state. Cad. Saúde Pública, 2020 Sep 18;36(9):e00185020. doi: https://doi.org/10.1590/0102-311x00185020. [ Links ]
19. Governo de Estado de Santa Catarina, Gestão da Saúde. Coronavírus: avaliação do risco potencial para covid-19 [Internet]. [Florianópolis (SC): SES; 2021 [citado em 26 jan. 2021]. Disponível em: http://www.coronavirus.sc.gov.br/gestao-da-saude/ [ Links ]
20. Ministério da Saúde (BR). Doença pelo coronavírus covid-19: Semana epidemiológica 35. Bol Epidemiol [Internet]. 29 ago. 2020 [acesso 26 jul. 2021]. Disponível em: https://antigo.saude.gov.br/images/pdf/2020/September/02/18h-Boletim-epidemiologico-COVID-29-final.pdf [ Links ]
21. Cavalcante JR, Cardoso-dos-Santos AC, Bremm JM, Lobo AP, Macário EM, Oliveira WK, et al. COVID-19 in Brazil: evolution of the epidemic up until epidemiological week 20 of 2020. Epidemiol Serv Saude. 2020;29(4):e2020376. doi: https://doi.org/10.5123/s1679-49742020000400010. [ Links ]
22. Portal Covid-19 Brasil. Monitoramento da taxa de letaldade (óbitos/confirmados) de covid-19: Brasil por estado [Website]. 2021 [acesso 25 jul. 2021]. Disponível em: https://ciis.fmrp.usp.br/covid19/estado-br/ [ Links ]
23. Valcarcel B, Avilez JL, Torres-Roman JS, Poterico JA, Bazalar-Palacios J, La La Vecchia C. The effect of early-stage public health policies in the transmission of covid-19 for South American countries. Rev Panam Salud Publica. 2020;44:e148. doi: https://doi.org/10.26633/RPSP.2020.148. [ Links ]
24. Conectas Direitos Humanos. Mapeamento e análises das normas jurídicas de resposta à covid-19 no Brasil. Bol Direitos Pandemia. 14 set. 2020 [acesso 21 jul. 2021];(5):1-18. Disponível em: https://www.conectas.org/publicacao/boletim-direitos-na-pandemia-no-5 [ Links ]
25. Siedner MJ, Harling G, Reynolds Z, Gilbert RF, Haneuse S, Venkataramani AS, et al. Social distancing to slow the US covid-19 epidemic: longitudinal pretest-posttest comparison group study. PLoS Med. 2020 Aug 11;17(8):e1003244. doi: https://doi.org/10.1371/journal.pmed.1003244. [ Links ]
26. Moraes RFD. Determinants of physical distancing during the covid-19 epidemic in Brazil: effects from mandatory rules, numbers of cases and duration of rules. Cien Saude Colet. 2020;25(9):3393-400. doi: https://doi.org/10.1590/1413-81232020259.21892020. [ Links ]
27. Aith F. Afirmação histórica do direito à saúde e os desafios para sua efetivação nos estados do século XXI. In: Santos AO, Lopes LT, organizadoras. Reflexões e futuro [Internet]. Brasília, DF: CONASS; 2021 [acesso 20 out. 2021]. (Coleção covid-19; vol. 6). p. 12-27. Disponível em: https://www.conass.org.br/biblioteca/volume-6-reflexoes-e-futuro/ [ Links ]
28. Supremo Tribunal Federal (BR). STF reconhece competência concorrente de estados, DF, municípios e União no combate à covid-19 [Internet]. Brasília, DF: STF; 15 abr. 2020 [acesso 20 out. 2021]. Disponível em: https://portal.stf.jus.br/noticias/verNoticiaDetalhe.asp?idConteudo=441447&ori=1 [ Links ]
29. Ferguson NM, Laydon D, Nedjati-Gilani G, Imai N, Ainslie K, Baguelin M, et al. Report 9: impact of non-pharmaceutical interventions (NPIs) to reduce COVID19 mortality and healthcare demand. 2020 Mar 16 [acesso 19 mar 2020]. doi: https://doi.org/10.25561/77482. [ Links ]
30. Prem K, Liu Y, Russell TW, Kucharski AJ, Eggo RM, Davies N, et al. The effect of control strategies to reduce social mixing on outcomes of the covid-19 epidemic in Wuhan, China: a modelling study. Lancet Public Health. 2020;5(5):e261-70. doi: https://doi.org/10.1016/S2468-2667(20)30073-6. [ Links ]
Received: June 14, 2021; Accepted: October 14, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
