










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.4 Brasília dez. 2021 Epub 06-Dez-2021
http://dx.doi.org/10.1590/s1679-49742021000400027
Original article
Prevalence of behavioral health risk factors and their simultaneous occurrence among students at a public university in Pelotas, state of Rio Grande do Sul, Brazil, 2017*
1Universidade Federal de Pelotas, Pelotas, RS, Brazil
Objective:
To estimate the prevalence of behavioral health risk factors and investigate clusters of simultaneous occurrences of these factors among students at a public university in Pelotas, state of Rio Grande do Sul, Brazil.
Methods:
This was a cross-sectional study among university students in the second semester of 2017. Physical inactivity, excessive sedentary behavior, inadequate sleep duration and smoking were the factors studied. Simultaneity of risk factors was evaluated using cluster analysis, through the ratio between observed and expected prevalence, and those that did not include the unit were considered clusters.
Results:
Among 1,716 students, the prevalence of inadequate sleep duration, physical inactivity, excessive sedentary behavior and smoking were 45.2% (95%CI 42.9;47.6), 44.4% (95%CI 42.7;47.2), 39.8% (95%CI 37.7;42.2) and 10.6% (95%CI 9.6;12.5) respectively. More than 80% of the students presented at least one risk factor. The clusters identified were related to inadequate sleep duration (O/E=1.15) and physical inactivity associated with sedentary behavior (O/E=1.24).
Keywords: Students; Physical Activity; Sedentary Behavior; Sleep; Smoking; Cross-sectional Studies
Introduction
Chronic conditions, such as cancers, diabetes mellitus and heart disease, present a high burden of disease worldwide.1.2Among the risk factors responsible for the onset and worsening of these conditions, smoking,1 physical inactivity,1.3 sedentary behavior4 and inadequate sleep duration stand out.5 A scoping review conducted in 2013 identified four simultaneous risk factors for the occurrence of chronic diseases: physical inactivity, smoking, alcoholism and inadequate diet, in which the first two factors were the most investigated.6 Other combinations of risk factors have been studied7 and a possible reason for this fact is the existence of synergistic effects between each set of risk factors.8 It could be seen a greater propensity for certain sets of risk factors to occur simultaneously, whose frequency was higher than expected.9 Understanding these combinations can direct the focus of interventions, increasing effectiveness and reducing costs related to unhealthy lifestyle.10
Evaluating new combinations of risk factors facilitates understanding of which health interventions may be more effective.
Among the general population, smoking and physical inactivity account for more than eight million deaths per year.1.3 In addition to these factors, excessive sedentary behavior and inadequate sleep duration are also associated with higher mortality,5.11 drawing researchers’ attention and being studied together with other health risk factors.8
Most university students, adolescents or young adults, present multiple health risk behaviors, but they are at a stage of life that favors long-term preservation or improvement of health conditions.12 Although this population is not the focus of interventions on risk factors, it is estimated that 50% of students from several universities worldwide are physically inactive,13 40% have inadequate sleep duration13 and sedentary behavior,14 and 15% are smokers.13
In this context, it is necessary to evaluate the simultaneous occurrence of health risk factors, both traditional (physical inactivity and smoking) and emerging factors (excessive sedentary behavior and inadequate sleep duration). Evaluating new combinations of risk factors facilitates understanding of which health interventions may be more effective.
The aim of this study was to estimate the prevalence of behavioral health risk factors and investigate clusters of simultaneous occurrences of these factors among students at a public university in the city of Pelotas, state of Rio Grande do Sul, Brazil.
Methods
This was a cross-sectional study conducted with undergraduate students at the Universidade Federal de Pelotas (UFPel), enrolled in the second semester of the academic year of 2017. UFPel has 90 in-class courses and has more than 20,000 students, of which 16,000 are at the undergraduate level. Data were collected between November 2017 and July 2018. The inclusion criteria in the study were: having entered undergraduate course in 2017; being 18 years of age or older; and having no severe physical or motor disabilities that would make it impossible or limited the practice of physical activity. All students who met these criteria were invited to take part in the study.
A pilot study was conducted with university students who had not been eligible for the study (entered UFPel by 2016), in order to evaluate the performance of data collection instrument. Before data collection, some contacts were made with the chancellor's office and principals or coordinators of the 80 in-class courses whose students entered university in the first semester of 2017, at Pelotas and Capão do Leão campuses. Subsequently, several visits to the classes were scheduled with the teachers of the eligible courses, on different days and at different times, aimed at the application of a questionnaire. In order to minimize selection bias, students were not informed about the date of the application of the survey questionnaire. The research instrument was developed on the Research Electronic Data Capture (RedCap),15 self-administered anonymously on tablets, and there was always a team qualified to answer any questions.
Sample size calculation was performed using the OpenEpi website (www.openepi.com) version 3.01. The reference population was 3,000 students, according to an estimate of university students enrolled at UFPel in the first semester. The sample size calculation considered the prevalence of two simultaneous risk factors of 40%, 95% confidence level and margin of error of 2 percentage points, plus 10% for losses and refusals. Thus, the final sample required was 1,434 individuals.
Four risk factors were evaluated: physical inactivity, excessive sedentary behavior, inadequate sleep duration and smoking. Physical inactivity was assessed using the leisure-time International Physical Activity Questionnaire in its short version, and those who did not meet the World Health Organization (WHO) recommendation of 150 minutes per week of moderate-intensity aerobic physical activity or at least 75 minutes of vigorous-intensity aerobic physical activity, or a combination of both, were considered physically inactive.16 Excessive sedentary behavior was defined as 'spending more than five hours a day in front of a screen'. As such, a question was asked: On average, on an ordinary weekday, how many hours do you watch TV, play video game or use your computer for any purpose?
Sleeping less than seven hours a night was considered as inadequate sleep duration. Sleep duration was measured by the answers to three questions about sleep habits from Monday to Friday: (i) when the individual goes to bed, (ii) the time between lying down and falling asleep, and (iii) when the individual wakes up. Based on the answers to these questions, the difference was calculated in minutes, between the time the individual wakes up and the time he or she goes to bed; finally, the latency between lying down and falling asleep was subtracted. In addition, the university students were asked about the smoking habit, and those who reported having smoked at least one cigarette per day in the last month were considered smokers.
The independent variables collected were: sex (male; female); age (in complete years, categorized: 18 to 19; 20 to 22; 23 or older); self-reported race/skin color (White; Black; brown; Asian/indigenous/other); marital status (single; married or in stable union; separated/divorced; or widowed); and the student's undergraduate course, categorized into four major areas (exact and land/agricultural sciences and engineering; health and biological sciences; applied social sciences and humanities; linguistics, letters and arts). University students’ economic status was evaluated according to the Associação Brasileira de Empresa de Pesquisa (ABEP) criteria, categorized into classes: A, B, C and D/E, being class A the richest one. We also evaluated the type of school attended in high school (public; private) and maternal education [illiterate or with incomplete elementary education; complete elementary education or incomplete high school education; complete high school education (or technical course) or incomplete higher education; complete higher education (or technologist course); complete postgraduate education]. The self-reported weight and height were used to calculate the university student's body mass index (BMI), according to the WHO classification: underweight (<18.5kg/m2); eutrophic (18.5 to 24.9 kg/m2); overweight (25 to 29.9 kg/m2) and obesity (³30 kg/m2).
For statistical analyses, those with complete information for all four risk factors were included. Descriptive analyses were performed using absolute and relative frequencies, and respective 95% confidence interval (95%CI) for the independent variables, stratified by sex, in addition to the description of risk factors and the cumulative number of these factors according to the independent variables. Fisher's exact test for dichotomous exposure and Pearson's chi-square test for exposures with more than two categories were used. Associations with p<0.05 were considered significant.
The presence of simultaneity of behavioral health risk factors in the study population was evaluated by means of cluster analysis, using the observed/expected prevalence ratio as a measure. The expected values were calculated for each of the 16 possible specific combinations, multiplying the observed prevalence of the present factors by the inverse of the observed proportion of the missing factors, assuming independence between the analyzed factors. The cluster was considered statistically significant when the observed/expected ratio was greater than one, and its respective 95%CI – calculated based on the binomial approximation – did not include the unit.17 Microsoft Excel 2016 software was used to analyze the observed and expected prevalence and their confidence intervals; and the statistical software package Stata version 15.1 (StataCorp, College Station, Texas, TX), was used for descriptive and association analyses.
The study project was approved by the Research Ethics Committee of the Faculty of Medicine of the Universidade Federal de Pelotas: Opinion No. 79250317.0.0000.5317. The students were informed about the objectives of the research and its possible risks, and only received the questionnaire after signing the Free and Informed Consent Form.
Results
In the first semester of 2017, 3,212 students entered the eligible undergraduate courses, of which 2,706 started in the second semester of that year and therefore they represent the target population of this study. Of these, 1,865 (68.9%) students were interviewed. Among losses (29.3%) and refusals (1.8%), the majority were male (52.8%), aged 23 years or older (46.7%) and studied 'exact and land/agricultural sciences and engineering' (38.3%).
Taking into consideration the four outcomes evaluated, 1,716 participants answered all questions, constituting the final sample of the study (92,0% of all students interviewed). Among them, 55,0% were female, about 42,0% aged between 18 and 19 years old and 72.4% reported being of White race/skin color. Nine out of ten university students reported being single and most of them attended high school in public school (72%) (Table 1). About 80% of the sample belonged to economic classes B and C and 54.2% had a mother with complete high school education or more. About one third of them studied 'applied social sciences and humanities' and 63,0% were classified as eutrophic (Table 1).
Table 1 Absolute (n) and relative (%) frequency of the socioeconomic, demographic and health variables of undergraduates (n=1,716) in the second semester at the Universidade Federal de Pelotas, Pelotas, state of Rio Grande do Sul, Brazil, 2017
| Variables | Total | Male | Female | ||||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Age (in years) | |||||||
| 18-19 | 713 | 41.9 | 304 | 39.8 | 409 | 43.7 | |
| 20-22 | 552 | 32.4 | 252 | 32.9 | 299 | 31.9 | |
| ≥23 | 438 | 25.7 | 209 | 27.3 | 229 | 24.4 | |
| Race/skin color | |||||||
| White | 1,241 | 72.4 | 559 | 72.4 | 681 | 72.2 | |
| Black | 217 | 12.7 | 93 | 12.1 | 124 | 13.2 | |
| Brown | 228 | 13.3 | 104 | 13.5 | 124 | 13.2 | |
| Asian/indigenous/other | 28 | 1.6 | 15 | 2.0 | 13 | 1.4 | |
| Marital Status | |||||||
| Single | 1,545 | 90.1 | 68 | 8.8 | 76 | 8.1 | |
| Married or in stable union | 144 | 8.4 | 695 | 90.0 | 849 | 90.1 | |
| Separated, divorced or widowed | 26 | 1.5 | 9 | 1.2 | 17 | 1.8 | |
| Type of school attended in high school | |||||||
| Public school | 1,235 | 72.0 | 550 | 71.3 | 684 | 72.5 | |
| Private school | 480 | 28.0 | 221 | 28.7 | 259 | 27.5 | |
| Economic statusa (ABEPb criteria) | |||||||
| A | 252 | 15.3 | 128 | 17.6 | 124 | 13.6 | |
| B | 734 | 44.7 | 329 | 45.1 | 405 | 44.3 | |
| C | 586 | 35.7 | 240 | 32.9 | 345 | 37.8 | |
| D-E | 71 | 4.3 | 32 | 4.4 | 39 | 4.3 | |
| Maternal education | |||||||
| Illiterate or incomplete elementary education | 377 | 22.1 | 156 | 20.4 | 221 | 23.5 | |
| Complete elementary school or incomplete high school education | 204 | 12.0 | 84 | 11.0 | 120 | 12.8 | |
| Complete high school education (technical course) or incomplete higher education | 539 | 31.5 | 237 | 31.0 | 301 | 31.9 | |
| Complete higher education (or technologist course) | 388 | 22.7 | 186 | 24.3 | 202 | 21.5 | |
| Complete postgraduate education | 199 | 11.7 | 102 | 13.3 | 97 | 10.3 | |
| Major areas of study (CNPqc criteria) | |||||||
| Exact and land/agricultural sciences and engineering | 495 | 28.9 | 274 | 35.5 | 220 | 23.3 | |
| Health and biological sciences | 317 | 18.5 | 126 | 16.3 | 191 | 20.3 | |
| Applied social sciences and humanities | 588 | 34.2 | 238 | 30.8 | 350 | 37.1 | |
| Linguistic, letters and arts | 316 | 18.4 | 134 | 17.4 | 182 | 19.3 | |
| Body mass index – BMI | |||||||
| Underweight | 91 | 5.4 | 22 | 2.9 | 69 | 7.4 | |
| Eutrophic | 1,072 | 63.0 | 493 | 64.4 | 578 | 61.7 | |
| Overweight | 370 | 21.7 | 181 | 23.7 | 189 | 20.2 | |
| Obesity | 169 | 9.9 | 69 | 9.0 | 100 | 10.7 | |
aVariable with the highest amount of missing data (n=73);
bABEP: Associação Brasileira das Empresas de Pesquisa;
cCNPq: Conselho Nacional de Desenvolvimento Científico e Tecnológico of the Ministry of Science, Technology and Innovations.
The prevalence of inadequate sleep duration was 45.2% (95%CI 42.9;47.6), while physical inactivity was 44.4% (95%CI 42.7;47.2). Excessive sedentary behavior and smoking showed prevalence of 39.8% (95%CI 37.7;42.2) and 10.6% (95%CI 9.6;12.5) respectively (Figure 1). According to the interviewees' sex, physical inactivity was more prevalent among females (52.4%) when compared to males (34.7%) (p<0.001), while inadequate sleep duration (p<0.001) and smoking (p=0.001) were more frequent among males. One third of the students presented two health risk factors at the same time, while one in ten presented three simultaneous factors. About 20% of males and 14% of females did not present any risk factors (Figure 1).
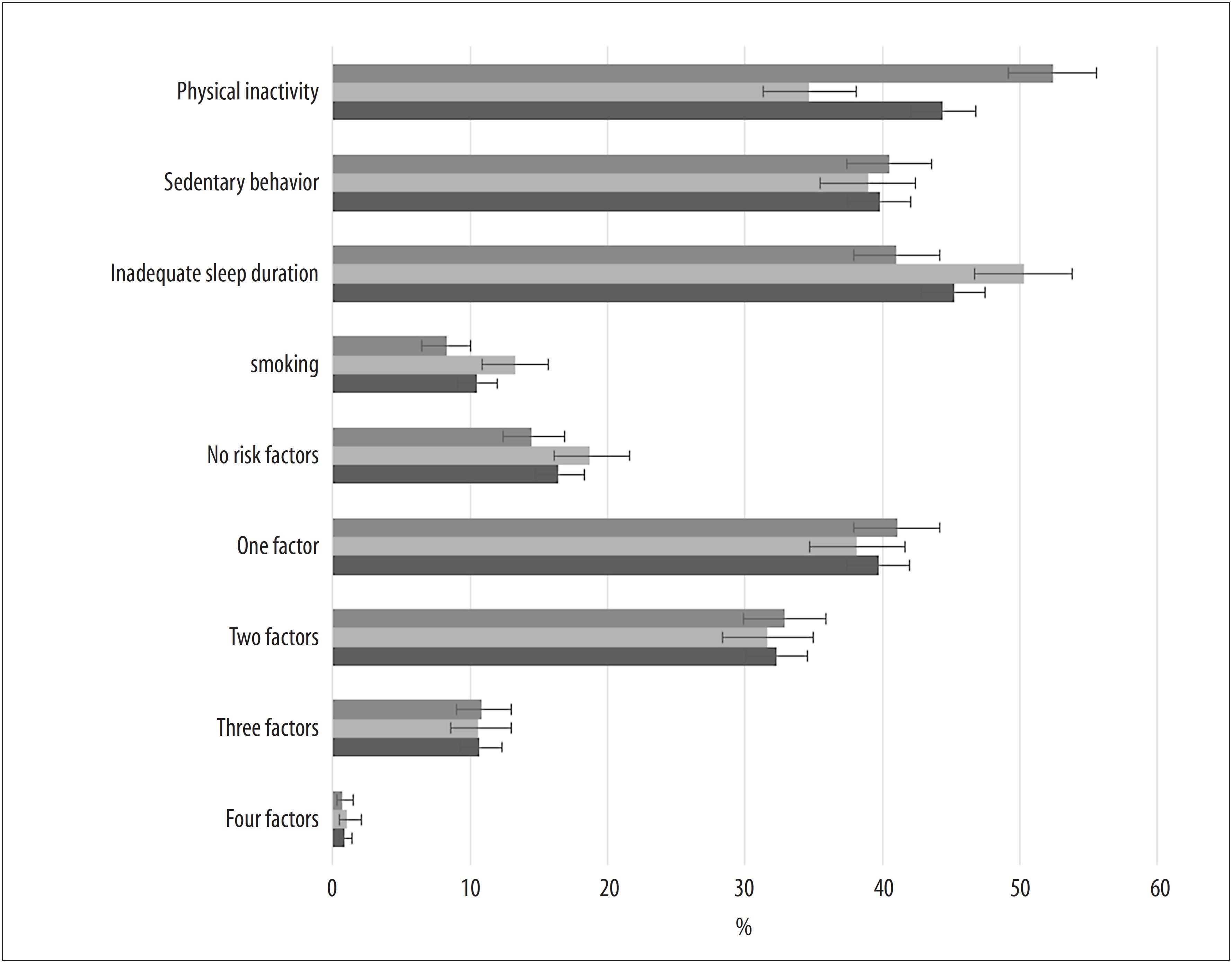
Figure 1 Prevalence (%) and 95% confidence interval of behavioral health risk factors and number of simultaneous risk factors, among undergraduate students in the second semester (n=1,716) at the Universidade Federal de Pelotas, Pelotas, state of Rio Grande do Sul, Brazil, 2017
Table 2 describes the prevalence of the four behavioral risk factors studied and the number of risk factors present according to the socioeconomic, demographic and health characteristics of the university students who were interviewed. There was an association between excessive sedentary behavior and age, more prevalent in younger individuals (18 and 19 years old) (44.7%; p<0.001). Smoking was more prevalent among older people (23 years or over) (15.1%; p=0.001). Excess sedentary behavior, in turn, was more prevalent among single individuals (41.6%; p<0.001), while inadequate sleep duration was more frequent among separated, divorced or widowed (73.1%; p=0.015). Regarding the number of risk factors present, most students of Asian, indigenous or other race/skin color presented only one risk factor (53.6%; p=0.037). Furthermore, one in five students studying 'health and biological sciences' presented no risk factors, a result higher and statistically different from the other courses/areas of knowledge (p=0.034) (Table 2).
Table 2 Prevalence of the four behavioral risk factors and the number of simultaneous risk factors, according to socioeconomic, demographic and health characteristics among undergraduate students in the second semester (n=1,716) at the Universidade Fedral de Pelotas, Pelotas, state of Rio Grande do Sul, Brazil, 2017
| Variable | Physical inactivity (%) | Sedentary behavior (%) | Inadequate sleep (%) | Smoking (%) | 0 factor (%) | 1 factor (%) | 2 factors (%) | 3 or 4 factors (%) | |
|---|---|---|---|---|---|---|---|---|---|
| n=762 | n=683 | n=775 | n=181 | n=282 | n=681 | n=554 | n=199 | ||
| Age (years) | |||||||||
| 18-19 | 43.2 | 44.7 | 44.3 | 8.4 | 16.3 | 39.2 | 33.1 | 11.4 | |
| 20-22 | 45.1 | 40.4 | 42.0 | 9.8 | 17.8 | 39.3 | 31.7 | 11.2 | |
| ≥23 | 45.2 | 31.3 | 49.3 | 15.1 | 15.5 | 40.9 | 31.3 | 12.3 | |
| p-valuea | 0.725 | <0.001 | 0.068 | 0.001 | 0.621 | 0.844 | 0.780 | 0.844 | |
| Race/skin color | |||||||||
| White | 44.6 | 39.1 | 44.1 | 10.2 | 17.3 | 39.5 | 31.9 | 11.3 | |
| Black | 43.3 | 44.7 | 46.5 | 10.1 | 17.5 | 33.6 | 36.5 | 12.4 | |
| Age (years) | |||||||||
| Brown | 46.5 | 39.5 | 49.6 | 11.4 | 11.0 | 45.1 | 30.7 | 13.2 | |
| Asian/indigenous/other | 28.6 | 35.7 | 46.4 | 25.0 | 10.7 | 53.6 | 28.6 | 7.1 | |
| p-valuea | 0.337 | 0.449 | 0.465 | 0.085 | 0.088 | 0.037 | 0.531 | 0.716 | |
| Marital status | |||||||||
| Single | 43.9 | 41.6 | 44.9 | 10.4 | 16.5 | 39.0 | 32.8 | 11.7 | |
| Married or in stable union | 50.0 | 23.6 | 43.8 | 11.8 | 18.8 | 44.4 | 25.7 | 11.1 | |
| Separated, divorced or widowed | 46.2 | 23.1 | 73.1 | 15.4 | 0 | 50.0 | 42.3 | 7.7 | |
| p-valuea | 0.363 | <0.001 | 0.015 | 0.623 | 0.058 | 0.247 | 0.122 | 0.802 | |
| Type of school attended in high school | |||||||||
| Public school | 45.8 | 39.6 | 45.5 | 10.1 | 16.0 | 39.3 | 33.3 | 11.4 | |
| Private school | 41.0 | 40.2 | 44.2 | 11.7 | 17.7 | 40.6 | 29.6 | 12.1 | |
| p-valuea | 0.083 | 0.826 | 0.627 | 0.381 | 0.384 | 0.660 | 0.150 | 0.737 | |
| Economic status (ABEPc criteria) | |||||||||
| A | 39.7 | 42.1 | 45.6 | 13.1 | 17.9 | 36.5 | 33.3 | 12.3 | |
| B | 43.7 | 40.1 | 43.7 | 10.1 | 17.7 | 40.6 | 29.3 | 12.4 | |
| C | 48.0 | 38.2 | 46.1 | 10.2 | 15.7 | 38.0 | 35.0 | 11.3 | |
| D-E | 45.1 | 45.1 | 46.5 | 8.5 | 11.3 | 42.2 | 36.6 | 9.9 | |
| p-valuea | 0.148 | 0.578 | 0.837 | 0.513 | 0.440 | 0.579 | 0.127 | 0.868 | |
| Major area of study (CNPqc criteria) | |||||||||
| Exact and land/agricultural sciences and engineering | 42.8 | 38.2 | 58.4 | 8.5 | 13.3 | 39.2 | 34.6 | 12.9 | |
| Health and biological sciences | 40.1 | 31.2 | 53.0 | 6.3 | 21.1 | 38.2 | 30.6 | 10.1 | |
| Applied social sciences and humanities | 47.1 | 44.2 | 34.7 | 12.8 | 16.2 | 41.8 | 30.1 | 11.9 | |
| Linguistic, letters and arts | 46.2 | 42.7 | 36.1 | 13.9 | 17.1 | 38.0 | 34.5 | 10.4 | |
| p-valuea | 0.166 | 0.001 | <0.001 | 0.002 | 0.034 | 0.598 | 0.314 | 0.568 | |
| Body mass index – BMI | |||||||||
| Underweight | 52.8 | 46.2 | 40.7 | 7.7 | 16.5 | 36.2 | 30.8 | 16.5 | |
| Eutrophic | 44.7 | 39.5 | 44.1 | 9.6 | 16.1 | 40.9 | 32.6 | 10.4 | |
| Overweight | 43.2 | 38.4 | 50.3 | 10.8 | 16.8 | 36.7 | 34.3 | 12.2 | |
| Obesity | 41.4 | 40.2 | 43.8 | 16.6 | 17.8 | 39.0 | 28.4 | 14.8 | |
| p-valuea | 0.333 | 0.594 | 0.155 | 0.039 | 0.958 | 0.473 | 0.577 | 0.135 | |
aPearson's chi-square test; b) Fischer's exact test;
cVariable with higher amount of missing data (n=38).
The 16 possible combinations of risk behaviors, the observed and expected prevalence, and their respective ratios are showed in Table 3, either for the entire sample or when stratified by sex. Presenting only inadequate sleep duration (O/E=1.15; 95%CI 1.04;1.27) and physical inactivity associated with excessive sedentary behavior (O/E=1.24; 95%CI 1.09;1.41) was considered as a cluster. In addition, the combination of excessive sedentary behavior with inadequate sleep time occurred less frequently than expected (O/E=0.81; 95%CI 0.69;0.96) (Table 3). In the analysis stratified by sex, among males, it could be seen the occurrence of physical inactivity concomitantly with sedentary behavior 1.42 times (95%CI 1.13;1.78) higher than expected at random, while for females, presenting only inadequate sleep duration was the only cluster identified (O/E=1.20; 95%CI 1.03;1.40) (Table 3).
Table 3 Prevalence and simultaneity of the four main risk factors, stratified by sex, among undergraduate students in the second semester (n=1,716) at the Universidade Federal de Pelotas, Pelotas, state of Rio Grande do Sul, Brazil, 2017
| Factors | Total | Male | Female | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | PIa | SBb | ISDc | Sd | Oe (%) | Ef (%) | O/Eg (95%CIh) | O (%) | E (%) | O/E (95%CIh) | O (%) | E (%) | O/E (95%CIh) |
| 0 | – | – | – | – | 16.4 | 16.4 | 1.00 (0.91;1.10) | 18.6 | 17.2 | 1.09 (0.95;1.24) | 14.5 | 15.3 | 0.95 (0.82;1.09) |
| 1 | + | – | – | – | 12.3 | 13.1 | 0.94 (0.83;1.06) | 7.4 | 9.1 | 0.81 (0.64;1.03) | 16.4 | 16.8 | 0.97 (0.85;1.10) |
| 1 | – | + | – | – | 10.0 | 10.9 | 0.92 (0.81;1.06) | 9.3 | 11.0 | 0.85 (0.69;1.05) | 10.6 | 10.4 | 1.02 (0.85;1.21) |
| 1 | – | – | + | – | 15.5i | 13.5 | 1.15 (1.04;1.27) | 18.7 | 17.4 | 1.08 (0.95;1.23) | 12.8i | 10.7 | 1.20 (1.03;1.40) |
| 1 | – | – | – | + | 1.9 | 1.9 | 0.96 (0.68;1.35) | 2.6 | 2.6 | 0.98 (0.64;1.51) | 1.3 | 1.4 | 0.92 (0.52;1.61) |
| 2 | + | + | – | – | 10.8i | 8.7 | 1.24 (1.09;1.41) | 8.3i | 5.8 | 1.42 (1.13;1.78) | 12.8 | 11.5 | 1.12 (0.96;1.30) |
| 2 | + | – | + | – | 10.1 | 10.8 | 0.93 (0.82;1.07) | 8.7 | 9.2 | 0.94 (0.76;1.17) | 11.2 | 11.7 | 0.96 (0.81;1.13) |
| 2 | + | – | – | + | 1.2 | 1.6 | 0.76(0.49;1.17) | 0.8 | 1.4 | 0.55 (0.25;1.23) | 1.5 | 1.5 | 0.97 (0.58;1.64) |
| 2 | – | + | + | – | 7.3i | 8.9 | 0.81 (0.69;0.96) | 9.2 | 11.1 | 0.83 (0.67;1.02) | 5.7 | 7.3 | 0.79 (0.61;1.02) |
| 2 | – | + | – | + | 1.3 | 1.3 | 1.05 (0.70;1.57) | 1.8 | 1.7 | 1.07 (0.64;1.80) | 1.0 | 0.9 | 1.01 (0.53;1.94) |
| 2 | – | – | + | + | 1.6 | 1.6 | 1.02 (0.71;1.47) | 2.9 | 2.7 | 1.07 (0.71;1.61) | 0.6 | 1.0 | 0.67 (0.30;1.47) |
| 3 | + | + | + | – | 7.1 | 7.1 | 0.99 (0.84;1.17) | 6.4 | 5.9 | 1.08 (0.83;1.40) | 7.6 | 8.0 | 0.96 (0.77;1.18) |
| 3 | + | + | – | + | 0.9 | 1.0 | 0.91 (0.56;1.48) | 0.9 | 0.9 | 1.01 (0.49;2.12) | 1.0 | 1.0 | 0.92 (0.48;1.76) |
| 3 | + | – | + | + | 1.2 | 1.3 | 0.96 (0.63;1.47) | 1.3 | 1.4 | 0.92 (0.50;1.69) | 1.2 | 1.1 | 1.11 (0.62;1.99) |
| 3 | – | + | + | + | 1.5 | 1.1 | 1.44 (0.99;2.11) | 2.1 | 1.7 | 1.21 (0.75;1.97) | 1.1 | 0.7 | 1.62 (0.87;3.01) |
| 4 | + | + | + | + | 0.9 | 0.8 | 1.03 (0.62;1.71) | 1.0 | 0.9 | 1.15 (0.58;2.28) | 0.7 | 0.7 | 1.03 (0.49;2.15) |
aPI: Physical inactivity;
bSB: sedentary behavior;
cISD: inadequate sleep duration;
dS: tobacco use;
eO: observed value;
fE: expected value;
gO/E: ratio between observed/ expected values;
h95%CI: 95% confidence interval;
iclustering.
Discussion
The most prevalent risk behaviors among university students were inadequate sleep duration and physical inactivity. The first was more prevalent in males, while the second one, in females. About 80% of the sample presented at least one risk factor. Only two clusters were observed:(i) inadequate sleep duration alone; and (ii) physical inactivity simultaneously with excessive sedentary behavior. Excessive sedentary behavior along with inadequate sleep time occurred less than expected. When stratified by sex, among males, only the clustering of physical inactivity was observed simultaneously with excessive sedentary behavior, while among females, only inadequate sleep duration was observed.
The observed prevalence of physical inactivity was lower than that found in 2019 in Porto Alegre, capital city of the state of Rio Grande do Sul (62.3%), and in all other Brazilian capitals, when 18-24 age group (50.6%),18 with the highest number of individuals addressed in this study was observed. In a study conducted in Florianópolis, the capital city of the state of Santa Catarina, with college freshmen in 2012, using the same cutoff point used in this study, a prevalence of physical inactivity of 18.5% was found.19 This difference can be explained, in part, by the disparity in the samples, although both were comprised of freshmen, they present different distributions regarding. Estimates from other low- and middle-income countries show that approximately 41% of university students are inactive, with women being the hardest hit by physical inactivity, a reality that corroborates that of university students in Pelotas.20
A systematic review on sedentary behavior, published in 2020, identified 125 studies with a university population, showing large differences in outcome measurement and in the cut-off points used among the studies consulted.21 Nevertheless, an average of more than seven hours per day related to this behavior was found.21 Among students in the first year of higher education in Greece, using a cut-off point of six hours (five hours were used in this study), a prevalence of approximately 40% of sedentary individuals was found, with no differences between the sexes. This finding is similar to that of the present study.14
Studies conducted with the use of accelerometers observed that, on average, approximately 10 hours per day are spent on sedentary activities.21.22 Despite the long period spent being sedentary, university students present more than one hour per day of moderate or vigorous-intensity physical activities, an important fact in order to mitigate the harms of a sedentary lifestyle.22.23
In addition, particularly among university students at UFPel, the time spent in front of a screen was evaluated, failing to measure an important part of this behavior, that is, the time spent sitting and dedicated to study; among Canadian university students, for example, this period is approximately three hours/day, which is considered one of the obstacles to the reduction of sedentary lifestyle.24
Regarding sleep duration, a multicenter study conducted at 26 universities in 2015, using reported sleep duration in a 24-hour period, found that approximately 39% of students slept less than six hours a day, most days;25 Despite the values similar to those obtained in the present study (39.8%), the difference between the present study and the forementioned study stands out with regard to the cutoff point adopted (one less hour of sleep) and the way the outcome was operationalized: in Pelotas, the average sleep duration on school days was used. It is worth mentioning that university students tend to sleep less on school days, when compared to weekends,26 possibly due to the academic activities provided on weekdays.
Smoking has been reduced in Brazil and worldwide.18 The observed prevalence in this study (10.6%) was slightly higher than the national average for 18 to 24 (7.9%) and 25 to 34 years of age (9.2%), according to data collected in a survey conducted by the Ministry of Health in 2019.18 However, this prevalence represents almost half of that found in a population-based study conducted with adults living in the urban area of Pelotas in 2010.27 Putting the sociodemographic differences aside, the study of the urban area of Pelotas reflects the reality of the city where UFPel is located. In Rio Grande, a municipality neighboring Pelotas, the prevalence of smoking among university students was 7.5% in 2017,28 and among first-year students at a university in Santa Catarina, 8.7% in 2012.19 European university students reported prevalence of approximately 30%,14.29 expected difference when compared to that of Brazilian students, due to tobacco use reduction programs adopted in the country.
Among the studies that evaluated the simultaneity of behavioral risk factors among university students, it could be seen that 20 to 27% of the students did not present any of these factors, results higher than those found in the present study, 16.4%.19.29 These differences can be explained by the factors studied; however, a significant number of university students maintain healthy lifestyle, in addition to that, students attending health and biological sciences courses were those who presented the highest occurrence of zero risk factors; probably, due to their interest in topics related to good health and quality of life, which is precisely the object of their studies. Moreover, taking into consideration that it is a sample with a high level of education, it was expected that there were fewer risk factors.27
A principal component analysis, the object of a study developed in 2018, with a sample of young Australians aged 18 years, classified more than 50% of them in a group characterized by a high probability of meeting guidelines for physical activity, sedentary behavior, sleep duration and smoking.30 This does not mean that the recommendations were followed, but that there is a statistical component aggregating those young people, given that they have similar characteristics. In this Study at UFPel, for example, a cluster encompassing the four evaluated outcomes was not observed.
Among the females who were interviewed in this study, the values found for 'inadequate sleep duration' were higher than expected, suggesting that those who reported sleeping less than seven hours a day tended to present only this risk factor. No studies were found with university students that have used (i) the same cluster approach used here and evaluated (ii) inadequate sleep duration. According to the first study conducted in Australia in 2015, seven risk factors were evaluated among people aged 45 years and over, of whom more than 5% presented only inadequate sleep duration as a risk factor.8
In this study conducted at UFPel, males presented more frequently physical inactivity concomitant with excessive sedentary behavior than expected. Here, it can be seen a combination of risk factors for mortality, either due to cardiometabolic diseases or another cause of death.7
Although we did not observe different populations other than university students, in this study, the clustering of physical inactivity concomitant with smoking has been usually reported,7 suggesting that the interrelationships between risk factors may be specific to populations. The combination of physical inactivity and inadequate sleep duration was the most frequently reported two-factor cluster in this study, although it is not statistically significant. In Germany, in 2008, among first year university students, the most prevalent clusters were 'inadequate fruit /vegetable consumption and low level of physical activity' and 'inadequate fruit/vegetable consumption and alcohol abuse'.29 The set of physical inactivity, excessive sedentary behavior and inadequate sleep duration represented the combination of three risk factors most commonly reported in this study, affecting more than 7% of the UFPel sample. However, among the Germans, the most frequently reported set of three risk factors was inadequate fruit and vegetable consumption simultaneously with low exercise and alcohol abuse, reported by more than 24% of university students in that country, showing clear differences based on the factors evaluated.29
This study presents some limitations, such as more than 30% of losses and refusals, although these are expected values for studies with this population.28 These losses may have underestimated the prevalence of inadequate sleep duration and smoking and, at the same time, overestimated the sex differences in physical inactivity, therefore capable of impacting on cluster analyses given that most losses are related to individuals at higher risk, such as males and older people. In order to reduce these losses, several visits were made to the classes, on different days and at different times, with no attempt limit, until the end of the fieldwork. Due to the fact that data collection was completed only at the end of the first semester of 2018, many students may have dropped, canceled their enrollment, or moved to another course or institution. Data from UFPel confirmed that 77% of the students who were part of the target population, enrolled in the semester following the end of the fieldwork, confirming the abandonment in the period studied. Thus, despite the losses, the findings of the study can be extrapolated to other Brazilian public universities with a similar profile, given that the system of federal institution admission throughout the country is the same. Another limitation of the study is the fact that risk factors established as relevant to this population were not quantified, e.g., inadequate diet, alcohol abuse and risky sexual behavior, in addition to external factors, which, in this age group, account for higher mortality rates, such as violence and traffic accidents.
The findings point to only two clusters – inadequate sleep duration and physical inactivity associated with excessive sedentary behavior – whose occurrences were higher than expected. However, high prevalence of risk factors can be seen in this population. This research with students at the UFPel represents one of the few studies with the objective of evaluating the simultaneous occurrence of traditional and emerging risk factors among university students, using the cluster approach. Due to the fact that they were in an educational institution, it was a contingent with a wide possibility of interventions, capable of influencing the adoption and/or perpetuation of good habits for the rest of their lives. Further studies are suggested to include health risk factors such as diet, drug use, overweight and obesity.
*Article derived from the Master's degree dissertation entitled ‘Simultaneity of behavioral health risk factors among students at a public university in southern Brazil’, submitted by Pedro Augusto Crespo da Silva to the Postgraduate Program in Epidemiology of the Universidade Federal de Pelotas, on January 24, 2019. The study received financial support from the Academic Excellence Program of the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, an organ of the Ministry of Education (Proex-CAPES/MEC): Process No. 0185/2017/23038.000288/2017-47
REFERENCES
GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global burden of disease study 2015. Lancet. 2016 Oct 8;388(10053):1659-724. doi: https://doi.org/10.1016/S0140-6736(16)31679-8. [ Links ]
GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020 Oct 17;396(10258):1223-49. doi: https://doi.org/10.1016/S0140-6736(20)30752-2. [ Links ]
Lee I-M, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012 Jul 21;380(9838):219-29. doi: http://doi.org/10.1016/S0140-6736(12)61031-9. [ Links ]
Biswas A, Oh PI, Faulkner GE, Bajaj RR, Silver MA, Mitchell MS, et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults a systematic review and meta-analysis. Ann Intern Med. 2015 Jan 20;162(2):123-32. doi: https://doi.org/10.7326/M14-1651. [ Links ]
Itani O, Jike M, Watanabe N, Kaneita Y. Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression. Sleep Med. 2017;32:246-56. doi: http://doi.org/10.1016/j.sleep.2016.08.006. [ Links ]
McAloney K, Graham H, Law C, Platt L. A scoping review of statistical approaches to the analysis of multiple health-related behaviours. Prev Med. 2013;56(6):365-71. doi: http://doi.org/10.1016/j.ypmed.2013.03.002. [ Links ]
Krokstad S, Ding D, Grunseit AC, Sund ER, Holmen TL, Rangul V, et al. Multiple lifestyle behaviours and mortality, findings from a large population-based Norwegian cohort study: the HUNT study. BMC Public Health. 2017 Jan 10;17(1):58. doi: http://doi.org/10.1186/s12889-016-3993-x [ Links ]
Ding D, Rogers K, van der Ploeg H, Stamatakis E, Bauman AE. Traditional and emerging lifestyle risk behaviors and all-cause mortality in middle-aged and older adults: evidence from a large population-based Australian cohort. PLoS Med. 2015 Dec 8;12(12): e1001917. doi: https://doi.org/10.1371/journal.pmed.1001917. [ Links ]
Costa FF, Benedet J, Leal DB, Assis MAA. Clustering of risk factors for non communicable diseases in adults from Florianopolis, SC.. Rev Bras Epidemiol. 2013;16(2):398-408. doi: https://doi.org/10.1590/S1415-790X2013000200015. [ Links ]
Prochaska JO, Velicer WF, Redding C, Rossi JS, Goldstein M, DePue J, et al. Stage-based expert systems to guide a population of primary care patients to quit smoking, eat healthier, prevent skin cancer, and receive regular mammograms. Prev Med. 2005;41(2):406-16. doi: https://doi.org/10.1016/j.ypmed.2004.09.050. [ Links ]
Biddle SJH, Bennie JA, Bauman AE, Chau JY, Dunstan D, Owen N, et al. Too much sitting and all-cause mortality: Is there a causal link?. BMC Public Health. 2016 Jul 26;16:635. doi: http://doi.org/10.1186/s12889-016-3307-3. [ Links ]
Nelson MC, Story M, Larson NI, Neumark-Sztainer D, Lytle LA. Emerging adulthood and college-aged youth: An overlooked age for weight-related behavior change. Obesity (Silver Spring). 2008;16(10):2205-11. doi: https://doi.org/10.1038/oby.2008.365. [ Links ]
Peltzer K, Pengpid S, Yung TKC, Aounallah-Skhiri H, Rehman R. Comparison of health risk behavior, awareness, and health benefit beliefs of health science and non-health science students: an international study. Nurs Health Sci. 2016;18(2):180-7. doi: https://doi.org/10.1111/nhs.12242. [ Links ]
Kritsotakis G, Psarrou M, Vassilaki M, Androulaki Z, Philalithis AE. Gender differences in the prevalence and clustering of multiple health risk behaviours in young adults. J Adv Nurs. 2016;72(9):2098-113. doi: https://doi.org/10.1111/jan.12981. [ Links ]
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap): a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377-81. doi: https://doi.org/10.1016/j.jbi.2008.08.010. [ Links ]
World Health Organization. Global recommendations on physical activity for health [Internet]. Geneva: WHO; 2010 [acesso 27 out. 2021]. Available from: https://www.who.int/dietphysicalactivity/publications/9789241599979/en [ Links ]
Goldstein MG, Whitlock EP, DePue J. Multiple behavioral risk factor interventions in primary care: summary of research evidence. Am J Prev Med. 2004;27(2 suppl):61-79. doi: https://doi.org/10.1016/j.amepre.2004.04.023. [ Links ]
Ministério da Saúde (BR). Vigitel Brasil 2019: vigilância de fatores de risco e proteção para doenças crônicas por inquérito telefônico: estimativas sobre frequência e distribuição sociodemográfica de fatores de risco e proteção para doenças crônicas nas capitais dos 26 estados [Internet]. Brasília, DF: MS; 2020 [acesso 27 out. 2021]. Available from: https://www.gov.br/saude/pt-br/centrais-de-conteudo/vigitel-brasil-2019-vigilancia-fatores-risco-pdf/view [ Links ]
Silva DAS, Petroski EL. The simultaneous presence of health risk behaviors in freshman college students in Brazil. J Community Health. 2012;37(3):591-8. doi: https://doi.org/10.1007/s10900-011-9489-9. [ Links ]
Pengpid S, Peltzer K, Kassean HK, Tsala JPT, Sychareun V, Müller-Riemenschneider F. Physical inactivity and associated factors among university students in 23 low-, middle- and high-income countries. Int J Public Health. 2015;60(5):539-49. doi: https://doi.org/10.1007/s00038-015-0680-0. [ Links ]
Castro O, Bennie J, Vergeer I, Bosselut G, Biddle SJH. How sedentary are university students?: a systematic review and meta-analysis. Prev Sci. 2020;21(3):332-43. doi: https://doi.org/10.1007/s11121-020-01093-8. [ Links ]
Peterson NE, Sirard JR, Kulbok PA, DeBoer MD, Erickson JM. Sedentary behavior and physical activity of young adult university students. Res Nurs Health. 2018;41(1):30-8. https://doi.org/10.1002/nur.21845. [ Links ]
Ekelund U, Steene-Johannessen J, Brown WJ, Fagerland MW, Owen N, Powell KE, et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality?: a harmonised meta-analysis of data from more than 1 million men and women. Lancet. 2016 Sep 24;388(10051):1302-10. doi: http://doi.org/10.1016/S0140-6736(16)30370-1 [ Links ]
Moulin MS, Irwin JD. An assessment of sedentary time among undergraduate students at a Canadian university. Int J Exerc Sci [Internet]. 2017;10(8):1116-29. Disponível em: https://digitalcommons.wku.edu/ijes/vol10/iss8/3 [ Links ]
Peltzer K, Pengpid S. Sleep duration and health correlates among university students in 26 countries. Psychol Health Med. 2016;21(2):208-20. doi: https://doi.org/10.1080/13548506.2014.998687. [ Links ]
Yadav A, Singh S. Relationship of chronotype to sleep pattern in a cohort of college students during work days and vacation days. Indian J Exp Biol. 2014[acesso 27 out. 2021];52(5):569-74. Disponível em: http://nopr.niscair.res.in/handle/123456789/28685?mode=full [ Links ]
Muniz LC, Schneider BC, Silva ICM da, Matijasevich A, Santos IS. Fatores de risco comportamentais acumulados para doenças cardiovasculares no sul do Brasil. Rev Saude Publica. 2012;46(3):534-42. doi: https://doi.org/10.1590/S0034-89102012005000021. [ Links ]
Paulitsch RG, Dumith SC, Susin LRO. Simultaneidade de fatores de risco comportamentais para doença cardiovascular em estudantes universitários. Rev Bras Epidemiol. 2017;20(4):624-35. doi: https://doi.org/10.1590/1980-5497201700040006. [ Links ]
Keller S, Maddock JE, Hannöver W, Thyrian JR, Basler H-D. Multiple health risk behaviors in German first year university students. Prev Med. 2008;46(3):189-95. doi: https://doi.org/10.1016/j.ypmed.2007.09.008. [ Links ]
Champion KE, Mather M, Spring B, Kay-Lambkin F, Teesson M, Newton NC. Clustering of multiple risk behaviors among a sample of 18-year-old Australians and associations with mental health outcomes: a latent class analysis. Front Public Health. 2018 May 7;6:135. doi: https://doi.org/10.3389/fpubh.2018.00135. [ Links ]
Received: April 09, 2021; Accepted: October 19, 2021
 This content is licensed under a Creative Commons Attribution 4.0 International License.
This content is licensed under a Creative Commons Attribution 4.0 International License.
