










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.30 no.4 Brasília dic. 2021 Epub 01-Nov-2021
http://dx.doi.org/10.1590/s1679-49742021000400011
Investigation of public health events of concern
Chickenpox outbreak among Venezuelan immigrants housed in shelters and occupancies in the state of Roraima, Brazil, 2019: a descriptive study
1 Ministério da Saúde, Programa de Treinamento em Epidemiologia Aplicada aos Serviços do Sistema Único de Saúde, Brasília, DF, Brazil
2 Ministério da Saúde, Coordenação-Geral do Programa Nacional de Imunizações, Brasília, DF, Brazil
3 Secretaria de Estado da Saúde de Roraima, Coordenação-Geral de Vigilância em Saúde, Boa Vista, RR, Brazil
4 Secretaria Municipal da Saúde de Boa Vista, Secretaria de Vigilância em Saúde, Boa Vista, RR, Brazil
Objective
To describe chickenpox outbreak among Venezuelan immigrants in shelters and occupancies in the municipalities of Pacaraima and Boa Vista, the state capital of Roraima, Brazil, and the control measures implemented.
Methods
This was a descriptive case series study, conducted between November 21 and December 13, 2019, based on secondary database obtained from the outbreak investigation made available by the General Coordination for the National Immunization Program. Descriptive analysis was performed using simple and relative frequency measurements, and measures of central tendency and dispersion were calculated.
Results
Of the 9,591 immigrants, 38 active cases and 1,459 susceptible to varicella were identified. With regard to active cases, 23 were female, and those aged under 9 years (17 cases) were the most affected.
Conclusion
People susceptible to chickenpox were identified during the investigation. Immunization actions aimed at reducing transmission were adopted, thus preventing severe cases, deaths and overload in local health care system.
Keywords: Chickenpox; Immunization; Disease Outbreaks; Vaccination; Descriptive Studies
Introduction
Chickenpox (varicella), caused by varicella-zoster virus (VZV), is a highly contagious disease. It can lead to complications such as skin infections, pneumonia, encephalitis and coagulopathy that in some cases require hospitalization.1,2 The incubation period for varicella from time of contact to rash onset is 10 to 21 days, and transmission occurs through direct contact with an individual with chickenpox or varicella-zoster, or by direct or indirect contact with respiratory tract secretions, skin lesions or contaminated objects.3 Its diagnosis is essentially clinical, and the main symptoms are rash, mild fever, headache, anorexia and vomiting.2 Varicella is a vaccine-preventable disease.
The World Health Organization (WHO) estimates that 4.2 million people are hospitalized each year for severe complications of varicella, and 4,200 die worldwide.4 In Brazil, hospitalizations due to chickenpox present a seasonal pattern, being higher between September and November.5 According to the Ministry of Health, in the period between 2012 and 2017, 602,136 cases and 38,612 hospitalizations due to chickenpox were reported in Brazil;6 from 2012 to 2016, 649 deaths were recorded, and they occurred more frequently among children aged 1 to 4 years (33.4%).6
Chickenpox vaccine was incorporated into the national vaccination schedule of the National Immunization Program (PNI) in 2013, as a combined vaccine, also known as tetravalent (measles, mumps, rubella and chickenpox) and, as of 2018, a second booster dose of tetravalent was administered in four-year-old children, and could also include those up to 6 years of age.7
Chickenpox should comprise the monitoring of important events for Brazilian Public Health, given that some Latin American countries, including Venezuela, do not provide vaccines against the disease in their public health systems.4
There has been an increase in the migration flows to the municipality of Pacaraima, on the border between Brazil and Venezuela, since 2013, which has been intensified since 2017, when it was recorded the entry of 111,581 Venezuelans into Brazil, due to the socio-political and humanitarian crisis in that country.8 The knowledge of the vulnerability of immigrants, as well as technical information on chickenpox outbreak among this population, have contributed to the planning and implementation of more effective actions in the region.
The objective of this study was to describe chickenpox outbreak among Venezuelan immigrants in shelters and occupancies in the municipalities of Pacaraima and Boa Vista, Roraima, Brazil, and the control measures implemented.
Methods
This was a descriptive case series study, which analyzed anonymized secondary data based on the investigation of the chickenpox outbreak among Venezuelan immigrants obtained from shelters and occupancies in the municipalities of Pacaraima and Boa Vista in the state of Roraima, in 2019. The database used in this study was made available in August 2020 by the General Coordination for the National Immunization Program (CGPNI).
The state of Roraima is comprised of 15 municipalities. Located in the North Region of Brazil, it has an estimated population of 631,181 inhabitants, shares a border with Venezuela, Guyana, and, with the Brazilian states of Amazonas and Pará.9 Boa Vista is its capital; Pacaraima is located in the extreme north of the state, 215 km from the capital, on the border between Brazil and Venezuela. It is one of the main gateways for Venezuelans into Brazil.9 In the year when this study took place, the two municipalities represented approximately 70.0% of the population of Roraima State.9
In 2019, the CGPNI took action in the face of an outbreak of chickenpox in the municipalities of Boa Vista and Pacaraima. The research participants were Venezuelan immigrants housed in 14 shelters and 14 occupancies in both municipalities, from November 21 to December 13, 2019.
For this investigation, an active search was carried out in all shelters and occupancies that had registered chickenpox cases. A semi-structured paper form was used, including variables of socioeconomic, demographic, clinical and epidemiological data.
For participant selection, the following definitions were adopted:
active case of chickenpox - an individual who presented maculo-papulovesicular rash, without other apparent cause, during the period of transmission of the disease, between November 21 to December 13, 2019; and
susceptible to chickenpox - an individual without proof of chickenpox vaccination, who did not have the disease in the past or when he or she was under 15 months of age.
Individuals who presented clinical manifestations compatible with chickenpox in the period from five to 26 days after getting the vaccine were excluded from the study because it was possibly vaccine side effects. Other definitions of events or situations used in the study were:
chickenpox outbreak - occurrence of two or more chickenpox cases, between November 21 to December 13, 2019;
vaccinated individual - an individual who, at 15 months of age, received a dose of tetravalent (chickenpox, measles, mumps and rubella) vaccine or a dose of triple viral vaccine and the monovalent varicella vaccine, and/or individual who, between 4 and 6 years of age, received a booster dose of monovalent varicella;
shelters - places that were adapted or built by the Brazilian Ministry of Defense, which provide temporary residence for immigrants;
occupancies - public buildings illegally occupied by immigrants; and
Chickenpox complications - hematological, neurological, respiratory, cutaneous, hepatic, urinary and/or bone complications resulting from chickenpox.
Socioeconomic and demographic variables analized were:
- symptom onset date;
- sex (male; female);
- age (in years: <2, 2 to 9; 10 to 19; 20 to 29; 30 to 39; 40 to 49);
- schooling (illiterate; complete elementary school; incomplete elementary school; complete high school; incomplete high school; complete higher education; incomplete higher education);
- had a job in Venezuela (yes; no);
- has a paid activity in Brazil (yes; no);
- year of family entry into Brazil;
- was assisted by Operation Welcome (yes; no);
- number of people per family;
- number of chickenpox cases in the family in 2019;
- intention to return to Venezuela (yes; no); and
- reasons not to return to Venezuela (crisis in his/her country; chose to live in Brazil).
Clinical and epidemiological variables included in the study were:
- set of signs and symptoms, which may be rash (yes; no), fever (yes; no), headache (yes; no), general malaise (yes; no), loss of appetite (yes; no), cough (yes; no), runny nose, and vomiting (yes; no);
- area of the body where the rash began (face; extremities; trunk; back; scalp);
- generalized rash at the time of the interview (yes; no);
- seeking medical care (yes; no);
- had complications (yes; no);
- has vaccination card (yes; no);
- vaccinated against chickenpox (yes; no);
-received information about the importance of vaccination (yes; no);
- types of complications (encephalitis; pneumonia; skin infection; ear infection);
- interval between the date of the rash onset and the date of entry into Brazil (number of full days).
All prevention and control actions implemented by the outbreak investigation teams had the support of the municipal and state teams of the PNI, totaling 15 nursing technicians. Among these actions, Varicella- Zoster immune globulin (human) (VariZIG) was administered in pregnant women and those under 1 year of age, and vaccination blockade was performed with tetravalent or monovalent vaccines, according to the technical determinants of PNI.
The analyses were performed using descriptive statistics, adopting simple and relative frequency measurements. Measures of central tendency (median) and dispersion (minimum and maximum values) were also calculated. The Epi Info 7.2™ and Excel 2013® were used. The results of the analyses were presented jointly for both municipalities - Pacaraima and Boa Vista - due to the transience of the majority of immigrants who spent little time in Pacaraima and chose Boa Vista as their destination.
The study project was submitted to the Brazil’s National Committee for Ethics in Research (CONEP) of the Ministry of Health and was approved. CONEP Opinion No. 4,416,520. November 24, 2020.
Results
During the study period, 9,591 immigrants from Venezuela living in the 14 shelters and 14 occupancies in the municipalities of Pacaraima and Boa Vista were identified. 1,500 immigrants lives in the shelters and occupancies where active cases and susceptible to chickenpox were found. Of these, 41 were considered active cases of chickenpox, initially, and three of which were discarded due to the possibility of being vaccine side effects, remaining 38 cases; 1,459 comprised the group of people for whom prevention and control measures were implemented during the fieldwork (Figure 1). Moreover, during the study, no deaths were recorded among the aforementioned active cases of chickenpox.
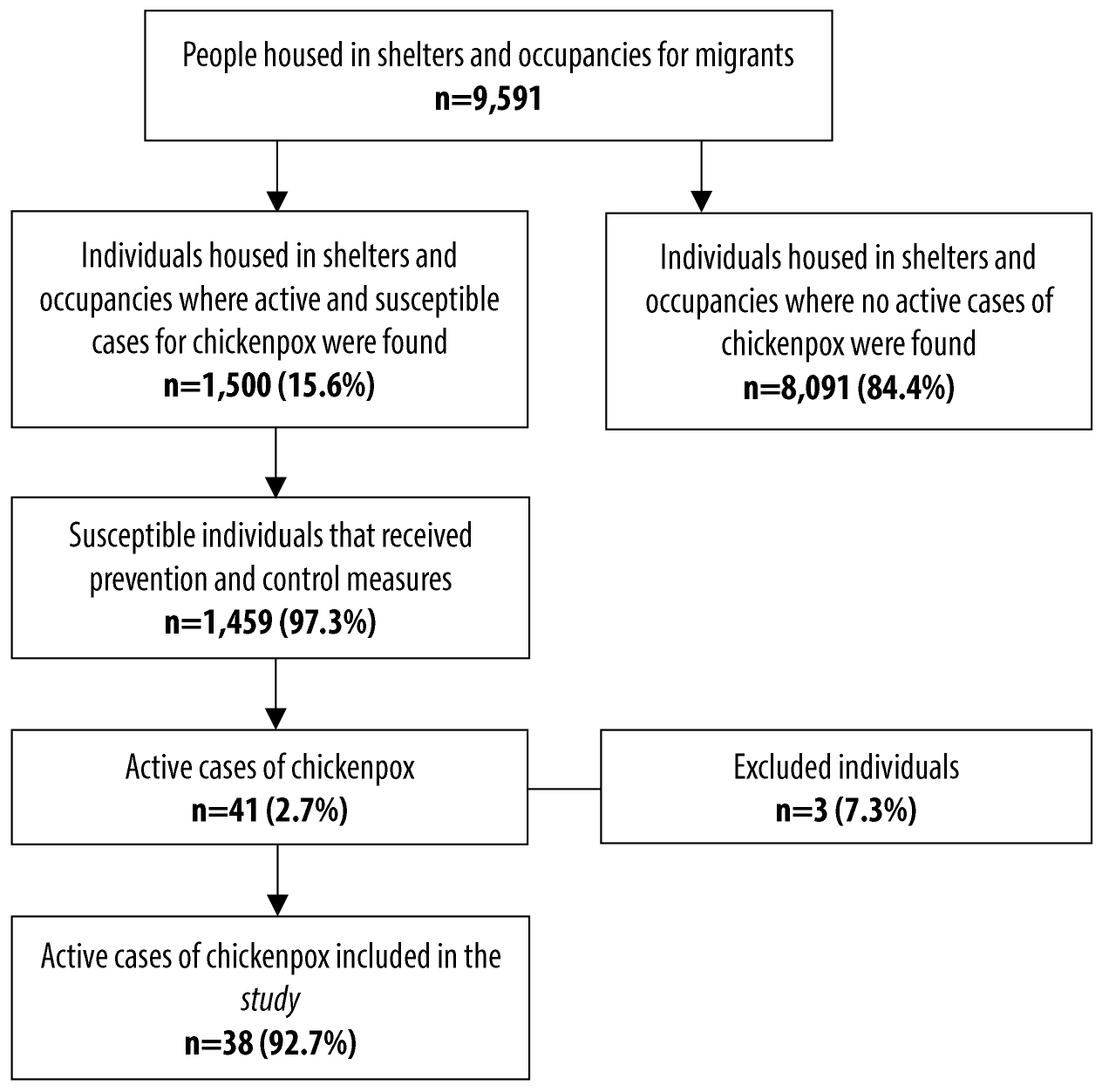
Figure 1 Flow chart of active search for active cases of chickenpox (n=38) in Pacaraima and Boa Vista, state of Roraima, Brazil, November 21 - December 13, 2019
Of the 38 cases evaluated, 23 were female; 17 were children under 9 years of age, being this age group the most affected, while 13 were people aged 10 to 19 years. As for schooling, 14 had incomplete elementary school. Regarding professional life, eight had no job in Venezuela and 11 did not work in Brazil (Table 1).
Table 1 Sociodemographic characteristics of chickenpox cases (n=38) in Boa Vista and Pacaraima, Roraima, Brazil, November 21 - December 13, 2019
| Sociodemographic characteristics | N |
|---|---|
| Sex | 38 |
| Male | 15 |
| Female | 23 |
| Schooling | 25 |
| Illiterate | 1 |
| Complete elementary school | 3 |
| Incomplete elementary school | 14 |
| Complete high school | 2 |
| Incomplete high school | 2 |
| Complete higher education | 1 |
| Incomplete higher education | 2 |
| Age group (in years) | 38 |
| Under 1 year old | 6 |
| 1 a 9 | 11 |
| 10 a 19 | 13 |
| 20 a 29 | 6 |
| 30 a 39 | 1 |
| 40 a 49 | 1 |
| Job in Venezuela | 14 |
| Yes | 6 |
| No | 8 |
| Has a paid activity in Brazil | 12 |
| Yes | 1 |
| No | 11 |
All 38 cases presented rash, 23 had fever, 12 had headache and 10 reported malaise. In 12 of them, papulovesicular rash started on the face and 30 presented generalized rash. Regarding medical care, 22 reported not having sought medical care; one individual presented skin infection as a complication (Table 2).
Table 2 Clinical and healthcare characteristics of chickenpox cases (n=38) in Boa Vista and Pacaraima, Roraima, Brazil, November 21 - December 13, 2019
| Clinical characteristics | N |
|---|---|
| Signs and symptoms | |
| Rash (papulovesicular) | 38 |
| Fever | 23 |
| Headache | 12 |
| General malaise | 10 |
| Loss of appetite | 5 |
| Cough | 3 |
| Runny nose | 2 |
| Vomiting | 1 |
| Area of the body where the rash began | |
| Face | 12 |
| Extremities | 9 |
| Trunk | 9 |
| Back | 6 |
| Scalp | 2 |
| Generalized rash | |
| Yes | 30 |
| No | 8 |
| Sought for medical care | |
| Yes | 16 |
| No | 22 |
| Had complications | |
| Yes | 1 |
| No | 37 |
Of the 38 cases, 31 had a vaccination card. Of these, 12 were not vaccinated and 18 had no indication of vaccination. Of the total cases, 25 reported having already received information about the importance of chickenpox vaccine (Table 3).
Tabela 3 Immunization characteristics of chickenpox cases (n=38) in Boa Vista and Pacaraima, Roraima, Brazil, November 21 - December 13, 2019
| Immunization characteristics | N |
|---|---|
| Has vaccination card | |
| Yes | 31 |
| No | 7 |
| Varicella vaccine | 31 |
| Yes | 1 |
| No | 12 |
| Does not apply | 18 |
| Received information about the importance of varicella vaccine | |
| Yes | 25 |
| No | 13 |
Taking into consideration the families with active cases of chickenpox during the study period, 184 people in total, with a median of four people per family, ranging from one to 13 individuals. In 2019, 84 members of the families were infected with chickenpox. With regard to the 37 immigrant families, 29 entered Brazil in 2019, through the border between Venezuela and the municipality of Pacaraima, were assisted by Operation Welcome and then went to Boa Vista. The median time from entry into Brazil to papulovesicular rash onset was 93 days, ranging from 24 to 1,095 days. Regarding the householders, 26 did not intend to return to Venezuela and of these, 15 reported being due to the crisis in their country.
It is also worth mentioning that 1,459 people received some kind of care related to prevention and control measures implemented during the fieldwork. Of these, 125 were children younger than 9 months, 53 pregnant women received a dose of Varicella- Zoster immune globulin (human) (VariZIG) and 1,281 received a dose of varicella-containing vaccine (tetraviral or monovalent) as vaccine blocking action.
Discussion
The findings on chickenpox outbreak in the municipalities of Pacaraima and Boa Vista, in the state of Roraima, showed that, taking into consideration the large population identified, the number of active cases was much lower than expected for the local scenario. The active cases were mostly related to children under 9 years of age and adolescents/young adults, corroborating the results of a study conducted in 2017, in Mexico, where a higher prevalence was found among individuals under 9 years of age.10
The number of pregnant women and children younger than 9 months observed in this study points to a serious public health problem, given the high risk of abortion and fetal malformation to which exposed pregnant women are susceptible, as well as the occurrence of severe cases, complications and even death.1
Almost all cases in this study presented mild symptoms and most of them did not seek medical care because chickenpox usually presents a benign course.11 However, a study conducted in France from 1987 to 2002 showed that chickenpox, often considered as a mild disease, can be responsible for severe complications in immunocompetent children.12
Most of the cases in this study reported having a vaccination card but they were not vaccinated against the disease. The literature suggests that migrant populations generally experience a higher burden of vaccine-preventable diseases and lower immunization rates.13 As of 2018, eleven Latin American countries implemented universal vaccination against chickenpox. However, data on the impact of vaccination are available only for Uruguay, Costa Rica and Brazil.14 In Uruguay, six years after the implementation of vaccination, at the end of 1999, there was an 81% reduction in the proportion of hospitalizations of children between 1 and 4 years of age related to chickenpox.15
Another study, conducted in Costa Rica in 2007, showed a decrease of 79.1% in reported cases and 87% in hospitalizations of children under 5 years of age. As for Brazil, vaccinated children aged 1 to 4 years, after three years of vaccine implementation in 2013, a 47.6% reduction in hospitalizations related to the disease was observed.16 This information confirms the importance of vaccination for chickenpox control.
More than half of the migrant families taking part in this study reported having been assisted by Operation Welcome, from which, when indicated, they received the following vaccines: triple viral, yellow fever, diphtheria, tetanus and pertussis (DTP) and diphtheria-tetanus (dT). Since the beginning of this migratory process in the state of Roraima, in 2017, the monovalent varicella vaccine has been also administered at the time of welcoming families. In 2013, according to PNI guidelines, vaccination began to be performed by the Primary Health Care of the Brazilian National Health System (SUS) in the municipalities of Pacaraima and Boa Vista.17
A Japanese study conducted with international adult immigrants between 2012 and 2016, showed that 44% of refugees had varicella infections after arrival in Denmark, thus it was deemed necessary to check VZV immunity for immigrants before they entered that country.18 The study conducted in Roraima, which analyzed the median time from the entry into Brazil to the rash onset, showed that the immigrants with chickenpox in Pacaraima and Boa Vista were probably infected in Brazil. This finding reinforces the importance of vaccination on the border at the time of entry into the country, given that the varicella vaccine in Venezuela was only available in the private health network by 2019.4
The large number of people who shared the same shelter, mostly unvaccinated, or who are not in the age group eligible to receive tetra viral vaccine, may have contributed to the permanence of chickenpox cases in shelters and occupancies, corroborating the results of a study conducted in Egypt, in the period from 2016 to 2017, when it was concluded that the incidence of chickenpox may be related to population density.19
Large-scale administration of immune globulin in children younger than 9 months and pregnant women, in addition to intensification of vaccination activities, were strategic actions aimed at interrupting transmission of the disease and preventing complications among children younger than 9 months, as well as possible congenital anomalies. This measure, implemented in Roraima, was also identified in a study conducted in 2012, during a chickenpox outbreak among African immigrants. At that time, early vaccination was considered necessary for all, when an outbreak was detected in closed-residential settings.20
As a limitation of this study, classification bias may have occurred, given the possibility of some excluded individuals having been active cases of chickenpox, underestimating the results.
Taking these results, it can be concluded that people susceptible to chickenpox were identified during this investigation, leading to the adoption of immunization actions aimed at controlling transmission, preventing severe cases and deaths, and overload in the local healthcare system. We have highlighted, in this study, the importance of actions intended to monitor the health status of those people, the possibility of timely treatment and the adoption of effective measures in order to control varicella-zoster virus infection.
Referências
1. Berezin EN, Feldman C. Varicela-zoster. In: Focaccia R, Veronesi R, editores. Tratado de infectologia. 5a ed. Sao Paulo: Atheneu; 2015. p. 723-34. [ Links ]
2. Ministério da Saúde (BR), Secretaria de Vigilância em Saúde. Guia de vigilância em saúde: volume único. 3a ed. Brasília, DF: MS; 2019. [ Links ]
3. Chan JY, Tian L, Kwan Y, Chan W, Leung C. Hospitalizations for varicella in children and adolescents in a referral hospital in Hong Kong, 2004 to 2008: a time series study. BMC Public Health. 2011 May 23:11(1):366. doi: https://doi.org/10.1186/1471-2458-11-366. [ Links ]
4. Arlant LHF, Garcia MCP, Avila Aguero MLA, Cashat M, Parellada CI, Wolfson LJ. Burden of varicella in Latin America and the Caribbean: findings from a systematic literature review. BCM Public Health. 2019 May 8;19(1):528. doi: https://doi.org/10.1186/s12889-019-6795-0. [ Links ]
5. Mota AM, Carvalho-Costa FA. Varicella zoster virus related deaths and hospitalizations before the introduction of universal vaccination with the tetraviral vaccine. J Pediatr (Rio J). 2016;92(4):361-6. doi: https://doi.org/10.1016/j.jpedp.2016.05.009. [ Links ]
6. Ministério da Saúde (BR). Saúde de A a Z [Internet]. Brasília, DF: Secretaria de Vigilância em Saúde; 2020 [citado 18 set. 2020]. Disponível em: http://saude.gov.br/saude-de-a-z/varicela-catapora [ Links ]
7. Silva ALM, Gouvêa JS, Silva ANMR, Machado LFA, Monteiro JC, Azevedo VN, et al. Impacto da vacinação contra varicela nos índices de morbimortalidade no Brasil. Braz J Health Rev. 2020;3(4);7236-49. doi: https://doi.org/10.34119/bjhrv3n4-003. [ Links ]
8. Câmara dos Deputados (BR). Primeiro relatório da comissão externa crise na fronteira da Venezuela com o Brasil [Internet]. Brasília, DF: Câmara dos Deputados; 2008 [citado 18 set. 2020]. Disponível em: https://www.camara.leg.br/proposicoesWeb/prop_codteor=1774525&filename=REL+1/2019+CEXVENEZ [ Links ]
9. Instituto Brasileiro de Geografia e Estatística. Cidades e estados [Internet]. Brasília, DF; 2020 [citado 18 set. 2020]. Disponível em: https://ibge.gov.br/ [ Links ]
10. Vázquez M, Cravioto P, Galván F, Guarneros D, Pastor VH. Varicela y herpes zóster: retos para la salud pública. Salud Publica Mex. 2017;59(6):650-6. doi: https://doi.org/10.21149/7997. [ Links ]
11. Losurdo G, Bertoluzzo L, Canale F, Timitilli A, Bondi A, Castagnola E, et al. Varicella and its complications as cause of hospitalization. Infez Med. 2005;13(4):229-34. Disponível em: https://europepmc.org/article/med/16388278. [ Links ]
12. Mallet E, Delalande-Dutilleul L, Marguet C, Mouterde O. Evaluation of varicella complications through a retrospective hospital survey in a paediatric center over 16 years in France. Arch Pediatr. 2004 Sep;11(9):1145-51. doi: http://doi.org/10.1016/j.arcped.2004.07.002. [ Links ]
13. Charania NA, Gaze N, Kung JY, Brooks S. Vaccine-preventable diseases and immunisation coverage among migrants and non-migrants worldwide: a scoping review of published literature, 2006 to 2016. Vaccine. 2019 May 6;37(20):2661-9. doi: https://doi.org/10.1016/j.vaccine.2019.04.001. [ Links ]
14. Ávila-Agüero ML, Beltrán S, Del Castillo JB, Castillo Diaz ME, Chaparro LE, Deseda C, et al. Varicella epidemiology in Latin America and the Caribbean. Expert Rev Vaccines. 2018;17(2):175-83. doi: https://doi.org/10.1080/14760584.2018.1418327. [ Links ]
15. Quian J, Rüttimann R, Romero C, Dall'Orso P, Cerisola A, Breuer T, et al. Impact of universal varicella vaccination on 1-year-olds in Uruguay: 1997-2005. Arch Dis Child. 2008;93(10):845-50. doi: http://dx.doi.org/10.1136/adc.2007.126243. [ Links ]
16. Avila-Aguero ML, Ulloa-Gutierrez R, Camacho-Badilla K, Soriano-Fallas A, Arroba-Tijerino R, Morice-Trejos A. Varicella prevention in Costa Rica: impact of a one-dose schedule universal vaccination. Expert Rev Vaccines. 2017;16(3):229-34. doi: https://doi.org/10.1080/14760584.2017.1247700. [ Links ]
17. Ministério da Saúde (BR), Secretaria de Vigilância em Saúde. Calendário vacinal. Brasília, DF: MS; 2020. [ Links ]
18. Takaya S, Kutsuna S, Katanami Y, Yamamoto K, Takeshita N, Hayakawa K, et al. Varicella in adult foreigners at a referral hospital, Central Tokyo, Japan, 2012-2016. Emerg Infect Dis. 2020;26(1):114-7. doi: https://dx.doi.org/10.3201/eid2601.170565. [ Links ]
19. Ibrahim EG, Abdel Wahed WY, Eid HM, Deeb WS. Seroprevalence of varicella-zoster virus among pregnant women in Fayoum Governorate, Egypt. J Egypt Public Health Assoc. 2019;94(1):2. doi: https://doi.org/10.1186/s42506-018-0002-5. [ Links ]
20. Haas EJ, Dukhan L, Goldstein L, Lyandres M, Gdalevich M. Use of vaccination in a large outbreak of primary varicella in a detention setting for African immigrants. Int Health. 2014 Sep;6(3):203-7. doi: https://doi.org/10.1093/inthealth/ihu017. [ Links ]
Received: March 15, 2021; Accepted: July 18, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
