










Serviços Personalizados
Journal

Artigo
 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Enviar este artigo por email
Enviar este artigo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares em
SciELO
Similares em
SciELO
Compartilhar

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versão impressa ISSN 1679-4974versão On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.31 no.1 Brasília 2022 Epub 14-Mar-2022
http://dx.doi.org/10.1590/s1679-49742022000100004
Original Article
Validation of a reduced instrument Diabetes-21 for assessing health-related quality of life among people with diabetes
1Universidade Estadual de Montes Claros, Departamento de Métodos e Técnicas Educacionais, Montes Claros, MG, Brazil
2Faculdades Unidas do Norte de Minas, Departamento de Enfermagem, Montes Claros, MG, Brazil
3Universidade Estadual de Montes Claros, Programa de Pós-Graduação em Ciências da Saúde, Montes Claros, MG, Brazil
Objective
To analyze the validity, reliability and interpretability of a short form instrument for assessing health-related quality of life among people with diabetes mellitus.
Methods
This was a validation study, comprised of the adaptation phases of the Diabetes-39 instrument (consisting of 5 domains and 39 items), pre-test, structural validity analyses (exploratory and confirmatory), reliability, concurrent validity and interpretability.
Results
The factorial structure of the short final version differed from the original instrument. The items were reduced from 39 to 21 and domains from 5 to 4. The factor loading, in exploratory and confirmatory analyses, ranged between 0.41 and 0.90 and between 0.51 and 0.89, respectively. Reliability was adequate (Cronbach’s alpha=0.91; Kappa≥0.60 in all items; intraclass correlation coefficient =0.91).
Conclusion
Diabetes-21, a short form instrument, was considered valid, reliable and interpretable for assessing health-related quality of life among people with diabetes mellitus.
Keywords: Diabetes Mellitus; Quality of Life; Reproducibility of Results; Factor Analysis, Statistical
Study contributions
Main results
Diabetes-21 was considered to be valid, reliable and interpretable for assessing health-related quality of life among people with diabetes attending primary care services.
Implications for services
It is an instrument that has potential for use by health professionals in providing care for people with diabetes, since it is capable of identifying impaired quality of life, as well as enabling health actions to be implanted.
Perspectives
It is expected that Diabetes-21 will be used in future research and also by health services to identify people in need of intervention, especially since it requires less application time.
Introduction
Diabetes mellitus is one of the leading causes of premature and preventable deaths in Brazil. The quality of life of the population frequently affected by health problems associated with diabetes reinforces the need to evaluate this condition, in addition to the follow-up and clinical treatment of the disease.1
The quality of life of people with diabetes mellitus has been assessed by the Diabetes-39 instrument, developed in the United States and adapted for Brazil. It is a multidimensional scale, comprised of 39 items that assess five domains of the quality of life of people with diabetes: energy and mobility; diabetes control; anxiety and worry; social burden; and sexual functioning. The higher the score obtained on the scale, the greater the negative impact on people’s quality of life.2,3
Diabetes-39 has been considered an adequate instrument to assess the quality of life of this population. However, in its cross-cultural adaptation for the Brazilian population, internal consistency and construct validity (convergent and discriminant validity) were the only psychometric properties assessed, therefore it is necessary to analyze its stability, structural validity (exploratory and confirmatory factor analyses) and interpretability.3 Although the Brazilian version has maintained the validity and reliability of the original version, it is a long instrument that requires considerable time and adequate environment for its application. The limitations of the instrument may discourage or create barriers to participation, both for people with diabetes and health professionals, while short questionnaires are rapidly applied, practical and economical.4-6
The validation of the efficacy of instruments that assess health conditions is crucial, as they may present limitations in their psychometric properties.7-9 A group of reseachers who are experts in the evaluation of measurement instruments developed the ‘COnsensus-based Standards for the selection of health Measurement INstruments’ (COSMIN), a checklist for analyzing the psychometric properties of instruments that assess health conditions. COSMIN, present in four domains, evaluates the validity, reliability, responsiveness and interpretability of the instruments.8,9 Epidemiological studies using instruments that have already been tested, regarding their validity and reliability, contribute to evidence-based practices in healthcare.10
Diabetes-39, when assessing the health-related quality of life of people with diabetes, contributes to identifying care needs and, consequently, reducing the risk of complications arising from the disease. A short version of this instrument may contribute to a shorter time of its application in epidemiological studies. In addition, during the validation process of an instrument, factor loadings or weights are obtained, which enable the estimation of a score in line with the importance that each question/item exerts on the construct. Therefore, considering the weight of each question/item in the interpretation of the instrument can lead to a more reliable result.9
This study aimed to analyze the validity, reliability and interpretability of a short form instrument for assessing health-related quality of life among people with diabetes mellitus.
Methods
Study design
This was a cross-sectional validation study conducted between 2016 and 2018, with users of Family Health Strategy (FHS) units in the city of Montes Claros, state of Minas Gerais, Brazil.
Context
Montes Claros, located in the north of Minas Gerais, is the sixth largest city in the state by population, occupies an area of 3,589,811km2 and had a human development index (HDI) of 0.770 in 2010. In 2020, its population was estimated at 413,487 inhabitants.11
Population and sample
The municipal management responsible for the FHS was contacted in order for us to obtain the lists with the enumeration of the family health strategy teams centers. Of the 73 health centers in Montes Claros, four were selected using simple random draw. Of these, two were used to assess the reliability and concurrent validity, and the other two health centers were used to estimate the structural validity and interpretability.
The managers of the FHS centers that had been randomly selected provided lists with the names of people with diabetes who were registered and assisted by FHS teams. Based on these data, people aged 18 years or older, registered in the FHS and who had diabetes, were considered eligible for this study. Those with three or more comorbidities, whose native language was not Portuguese, who had visual or hearing impairment and presented signs of alcohol or drug intoxication at the time of the interviews; and the elderly with cognitive impairment, which could be verified using the mini mental state examination, were excluded.12 The instruments that presented three or more incomplete data were considered losses.
Thus, the study sample was divided into two different groups:
The reliability group (internal consistency and stability) and concurrent validity of the instrument, in which 50 people with diabetes registered in the health units were selected, given that the samples consisting of 50 to 100 people were sufficient for these stages;13 and
The group of exploratory and confirmatory factor analyses, and interpretability, in which the participants were selected through the calculation of a probabilistic sampling for an infinite population, taking into consideration the proportion of 50% of people with diabetes and quality of life impairment, 95% confidence level, sampling error of 6 percentage points and an increase of 10% for losses.14
Variables
The sociodemographic and economic status investigated were: sex (male; female); age group (in years, categorized into quartiles: 22 to 54; 55 to 61; 62 to 68; 69 or over); schooling (in complete years of study: 0; 1 to 4; 5 to 8; 9 to 11; 12 or more); marital status (married/stable union; single/widowed/divorced/ separated); race/skin color (White; Asian; Black; Brown; Indigenous; had no information); family income [up to BRL 998.00; above BRL 998.00 (minimum wage at the time of the study)]; and spending on medicines (no; yes).
Cognitive impairment, exclusion criteria of the study, was defined according to different cut-off points - based on schooling - using the mini mental state examination: 13 for people without education; 18 for low and medium schooling levels (1 to 8 incomplete years of schooling); and 26 for high schooling level (8 or more years of schooling).12
Participants whose scores fell below the lower limit of 95% confidence interval (95%CI) for the mean in each dimension were classified as having impaired quality of life (yes; no).
Data sources and measurement
Diabetes-39, the instrument that was assessed, was culturally adapted to Brazilian Portuguese.3 Its 39 items are distributed into five domains: energy and mobility; diabetes control; social burden; sexual functioning; anxiety and worry. Its short version was called Diabetes-21.
In addition, a change in the response scale was made (1 = was not affected; 2 = little affected; 3 = sometimes affected; 4 = very affected; 5 = extremely affected), replacing the original proposal of Diabetes-39 (horizontal bar divided into boxes, that were numbered from 1 to 7).3
To verify the validity, reliability and interpretability of Diabetes-21, the following steps were applied: pre-test, structural validity (exploratory and confirmatory factor analysis), concurrent validity, reliability (internal consistency and stability) and interpretability.
For the pre-test, 20 individuals with diabetes who were selected using convenience sampling and registered in the first health unit selected to compose the sample for the study, were interviewed. The objective of this stage was to analyze the applicability of the instrument before its use in the final sample of the study. After the pre-test, the interviewers were invited to hold a meeting with the researchers to report their perception regarding the application of the instrument with a new response scale. This meeting was conducted as a focus group, comprised of ten judges who worked as researchers and/or providing care to people with diabetes (2 endocrinologists, 2 epidemiologists, 2 nurses, 1 physiotherapist, 1 nutritionist, 1 physical education teacher and 1 dentist).
In addition to Diabetes-39, this study used the short form of World Health Organization Quality Of Life - BREF (WHOQOL-BREF). It is an instrument for assessing quality of life, but it is not specific for people with diabetes, consists of two general questions and 26 related to four domains: physical, psychological, environmental and social. Their answers consider a Likert scale that measures intensity, frequency, capacity and evaluation. The scores of each domain were transformed into a scale from 0 to 100, reversed and dichotomized by the lower limit of 95%CI for the mean. Individuals whose scores fell below this limit, in each domain, were classified as having impaired quality of life.15
Bias control
The participants - from all stages of the study - were interviewed at home, individually and in a reserved room.
The measurement bias was minimized through the theoretical and practical training of the interviewers. They were trained to minimize the intrinsic subjectivity of the interviews. The training included people with diabetes who did not take part in the study.
Statistical analyses
Descriptive analysis of categorical variables was performed, estimating absolute and relative frequencies. For the continuous variables, the mean and standard deviation (SD) were calculated, and the 95%CI was estimated, in addition to minimum and maximum values.
To estimate concurrent validity, Spearman’s correlation coefficient was used to verify the association between the variables of the instruments (WHOQOL-BREF and Diabetes-21; Diabetes-39 and Diabetes-21), given that the data did not present normal distribution. Then, the correlation test was applied between the scales generated by these same instruments. The correlations between Diabetes-21 scores and the age and schooling of the participants were also analyzed.
The reliability of the instrument was measured through internal consistency and stability. Internal consistency was tested using Cronbach’s alpha calculation (α), and values of ≥0.7 were considered acceptable.13 To estimate the stability of the instrument, the test-retest was applied, in which the ability of the instrument to produce similar results was verified, measuring the event among the same participants in different situations, by calculating the intraclass correlation coefficient. The test-retest was applied with an interval of 7 to 14 days.5,13 The weighted Kappa coefficient was calculated to assess the agreement of each of the items of the short version of the instrument, considering as acceptable the cutoff point ≥0.60.16
The evaluation of the structural validity of Diabetes-39 was performed using exploratory and confirmatory factor analyses:
Regarding exploratory factor analysis, the correlation matrix of the instrument variables was analyzed (considered significant p-value<0.05), along with the following tests and analyses:17-19 (i) the Kaiser-Meyer-Olkin test (ranging from 0 to 1; values <0.50 indicate inadequate method);18 (ii) Bartlett’s scouting test (p-value<0.05 indicates that the correlation matrix differs from an identity matrix and therefore there are relationships among the variables included in the analysis); (iii) the identification of commonalities (estimation of the shared or common variance between variables) and their contribution to each item (>0.5 acceptable levels of explanation; lower or equal values indicate that the item should be excluded); (iv) the analysis of the factor loadings of each item regarding the extracted components (0.40 as an acceptable limit of the contribution of the item to the creation of the factor); (v) the definition of the number of factors, based on the graphical evaluation of the scree plot (graph of eigenvalues versus number of factors in the order of extraction), in the verification of the eigenvalue (greater than 1) and observation of the cumulative percentage of the total variance; and (vi) principal component analysis, in which the variables were rotated - orthogonal rotation (varimax).
With the regard to confirmatory factor analysis, the maximum likelihood method was used.18 To adjust the model, the following indices were considered:19,20 (i) the ratio between Pearson’s chi-square and the degrees of freedom (excellent = 1-2; good = 2-3; acceptable = 4-5; rejected = >5); (ii) the quality index of the adjustment (adequate values: ≥0.90); (iii) the root mean square error of approximation (adequate <0.08); (iv) the comparative fit index (adequate values: ≥0.90); and (v) the Tucker-Lewis index (adequate values: ≥0.90).
The order of the questions was reorganized in the short form instrument. To interpret it, we used the weighted additive model, taking into consideration the factor loading attributed to each item, for example: Question 9 x 0.63 (factor loading).13 These estimates were performed through the ratio between the sum of different items that constitute the factors, multiplied by the respective factorial weights (factor loading), and the sum of the factorial weights that were attributed, being considered the best quality of life that one that achieved the lowest score, given that it is a Likert-type response scale, from 1 (not affected) to 5 (extremely affected). The variable was transformed into a binary categorical variable when a cutoff point was considered; as such, the values were transformed into a scale from 0 to 100 14,21,22 reversed and dichotomized by the lower limit of 95%CI for the mean. Thus, participating individuals who scored below this limit in each domain (energy and mobility, 35.91; diabetes control and social burden, 32.49; sexual functioning, 31.47; anxiety and worry, 38.10) were considered with impaired quality of life.22
Statistical Package for the Social Science (SPSS) version 24.0 and Microsoft Excel were used for all analyses.
Ethical aspects
The study was approved by the Research Ethics Committee of the Universidade Estadual de Montes Claros (CEP/Unimontes) on March 22, 2016: Opinion No. 1,461,818; Certificate of Submission for Ethical Appreciation (CAAE) No. 54417616.1.0000.5146. All participants signed the Free and Informed Consent Form.
Results
The mean age of the 50 participants of the verification stage of reliability and concurrent validity was 61 years (SD=11.1; minimum value, 36; maximum value, 87) and mean years of schooling of 7.5 (SD=3.9; minimum value, 0; maximum value, 12). At this stage, there were no exclusions, losses or refusals of the participants.
A total of 297 participants were invited to structural analysis and interpretability stage (Figure 1). However, due to 5 losses and 4 refusals, 288 people with diabetes, whose mean age was 60 years (ranging from 22 to 92 years: SD=11.7) took part in the study. The sociodemographic, economic and quality of life information of the participants can be found in Table 1.
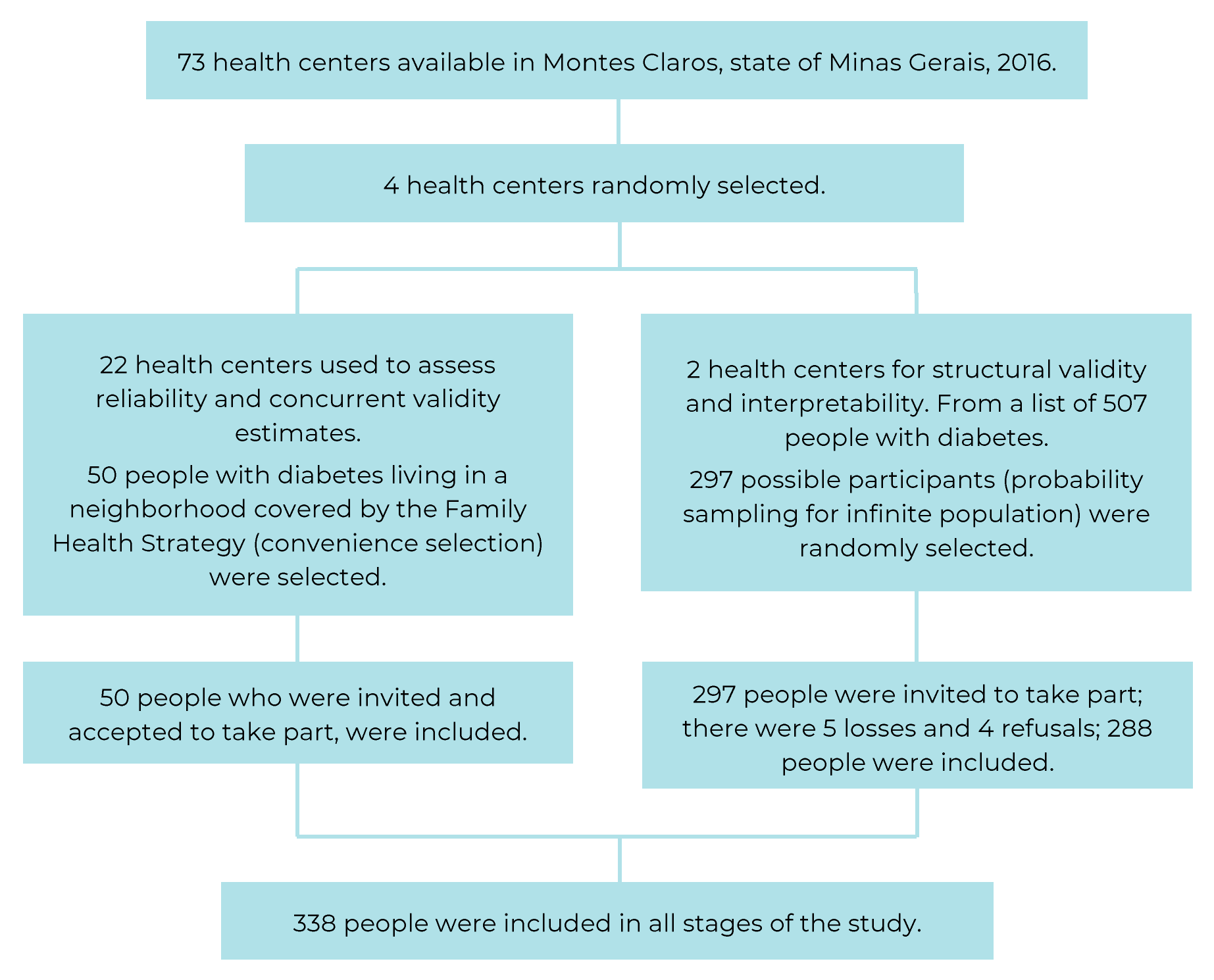
Figure 1 Selection process of people with diabetes mellitus assisted by the Family Health Strategy, Montes Claros, state of Minas Gerais, Brazil, 2019
Table 1 Distribution of sociodemographic and economic characteristics and quality of life among people with diabetes mellitus (n=338) assisted by the Family Health Strategy, Montes Claros, state of Minas Gerais, Brazil, 2019
| Sociodemographic and economic status | Study Population | Quality of life affected in the Diabetes-21 domains (n=288) | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n=50 | n=288 | Sexual functioning | Energy e mobility | Diabetes control and social burden | Anxiety and worry | ||||||||||||||
| Total | Yes | No | Yes | No | Yes | No | Yes | No | |||||||||||
| N | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | |
| Sex | |||||||||||||||||||
| Female | 34 | 189 | 65.6 | 133 | 73.1 | 56 | 52.8 | 93 | 59.2 | 96 | 73.3 | 100 | 64.1 | 89 | 67.4 | 87 | 60.0 | 102 | 71.3 |
| Male | 16 | 99 | 34.4 | 49 | 26.9 | 50 | 47.2 | 64 | 40.8 | 35 | 26.7 | 56 | 35.9 | 43 | 32.6 | 58 | 40.0 | 41 | 28.7 |
| Age group (years)a | |||||||||||||||||||
| 22-54 | 8 | 81 | 28.1 | 50 | 27.5 | 31 | 29.3 | 39 | 24.8 | 42 | 32.1 | 37 | 23.7 | 44 | 33.4 | 29 | 20.0 | 52 | 36.3 |
| 55-61 | 14 | 62 | 21.5 | 39 | 21.4 | 23 | 21.7 | 35 | 22.3 | 27 | 20.6 | 30 | 19.2 | 32 | 24.2 | 28 | 19.3 | 34 | 23.8 |
| 62-68 | 11 | 78 | 27.1 | 43 | 23.6 | 35 | 33.0 | 45 | 28.7 | 33 | 25.2 | 46 | 29.5 | 32 | 24.2 | 45 | 31.0 | 33 | 23.1 |
| ≥69 | 11 | 67 | 23.3 | 50 | 27.5 | 17 | 16.0 | 38 | 24.2 | 29 | 22.1 | 43 | 27.6 | 24 | 18.2 | 43 | 29.7 | 24 | 16.8 |
| Schooling (years)a | |||||||||||||||||||
| 0 | 2 | 17 | 6.0 | 12 | 6.7 | 5 | 4.7 | 8 | 5.3 | 9 | 7.0 | 8 | 5.1 | 9 | 6.8 | 8 | 5.5 | 9 | 6.2 |
| 1-4 | 11 | 65 | 22.6 | 37 | 20.3 | 28 | 26.7 | 28 | 17.9 | 37 | 28.2 | 34 | 21.9 | 31 | 23.5 | 30 | 20.8 | 35 | 24.5 |
| 5-8 | 11 | 89 | 31.0 | 59 | 32.4 | 30 | 28.6 | 52 | 33.3 | 37 | 28.2 | 48 | 31.0 | 41 | 31.1 | 43 | 29.9 | 46 | 32.2 |
| 9-11 | 10 | 49 | 17.1 | 31 | 17.0 | 18 | 17.1 | 28 | 17.9 | 21 | 16.0 | 28 | 18.1 | 21 | 15.9 | 25 | 17.4 | 24 | 16.8 |
| ≥12 | 8 | 67 | 23.3 | 43 | 23.6 | 24 | 22.9 | 40 | 25.6 | 27 | 20.6 | 37 | 23.9 | 30 | 22.7 | 38 | 26.4 | 29 | 20.3 |
| Marital status | |||||||||||||||||||
| Married/stable union | 33 | 174 | 60.4 | 103 | 56.5 | 71 | 67.0 | 96 | 61.1 | 78 | 59.5 | 88 | 56.4 | 86 | 65.2 | 85 | 58.6 | 89 | 62.2 |
| Single/widowed/divorced/separated | 17 | 114 | 39.6 | 79 | 43.5 | 35 | 33.0 | 61 | 38.9 | 53 | 40.5 | 68 | 43.6 | 46 | 34.8 | 60 | 41.4 | 54 | 37.8 |
| Race/skin color | |||||||||||||||||||
| White | 22 | 89 | 30.9 | 58 | 31.9 | 31 | 29.2 | 47 | 29.9 | 42 | 32.1 | 46 | 29.5 | 43 | 32.5 | 46 | 31.7 | 43 | 30.0 |
| Asian | 4 | 14 | 4.9 | 7 | 3.8 | 7 | 6.6 | 5 | 3.2 | 9 | 6.9 | 5 | 3.2 | 9 | 6.8 | 5 | 3.4 | 9 | 6.3 |
| Black | 4 | 36 | 12.5 | 25 | 13.7 | 11 | 10.4 | 20 | 12.7 | 16 | 12.2 | 16 | 10.3 | 20 | 15.2 | 14 | 9.7 | 22 | 15.4 |
| Brown | 20 | 134 | 46.5 | 82 | 45.1 | 52 | 49.1 | 75 | 47.8 | 59 | 45.0 | 79 | 50.6 | 55 | 41.7 | 72 | 49.7 | 62 | 43.4 |
| Indigenous | - | 3 | 1.0 | 2 | 1.1 | 1 | 0.9 | 3 | 1.9 | - | 0.0 | 3 | 1.9 | - | 0.0 | 2 | 1.4 | 1 | 0.7 |
| No information provided | - | 12 | 4.2 | 8 | 4.4 | 4 | 3.8 | 7 | 4.5 | 5 | 3.8 | 7 | 4.5 | 5 | 3.8 | 6 | 4.1 | 6 | 4.2 |
| Household incomea | |||||||||||||||||||
| Up to BRL 998.00 | 8 | 81 | 30.2 | 54 | 31.8 | 27 | 27.6 | 38 | 26.2 | 43 | 35.0 | 38 | 26.2 | 43 | 35.0 | 34 | 25.6 | 47 | 34.8 |
| Over BRL 998.00 | 42 | 187 | 69.8 | 116 | 68.2 | 71 | 72.4 | 107 | 73.8 | 80 | 65.0 | 107 | 73.8 | 80 | 65.0 | 99 | 74.4 | 88 | 65.2 |
| Spending on medicines | |||||||||||||||||||
| Yes | - | 147 | 51.0 | 89 | 48.9 | 52 | 49.1 | 79 | 50.3 | 62 | 47.3 | 78 | 50.0 | 63 | 47.7 | 74 | 51.0 | 67 | 46.9 |
| No | - | 141 | 49.0 | 93 | 51.1 | 54 | 50.9 | 78 | 49.7 | 69 | 52.7 | 78 | 50.0 | 69 | 52.3 | 71 | 49.0 | 76 | 53.1 |
a) The number of respondents is lower than the number of participants, due to refusal to answer this variable.
The internal consistency of Diabetes-21 was high (α=0.91). Furthermore, the removal of any of the items did not alter the internal consistency of its construct (all items presented α=0.91). The agreement of the 21 items of the instrument was adequate (Kappa ≥0.60) (Table 2). Stability was good (intraclass correlation coefficient=0.91).
Table 2 Domain agreement, according to the removal of each item of Diabetes-21 (n=50), among people with diabetes mellitus assisted by the Family Health Strategy, Montes Claros, state of Minas Gerais, Brazil, 2019
| Item and domains | Weighted Kappa | p-valuea |
|---|---|---|
| Energy and mobility | ||
| 1. By feeling of weakness | 0.67 | <0.001 |
| 2. By how far you can walk | 0.60 | <0.001 |
| 3. By any daily exercise requirements | 0.85 | <0.001 |
| 4. By not being able to do housework or other jobs around the house | 0.93 | <0.001 |
| 5. By needing to rest often | 0.83 | <0.001 |
| 6. By having trouble caring for yourself (dressing, bathing or using the toilet) | 0.76 | <0.001 |
| 7. By walking more slowly than others | 0.92 | <0.001 |
| Diabetes control and social burden | ||
| 8. By food restrictions required to control your diabetes | 0.82 | <0.001 |
| 9. By losing control of your blood sugar levels | 0.76 | <0.001 |
| 10. By testing your blood sugar levels | 0.77 | <0.001 |
| 11. By getting your diabetes well controlled | 0.82 | <0.001 |
| 12. By the need to eat at regular intervals | 0.83 | <0.001 |
| 13. By the restrictions your diabetes places on your family and friends | 0.84 | <0.001 |
| 14. By being embarrassed because you have diabetes | 0.73 | <0.001 |
| 15. By doing things your family and friends do not do | 0.87 | <0.001 |
| Sexual functioning | ||
| 16. By diabetes interfering with your sex life | 0.61 | <0.001 |
| 17. By problems with sexual functioning | 0.90 | <0.001 |
| 18. By a decreased interest in sex | 0.87 | <0.001 |
| Anxiety and worry | ||
| 19. By worries about money matters | 0.82 | <0.001 |
| 20. By stress or pressure in your life | 0.90 | <0.001 |
| 21. By feeling depressed or low | 0.90 | <0.001 |
a) Z-test, Weighted Kappa.
The factorial structure of the final version of Diabetes-21 showed differences regarding the original structure. Questions 1, 3, 4, 6, 7, 12, 13, 14, 16, 18, 25, 27, 31, 33, 35, 37, 38 and 39 from Diabetes-39 instrument were removed, because they showed commonality lower than 0.5. Thus, it was reduced, from 39 to 21 items, with a decrease in the number of domains from 5 to 4, observed in exploratory factor analysis (energy and mobility; diabetes control and social burden; sexual functioning; anxiety and concern), due to the union of the dimensions ‘diabetes control’ and ‘social burden’. The union of these two dimensions resulted in better internal consistency and stability of the instrument. All dimensions presented good internal consistency (α≥0.70). Factor loadings ranged from 0.41 (item 15) to 0.90 (item 17); the dimension ‘sexual functioning’ presented the highest factor loading (values >0.75) (Table 3).
Table 3 Commonalities, factor loadings of each item by extracted factor and Cronbach’s alpha (α) by Diabetes-21 factor (n=288),a among people with diabetes mellitus assisted by the Family Health Strategy, Montes Claros, state of Minas Gerais, Brazil, 2019
| Diabetes-21 - Item and domains | Commonalities | Factor 1 | Factor 2 | Factor 3 | Factor 4 | Cronbach’s alpha |
|---|---|---|---|---|---|---|
| Factor: energy and mobility | ||||||
| 1. By feeling of weakness | 0.47 | 0.49 | 0.20 | 0.16 | 0.41 | 0.83 |
| 2. By how far you can walk | 0.62 | 0.72 | 0.26 | 0.03 | 0.19 | |
| 3. By any daily exercise requirements | 0.46 | 0.59 | 0.34 | -0.01 | 0.01 | |
| 4. By not being able to do housework or other jobs around the house | 0.61 | 0.74 | 0.07 | 0.21 | 0.10 | |
| 5. By needing to rest often | 0.57 | 0.70 | 0.18 | 0.17 | 0.17 | |
| 6. By having trouble caring for yourself (dressing, bathing or using the toilet) | 0.43 | 0.61 | 0.05 | 0.20 | 0.11 | |
| 7. By walking more slowly than others | 0.61 | 0.67 | 0.298 | 0.12 | 0.25 | |
| Factor: diabetes control and social burden | ||||||
| 8. By food restrictions required to control your diabetes | 0.55 | 0.06 | 0.73 | -0.07 | 0.11 | 0.86 |
| 9. By losing control of your blood sugar levels | 0.46 | 0.28 | 0.54 | 0.22 | 0.20 | |
| 10. By testing your blood sugar levels | 0.60 | 0.24 | 0.71 | 0.06 | 0.17 | |
| 11. By getting your diabetes well controlled | 0.63 | 0.17 | 0.73 | 0.23 | 0.13 | |
| 12. By the need to eat at regular intervals | 0.58 | 0.28 | 0.66 | 0.23 | 0.13 | |
| 13. By the restrictions your diabetes places on your family and friends | 0.62 | 0.33 | 0.64 | 0.23 | 0.22 | |
| 14. By being embarrassed because you have diabetes | 0.49 | 0.14 | 0.47 | 0.29 | 0.40 | |
| 15. By doing things your family and friends do not do | 0.54 | 0.57 | 0.41 | 0.10 | 0.19 | |
| Factor: sexual functioning | ||||||
| 16. By diabetes interfering with your sex life | 0.79 | 0.16 | 0.14 | 0.85 | 0.10 | 0.86 |
| 17. By problems with sexual functioning | 0.84 | 0.09 | 0.14 | 0.90 | 0.07 | |
| 18. By a decreased interest in sex | 0.71 | 0.29 | 0.20 | 0.76 | 0.11 | |
| Factor: anxiety and worry | ||||||
| 19. By worries about money matters | 0.56 | 0.15 | 0.16 | 0.07 | 0.71 | 0.70 |
| 20. By stress or pressure in your life | 0.77 | 0.16 | 0.19 | -0.00 | 0.84 | |
| 21. By feeling depressed or low | 0.55 | 0.32 | 0.22 | 0.23 | 0.59 | |
a) Analysis performed from factor extraction using the principal component method, followed by a orthogonal rotation (varimax).
The eigenvalues found in each factor were: 1.48 (energy and mobility, factor 1); 1.18 (diabetes control and social load, factor 2); 8.00 (sexual functioning, factor 3); and 1.77 (anxiety and worry, factor 4). The variance explained by each factor was 7.1% (factor 1), 5.6% (factor 2), 38.1% (factor 3) and 8.5% (factor 4).
The results of the Kaiser-Meyer-Olkin test (0.91) and Bartlett’s test of sphericity (2,579.51) of Diabetes-21 were satisfactory and adequate (p<0.001). Their structure was explained by four latent factors, indicated by the graphical evaluation of the scree plot (inflection point of the curve). The factors explained 59.3% of the total variance. The final version of Diabetes-21 is presented as a supplementary material (Supplementary Material 1).
Confirmatory factor analysis showed indices adequate to the tested model (ratio between chi-square and degrees of freedom, 2.22; fit quality index, 0.88; the root mean square error of approximation, 0.06; comparative fit index, 0.91; Tucker-Lewis index, 0.90). Factor loadings ranged from 0.51 (Q34) to 0.89 (Q23). Figure 2 systematizes confirmatory factor analysis of Diabetes-21.
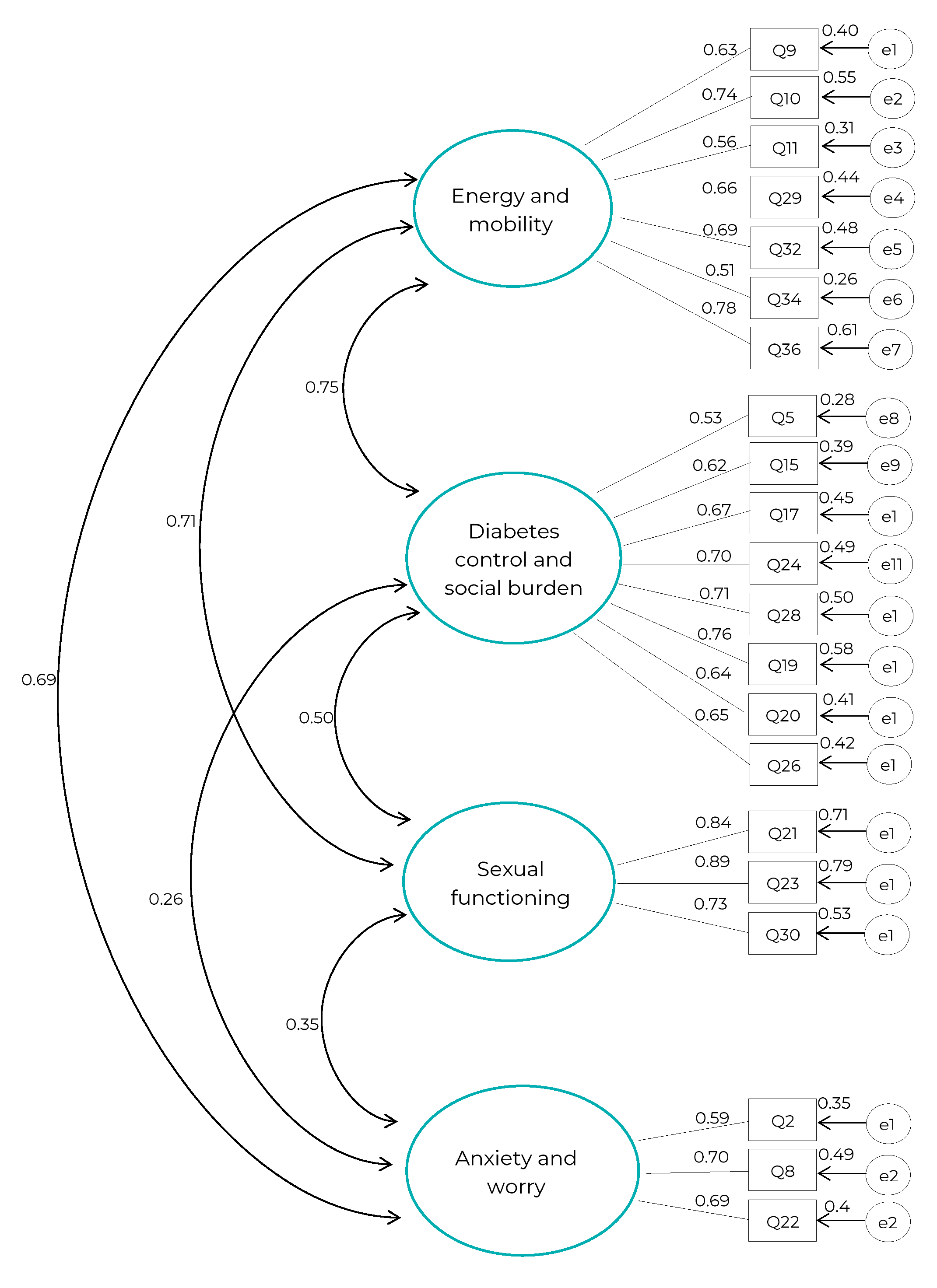
Figure 2 Confirmatory factor analysis of Diabetes-21 (n=288) among people with diabetes mellitus assisted by the Family Health Strategy, Montes Claros, state of Minas Gerais, Brazil, 2019
There was a negative correlation with age (Spearman’s correlation coefficient = -0.14; p=0.021) and positive correlation with schooling (Spearman’s correlation coefficient = 0.76; p=0.001). Spearman’s correlation coefficient value between the total score of Diabetes-39 and Diabetes-21 was strong (0.97; p<0.001). It could be seen a mean correlation between the total score of the WHOQOL-BREF and the Diabetes-21 (0.51; p<0.001).
The mean values found in the Diabetes-21 domains were: energy and mobility (37.85; SD=16.71; 95%CI 35.91;39.78); diabetes control and social burden (34.22; SD=14.93; 95%CI 32.4 9;35.96); sexual functioning (33.77; SD=19.80; 95%CI 31.47;36.06); anxiety and worry (40.03; SD=16.60; 95%CI 38.10;41.95).
Poor health-related quality of life was more frequent in the domain ‘sexual functioning’ (63.2%), followed by the domains ‘energy and mobility’ (54.5%; n=157), ‘diabetes control and social burden’ (54.2%; n=156) and ‘anxiety and worry’ (50.3%; n=145).
Discussion
Diabetes-21 instrument was considered to be valid, reliable and interpretable by the users of primary health care in Montes Claros, state of Minas Gerais. Regarding exploratory factor analysis, it could be seen an association between the items present in the domains ‘social burden’ and ‘diabetes control’, and the union of these domains was performed. The confirmatory factor analysis showed satisfactory adjustment for the acceptance of the proposed theoretical model. With regard to the concurrent validity of Diabetes-21, it could be seen that the highest level of quality of life was positively correlated with schooling; and negatively with age. Estimates of reliability, in general and within each domain, showed satisfactory reliability, both in stability and internal consistency. Diabetes-21 instrument was able to discriminate levels of quality of life among participants, showing good reliability and validity.
Some limitations of the study should be taken into consideration. Convenience sampling was used to verify reliability and concurrent validity; this type of sampling presents limitations regarding the results and conclusions, given that they cannot be generalized to the entire population, due to the selection bias. However, the results of this sample show a variability related to the variables investigated, suggesting that it may represent the general population. Criterion validity includes estimates of concurrent and predictive validity, although predictive validity could not be estimated due to the absence of a gold standard.9 Thus, the concurrent validity was estimated by the correlation between the scores obtained from Diabetes-21 related to the age and schooling of the participants. Responsiveness was not estimated because this is a cross-sectional study that was not designed to detect changes over time.
No structural validation studies on Diabetes-39 with reduction of items or domains were found. In this study, the reduction was based on the need to review the instruments before applying them in specific samples, because both intrinsic and extrinsic factors to the disease may change over time. The results found in this research corroborate those of previous studies, because when comparing Diabetes-39 with other instruments, it was considered to be adequate, as it had been previously used in the investigation of quality of life among people with diabetes.23-25
Regarding Diabetes-21, it could be seen that poor quality of life was more frequent in the domain ‘sexual functioning’. Several factors are related to sexual dysfunction among people with diabetes. Vascular anomalies, endocrine disorders, emotional impact and medications used for the treatment can cause ejaculation problems, erectile dysfunction and arousal disorder, and thus, decreased desire.26,27 As such, sexual functioning should be taken into consideration in the treatment of diabetes, in the same way as any emotional aspects that can impact people’s quality of life.23
The mean value showed in the domain ‘diabetes control and social burden’ is similar to that found in a study that evaluated the psychometric properties of Diabetes-39 among people with diabetes in Jordan (32,7).22 People with diabetes undergo lifestyle changes, given the need to follow treatment, and this behavior change can result in reduction in leisure activities and the time spend with family and friends.28 Therefore, it is believed that people with diabetes are more likely to develop diseases such as anxiety and depression, due to the social impact that this disease causes.29
The assessment of concurrent validity suggests that schooling has a positive impact on the quality of life of people with diabetes. This result corroborates those of a study conducted in the city of Ourense, Spain, in 2015, when it was suggested that schooling and the understanding of health condition can enable the adoption of healthy habits in the daily lives of people with diabetes, contributing to the improvement of quality of life.30
The assessment of Diabetes-21 reliability, as well as the original instrument, Diabetes-39, showed satisfactory internal consistency.3,22 The levels of assessment of Diabetes-21 enabled the interpretation of ‘quality of life construct among people with diabetes’. The same study conducted in Jordan, among 368 people with diabetes,22 assessed quality of life using the Diabetes-39 instrument and also a similar form of interpretation of the instrument adopted in this study, in which the values were transformed to a 0 to 100 scale.
The reduction of the instrument’s items may generate loss of comparability, given that most existing studies have used Diabetes-39. As such, more psychometric studies using Diabetes-21 should be carried out in order to better understand its structure and thus, consider it valid and reliable.
Diabetes-21 instrument proved to be promising for assessing health-related quality of life among people with diabetes, and can be a useful tool for researchers. In addition, it is as an effective instrument to be used by health professionals in the context of care for people with diabetes mellitus, because it is able to identify impairment in quality of life and enable the implementation of actions aimed at minimizing the impacts of the disease.
REFERENCES
1. Rodrigues AMAM, Cavalcanti AL, Pereira JLSH, Araújo CLC, Bernardino IM, Soares RL, et al. Use of the health services according to social determinants, health behaviors and quality of life among diabetics. Cien Saude Colet. 2020;25(3):845-58. doi: 10.1590/1413-81232020253.19532018 [ Links ]
2. Boyer JG, Earp JA. The development of an instrument for assessing the quality of life of people with diabetes. Diabetes-39. Med Care. 1997;35(5):440-53. doi: 10.1097/00005650-199705000-00003 [ Links ]
3. Queiroz FA, Pace AE, Santos CB. Cross-cultural adaptation and validation of the instrument Diabetes - 39 (D-39): brazilian version for type 2 diabetes mellitus patients - stage 1. Rev Lat Am Enfermagem. 2009;17(5):708-15. doi: 10.1590/S0104-11692009000500018 [ Links ]
4. Miyamoto ST, Paganotti MA, Serrano EV, Giovelli RA, Valim V. Assessment of fatigue and dryness in primary Sjögren's syndrome: Brazilian version of "Profile of Fatigue and Discomfort - Sicca Symptoms Inventory (short form) (PROFAD-SSI-SF)". Rev Bras Reumatol. 2015;55(2):113-22. doi: 10.1016/j.rbre.2014.10.002 [ Links ]
5. Roque H, Veloso A, Ferreira PL. Versão portuguesa do questionário EUROPEP: contributos para a validação psicométrica. Rev Saude Publica. 2016;50:61. doi: 10.1590/S1518-8787.2016050006259 [ Links ]
6. Valim MD, Marziale MHP, Hayashida M, Rocha FLR, Santos JLF. Validity and reliability of the Questionnaire for Compliance with Standard Precaution. Rev Saude Publica. 2015;49:87. doi: 10.1590/S0034-8910.2015049005975 [ Links ]
7. Marques SRL, Lemos SMA. Health literacy assessment instruments: literature review. Audiol Commun Res. 2017;22:e1757. doi: 10.1590/2317-6431-2016-1757 [ Links ]
8. Colucci MZO, Costa Alexandre NM, Milani D. Construction of measurement instruments in the area of health. Cien Saude Colet. 2015;20(3):925-36. doi: 10.1590/1413-81232015203.04332013 [ Links ]
9. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN study reached international consensus on taxonomy, terminology, and definitions of measurement properties for health-related patient-reported outcomes. J Clin Epidemiol. 2010;63(7):737-45. doi: 10.1016/j.jclinepi.2010.02.006 [ Links ]
10. Faria HTG, Veras VS, Xavier ATF, Teixeira CRS, Zanetti ML, Santos MA. Quality of life in patients with diabetes mellitus before and after their participation in an educational program. Rev Esc Enferm USP. 2013;47(2):348-54. doi: 10.1590/S0080-62342013000200011 [ Links ]
11. Instituto Brasileiro de Geografia e Estatística. Cidades e estados: Montes Claros [Internet]. Brasília: Instituto Brasileiro de Geografia e Estatística; [data desconhecida] [citado 2021 jan 15]. Disponível em: https://www.ibge.gov.br/cidades-e-estados/mg/montes-claros.html [ Links ]
12. Bertolucci PHF, Brucki SMD, Campacci SR, Juliano Y. O mini-exame do estado mental em uma população geral: impacto da escolaridade. Arq Neuro-Psiquiatr. 1994;52(1):1-7. doi: 10.1590/S0004-282X1994000100001 [ Links ]
13. Hair Júnior JF, Black WC, Babin B, Anderson RE, Tatham RL. Análise multivariada de dados. 6. ed. Porto Alegre: Bookman; 2009. [ Links ]
14. Luiz RR, Magnanini MMF. A lógica da determinação do tamanho da amostra em investigações epidemiológicas. Cad. Saúde Coletiva. 2000;8(2):9-28. [ Links ]
15. The World Health Organization. Quality of Life Assessment (WHOQOL): position paper from the World Health Organization. Soc Sci Med. 1995;41(10):1403-9. doi: 10.1016/0277-9536(95)00112-k [ Links ]
16. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159-174. [ Links ]
17. Artes R. Aspectos estatísticos da análise fatorial de escalas de avaliação. Rev Psiquiatr Clin. 1998;25(5):223-8. [ Links ]
18. Reis E. Estatística multivariada aplicada. Lisboa: Edições Silabo; 1997. [ Links ]
19. Maroco JP. Análise de equações estruturais: fundamentos teóricos, software & aplicações. 2. ed. Pêro Pinheiro: ReportNumber; 2014. [ Links ]
20. Sousa LMM, Marques-Vieira CMA, Carvalho MLR, Veludo F, José HMG. Fidelidade e validade na construção e adequação de instrumentos de medida. Enformação. 2015;5:25-32. [ Links ]
21. Harper A, Power M. Steps for checking and cleaning data and computing domain scores for the WHOQOL-bref [Internet]. Geneva: World Health Organization; 1996 [cited 2021 jan. 19]. Available from: https://www.who.int/mental_health/media/en/76.pdf [ Links ]
22. Khader YS, Bataineh S, Batayha W. The Arabic version of Diabetes-39: psychometric properties and validation. Chronic Illn. 2008;4(4):257-63. doi: 10.1177/1742395308100647 [ Links ]
23. Zulian LR, Santos MA, Veras VS, Rodrigues FFL, Arrelias CCA, Zanetti ML. Quality of life in patients with diabetes using the diabetes 39 (D-39) instrument. Rev Gaucha Enferm. 2013;34(3):138-146. doi: 10.1590/S1983-14472013000300018 [ Links ]
24. Lamu AN, Chen G, Gamst-Klaussen T, Olsen JA. Do country-specific preference weights matter in the choice of mapping algorithms? The case of mapping the Diabetes-39 onto eight country-specific EQ-5D-5L value sets. Qual Life Res. 2018;27(7):1801-14. doi: 10.1007/s11136-018-1840-5 [ Links ]
25. Mahgoub AO, Abdelgadir E. The association between health-related quality of life and Ramadan fasting in diabetic patients: a survey using a structured D-39 assessment tool. a Sudanese cohort. J Fasting Health. 2017;5(1):24-30. doi: 10.22038/jfh.2017.21682.1080 [ Links ]
26. Rutherford D, Collier A. Sexual dysfunction in women with diabetes mellitus. Gynecol Endocrinol. 2005;21(4):189-92. doi: 10.1080/09513590400021110 [ Links ]
26. Enzlin P, Mathieu C, van Der Bruel A, Vanderschueren D, Demyttenaere K. Prevalence and predictors of sexual dysfunction in patients with type 1 diabetes. Diabetes Care. 2003;26(2):409-14. doi: 10.2337/diacare.26.2.409 [ Links ]
28. Weinger K, Lee J. Psychosocial and psychiatric challenges of diabetes mellitus. Nurs Clin North Am. 2006;41(4):667-80. doi: 10.1016/j.cnur.2006.07.002 [ Links ]
29. Antúnez M, Bettiol AA. Depression in patients with type 2 diabetes who attend an outpatient clinic of internal medicine. Acta Med Colomb. 2016;41(2):102-110. [ Links ]
30. Fernández-Silva MJ, Alonso-González A, González-Pérez E, Gestal-Otero JJ, Díaz-Grávalos GJ. Health literacy in patients with type 2 diabetes: a cross-sectional study using the HLS-EU-Q47 questionnaire. Semergen. 2019;45(1):30-6. doi: 10.1016/j.semerg.2018.08.003. [ Links ]
Financing The research received financial support from the Fundação de Amparo à Pesquisa do Estado Minas Gerais (FAPEMIG: Process No. BIP-00384-16) and the Conselho Nacional de Desenvolvimento Científico e Tecnológico/ Ministry of Science, Technology and Innovation (CNPq/MCTI: Process No. 456224/2014-9). Andréa Maria Eleutério de Barros Lima Martins receives a productivity scholarship from CNPq (Process No. 302473/2018-1).
Associated academic workArticle derived from the Doctoral thesis entitled ‘Development and evaluation of instruments related to health literacy and quality of life among people with diabetes mellitus’, submitted by Árlen Almeida Duarte de Sousa to the Postgraduate Program in Health Sciences of the Universidade Estadual de Montes Claros (Unimontes) on May 28, 2019.
Supplementary Material 1
Final version of Diabetes-21
| Diabetes-21 | |||||
|---|---|---|---|---|---|
| People’s quality of life is affected by many things. These things might include health, leisure and vacation opportunities, friends and family, and a job. This questionnaire is designed to help us understand what affects the quality of life of people with diabetes. Below, there are some questions about your quality of life. For each sentence, put a check in the box to show how much that factor affects your quality of life, according to the legend: (1) not affected (2) little affected (3) sometimes affected (4) very affected (5) extremely affected | |||||
| During the past month, how much was the quality of your life affected by: | 1 | 2 | 3 | 4 | 5 |
| 1. feelings of weakness | |||||
| 2. how far you can walk | |||||
| 3. Any daily exercise requirements | |||||
| 4. not being able to do housework or other jobs around the house | |||||
| 5. needing to rest often | |||||
| 6. having trouble caring for yourself (dressing, bathing or using the toilet) | |||||
| 7. walking more slowly than others | |||||
| 8. food restrictions required to control your diabetes | |||||
| 9. losing control of your blood sugar levels | |||||
| 10. having to test your blood sugar levels | |||||
| 11. getting your diabetes well controlled | |||||
| 12. the need to eat at regular intervals | |||||
| 13. the restrictions your diabetes places on your family and friends | |||||
| 14. being embarrassed because you have diabetes | |||||
| 15. doing things that your family and friends don’t do | |||||
| 16. diabetes interfering with your sex life | |||||
| 17. problems with sexual functioning | |||||
| 18. a decreased interest in sex | |||||
| 19. worries about money matters | |||||
| 20. stress or pressure in your life | |||||
| 21. feeling depressed or low | |||||
| Overall assessment | |||||
| How satisfied are you with your overall quality of life? | |||||
| (1) not satisfied at all (2) dissatisfied (3) neither satisfied nor dissatisfied (4) satisfied (5) very satisfied | |||||
| How serious do you think your diabetes is? | |||||
| (1) not serious (2) serious (3) more or less serious (4) very serious (5) extremely serious | |||||
Received: April 22, 2021; Accepted: October 14, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
