










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.31 no.1 Brasília 2022 Epub 29-Mar-2022
http://dx.doi.org/10.1590/s1679-49742022000100016
Original Article
Prevalence and factors associated with the use of sleep-inducing medication among women receiving Primary Health Care: a cross-sectional study in Vitória, Espírito Santo, Brazil, 2014
1Universidade Federal do Espírito Santo, Departamento de Enfermagem, Vitória, ES, Brazil
2Universidade Federal do Espírito Santo, Programa de Pós-Graduação em Saúde Coletiva, Vitória, ES, Brazil
3Universidade Federal de São Paulo, Escola Paulista de Enfermagem, São Paulo, SP, Brazil
Objective
To verify prevalence and factors associated with the use of sleep-inducing medication among women receiving primary health care (PHC) in Vitória, ES, Brazil.
Methods
This was a cross-sectional study conducted in 2014 with women aged 20-59. We analyzed association of sleep-inducing medication use with socioeconomic factors and experiences of violence (Poisson regression).
Results
Out of 991 participants, 18.5% were using sleep-inducing medication and 45.9% had used it at some point in their lives. Current and lifetime use of these medications was associated with age, years of education, as well as psychological, physical and sexual violence in the last year (p-value<0.05). Lower family income (PR=1.30; 95%CI 1.03;1.64) and controlling partner (PR=1.35; 95%CI 1.08;1.69) were associated with current use, while experience of sexual violence in childhood (PR=1.33; 95%CI 1.13;1.56) was associated with lifetime use.
Conclusion
Use of sleep-inducing medication was frequent among PHC service users, and was associated with socioeconomic factors and experiences of violence.
Keywords: Sleep Aids, Pharmaceutical; Sleep; Mental Health; Violence Against Women; Socioeconomic Factors; Observational Study
Study contribution
Main results
Use of sleep-inducing medication was associated with socioeconomic factors and experience of violence. Women who had experienced three types of violence in the past 12 months were twice as likely to use these medications.
Introduction
Sleep-related complaints are quite frequent in health care.1 Work overload, daily contact with technology and sociocultural trends can negatively interfere with sleep quality and patterns.2 In addition, with regard to sleep quality, there are differences between the sexes, with a higher frequency of sleeping difficulties and sleep disorders in females.3
A meta-analysis study, investigating differences between the sexes regarding occurrence of insomnia, found a 41.0% higher predisposition to insomnia among women when compared to men.4 In Spain, among 2,144 individuals observed, women were found to be three times more likely to use sleep-inducing medication.5 In Brazil, a study with 743 male and female adults conducted in a city in the interior region of the state of São Paulo in 2012, found a prevalence rate of 46.7% for sleep disorders among the participants, and they were more frequent in women (52.1%).6 Data from the 2013 National Health Survey showed that one in every 13 Brazilians used sleep-inducing medication, and this behavior was 2.2 times more prevalent in women: prevalence ratio (PR) = 2.21; 95% confidence interval (95%CI) = 1.97; 2.47.7
Poor sleep quality impacts quality of life, affects cognitive performance, memory, concentration and, furthermore, impairs the social, family and work context.8 Among women, use of sleep-inducing medication is related to advancing age, presence of chronic disease,9 physiological and hormonal changes,10 social and family problems,11 low schooling levels and low income.12 Sociodemographic status is seen as one of the main reasons for using these drugs.11
It is worth noting that some women use sleep inducers to relieve unpleasant feelings and emotions,13 which include issues such as physical and emotional exhaustion, insomnia, depression, anxiety, nervousness and fear.13 In this scenario, we highlight the experience of intimate partner violence, a phenomenon that causes moral harm or damage to property and physical, sexual or psychological suffering to women, and may or may not lead to death.14
Various studies demonstrate the detrimental effects of intimate partner violence on sleep quality.15,16 In Florianópolis, capital of the state of Santa Catarina, the dynamics of domestic violence were analyzed based on the discourse of battered women and their partners, about episodes of domestic violence recorded in the period from October 2006 to January 2007; the result showed that 56.7% of women used medication because of experiencing violence, and the amounts and frequency with which they used medication were not necessarily subject to medical supervision.17
The increase in the use of these medications among women is a public health problem and requires health workers to pay greater attention when providing care to these women.13
The objective of this study was to verify prevalence and factors associated with the use of sleep-inducing medication among women receiving primary health care (PHC) in Vitória, capital of the state of Espírito Santo, Brazil, between March and September 2014.
Methods
Design
This was a cross-sectional study conducted with women aged 20-59 receiving care in all 26 of Vitória’s primary health care centers between March and August 2014.
Background
Vitória has 327,801 inhabitants and is the state’s fourth most populous municipality with a population density of 3,338 inhab./km2. Vitória’s municipal human development index (HDI-M) is 0.845 and some 98% of its households have basic sanitation.18 The municipality has the largest number of health care facilities in Espírito Santo and has 93.3% primary health care coverage.19
The study scenario was comprised of the municipality’s 26 primary health care centers belonging either to the Family Health Strategy or the Community Health Agent Program.
Sample size
We used OpenEpi version 3 to calculate the sample size, considering a 5% margin of error, a 95% confidence level, 80% power and an exposed/unexposed ratio of 1. We added 10% to the result of this calculation to account for possible losses, plus 30% for adjusted analyses, totaling a sample of 998 women.
Participants
The distribution of participants to be interviewed at the primary health care centers was defined by sampling proportional to the number of health service users aged 20 to 59 years old registered with each health center. The women were randomly selected. Eligible participants were women who used the services of the Brazilian National Health System (SUS) aged 20 to 59 years old who were on primary health care center waiting lists and who had or had had an intimate partner in the 12 months prior to data collection.
After ‘agreement’ and signing of the Free and Informed Consent form, the interviews used to collect data were carried out in a closed room where there were only the interviewee and the interviewer. At the end of the interview, all participants received a folder containing educational and informative material and addresses of the main services for women in situations of violence.
Study variables
The study outcomes were ‘current use of sleep-inducing medication’ (yes; no) and ‘lifetime use of sleep-inducing medication’ (yes; no).
In order to analyze associated factors, the following independent variables were included:
a) Socioeconomic characteristics
age group (in completed years: 20-39; 40-59);
race/skin color (white; black; yellow; brown; indigenous);
schooling (in years of study: less than 5; 5-8; 9-11; 12 or more);
marital status (does not have a partner; has a partner); and
family income (in BRL: up to BRL 1,500; above BRL 1,500).
b) Experience of violence
Data source and measurements
The data were collected with the help of a standardized and structured printed questionnaire, administered by the interviewers to obtain data on the participants’ socioeconomic characteristics, experience of violence and use of sleep-inducing medication.
The two study outcomes, current use and lifetime use of sleep-inducing medication, were established by asking the following questions: have you taken sleeping pills at any time during your life? and are you currently taking sleeping pills?, with the option of replying (yes or no).
In order to itemize experience of violence against women perpetrated by intimate partners, we administered a World Health Organization (WHO) questionnaire validated in Brazil: World Health Organization Violence Against Women.20 This instrument contains questions about types of violence (psychological, physical and/or sexual) suffered in the last 12 months, classified as follows: no type of violence; one type of violence; two types of violence; three types of violence. In turn, the ‘controlling partner’ independent variable, also defined in accordance with the WHO, considered as behaviors intended to isolate the person from family and friends, control places and access to places and information.20
Bias control
The field team (interviewers and supervisors, all female) was trained to ensure interview standardization and best instrument administration. In the period prior to the collection, a pilot study was conducted in which 50 interviews were carried out with women using the eligible primary health care centers to observe the interviewers’ posture and administration of the questionnaires. Those interviews were not included in this research. Daily, during data collection, supervisors monitored the interviews and performed quality control.
Statistical analyses
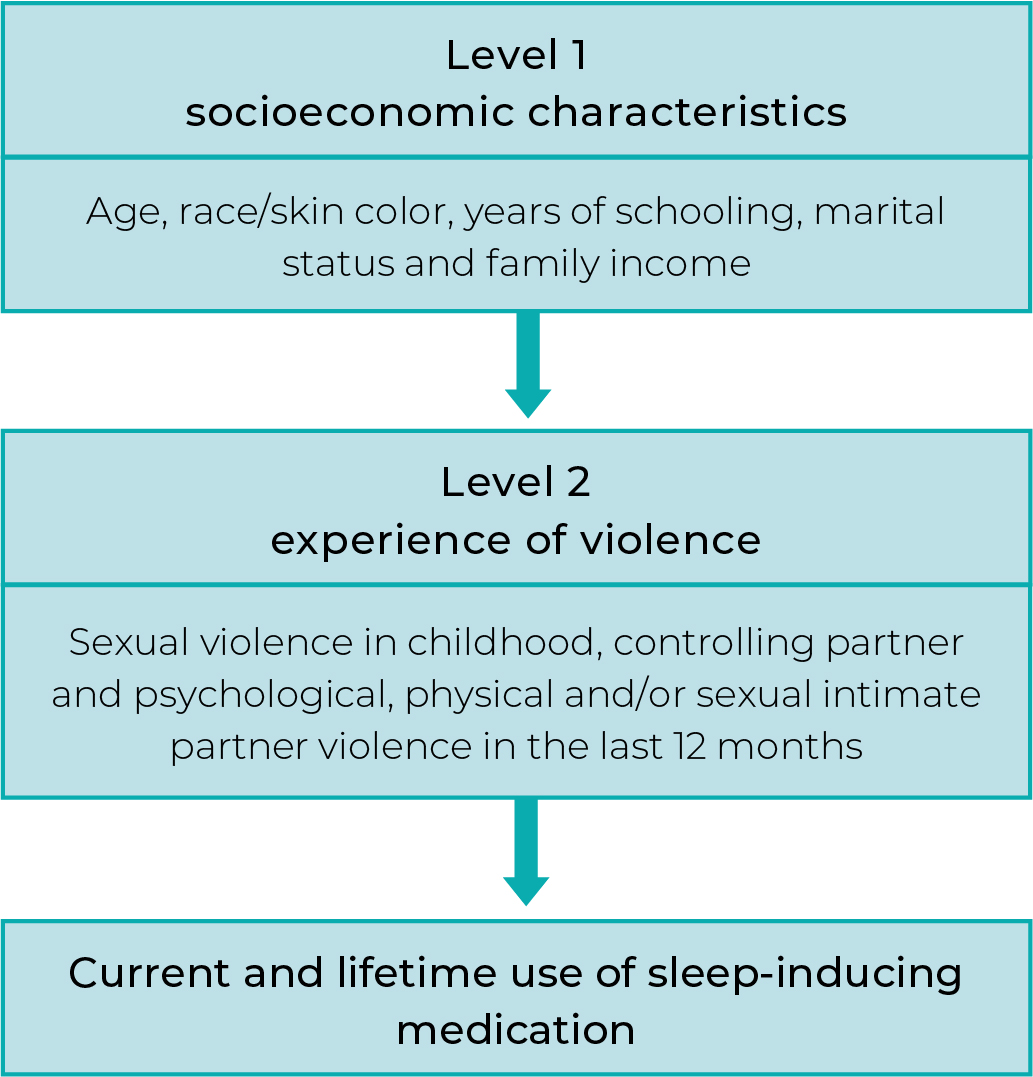
Analyses were performed using the Stata 13.0 statistical package. Descriptive data were presented as absolute and relative frequencies and 95%CIs. Pearson’s chi-square test or linear trend chi-square test was performed for bivariate analysis. Poisson regression was used for analysis of association, calculating crude and adjusted prevalence ratios (PR) and respective 95%CIs as a measure of effect. The adjusted analysis followed a hierarchical model, in which socioeconomic variables were considered as distal variables, and experiences of violence as proximal variables (Figure 1). We adopted a p-value<0.20 for inclusion in the model in the crude analysis, and a p-value<0.05 for keeping the variables in the model.
Results
Seven of the 998 women invited to take part in this study refused. The final study sample totaled 991 women, 18.5% (183) of whom were using sleep-inducing medication and 45.9% (455) had used this class of medication at some time in their lives.
Table 1 shows the characteristics of the participants. The majority were in the 40 to 59 age group (65.4%; n=648), were of brown race/skin color (50.8%; n=503), had 9-11 years of schooling (52.5%; n=521), had a partner (74.0%; n=733) and had family income above BRL 1,500 (65.4%; n=648).
Table 1 Prevalence of current and lifetime use of sleep-inducing medication among women receiving Primary Health Care (n=991), according to socioeconomic characteristics and experience of violence, Vitória, Espírito Santo, Brazil, March-August 2014
| Variables | n | % | Lifetime | Current use | ||
|---|---|---|---|---|---|---|
| % (95%CIa) | p-value | % (95%CIa) | p-value | |||
| Socioeconomic characteristics | ||||||
| Age group (in years) | <0.001 | <0.001 | ||||
| 20-39 | 343 | 34.6 | 39.0 (35.3;42.9) | 28.7 (23.3;34.7) | ||
| 40-59 | 648 | 65.4 | 57.6 (52.5;62.6) | 55.4 (46.8;60.2) | ||
| Race/skin color | 0.287 | 0.939 | ||||
| White | 215 | 21.7 | 51.6 (44.9;58.3) | 43.2 (34.3;52.6) | ||
| Black | 239 | 24.1 | 43.5 (37.3;49.9) | 38.5 (29.6;48.2) | ||
| Yellow | 23 | 2.3 | 34.8 (18.1;56.2) | 37.5 (11.5;73.6) | ||
| Brown | 503 | 50.8 | 45.3 (41.0;49.7) | 39.5 (33.3;46.0) | ||
| Indigenous | 11 | 1.1 | 36.4 (13.6;67.5) | 50.0 (9.4;0.6) | ||
| Schooling (in years of study) | 0.007 | <0.001 | ||||
| Less than 5 | 112 | 11.3 | 50.9 (41.7;60.0) | 64.9 (51.6;76.2) | ||
| 5-8 | 191 | 19.3 | 49.2 (42.1;56.3) | 43.6 (33.9;53.8) | ||
| 9-11 | 521 | 52.5 | 40.9 (36.7;45.2) | 32.4 (26.4;39.0) | ||
| 12 or more | 167 | 16.9 | 54.5 (46.9;61.9) | 39.6 (30.0;50.0) | ||
| Marital status | 0.342 | 0.785 | ||||
| Has a partner | 733 | 74.0 | 45.0 (41.4;48.6) | 40.6 (35.4;46.0) | ||
| Does not have a partner | 258 | 26.0 | 48.5 (42.3;54.5) | 39.2 (30.9;48.1) | ||
| Family income (in BRL) | 0.736 | 0.083 | ||||
| Up to BRL 1,500 | 343 | 34.6 | 46.6 (41.4;51.9) | 45.6 (38.0;53.4) | ||
| Above BRL 1,500 | 648 | 65.4 | 45.5 (41.7;49.4) | 37.3 (31.9;43.0) | ||
| Experience of violence | ||||||
| Controlling partner | 0.038 | 0.016 | ||||
| No | 486 | 51.8 | 42.6 (38.3;47.1) | 34.8 (28.6;41.6) | ||
| Yes | 452 | 48.2 | 49.3 (44.7;53.9) | 46.2 (39.7;52.7) | ||
| Sexual violence in childhood | 0.003 | 0.364 | ||||
| No | 870 | 87.8 | 44.1 (40.8;47.4) | 39.3 (34.5;44.3) | ||
| Yes | 121 | 12.2 | 58.7 (49.7;67.1) | 45.1 (33.9;56.8) | ||
| Types of intimate partner violencec | 0.013b | 0.004b | ||||
| No type of violence | 717 | 72.4 | 43.0 (39.4;46.6) | 37.3 (32.1;42.9) | ||
| One type of violence | 167 | 16.8 | 55.1 (47.5;62.5) | 40.2 (30.6;50.6) | ||
| Two types of violence | 83 | 8.4 | 50.6 (39.9;61.2) | 46.7 (32.9;62.7) | ||
| Three types of violence | 24 | 2.4 | 54.2 (34.2;72.9) | 84.6 (53.3;96.4) | ||
a) 95%CI: 95% confidence interval; b) Trend p-value; c) Psychological, physical and sexual intimate partner violence in the last 12 months.
It is noteworthy that 48.2% (452) of the women interviewed stated that their partners were controllers, while 12.2% (121) stated that they had suffered sexual violence in their childhood. Furthermore, 16.8% (167) of the women had experienced one type of violence in the last year, 8.4% (83) had been victims of two types, and 2.4% (24) had experienced all three types of violence (psychological, physical and sexual).
The bivariate analysis showed that the highest percentage of users who had used sleep-inducing medication in their lifetimes or were using this type of medication at the time of the interview was related to age, schooling, having a controlling partner, as well as experiencing intimate partner violence in the past 12 months. In addition, women with a history of sexual violence in their childhood had higher frequencies of lifetime use of sleep-inducing medication (p-value<0.05).
After adjustment for confounding variables, lifetime and current sleep-inducing medication use remained associated with age group, years of education and experiencing partner violence in the past 12 months, as presented in Table 2. Prevalence of lifetime sleep-inducing medication use in women aged 40-59 was 1.45 higher (95%CI 1.27;1.66) compared to prevalence of lifetime use among those aged 20-39. Current use of sleep-inducing medication was 1.82 time higher (95%CI 1.43;2.32) among older women (40-59 years old) compared to younger women (20-39 years old). Prevalence of lifetime use of sleep-inducing medication among women with higher levels of schooling (12 years or more of study) was 1.3 time higher (95%CI 1.03;1.64) when compared to those who had less than 5 years of study. With regard to current use of sleep-inducing medication, lower prevalence rates were found in the group with 5 to 11 years of schooling compared to the group with less schooling (p-value<0.05).
Table 2 Crude and adjusted analyses of association of socioeconomic characteristics and experience of violence with current and lifetime use of sleep-inducing medication among women receiving Primary Health Care (n=991), Vitória, Espírito Santo, Brazil, March-August 2014
| Variables | Lifetime | Current use | ||||||
|---|---|---|---|---|---|---|---|---|
| Crude | Adjusted | Crude | Adjusted | |||||
| RPa (95%CIb) | p-value | RPa (95%CIb) | p-value | RPa (95%CIb) | p-value | RPa (95%CIb) | p-value | |
| Socioeconomic characteristics | ||||||||
| Age group (in years) | <0.001 | <0.001 | <0.001 | <0.001 | ||||
| 20-39 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 40-59 | 1.48 (1.29;1.68) | 1.45 (1.27;1.66) | 1.87 (1.48;2.36) | 1.82 (1.43;2.32) | ||||
| Schooling (in years of study) | 0.006 | 0.011 | <0.001 | 0.007 | ||||
| Less than 5 | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 5-8 | 0.97 (0.77;1.21) | 1.05 (0.83;1.32) | 0.67 (0.50;0.91) | 0.73 (0.54;0.98) | ||||
| 9-11 | 0.80 (0.65;0.99) | 0.98 (0.79;1.22) | 0.50 (0.38;0.66) | 0.62 (0.46;0.82) | ||||
| 12 or more | 1.07 (0.85;1.35) | 1.30 (1.03;1.64) | 0.61 (0.44;0.84) | 0.83 (0.58;1.17) | ||||
| Family income (in BRL) | 0.647 | 0.079 | 0.029 | |||||
| Up to BRL 1,500 | 1.02 (0.94;1.11) | - | - | 1.22 (0.98;1.53) | 1.30 (1.03;1.64) | |||
| Above BRL 1,500 | 1.00 | - | 1.00 | 1.00 | ||||
| Experience of violence | ||||||||
| Controlling partner | 0.039 | 0.056 | 0.018 | 0.009 | ||||
| No | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Yes | 1.16 (1.01;1.33) | 1.14 (0.99;1.31) | 1.33 (1.05;1.68) | 1.35 (1.08;1.69) | ||||
| Sexual violence in childhood | 0.001 | 0.001 | ||||||
| No | 1.00 | 1.00 | - | - | - | - | ||
| Yes | 1.33 (1.12;1.57) | 1.33 (1.13;1.56) | - | - | ||||
| Types of intimate partner violencec | 0.015 | 0.041 | <0.001 | <0.001 | ||||
| No type of violence | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| One type of violence | 1.28 (1.09;1.50) | 1.24 (1.06;1.46) | 1.08 (0.81;1.44) | 1.08 (0.82;1.40) | ||||
| Two types of violence | 1.18 (0.94;1.48) | 1.18 (0.93;1.48) | 1.28 (0.90;1.80) | 1.22 (0.89;1.66) | ||||
| Three types of violence | 1.26 (0.86;1.84) | 1.25 (0.87;1.81) | 2.27 (1.72;2.98) | 2.39 (1.83;3.10) | ||||
a) PR: Prevalence ratio; b) 95%CI: 95% confidence interval; c) Psychological, physical and sexual intimate partner violence in the last 12 months.
Family income and partner profile were shown to be factors associated with current sleep-inducing medication use: prevalence increased 1.30 time (95%CI 1.03;1.64) among women with lower income (up to BRL 1,500) and 1.35 time (95%CI 1.08;1.69) among women whose partners were controllers.
In relation to exposure to sexual violence in childhood, this was associated with lifetime use of sleep-inducing medication (PR=1.33; 95%CI 1.13;1.56), when compared to women who reported not having been victims of this type of violence. Regarding intimate partner violence, the results showed that lifetime use of sleep-inducing medication was 24% (95%CI 1.06;1.46) more prevalent among women who experienced violence in the last 12 months, when compared to those who were not victims of violent acts. Also, current medication use was 2.4 times (95%CI 1.83;3.10) higher among women who had experienced the three types of violence (psychological, physical, and sexual) in the past 12 months compared with those who had no history of violence.
Discussion
Among women who used primary health care services in Vitória, Espírito Santo, being older, having a lower level of schooling and having suffered intimate partner violence in the past 12 months were associated with greater use of sleep-inducing medication, both currently and during lifetime. In addition, occurrence of sexual violence in childhood was associated with lifetime use of sleep-inducing medication, while having lower income and a controlling partner was associated with current use.
In this study, prevalence of current use of sleep-inducing drugs was close to 20% among the women interviewed, while almost half of them had used these drugs at some time in their lives. A survey conducted in a Brazilian urban setting showed that 22.2% of the women interviewed were taking benzodiazepine anxiolytics.21 A study conducted in the second half of 2012, in the city of Presidente Prudente, SP, identified that women reported greater difficulty in sleeping, which may induce use of sleep-inducing medication.6
Standing out among other issues capable of influencing sleep is the important role that women play in different activities, both in society and in caring for the home, which can interfere with their mental health.22 In general, women have higher levels of anxiety and depression, and their sleep is disturbed by personal or professional worries.23
In this study, prevalence of lifetime and current use of sleep-inducing medication was higher among women in the 40-59 age group, when compared to women in the 20-39 age group. In the interior region of the state of Minas Gerais, higher prevalence of tranquilizer use was also found in the 40-59 age group (44.6%). Use of this medication with advancing age may occur due to work overload, daily stress, as well as body transformations that occur in this stage of life, due to the menopause.24
Research conducted in 2013 in a medium-sized municipality in the western region of Minas Gerais indicated that insomnia and anxiety affect women with lower levels of schooling more,12 which could justify the higher frequency we found in our study of current use of sleep-inducing medication among women with lower levels of schooling. Higher schooling levels may have a positive effect on self-care health behaviors, promoting better quality sleep6 and, as such, may contribute to the lower frequency of current sleep-inducing medication use in this group.
The frequency of use of this type of medication was also higher among women with lower family income. This finding is similar to that of another study, in which the highest frequency of benzodiazepine use was reported among low-income women. Lower income groups may resort to the use of medication to solve the psychosocial difficulties of life.25
Having a controlling partner increased the prevalence of current sleep-inducing medication use. Occurrence of sexual violence in childhood also increased lifetime prevalence of use of this medication. Research with 613 Chinese women revealed that among the various forms of intimate partner violence, controlling actions had the most detrimental consequences for women’s mental health.21 Moreover, the onset of drug abuse is related to the occurrence of vital events, such as childhood sexual violence.12
Among the participants analyzed, prevalence of use of sleep-inducing medication was higher among women who had experienced some type of violence in the last 12 months, whether psychological, physical or sexual. A study conducted in 2016, in the municipality of Serra, also in the state of Espírito Santo, aimed at characterizing women in situations of violence, found that the main complaint of 69.1% of the victims was inadequate sleep, while some 39% had used tranquilizers in the last four weeks. 26 A study conducted in 2007 on violence and use of psychoactive substances in the cities of São Paulo and Recife, showed that 62.8% of women who suffered psychological violence took tranquilizers, 37.2% of those exposed to physical violence took tranquilizers and 20.9% of those who suffered sexual violence also used these drugs.27
Women who are victims of intimate partner violence may have sleep disorders.16 According to a cross-sectional study conducted in Spain between December 2009 and January 2010, frequency of tranquilizer and anxiolytic use is around 180% higher among women who recognize that they are experiencing intimate partner violence, compared to those who do not recognize that they are in this situation. That study also found greater use of other classes of medications, such as antidepressants, analgesics and anti-inflammatory drugs.28
In this context, healthcare professionals have a relevant role in relation to users of sleep-inducing drugs, as they are responsible for promoting the rational use of these drugs, guiding and warning about their harmful effects when used improperly.29 Screening of sleep patterns is still not systematic. Thus, quality of sleep is constantly neglected, causing women to be treated and medicated in response to their complaints rather than in response to the source of the problem, which may be a result of violence suffered at home.27
The composition of this study’s sample -women who use public health services - can be mentioned as a limitation, as it limits the scope of the results, which are not representative of the female share of the general population. Users of public health services tend to present more sleep disorders13 and so prevalence of medication use may be overestimated. On the other hand, the question used to ask women directly about use of sleep-inducing medication had a dichotomous answer option (no or yes), i.e., no medical records or prescriptions were consulted, which may have led to underestimated prevalence. Similarly, no information was collected on the type of medication, which could be pharmaceutical or herbal, nor on how the medications were acquired, which could have been self-medication resulting from it being indicated by someone close to them, a medical prescription given by Family Health Strategy services or by a psychiatrist working in public or private services. Another point to be considered is the absence of behavioral characteristics regarding use of alcohol, cigarettes and drugs as variables. The ‘sexual violence’ in childhood variable was obtained by asking a direct question, with a dichotomous answer, equally subject to underestimation.
It is possible to conclude that use of sleep-inducing medication was frequent among women users of PHC services in the municipality of Vitória. Socioeconomic aspects and experiencing violence were associated with higher intake of these medications. As such, it is of the utmost importance for health professionals to be aware of use of this medication, as well as to investigate possible factors associated with this practice. It is therefore essential that these professionals offer women attentive listening and holistic care, in order to be able to unveil the factors associated with use of this medication, such as experiencing violence - often omitted by women - in order to enable its cycle to be broken. Finally, it is important to develop further studies on the impact of violence on use of sleep-inducing drugs. We hope that the results presented here will contribute to the expansion of the debates about the impacts that violence can have on women’s health.
REFERENCES
1. Ribeiro NF. Tratamento da Insônia em Atenção Primária à Saúde. Rev Bras Med Fam Comunidade. 2016;11(38):1-14. doi: 10.5712/rbmfc11(38)1271 [ Links ]
2. Sholat T. Impact of lifestyle and technology developments on sleep. Nat Sci Sleep. 2012;4:19-31. doi: 10.2147/NSS.S18891 [ Links ]
3. Uhlig BL, Sand T, Odegård SS, Hagen K. Prevalence and associated factors of DSM-V insomnia in Norway: the Nord-Trøndelag Health Study (HUNT 3). Sleep Med. 2014;15:708-13. doi: 10.1016/j.sleep.2014.01.018 [ Links ]
4. Zhang B, Wing YK. Sex differences in insomnia: a meta-analysis. Sleep. 2006;29(1):85-93. doi: 10.1093/sleep/29.1.85 [ Links ]
5. Madrid-Valero JJ, Martínez-Selva JM, Couto BR, Sánchez-Romera JF, Ordoñana JR. Age and gender effects on the prevalence of poor sleep quality in the adult population. Gac Sanit. 2017;31(1):18-22. doi: 10.1016/j.gaceta.2016.05.013 [ Links ]
6. Zanuto EAC, Lima MCS, Araújo RG, Silva EP, Anzolin CC, Araujo MYC, et al. Distúrbios do sono em adultos de uma cidade do estado de São Paulo. Rev Bras Epidemiol. 2015;18(1):42-53. doi: 10.1590/1980-5497201500010004 [ Links ]
7. Kodaira K, Silva MT. Sleeping pill use in Brazil: a population-based, cross-sectional study. BMJ Open. 2017;7(7):e016233. doi: 10.1136/bmjopen-2017-016233 [ Links ]
8. Kubota AMA, Silva MNR, Masioli AB. Aspectos da insônia no adulto e a relação com o desempenho ocupacional. Rev Ter Ocup Univ. 2014;25(2):119-25. doi: 10.11606/issn.2238-6149.v25i2p119-125 [ Links ]
9. Silva PA, Almeida LY, Souza J. O uso de benzodiazepínicos por mulheres atendidas em uma Unidade de Saúde da Família. Rev Esc Enferm USP. 2019;53:e03419. doi: 10.1590/s1980-220x2017038903419 [ Links ]
10. Souza CL, Aldrighi JM, Lorenzi-Filho G. Qualidade do sono em mulheres paulistanas no climatério. Rev Assoc Med Bras. 2005;51(3):170-6. doi: 10.1590/S0104-42302005000300019 [ Links ]
11. Bezerra DS, Bonzi ARB, Siva GR, Lima AKBS. Mulheres e o uso de benzodiazepínicos: uma revisão integrativa. Temas em Saúde [Internet]. 2018 [citado 2020 mar 14];18(2):204-215. Disponível em: http://temasemsaude.com/wp-content/uploads/2018/07/18213.pdf [ Links ]
12. Silva VP, Botti NCL, Oliveira VC, Guimarães EAA. Perfil epidemiólogico dos usuários de benzodiazepínicos na atenção primária à saúde. R Enferm Cent O Min. 2015;5(1):1393. doi: 10.19175/recom.v0i0.546 [ Links ]
13. Pontes CAL, Silveira LC. Abuso de benzodiazepínicos entre mulheres: o que esse fenômeno revela? Sanare. 2017 [citado 2020 mar 14];16(1):15-23. Disponível em: https://sanare.emnuvens.com.br/sanare/article/view/1089/600 [ Links ]
14. Paulino-Pereira FC, Santos LGA, Mendes SCC. Gênero e identidade: possibilidades e contribuições para uma cultura de não violência e equidade. Psicol Soc. 2017;29:e172013. doi: 10.1590/1807-0310/2017v29172013 [ Links ]
15. Campbell JC. Health consequences of intimate partner violence. Lancet. 2002;359(9314):1331-6 [acesso em 02 dez 2020]. doi: 10.1016/s0140-6736(02)08336-8 [ Links ]
16. Campbell JC, Lewandowski LA. Mental and physical health effects of intimate partner violence on women and children. Psychiatr Clin North Am. 1997;20(2):353-74. doi: 10.1016/s0193-953x(05)70317-8 [ Links ]
17. Deeke LP, Oliveira WF, Coelho EBS. A dinâmica da violência doméstica: uma análise a partir dos discursos da mulher agredida e de seu parceiro. Saude Soc. 2009;18(2):248-58. doi: 10.1590/S0104-12902009000200008 [ Links ]
18. Instituto Brasileiro de Geografia e Estatística. Censo demográfico 2010 - Espírito Santo - Cariacica [Internet]. Rio de Janeiro: Instituto Brasileiro de Geografia e Estatística; 2017 [citado 2021 jan 29]. Disponível em: https://cidades.ibge.gov.br/brasil/es/cariacica/panorama [ Links ]
19. Ministério da Saúde (BR). Secretaria de Atenção Primária à Saúde. E-Gestor atenção básica: cobertura da atenção básica. Brasília: Ministério da Saúde; 2021 [citado 2021 maio 01]. Disponível em: https://egestorab.saude.gov.br/paginas/acessoPublico/relatorios/relHistoricoCoberturaAB.xhtml [ Links ]
20. Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R, editores. Relatório mundial sobre violência e saúde. Genebra: Organização Mundial da Saúde; 2002 [citado 2021 ago 01]. Disponível em: http://portaldeboaspraticas.iff.fiocruz.br/wp-content/uploads/2019/04/14142032-relatorio-mundial-sobre-violencia-e-saude.pdf [ Links ]
21. Tiwari A, Chan KL, Cheung DST, Fong DYT, Yan ECW, Tang DHM. The differential effects of intimate terrorism and situational couple violence on mental health outcomes among abused Chinese women: a mixed-method study. BMC Public Health. 2015;15:314.doi: 10.1186/s12889-015-1649-x [ Links ]
22. Prado MAMB, Francisco PMSB, Barros MBA. Uso de medicamentos psicotrópicos em adultos e idosos residentes em Campinas, São Paulo: um estudo transversal de base populacional. Epidemiol Serv Saúde. 2017;26(4):747-58.doi: 10.5123/s1679-49742017000400007 [ Links ]
23. Oliveira RF, Daniele TMC, Façanha CFS, Forti AC, Bruin PFC, Bruin VMS. Adiponectin levels and sleep deprivation in patients with endocrine metabolic disorders. Rev Assoc Med Bras. 2018;64(12):1122-8. doi: 10.1590/1806-9282.64.12.1122 [ Links ]
24. Alves DMP, Coelho VGM, Kohler LM. Perfil de um grupo de usuários de clonazepam no município de Manhuaçu. Rev Educ Meio Amb e Saúde. 2016;6(1):44-60. [ Links ]
25. Nordon DG, Akamine K, Novo NF, Hubner CVK. Características do uso de benzodiazepínicos por mulheres que buscavam tratamento na atenção primária. Rev Psiquiatr RS. 2009;31(3):151-8. doi: 10.1590/S0101-81082009000300004 [ Links ]
26. Leite FMC, Silva ACA, Bravim LR, Tavares FL, Primo CC, Lima EFA. Mulheres vítimas de violência: percepção, queixas e comportamentos relacionados à sua saúde. Rev Enferm UFPE on line. 2016;10(Supl. 6):4854-61. doi: 10.5205/reuol.8200-71830-3-SM.1006sup201618 [ Links ]
27. Silva VN. Violência e uso de substâncias psicoativas: um estudo com mulheres usuárias de um serviço de Atenção Primária à Saúde de São Paulo [dissertação]. São Paulo (SP): Universidade de São Paulo; 2008. Disponível em: https://www.teses.usp.br/teses/disponiveis/5/5137/tde-24112008-134920/pt-br.php [ Links ]
28. Sonego M, Gandarillas A, Zorrilla B, Lasheras L, Pires M, Anes A, et al. Unperceived intimate partner violence and women's health. Gac Sanit. 2013;27(5):440-6. doi: 10.1016/j.gaceta.2012.11.009 [ Links ]
29. Nunes BS, Bastos FM. Efeitos colaterais atribuídos ao uso indevido e prolongado de benzodiazepínicos. Saúde Cienc Açao. 2016 [2020 mar 14];3(1):71-82. Disponível em: http://revistas.unifan.edu.br/index.php/RevistaICS/article/view/234/177 [ Links ]
Associate Academic Work This manuscript was derived from the final degree course assignment entitled ‘Use of sleeping pills: prevalence and association with intimate partner violence’, defended by Jasmine Cristina Soares Xavier at the Department of Nursing of the Universidade Federal do Espírito Santo, in 2019.
Received: May 06, 2021; Accepted: December 21, 2021
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
