










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkEpidemiologia e Serviços de Saúde
versión impresa ISSN 1679-4974versión On-line ISSN 2237-9622
Epidemiol. Serv. Saúde vol.31 no.1 Brasília 2022 Epub 05-Mayo-2022
http://dx.doi.org/10.1590/s1679-49742022000100021
Original Article
Diabetes as a factor associated with hospital deaths due to COVID-19 in Brazil, 2020
1 Universidade Estadual do Ceará, Programa de Pós-Graduação em Cuidados Clínicos em Enfermagem e Saúde Fortaleza, CE, Brazil
2 Universidade Estadual do Ceará, Graduação em Enfermagem, Fortaleza, CE, Brazil
Objective:
To analyze the association between diabetes mellitus and hospital deaths due to Covid-19 in Brazil, from February to August 2020.
Methods:
This was a cross-sectional study on hospitalized flu-like syndrome cases, with a positive test result for COVID-19, reported on the Influenza Epidemiological Surveillance Information System. Poisson regression with robust variance was used to estimate the magnitude of the association between diabetes and deaths.
Results:
Data from 397,600 hospitalized cases were analyzed, of which 32.0% (n = 127,231) died. The prevalence of death among people with diabetes was 40.8% (PR = 1.41; 95%CI 1.39;1.42). After adjustments for the variables sociodemographic and comorbidities, it could be seen that those with diabetes (95%CI 1.14;1.16) were 1.15 time more likely to die.
Conclusion:
3 out of every 20 deaths due to COVID-19 occurred among individuals with diabetes mellitus, highlighting this population susceptibility and the need to control this chronic disease.
Keywords: Diabetes Mellitus; Coronavirus Infections; Mortality; Hospitalization; Cross-Sectional Studies
Study contributions
Main results
The prevalence of deaths among hospitalized cases of COVID-19 with diabetes was higher when compared to hospitalized cases of COVID-19 without diabetes mellitus, in Brazil. Three out of every 20 deaths due to COVID-19 occurred among individuals with diabetes.
INTRODUCTION
In the last two years, science has sought to identify clinical characteristics associated with the severity of COVID-19, including the role of diabetes mellitus in the morbidity and mortality from this disease. Individuals with diabetes mellitus usually present greater severity of COVID-19, a fact observed in other viral pandemics, such as severe acute respiratory syndrome (SARS), in 2003, influenza A(H1N1), in 2009, and Middle East respiratory syndrome coronavirus in 2012.1-3
Diabetes is frequently associated with other clinical conditions, such as arterial hypertension, overweight, heart and kidney diseases.4 Regarding the clinical evolution of diabetic individuals hospitalized with COVID-19, it can be seen that the presence of comorbidities influences the clinical prognosis,5 and that the infection caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) seems to contribute to worsening the clinical alterations resulting in hyperglycemia, increasing the risk of diabetic emergencies and death.5 The main factor attributed to COVID-19 complications in individuals with diabetes is related to disease-associated microangiopathy and the potential direct toxicity of SARS-CoV-2 in metabolically relevant tissues, including pancreatic beta cells, targets of insulin action.6,7 Another hypothesis for worsening COVID-19 in people with diabetes attributes inflammation and oxidative stress and, consequently insulin resistance, to the angiotensin-converting enzyme 2 (ACE2), in the pathogenesis of type 2 diabetes and COVID-19.8
With regard to the Brazilian scenario, as at June 2021, data revealed that more than 18 million people were infected with the novel coronavirus and more than 500,000 deaths due COVID-19 disease were recorded, putting the country in the spotlight in the global pandemic scenario in relation to the occurrence of cases. Therefore, scientists from all over the world have been worried about cumulative evidence on worsening COVID-19 prognosis in people with diabetes, especially in countries with a high prevalence of both diseases, such as Brazil.3
Thus, it is important a better understanding of the role of diabetes in deaths due to COVID-19 in a country with the fourth highest prevalence of diabetes in the world, especially when the syndemic potential of these diseases is recognized.9 As such, the aim of this study was to analyze the association between diabetes mellitus and hospital deaths due to COVID-19 in Brazil.
METHODS
This was a cross-sectional study, conducted between November 2020 and February 2021, on COVID-19 cases reported on the Influenza Epidemiological Surveillance Information System (SIVEP-Gripe) from February to August 2020. SIVEP-Gripe, a Brazilian health information system, gathers national epidemiological data on suspected and confirmed cases of any disease presenting flu-like symptoms, including COVID-19. SIVEP-Gripe provides sociodemographic, clinical laboratory, comorbidity and hospitalization data.
This study included reported and confirmed cases of people hospitalized with flu-like symptoms and positive reverse transcription-polymerase chain reaction (RT-PCR) test for SARS-CoV-2 nationwide. We also established, as inclusion criteria in this study, hospitalization due to the disease. According to national protocols, hospitalized cases are those with moderate and severe flu-like symptoms, and a positive test result for COVID-19.
The main exposure of the study was to present diabetes (yes; no), being verified in self-report, during admission interview, being a laboratory-confirmed diagnosis, during hospitalization, duly registered on the notification system. The main outcome was death (yes; no), recorded on the notification system.
The following variables were considered, recognized as possible confounders in the association between diabetes mellitus and deaths due to COVID-19:
-
Sociodemographic
Age group [in years: young (under 18 years of age); adult (18 to 59); elderly (60 or over)], created from the variable 'age';
Sex (male; female).
Schooling (illiterate; elementary education, cycle 1; elementary education, cycle 2; high school; higher education).
-
Clinical signs and symptoms
Vomiting, diarrhea, dyspnea, fever, oxygen saturation <95% (yes; no).
-
Comorbidities
Pneumopathies, neurological disorders, liver disease, heart disease, kidney diseases, immunodepression (yes; no).
-
Severe conditions during hospitalization
Nosocomial infection and intensive care unit admission (yes; no).
The theoretical model used to assess the association between diabetes mellitus and death due to COVID-19 was developed using the web-based software DAGitty (http://www.dagitty.net). It is worth highlighting that the directed acyclic graph (DAG) shows the theoretical model developed by the researchers, who established possible relationships between confounding variables or mediators of association and also selection and information biases.10
Regarding the DAG presented in this research (Figure 1), it can be seen that the direct relationship between having diabetes and death due to COVID-19 was tested, given that only people hospitalized due to the second condition took part in this study. We can also identify the possible mediating variables of this association, such as signs and symptoms (vomiting, diarrhea, fever, dyspnea, anosmia and oxygen saturation <95%), nosocomial infection and severity (identified as intensive care unit admission). The other variables were defined, in the theoretical model, as possible confounders of association.
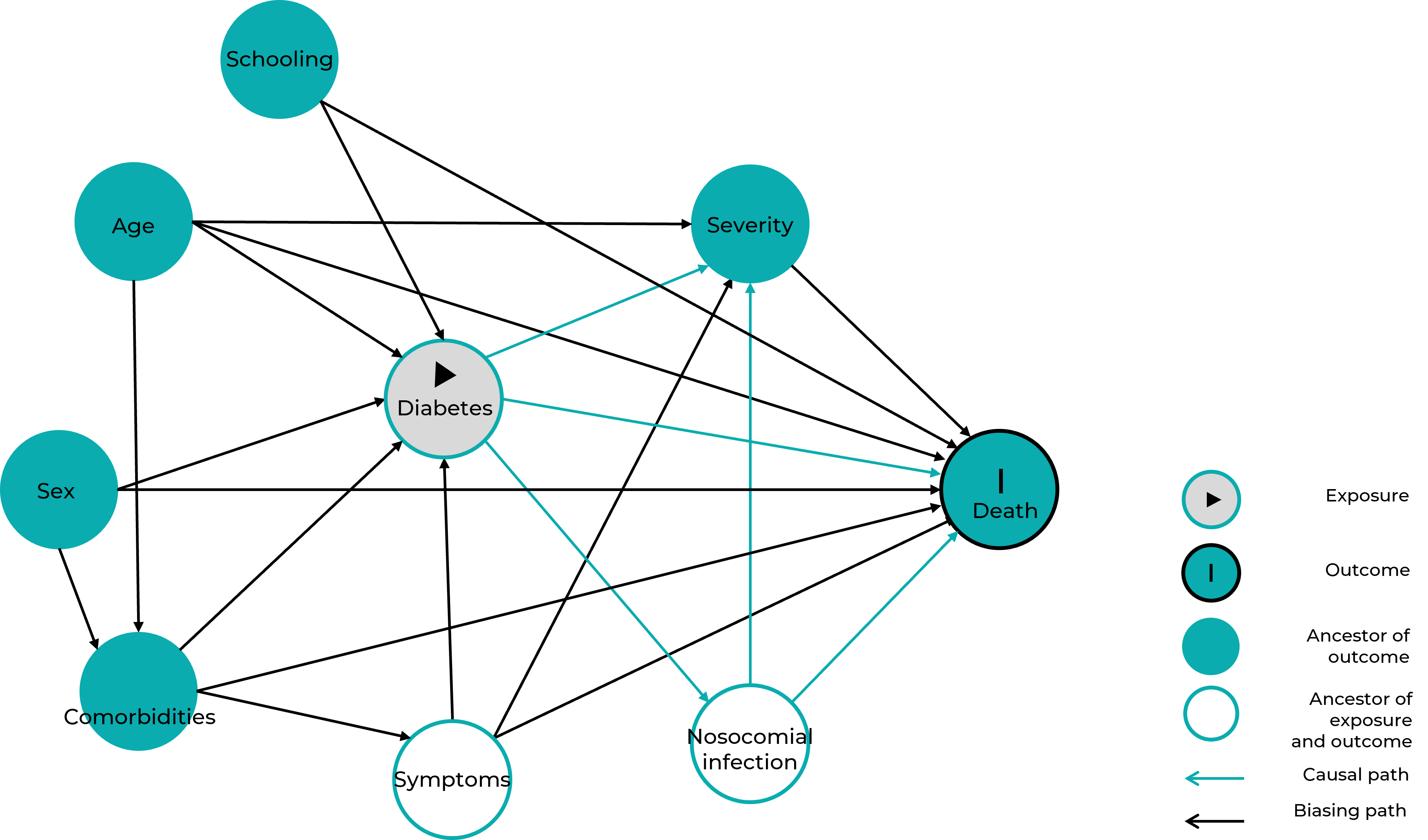
Figure 1 Directed acyclic graph of the relationship between diabetes mellitus and deaths due to COVID-19
For data analysis, we initially calculated the case fatality ratio due COVID-19, estimated by the ratio between the number of deaths and the total number of confirmed cases of the disease, multiplied by 100. Then, the descriptive analysis of variables was performed. Categorical variables were described using simple and relative frequencies. The association between these variables and 'death' outcome was verified using Pearson's chi-square test.
In order to test the hypothesis presented in the DAG, regarding a direct relationship between diabetes and COVID-19, Poisson regression model with robust variance estimator was used, adopting p-value <0.20 for entry in the model. This regression model was inserted due to the high prevalence of the outcome.11 Thus, initially, the association between diabetes and the outcome was verified in a crude model and then adjustments were made for potential confounding factors, as shown in Figure 1. Thus, the set of minimum adjustments sufficient to estimate the adjusted effect of diabetes on death was made by including sociodemographic variables (age, sex and schooling) and comorbidities or disease-associated (pneumopathies, neurological disorders, asthma, liver disease, kidney failure, immunodepression and heart disease) in the regression model.
The final model was defined after complete adjustment of confounding variables (sociodemographic and comorbidities). The strength of association was calculated using the prevalence ratio (PR) and 95% confidence interval (95%CI). The adequacy of the models was evaluated according to the pseudo R2 value (used for binary outcomes), which showed how much the model can explain the variation of the data presented: it is expected that the higher the pseudo R2, the better the model. In addition, the akaike information criterion (AIC) and the bayesian information criterion (BIC) were used, therefore it is expected that the lowest value presents the best fit.
It was not necessary to submit this study to a Research Ethics Committee, because the database, made available by the Brazilian Ministry of Health, with open access, does not allow any identification of notified cases, such as name or address. The researchers also complied with the ethical guidelines for handling, analysis and publication of data, as recommended by the National Health Council, resolution No. 466, published on December 12, 2012, and No. 510, of April 7, 2016.
Results
Database retrieved from the SIVEP-Gripe platform had a total of 1,048,575 notifications by the end of the study period. 359,575 of which were related to discarded cases and 271,334 did not present the test result for COVID-19, both datasets were excluded from the study; another 12,776 non-hospitalized cases, and 7,693 without information about the date of hospitalization were also disregarded. Therefore, the basis for this research was comprised of a total of 397,600 hospitalized confirmed COVID-19 cases. The application of the criteria reduced the total missing values of the variables studied to less than 1%. Among the variables analyzed, the percentage of ignored information on the variables 'sex' and 'schooling' were 0.02% (n = 84) and 0.8% (n = 3,184), respectively.
Of the total of 397,600 hospitalized COVID-19 cases, in Brazil, 32.0% (n = 127,231) died. The prevalence of death among people with diabetes was 40.8% (n = 41,766), with a statistical association between diabetes and death (p<0.001). Figure 2 shows the increase in case fatality ratio due to COVID-19, when associated with diabetes, in all the months studied, ranging from 2,712 (28.6%) to 5,067 (50.1%) in the selected period. Table 1 presents an analysis of the characteristics of deaths due to COVID-19. It could be seen the association between death due to the disease and sociodemographic variables and the pathological processes that were observed (p<0.001).
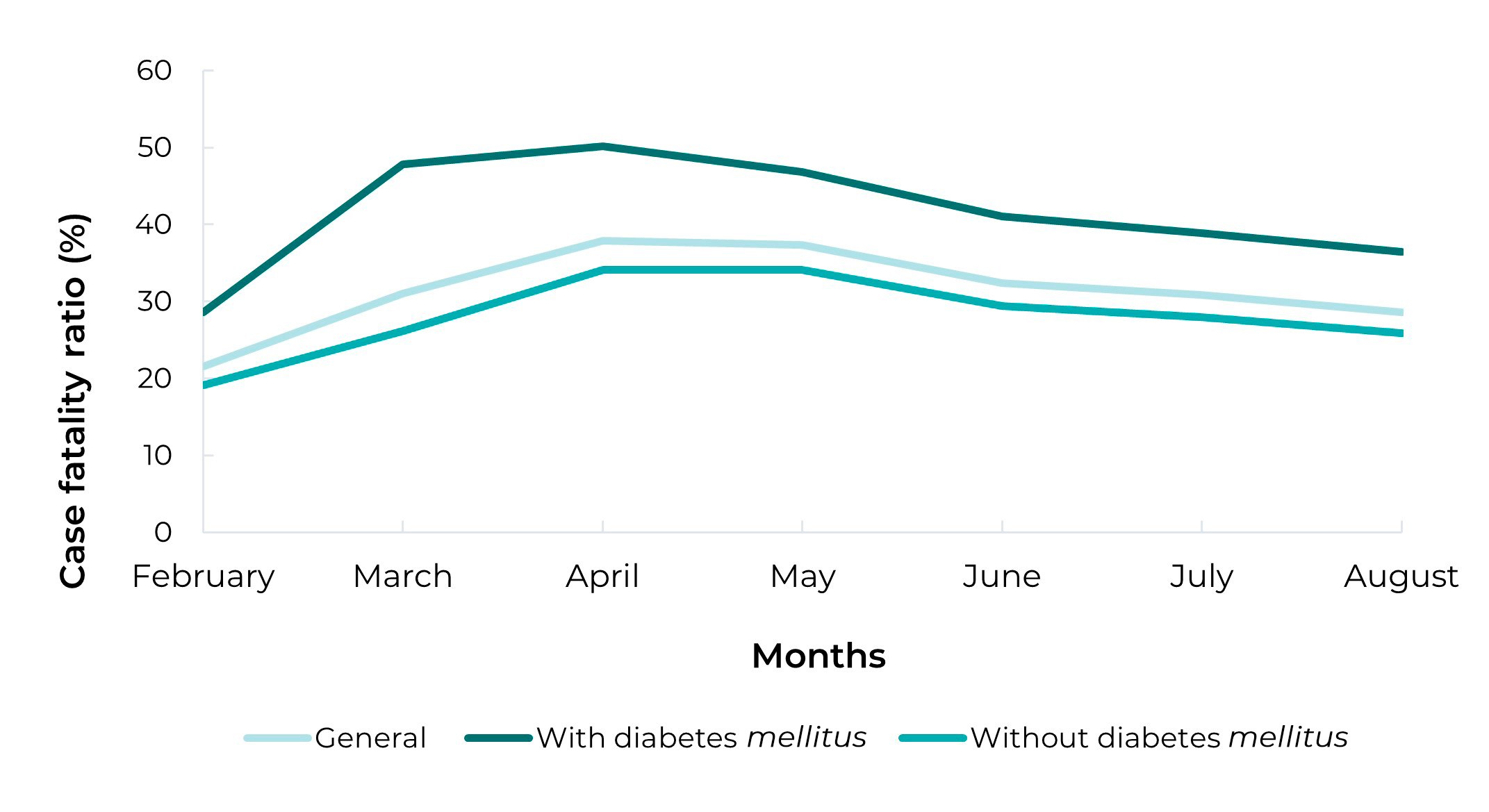
Figure 2 Distribution of case fatality ratio due to COVID-19 among hospitalized people and in the group of cases, with or without diabetes mellitus, Brazil, 2020
Table 1 Characteristics associated with death among people hospitalized with COVID-19 (n = 397,600), Brazil, 2020
| Characteristics | Total (%) | Death | p-value | |
|---|---|---|---|---|
| Yes (%) | No (%) | |||
| Diabetes mellitus | <0.001a | |||
| Yes | 102,389 (25.7) | 41.776 (40.8) | 60.613 (59.2) | |
| No | 295,211 (74.3) | 85,455 (28.4) | 209.756 (71.1) | |
| Age group (years) | <0.001a | |||
| <18 | 8,686 (2.2) | 668 (7.7) | 8,018 (92.3) | |
| 18-59 | 191,489 (48.2) | 38,555 (20.1) | 152,934 (79.9) | |
| ≥60 | 197,425 (49.6) | 88,008 (44.6) | 109,417 (55.4) | |
| Sex | <0.001a | |||
| Female | 223,903 (56.3) | 73,777 (32.9) | 150,126 (67.1) | |
| Male | 173,613 (43.7) | 53,431 (30.8) | 120,182 (69.2) | |
| Schooling | <0.001a | |||
| Illiterate | 127,472 (32.3) | 41,985 (32.9) | 85,487 (67.1) | |
| Elementary education - cycle 1 | 38,291 (9.7) | 15,982 (41.7) | 22,309 (58.3) | |
| Elementary education - cycle 2 | 164,590 (41.7) | 54,034 (32.8) | 110,556 (67.2) | |
| High school | 43,335 (11.0) | 10,888 (25.1) | 32,447 (74.9) | |
| Higher education | 20,728 (5.3) | 4,079 (19.7) | 16,649 (80.3) | |
| Vomiting | <0.001a | |||
| Yes | 32,135 (8.1) | 8,580 (26.7) | 23,555 (73.3) | |
| No | 365,465 (91.9) | 118,651 (32.5) | 246,814 (67.5) | |
| Diarrhea | <0.001a | |||
| Yes | 54,249 (13.6) | 13,779 (25.4) | 40,470 (74.6) | |
| No | 343,351 (86.4) | 113,452 (33.0) | 229.899 (67,0) | |
| Anosmia | <0.001a | |||
| Yes | 15,692 (3.9) | 2,999 (19.1) | 12,693 (80.9) | |
| No | 381,908 (96.1) | 124,232 (32.5) | 257,676 (67.5) | |
| Dyspnea | <0.001a | |||
| Yes | 281,356 (70.8) | 99,179 (35.2) | 182,177 (64.7) | |
| No | 116,244 (29.2) | 24,052 (24.1) | 88,192 (75.9) | |
| Fever | <0.001a | |||
| Yes | 257,978 (64.9) | 76,893 (29.8) | 181,085 (70.2) | |
| No | 139,622 (35.1) | 50,338 (36.0) | 89,284 (64.0) | |
| Pneumopathies | <0.001a | |||
| Yes | 14,964 (3.8) | 7,589 (50.7) | 7,375 (49.3) | |
| No | 382,636 (96.2) | 119,642 (31.3) | 262,994 (68.7) | |
| Neurological disorders | <0.001a | |||
| Yes | 15,875 (4.0) | 8,356 (52.6) | 7,519 (47.4) | |
| No | 381,725 (96.0) | 118,875 (31.1) | 262,850 (68.9) | |
| Asthma | <0.001a | |||
| Yes | 10,695 (2.7) | 2,750 (25.7) | 7,945 (74.3) | |
| No | 386,905 (97.3) | 124,481 (32.1) | 262,424 (67.8) | |
| Liver disease | <0.001a | |||
| Yes | 3,662 (0.9) | 1,885 (51.5) | 1,777 (48.5) | |
| No | 393,938 (99.1) | 125,346 (31.8) | 268,592 (68.2) | |
| Heart disease | <0.001a | |||
| Yes | 135,387 (34.0) | 54,190 (40.0) | 81,197 (60.0) | |
| No | 262,213 (66.0) | 73,041 (27.9) | 189,172 (72.1) | |
| Kidney diseases | <0.001a | |||
| Yes | 16,924 (4.3) | 9,031 (53.4) | 7,893 (46.6) | |
| No | 380,676 (95.7) | 118,200 (31.0) | 262,476 (69.0) | |
| Immunodepression | <0.001a | |||
| Yes | 10,879 (2.7) | 4,946 (45.5) | 5,933 (54.5) | |
| No | 386,721 (97.3) | 122,285 (31.6) | 264,436 (68.4) | |
| Nosocomial infection | <0.001a | |||
| Yes | 8,384 (2.1) | 4,005 (47.8) | 4,379 (52.2) | |
| No | 389,216 (97.9) | 123,226 (31.7) | 265,990 (68.3) | |
| Oxygen saturation <95% | <0.001a | |||
| Yes | 229,440 (57.7) | 87,948 (38.3) | 141,492 (61.7) | |
| No | 168,160 (42.3) | 39,283 (23.4) | 128,877 (76.6) | |
| Intensive care unit admission (ICU) | <0.001a | |||
| Yes | 64,868 (16.3) | 37,899 (58.4) | 26,969 (41.6) | |
| No | 332,732 (83.7) | 89,332 (26.8) | 243,400 (73.2) | |
| Total | 397,600 (100.0) | 127,231 (32.0) | 270,369 (68.0) | |
a) Pearson’s chi-squared test.
The crude prevalence ratio of the association between diabetes and death due to COVID-19 was 1.48 (95%CI 1.39;1.42) (Table 2). The prevalence ratio was 1.20 (95%CI 1.19;1.21) after adjusting for sociodemographic factors (model 2). In the analysis adjusted for variables related to the presence of comorbidities (model 3), the PR value became 1.15 (95%CI 1.14;1.16), representing a 15% higher prevalence of death among Brazilians with diabetes hospitalized due to COVID-19.
Table 2 Association between diabetes mellitus and death among people hospitalized with COVID-19 (n = 394,337), Brazil, 2020
| Models | Death | |||||
|---|---|---|---|---|---|---|
| PRa | 95%ICb | p-valuec | R2d | AICe | BICf | |
| Model 1 (crude)g | 1.41 | 1.39;1.42 | <0.001 | 0.6% | 541,244.0 | 541,265.8 |
| Model 2h | 1.20 | 1.19;1.21 | <0.001 | 4.1% | 519,680.3 | 519,778.3 |
| Model 3i | 1.15 | 1.14;1.16 | <0.001 | 4.7% | 516,191.6 | 516,365.8 |
a) PR: Prevalence ratio; b) 95%CI: 95% confidence interval; c) P-value referring to robust Poisson regression analysis; d) R2: coefficient of determination; e) AIC: Akaike information criterion; f) BIC: Bayesian information criterion; g) Model 1: Diabetes mellitus; h) Model 2: Model 1 + age group + sex + schooling; i) Model 3: Model 2 + pneumopathy + neurological disease + asthma + liver disease + renal dysfunction + immunodepression + heart disease.
In the crude model, R² = 0.6%; AIC = 541,244.00; BIC = 541,265.8 were obtained. In contrast, the final model presented: R² = 4.7%; AIC=516,191.6; BIC = 516,874.8 (Table 2). The application of adjustment criteria indicated in the method confirmed the final model as the most appropriate for the estimates of the presented outcome.
Discussion
The study showed that in Brazil, the prevalence of death due to COVID-19 among hospitalized cases was higher among individuals with diabetes mellitus, compared to non-diabetic people, between February and August 2020. These results contribute to a better knowledge of the clinical profile of people infected with SARS-CoV-2 virus and the understanding of how chronic diseases can affect the prognosis of COVID-19.
The association between diabetes and deaths due to COVID-19 remained, even to a lesser extent, after adjustments for confounding factors (sociodemographic and comorbidity variables), as demonstrated in other studies.12,13
This work has some limitations. The main one refers to information on the diagnosis of diabetes, the main self-reported predictor variable. The second limitation is related to the use of secondary data, obtained for clinical and non-research purposes, and may represent problems of incompleteness or inadequacies in filling out, interfering in the results found, although the inclusion and exclusion criteria applied may reduce this bias. Another limiting factor is the large amount of ignored information regarding some variables. For example, even with the criteria used by the authors in the population-based selection, the variable 'obesity' was not considered because it presented a high percentage of missing data. Finally, the analysis restricted to hospitalized cases may have overestimated the association between diabetes and deaths due to COVID-19. However, this is a hospital-based study, in which i) diabetes cases are more likely to achieve greater severity and a higher number of comorbidities, while ii) COVID-19 cases tend to be moderate or severe.
Several studies have sought to better characterize the clinical profiles of infection caused by the novel coronavirus, including the most frequent signs and symptoms, and to identify factors associated with the prognosis of COVID-19. In Brazil, as in most developing countries,14 diabetes was identified as a cause of premature mortality and disability, according to a study15 that showed that 61% of individuals hospitalized with COVID-19 died and presented at least one comorbidity, especially heart disease and diabetes.
The literature reports different levels of prevalence of cases presenting diabetes associated with COVID-19, in several countries in the world. In Italy, for example, studies showed a 17% to 35% variation in the prevalence of associated diseases.16 Systematic review and meta-analysis of random effects showed a 35% chance of severe cases and a 50% chance of death among diabetic people with COVID-19;17 a Brazilian cross-sectional study showed 46.9% prevalence of diabetes and COVID-19;18 while a historical cohort study, followed in a city in Northeastern Brazil, showed 5.5%, of these, 49.1% died.19
Several hypotheses may explain the association between diabetes and death due to COVID-19 among hospitalized people. One of them is that diabetes, as a chronic disease, alters metabolic functions and thus immune responses, making the disease carriers more susceptible to SARS-CoV-2 infections. In individuals with diabetes, metabolic processes, important mediators of defense mechanisms, do not act appropriately in order to protect the body against physiological damage resulting from infections.19 In addition, diabetes increases the risk of pulmonary fibrosis, obstructive pulmonary disease and reduced lung function, which may also decrease organ oxygenation.20
The concurrence of these two diseases can also contribute to the occurrence of thromboembolic events, by increasing D-dimer and fibrinogen levels, potentiating the risks of unfavorable outcomes in these individuals. Hypercoagulable state associated with diabetes and COVID-19 may lead to an amputation. A study conducted in the United States indicates that during the pandemic, diabetic people with COVID-19 were 10.8 times more likely to undergo any level of amputation, and the risk of major amputation (above ankle level) likewise increased.21 As such, it is worth highlighting that glycemic control is fundamental to the prevention of these conditions.22,23
Another relevant point is the fact that the various levels of social isolation adopted during the months of the pandemic have changed people's lifestyle, their prolonged staying at home, increasing anxiety and food consumption.24 This may have implied a higher calorie intake, lower energy expenditure and metabolic instability,25,26 those are factors that have a significant impact on people with diabetes due to the glycemic changes caused by the disease.
Taking these results, it can be concluded that the prevalence of death due to COVID-19 among hospitalized people with diabetes was 15% higher when compared to the prevalence of hospitalized COVID-19 cases without diabetes in Brazil. During the pandemic, the greatest vulnerability to COVID-19 was found among the population with diabetes. These findings suggest the need to develop strategies for prevention and management of COVID-19 in people with diabetes mellitus.
REFERENCES
1. Yan Y, Yang Y, Wang F, Ren H, Zhang S, Shi X, et al. Clinical characteristics and outcomes of patients with severe COVID-19 with diabetes. BMJ Open Diabetes Research and Care. 2020;8(1): e001343. doi: 10.1136/bmjdrc-2020-001343 [ Links ]
2. Down S. COVID-19 and diabetes. Diabetes & Primary Care. 2020;22(2):25-6. [ Links ]
3. Brito VP, Carrijo AMM, Olveira SV. Association between Diabetes Mellitus and the severity of COVID-19 and its potential mediating factors: a systematic review. Rev Thema. 2020;18:204-17. doi: 10.15536/thema.V18.Especial.2020.204-217.1820 [ Links ]
4. Souza CL, Oliveira MV. Fatores associados ao descontrole glicêmico de diabetes mellitus em pacientes atendidos no Sistema Único de Saúde no Sudoeste da Bahia. Cad Saude Colet. 2020;28(1):153-64. doi: 10.1590/1414-462X202028010319 [ Links ]
5. Escosteguy CC, Eleuterio TA, Pereira AGL, Marques MRVE, Brandão AD, Batista JPM. COVID-19: estudo seccional de casos suspeitos internados em um hospital federal do Rio de Janeiro e fatores associados ao óbito hospitalar. Epidemiol Serv Saude. 2020;30(1):e2020750. doi: 10.1590/S1679-49742021000100023 [ Links ]
6. Pérez-Martínez P, Sánchez FJC, Gómez JC, Gómez-Huelgas R. Resolviendo una de las piezas del puzle: COVID-19 y diabetes tipo 2. Rev Clin Esp. 2020;220(8):507-10. doi: 10.1016/j.rce.2020.05.003 [ Links ]
7. Muniangi-Muhitu H, Akalestou E, Salem V, Misra S, Oliver NS, Rutter GA. COVID-19 and diabetes: a complex bidirectional relationship. Front Endocrinol. 2020;11:582936. doi: 10.3389/fendo.2020.582936 [ Links ]
8. Sourij H, Aziz F, Brauer A, Clardi C, Clodi M, Fasching P, et al. COVID-19 fatality prediction in people with diabetes and prediabetes using a simple score at hospital admission. Diabetes Obes Metab. 2021;23(2):589-98. doi: 10.1111/dom.14256 [ Links ]
9. International Diabetes Federation. IDF Diabetes Atlas. 4th ed. [Brussels]: International Diabetes Federation; 2009 [cited 2022 jan 12]. Available from: https://www.idf.org/component/attachments/attachments.html?id=811&task=download [ Links ]
10. Cortes TR, Faerstein E, Struchiner CJ. Use of causal diagrams in epidemiology: application to a situation with confounding. Cad Saúde Pública. 2016;32(8):e001033115. doi: 10.1590/0102-311X00103115 [ Links ]
11. Coutinho LMS, Scazufca M, Menezes PR. Methods for estimating prevalence ratios in cross-sectional studies. Rev Saude Publica. 2008;42(6):992-8. doi: 10.1590/S0034-89102008000600003 [ Links ]
12. Kumar A, Arora A, Sharma P, Anikhindi SA, Bansal N, Singla V, et al. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab Syndr. 2020;14(4):535-45. doi: 10.1016/j.dsx.2020.04.044 [ Links ]
13. Huang I, Lim MA, Pranata R. Diabetes mellitus is associated with increased mortality and severity of disease in COVID-19 pneumonia - A systematic review, meta-analysis, and meta-regression. Diabetes Metab Syndr. 2020;14(4):395-403. doi: 10.1016/j.dsx.2020.04.018 [ Links ]
14. Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Especial: doença pelo coronavírus 2019. Bol Epidemiol. 2020 [citado 2022 jan 02];23. Disponível em: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/boletins-epidemiologicos/covid-19/2021/boletim-epidemiologico-covid-19-no-23.pdf/view [ Links ]
15. Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, et al. Baseline characteristics and outcomes of 1.591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16):1574-81. doi: 10.1001/jama.2020.5394 [ Links ]
16. Centers for Disease Control and Prevention. Preliminary estimates of the prevalence of selected underlying health conditions among patients with coronavirus disease 2019. MMWR Morb Mortal Wkly Rep. 2020;69(13):382-6. doi: 10.15585/mmwr.mm6913e2 [ Links ]
17. Almeida-Pititto B, Dualib P, Zajdenverg L, Dantas JR, Souza FD, Rodacki M, et al. Severity and mortality of COVID19 in patients with diabetes, hypertension and cardiovascular disease: a meta-analysis. Diabetol Metab Syndr. 2020;12:75. doi: 10.1186/s13098-020-00586-4 [ Links ]
18. Garces TS, Sousa GJB, Florêncio RS, Cestari VRF, Pereira MLD, Moreira TMM. COVID-19 in a state fo Brazilian Northeast: prevalence and associated factors in people with flu-like syndrome. J Clin Nurs. 2020;29(21-22):4343-8. doi: 10.1111/jocn.15472 [ Links ]
19. Sousa GJB, Garces TS, Cestari VRF, Florêncio RS, Moreira TMM, Pereira MLD. Mortality and survival of COVID-19. Epidemiol Infect. 2020;148:e123. doi: 10.1017/S0950268820001405 [ Links ]
20. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020; 395(10229):1054-62. doi: 10.1016/S0140-6736(20)30566-3 [ Links ]
21. Casciato DJ, Yancovitz S, Thompson J, Anderson S, Bischoff A, Ayres S, et al. Diabetes-related major and minor amputation risk increased during the COVID-19 pandemic. J Am Podiatr Med Assoc. 2020;20:224. doi: 10.7547/20-224 [ Links ]
22. Acquah S. Implications of COVID-19 pandemic on evolution of diabetes in malária-endemic african region. J Diabetes Res. 2020:8205261. doi: 10.1155/2020/8205261 [ Links ]
23. Wang Z, Du Z, Zhu F. Glycosylated hemoglobin is associated with systemic inflammation, hypercoagulability, and prognosis of COVID-19 patients. Diabetes Res Clin Pract. 2020;164:108214. doi: 10.1016/j.diabres.2020.108214 [ Links ]
24. Wijaya I, Andhika R, Huang I. Hypercoagulable state in COVID-19 with diabetes mellitus and obesity: Is therapeutic-dose or higher-dose anticoagulant thromboprophylaxis necessary?. Diabetes Metab Syndr. 2020;14(5):1241-2. doi: 10.1016/j.dsx.2020.07.015 [ Links ]
25. Biancalana E, Parolini F, Mengozzi A, Solini A. Short-term impacto f COVID-19 lockdown on metabolic controlo f patients with well-controlled type 2 diabetes: a single-centre observational study. Acta Diabetol. 2020;58(4):431-6. doi: 10.1007/s00592-020-01637-y [ Links ]
26. Ghosh A, Arora B, Gupta R, Anoop S, Misra A. Effects of nationwide lockdown during COVID-19 epidemic on lifestyle and other medical issues of patients with type 2 diabetes in north India. Diabetes Metab Syndr. 2020;14(5): 917-20. doi: 10.1016/j.dsx.2020.05.044 [ Links ]
Received: October 05, 2021; Accepted: March 31, 2022
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
