











 texto em
texto em  Inglês (pdf)
Inglês (pdf)
 Artigo em XML
Artigo em XML Referências do artigo
Referências do artigo
 Curriculum ScienTI
Curriculum ScienTI Enviar este artigo por email
Enviar este artigo por email Citado por SciELO
Citado por SciELO  Similares em
SciELO
Similares em
SciELO 
 Permalink
PermalinkStudy contributions
Main results
The violence against the elderly most notified was physical violencefollowed by psychological and self-inflicted violence. Completeness of some important notification form fields was lower than expected.
Introduction
The instructions for notification of interpersonal and self-inflicted violence, published by the Ministry of Health in 2016, define cases to be notified on the Notifiable Health Conditions Information System (Sistema de Informação de Agravos de Notificação − SINAN) as “suspected or confirmed cases of domestic/intrafamily violence, sexual violence, self-inflicted violence, human trafficking, slave labor, child labor, torture, legal intervention, and homophobic violence against females and males of all ages. In the case of extra-family/community violence, only the following shall be notified: violence against children, adolescents, women, elderly people, people with disabilities, Indigenous and LGBT people”.1 Specifically in relation to violence against the elderly (VAE), the instructions classify this type of violence according to its nature, namely psychological violence, physical violence, sexual violence, violence against property, neglect, torture and human trafficking.1
VAE is a public health problem in many parts of the world, including Brazil.2,3 Data from a systematic review and meta-analysis of VAE prevalence based on 52 articles published between 1992 and 2015, from 28 countries in diverse geographical locations (America, Europe, Asia, Pacific, Mediterranean), found that overall prevalence of different manifestations of violence was 15.7%, i.e., around one in six people over 60 years old had been a victim of violence.3 Women are the main victims of violence in this age group.2,4
In Brazil, data on VAE prevalence are still scarce and difficult to systematize because they include only a few types of violence, are measured differently by various studies, and are concentrated in the South and Southeast regions of the country.2,4 In the city of Niterói, located in the state of Rio de Janeiro, one population-based study was conducted on VAE, in 2006, with individuals over 60 years old, non-institutionalized and living in areas covered by the then Family Health Program, now referred to as the Family Health Strategy. In that study the prevalence of physical violence against the elderly was 10.1%.5
Given the accelerated aging of the population in more recent decades,6 and given the implementation of the Violence and Accidents Surveillance System (Sistema de Vigilância de Violências e Acidentes − VIVA) as part SINAN, in 2006, and the inclusion of VAE on the list of compulsorily notifiable health conditions, the number of VAE notifications has been increasing in Brazil.7 Between 2006 and 2011, the number of notifications increased by around 261%.7 In the first half of 2020 (first year of the COVID-19 pandemic), reports of VAE received by the Disque 100 rights violations reporting service also showed an increase: 40.3% of the reports of violations against the elderly received by the service referred to neglect; 24.6%, to psychological violence; 20.1%, to violence against property and 12.2%, to physical violence.8
Studies analyzing the profile of VAE notifications in Brazil are, for the most part, restricted to the period before the COVID-19 pandemic. Eleven studies on the subject were identified, conducted in different regions of the country: three addressed notifications made nationwide,7,9,10 one was conducted in the states of the Southern region,11 two were conducted using data from the state of Rio Grande do Sul,12,13 one was conducted in the state of Espírito Santo,14 two involved notifications in the city of São Paulo City,15,16 one in the city of Campinas17 and one using data from the state of Pernambuco.18 The completeness of the fields of the notification form for violence against the elderly was not assessed in these studies.
The COVID-19 pandemic contributed to the increase in cases of VAE due to the increased vulnerability of the elderly, resulting from isolation, abandonment by family members, reduced purchasing power, as well as a reduction in support networks, access to health services and social protection.19 It is noteworthy that there are no published national studies that analyze this type of violence during the COVID-19 pandemic.
Studies analyzing the profile of VAE notifications before and during the pandemic, as well as the analysis of the quality of these data, including evaluation of the completeness of the notification form fields, are of great relevance and necessary. Considering Brazil’s size and regional diversity, gaining knowledge about this problem at the local level can contribute to understanding its characteristics, besides enabling evaluation of the quality of this type of information in municipalities with similar characteristics to the municipality we studied here, the results of which we hope will be of great value for raising the awareness of health service managers and workers, in all the Brazilian federative units, given the importance of recording notifications as part of service routines. When this information is of good quality, it enables the development and implementation of concrete actions that are more in keeping with the profile identified, so as to ensure prevention, reception of cases, and follow-up of situations involving VAE.
The objective of this study was to analyze the profile of notifications of VAE and their degree of completeness in the city of Niterói, state of Rio de Janeiro, Brazil.
Methods
This is a descriptive study having as its data source VAE notification forms held on the SINAN for the period from January 2011 to December 2020.
Niterói is located in the metropolitan region of Rio de Janeiro. It has an estimated population of 515,317 inhabitants in 2020,20 19.5% of whom are over 60 years old, according to data from the Brazilian National Health System’s Department of Information Technology (Departamento de Informática do Sistema Único de Saúde − DATASUS).21 In 2018, 29.5% of the city’s households reported per capita monthly income of up to half a minimum wage.20 Niterói is in seventh place in Brazil, and in first place in the state of Rio de Janeiro, in the classification of municipalities with the highest human development index (HDI): 0.873.20
The municipality has had a Violence Surveillance Committee since 2014. It is headed by a team from the Methodological Supervision Sector (Setor de Supervisão Metodológica − DESUM), which reports to the Vice Presidency of Collective, Outpatient and Family Care (Vice-Presidência de Atenção Coletiva, Ambulatorial e da Família), within the City Health Department. The Committee is comprised of health professionals from the Primary Care teams, representatives of school institutions, the hospital network, and related bodies, such as the Social Assistance Reference Center (Centro de Referência de Assistência Social) and the Guardianship Council (Conselho Tutelar), among others. This Committee, which meets every two months, monitors the cases notified by technicians working with situations of violence and technicians from the municipal Surveillance Coordination service. All notified cases (new or in progress) are sent to the reference teams for monitoring. The majority of the notifications are made by hospital units, following provision of urgent and emergency care.
In accordance with VIVA-SINAN system instructions, in this study suspected or confirmed cases of VAE were defined as “interpersonal psychological violence, physical violence, sexual violence, violence against property, torture, human trafficking, neglect, as well as self-inflicted violence and/or suicide attempt, against an individual aged 60 or over”.1 The study included the notifications held on the VIVA-SINAN system of cases involving individuals aged 60 or over of both sexes.
The SINAN data were provided to the researchers by the City Health Department’s Epidemiological Surveillance service in March 2021. The data did not contain any information that could enable identification of the people involved in the cases. In order to evaluate the percentage completeness of the different fields of the notification form, the frequency of missing data and fields filled in as “unknown” was analyzed for each of the variables considered in the analysis, performed year by year, according to the standards recommended for the SINAN system: good completeness (category 1), when more than 75.0% of the fields are filled out; regular completeness (category 2), between 50.1% and 75.0%; poor completeness (category 3), from 25.1% to 75.0%; or very poor completeness (category 4), 25.0% or less of the fields filled out.1
The sociodemographic variables relating to the profile of the victims were: age (in completed years); sex (male; female; unknown); race/skin color (White; mixed race; Black, Indigenous; Asian; and unknown); schooling (illiterate; 1st to 4th grade incomplete; 4th grade complete; 5th to 8th grade incomplete; elementary school complete; high school incomplete; high school complete; higher education incomplete; higher education complete; not applicable; unknown); and marital status (single; married/living together; widowed; separated; not applicable; unknown). In addition, we analyzed the variable regarding the presence of any type of disability or disorder (yes; no; unknown).
The variables related to the characterization of the situations of violence were: place of occurrence (residence; collective housing; school; sports facility; bar or similar; public road; commerce/services; industry/construction; other; unknown); recurrence (yes; no; unknown); and means of assault (physical force/pushing; hanging; blunt object; sharp object; hot substance/object; poisoning; intoxication; firearm; threat; other). The types of violence suffered were categorized as follows: psychological, physical, sexual, neglect, self-inflicted injury and/or suicide attempt, other (torture, human trafficking, and violence against property). We also analyzed whether there had been referral to other reference services (yes; no; unknown).
The variables corresponding to the possible perpetrator of the assault were: sex of the probable perpetrator (male; female; both sexes; unknown); number of people involved (one; two or more; unknown); relationship to the victim (father; mother; spouse; ex-spouse; boyfriend/girlfriend, ex-boyfriend/girlfriend; son/daughter; brother/sister; friend/acquaintance; stranger; caregiver; boss; person with institutional relationship; the person him/herself; other; unknown); and suspected use of alcohol (yes; no; unknown).
For the purpose of presenting the profile of the cases reported, the cases were analyzed year by year, according to the variables described. The description of the profile of the reported cases was based only on the fields of the forms that had regular and good completeness.
The results were presented in absolute numbers and percentages. The comparison of each type of violence reported, according to the characteristics of the victim and the possible perpetrator, was analyzed using Pearson’s chi-square test (χ2), with a 5% significance level, to identify statistically significant differences.
The moving-average smoothers method was used to estimate the smoothed trend of the number of notifications over the selected years. All analyses were performed using Stata software, version 15.
The research project was exempted from approval by the Universidade do Estado do Rio de Janeiro Research Ethics Committee, in accordance with National Health Council Resolution No. 466, dated December 12, 2012,22 since the study used secondary data derived from a public domain database, provided by the Niterói City Health Department’s Epidemiological Surveillance service in March 2021. The database provided contained no information capable of identifying the cases.
Results
There were 486 notifications of VAE in the period from January 2011 to December 2020 in the municipality of Niterói. The following information showed good completeness: sex; age; race/skin color; all types of violence against the elderly; and relationship between the aggressor and the victim. The following fields of the form showed regular completeness: marital status; having a disability/disorder; place of occurrence; number of people involved; and sex of the aggressor. The fields referring to the victim’s schooling, recurrence of the event, suspected alcohol use by the aggressor, and referral to another health sector had very poor/poor completeness in all years of the times series (Table 1).
Table 1 Completeness of fields on the violence against the elderly notification forms, Niterói, Rio de Janeiro, Brazil, 2011-2020
| Variables | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | Total | Completeness |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| (n = 3) | (n = 14) | (n = 9) | (n =6) | (n = 44) | (n = 37) | (n = 79) | (n = 75) | (n = 109) | (n = 110) | (n = 486) | ||
| % | % | % | % | % | % | % | % | % | % | % | ||
| Individual notification | ||||||||||||
| Sex | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | Good |
| Age | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | Good |
| Race/skin color | 100.0 | 92.8 | 88.9 | 83.3 | 75.0 | 67.5 | 91.1 | 81.3 | 69.7 | 70.0 | 76.7 | Good |
| Schooling | 100.0 | 14.3 | 55.5 | 50.0 | 27.2 | 13.5 | 11.4 | 23.5 | 11.0 | 21.8 | 32.8 | Very poor |
| Marital status | 100.0 | 85.7 | 66.6 | 83.3 | 47.7 | 43.2 | 55.7 | 54.6 | 44.0 | 55.4 | 52.9 | Regular |
| Disability or disorder | 66.6 | 64.3 | 55.5 | 50 | 36.3 | 37.8 | 70.9 | 36 | 66.0 | 66.3 | 57.0 | Regular |
| Occurrence | ||||||||||||
| Place of occurrence | 100.0 | 100.0 | 88.9 | 66.6 | 63.6 | 72.9 | 65.8 | 78.6 | 92.6 | 97.2 | 82.9 | Good |
| Recurrence | 100.0 | 64.3 | 77.8 | 66.6 | 43.2 | 35.1 | 30.4 | 37.3 | 35.8 | 50.9 | 41.5 | Poor |
| Type of violence | ||||||||||||
| Physical | 100.0 | 92.8 | 100.0 | 100.0 | 97.7 | 97.3 | 98.7 | 96 | 98.1 | 95.4 | 97.1 | Good |
| Neglect/abandonment | 100.0 | 92.8 | 100.0 | 83.3 | 97.7 | 97.3 | 98.7 | 96 | 99.1 | 98.1 | 97.7 | Good |
| Psychological | 100.0 | 100.0 | 100.0 | 83.3 | 90.9 | 97.3 | 97.4 | 89.3 | 96.3 | 92.7 | 94.2 | Good |
| Sexual | 100.0 | 100.0 | 100.0 | 100.0 | 93.2 | 100.0 | 98.7 | 94.6 | 99.1 | 99.1 | 97.2 | Good |
| Self-inflicted and/or suicide attempt | 100.0 | 92.8 | 88.9 | 83.3 | 97.7 | 100.0 | 97.4 | 94.6 | 99.1 | 98.2 | 97.3 | Good |
| Other | 100.0 | 92.8 | 100.0 | 83.3 | 93.2 | 94.6 | 97.4 | 89.3 | 96.3 | 94.5 | 94.4 | Good |
| Probable aggressor | ||||||||||||
| Number of people involved | 100.0 | 64.3 | 100.0 | 100.0 | 43.2 | 32.4 | 59.5 | 64.0 | 84.4 | 87.2 | 70.1 | Regular |
| Sex | 100.0 | 71.4 | 100.0 | 100.0 | 50 | 35.1 | 48.1 | 66.6 | 79.8 | 84.6 | 68.1 | Regular |
| Relationship to the victim | 100.0 | 92.8 | 88.9 | 100.0 | 54.5 | 51.3 | 70.9 | 76.0 | 92.6 | 92.7 | 80.0 | Good |
| Alcohol misuse | 33.3 | 42.8 | 44.4 | 66.6 | 15.9 | 37.8 | 45.5 | 37.3 | 37.6 | 56.3 | 41.7 | Poor |
| Referral | 66.6 | 71.4 | 33.3 | 83.3 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 100.0 | 97.5 | Good |
The description of the profile of the victims of violence is shown in Table 2. Most victims were female (54.3%), aged between 60 and 69 years (51.2%) and most of them were classified as being of White race/skin color (45.5%). Regarding place of occurrence, 62.3% of the episodes happened at home. The types of violence most reported were physical violence (48.1%), neglect/abandonment (34.3%) and psychological violence (22.2%). About 21% of the reported cases related to self-inflicted injuries and/or suicide attempts. Except for physical violence and neglect/abandonment, which were more present among males, the other types of violence were more frequent among females, especially sexual violence. This type of violence was only reported by females. A small part of the reported cases was referred to another health service (3.3%), and these victims were mainly female.
Table 2 Characteristics of cases of violence among elderly people notified on the Notifiable Health Conditions Information System, according to sex, Niterói, Rio de Janeiro, Brazil, 2011-2020
| Variables | Total | Male | Female | p-valuea | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| 486 | 100.0 | 222 | 45.7 | 264 | 54.3 | ||
| Age (years) | |||||||
| 60-69 | 249 | 51.2 | 117 | 52.7 | 132 | 50.0 | 0.112 |
| 70-79 | 134 | 27.6 | 67 | 30.2 | 67 | 25.4 | |
| ≥ 80 | 103 | 21.2 | 38 | 17.1 | 65 | 24.6 | |
| Race/skin color | |||||||
| White | 221 | 45.5 | 106 | 47.7 | 115 | 43.9 | 0.698 |
| Black | 152 | 31.3 | 67 | 30.2 | 85 | 32.4 | |
| Unknown/missing | 113 | 23.2 | 49 | 22.1 | 64 | 23.7 | |
| Schooling (years of study) | |||||||
| < 4 | 20 | 4.1 | 5 | 2.2 | 15 | 5.7 | 0.138 |
| 4-7 | 16 | 3.3 | 7 | 3.2 | 9 | 3.4 | |
| 8-10 | 14 | 2.9 | 4 | 1.8 | 10 | 3.8 | |
| ≥ 11 | 38 | 7.8 | 16 | 7.2 | 22 | 8.3 | |
| Unknown/missing | 398 | 81.9 | 190 | 85.6 | 208 | 78.8 | |
| Marital status | |||||||
| Single | 95 | 19.5 | 48 | 21.6 | 47 | 17.8 | <0.001 |
| Married/living together | 69 | 14.2 | 45 | 20.3 | 24 | 9.1 | |
| Widowed | 73 | 15.0 | 12 | 5.4 | 61 | 23.1 | |
| Separated | 20 | 4.1 | 9 | 4.1 | 11 | 4.2 | |
| Unknown/missing | 229 | 47.2 | 108 | 48.6 | 121 | 45.8 | |
| Disability or disorder | |||||||
| Yes | 132 | 27.2 | 55 | 24.8 | 77 | 29.2 | 0.034 |
| No | 145 | 29.8 | 57 | 25.7 | 88 | 33.3 | |
| Unknown/missing | 209 | 43.0 | 110 | 49.5 | 99 | 37.5 | |
| Place of occurrence | |||||||
| Residence | 303 | 62.3 | 114 | 51.3 | 189 | 71.6 | <0.001 |
| Outros | 100 | 20.6 | 55 | 24.7 | 45 | 17.0 | |
| Unknown/missing | 83 | 17.1 | 53 | 24.0 | 30 | 11.4 | |
| Recurrence | |||||||
| Yes | 114 | 23.4 | 30 | 13.5 | 84 | 31.8 | <0.001 |
| No | 88 | 18.2 | 43 | 19.3 | 45 | 17.0 | |
| Unknown/missing | 284 | 58.4 | 149 | 67.2 | 135 | 51.2 | |
| Type of violenceb | |||||||
| Psychological | 108 | 22.2 | 41 | 18.4 | 67 | 25.4 | 0.060 |
| Physical | 234 | 48.1 | 108 | 48.6 | 126 | 47.7 | 0.989 |
| Sexual | 12 | 2.4 | 0 | 0.0 | 12 | 4.5 | 0.001 |
| Neglect/abandonment | 167 | 34.3 | 77 | 34.7 | 90 | 34.1 | 0.947 |
| Othersc | 17 | 3.5 | 7 | 3.1 | 10 | 3.8 | 0.660 |
| Self-inflicted injury and/or suicide attempt | 104 | 21.4 | 43 | 19.3 | 61 | 23.1 | 0.251 |
| Means of assault | |||||||
| Physical force | 95 | 37.9 | 44 | 38.6 | 51 | 37.2 | 0.081 |
| Sharp object | 17 | 6.8 | 9 | 7.9 | 8 | 5.8 | 0.037 |
| Threat | 14 | 5.6 | 1 | 0.9 | 13 | 9.5 | 0.002 |
| Poisoning | 11 | 4.4 | 5 | 4.4 | 6 | 4.4 | 0.132 |
| Blunt object | 9 | 3.6 | 6 | 5.3 | 3 | 2.2 | 0.046 |
| Firearm | 6 | 2.4 | 4 | 3.5 | 2 | 1.5 | 0.039 |
| Hot substance/object | 4 | 1.6 | 0 | 0.0 | 4 | 2.9 | 0.019 |
| Hanging | 1 | 0.4 | 0 | 0.0 | 1 | 0.7 | 0.028 |
| Outros | 72 | 28.7 | 32 | 28.1 | 40 | 29.2 | 0.017 |
| Referral | |||||||
| Yes | 16 | 3.3 | 2 | 1.0 | 14 | 5.3 | 0.207 |
| No | 458 | 94.2 | 214 | 96.3 | 244 | 92.5 | |
| Unknown/missing | 12 | 2.5 | 6 | 2.7 | 6 | 2.2 | |
a) Pearson’s chi-square test (χ2) for heterogeneity; b) Notifications of violence against an elderly person can include suspicion of one or more types of violence; c) Other forms of violence were taken into consideration (torture, violence against property and human trafficking).
Table 3 shows the profile of the alleged perpetrators. Most cases of VAE involved just one perpetrator (52.1%) and 33.5% of these aggressors were male. Regarding the possible perpetrator of the act of violence, the victim him/herself (i.e., self-inflicted violence) was most frequent (24.3%), followed by son/daughter (22.2%) and acquaintances (13.2%).
Table 3 Characteristics of possible aggressors in cases of violence notified on the Notifiable Health Conditions Information System, according to sex, Niterói, Rio de Janeiro, Brazil, 2011-2020
| Variables | Total | Male | Famale | |||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Number of people involved in violence | ||||||
| One | 253 | 52.1 | 99 | 44.6 | 154 | 58.3 |
| Two or more | 88 | 18.1 | 39 | 17.6 | 49 | 18.6 |
| Unknown/missing | 145 | 29.8 | 84 | 37.8 | 61 | 23.1 |
| Sex of the aggressor | ||||||
| Male | 163 | 33.5 | 90 | 40.5 | 73 | 27.6 |
| Female | 125 | 25.7 | 24 | 10.8 | 101 | 38.3 |
| Both | 43 | 8.9 | 20 | 9.0 | 23 | 8.7 |
| Unknown/missing | 155 | 31.9 | 88 | 39.7 | 67 | 25.4 |
| Aggressor’s relationship to the victim | ||||||
| Spouse/ex-spouse | 33 | 6.8 | 13 | 5.9 | 20 | 7.6 |
| Son/daughter | 108 | 22.2 | 41 | 18.5 | 67 | 25.4 |
| Brother/sister | 22 | 4.5 | 11 | 5.0 | 11 | 4.2 |
| Friend/acquaintance | 64 | 13.2 | 25 | 11.3 | 39 | 14.8 |
| Caregiver | 19 | 3.9 | 5 | 2.3 | 14 | 5.3 |
| The victims themselves | 118 | 24.3 | 49 | 22.1 | 69 | 26.1 |
| Aggressor suspected of being under the influence of alcohol | ||||||
| Yes | 52 | 10.7 | 19 | 8.6 | 33 | 12.5 |
| No | 151 | 31.1 | 60 | 27.0 | 91 | 34.5 |
| Unknown/missing | 283 | 58.2 | 143 | 61.4 | 140 | 53.0 |
Table 4 shows the characteristics of the cases reported by type of violence suffered, according to some of the socio-demographic characteristics of the victim. The greater part of the notifications of physical violence referred to elderly people between 60 and 69 years old (64.1%), those who were single (40.1%), with no disability or disorder (75.0%), and most occurred at home (61.2%).
Table 4 Frequency of notifications against elderly people on the Notifiable Health Conditions Information System, according to victim characteristics and type of violence, Niterói, Rio de Janeiro, Brazil, 2011-2020
| Variables | Physical | Neglect/abandonment | Psychological | Sexual | Self-inflicted | Othera | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | p-valueb | n (%) | p-valueb | n (%) | p-valueb | n (%) | p-valueb | n (%) | p-valueb | n (%) | p-valueb | |
| Sex | 0.989 | 0.947 | 0.060 | 0.001 | 0.251 | 0.660 | ||||||
| Male | 108 (46.2) | 77 (53.9) | 41 (38.0) | 0 (0.0) | 43 (58.6) | 7 (58.8) | ||||||
| Female | 126 (53.8) | 90 (46.1) | 67 (62.0) | 12 (100.0) | 61 (41.4) | 10 (41.2) | ||||||
| Age (years) | < 0.001 | < 0.001 | 0.233 | 0.449 | 0.331 | 0.344 | ||||||
| 60-69 | 150 (64.1) | 46 (27.5) | 64 (59.2) | 8 (66.7) | 59 (56.7) | 6 (35.3) | ||||||
| 70-79 | 61 (26.1) | 50 (30.0) | 26 (24.1) | 3 (25.0) | 28 (27.0) | 6 (35.3) | ||||||
| ≥ 80 | 23 (9.8) | 71 (42.5) | 18 (16.7) | 1 (8.3) | 17 (16.3) | 5 (29.4) | ||||||
| Race/skin color | 0.393 | 0.961 | 0.370 | 0.754 | 0.272 | 0.994 | ||||||
| White | 113 (56.7) | 89 (58.9) | 49 (54.5) | 7 (63.6) | 34 (66.7) | 10 (58.8) | ||||||
| Black | 86 (43.3) | 61 (41.1) | 41 (45.5) | 4 (36.3) | 17 (33.3) | 7 (41.2) | ||||||
| Schooling (years of study) | 0.835 | 0.254 | 0.523 | 0.657 | 0.291 | 0.416 | ||||||
| < 4 | 13 (23.6) | 7 (35.0) | 6 (25.0) | 1 (33.3) | 2 (12.5) | 2 (50.0) | ||||||
| 4-7 | 9 (16.4) | 4 (20.0) | 4 (16.7) | 0 (0.0) | 3 (18.8) | 0 (0.0) | ||||||
| 8-10 | 10 (18.2) | 4 (20.0) | 6 (25.0) | 0 (0.0) | 1 (6.2) | 0 (0.0) | ||||||
| ≥ 11 | 23 (41.8) | 5 (25.0) | 8 (33.3) | 2 (66.7) | 10 (62.5) | 2 (50.0) | ||||||
| Marital status | 0.001 | 0.003 | 0.157 | 0.128 | 0.724 | 0.368 | ||||||
| Single | 53 (40.1) | 37 (36.6) | 22 (34.9) | 4 (44.4) | 10 (30.3) | 3 (30.0) | ||||||
| Married/living together | 41 (31.1) | 22 (21.8) | 23 (36.6) | 0 (0.0) | 11 (33.3) | 5 (50.0) | ||||||
| Widowed | 23 (17.4) | 39 (38.6) | 13 (20.6) | 5 (55.6) | 10 (30.3) | 2 (20.0) | ||||||
| Separated | 15 (11.4) | 3 (3.0) | 5 (7.9) | 0 (0.0) | 2 (6.1) | 0 (0.0) | ||||||
| Disability or disorder | < 0.001 | < 0.001 | 0.022 | 0.121 | < 0.001 | 0.233 | ||||||
| Yes | 33 (25.0) | 66 (61.1) | 19 (33.9) | 2 (22.2) | 43 (76.8) | 6 (66.7) | ||||||
| No | 99 (75.0) | 42 (38.9) | 37 (66.1) | 7 (77.8) | 13 (23.2) | 3 (33.3) | ||||||
| Place of occurrence | < 0.001 | 0.184 | 0.603 | 0.058 | 0.001 | 0.762 | ||||||
| Residence | 98 (61.2) | 119 (78.8) | 58 (73.4) | 5 (50.0) | 88 (87.1) | 10 (71.4) | ||||||
| Outros | 62 (38.8) | 32 (21.2) | 21 (26.6) | 5 (50.0) | 13 (12.9) | 4 (28.6) | ||||||
| Recurrence | 0.439 | 0.008 | 0.014 | 0.001 | 0.485 | 0.173 | ||||||
| Yes | 55 (53.9) | 46 (69.7) | 37 (71.1) | 0 (0.0) | 22 (51.2) | 5 (83.3) | ||||||
| No | 47 (46.1) | 20 (30.3) | 15 (28.9) | 8 (100.0) | 21 (48.8) | 1 (16.7) | ||||||
a) Other types of violence were taken into consideration (torture, violence against property and human trafficking); b) We used Pearson’s chi-square test (χ2) for heterogeneity, taking a 5% significance level, to identify statistically significant differences.
Notifications of neglect/abandonment were proportionally higher among elderly males (53.9%), aged 80 years or more (42.5%), single or widowed (75.2%), with physical disability or disorder (61.1%) and history of past victimization (69.7%). The cases of sexual violence notified were exclusively against females, with no record of recurrence, while most of the records of self-inflicted violence related to elderly people with some type of disability or disorder (76.8%). Psychological violence and other types of violence (property, torture and human trafficking) showed no statistically significant differences, according to the characteristics studied (Table 4).
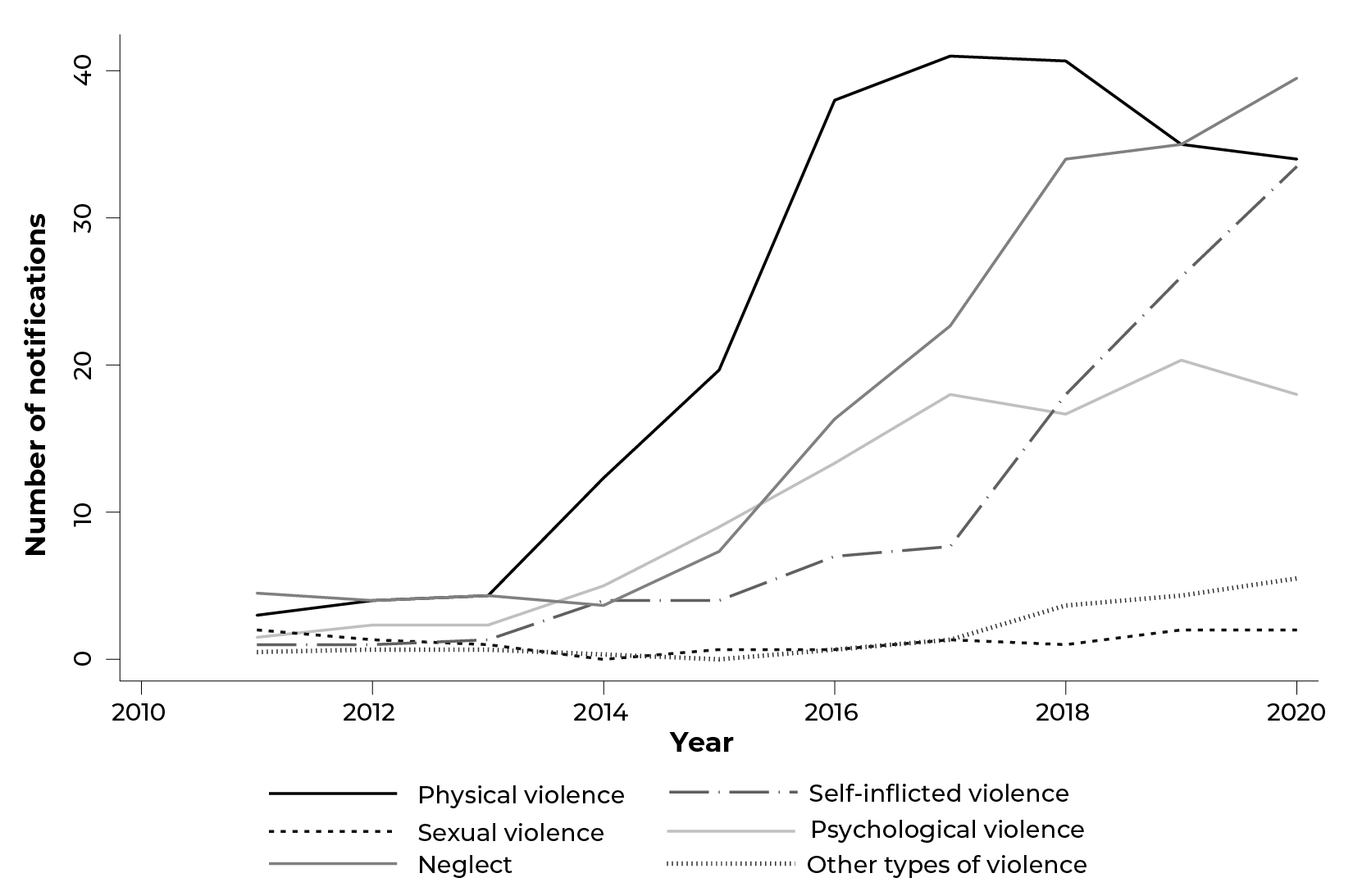
Figure 1 shows the smoothed trend of violence notifications over the period assessed. An increasing trend was found in notifications of self-inflicted violence, sexual violence, neglect/abandonment and other types of violence (torture, property violence and human trafficking). In 2020 (first year of the COVID-19 pandemic) the number of notifications increased for most types of violence analyzed, with the exception of physical and psychological violence.
Discussion
This study found that some of the notification form fields had a higher degree of incompleteness, namely: repeat violence, suspected alcohol use by the aggressor, victim’s schooling, and referral to another health sector. The type of violence most frequently reported was physical violence, followed by psychological and self-inflicted violence. For most types of violence analyzed, there was an increase in reported cases throughout the period assessed, including in the year in which the pandemic began (2020).
Studies using SINAN data can be useful for a general understanding of the quality of surveillance systems, completeness in filling out forms, besides enabling identification of weaknesses in these systems.23 Our analysis of VAE notification completeness found a variation in the pattern of filling out mandatory and essential variable fields; only the key fields showed good completeness. This evaluation of the key fields, however, should not be analyzed as a positive factor in the notification process, since without these fields it is not possible to input notification form information to the VIVA system database.
As for the mandatory variables, use of alcohol showed poor completeness, which leads to the discussion about possible difficulties in identifying and reporting this characteristic, as well as the importance of filling out this field in order to gain understanding of the problem and develop intervention strategies.24 Although the literature points to the use of alcohol as an important risk factor for the occurrence of all types of violence, including violence against the elderly,24 the poor completeness of these notifications does not allow us to assess whether this occurs in Niterói and therefore compromises assertive planning of health actions that address alcohol use from the perspective of VAE in the municipality.
Regarding the variables identified as essential, we highlight the classification of very poor completeness for the field related to schooling, for which the frequency of “unknown” information was 81.9%, this being high in comparison with the findings of the study conducted in southern Brazil,12 and the study conducted in the city of Recife,18 which found frequencies of 30.5% and 52.4%, respectively. It is noteworthy that important aspects for understanding the profile of the victim and the episode of violence showed regular to very poor completeness, namely: schooling, marital status, presence of disorder/disability, and repeat violence. The lack of this information makes it impossible to gain a better understanding of the profile of violence and its victims.
Another aspect to be highlighted, related to the low completeness of some fields of the forms, is that this information does not refer only to 2020, the year in which the COVID-19 pandemic began. The findings of this study show that low completion is a long-standing problem, found in the years prior to the pandemic. Improved completeness of the fields of the form should be encouraged, given its importance for identifying cases and consequently, developing policies more in keeping with the profile most vulnerable to this type of violence.12,18,23
When analyzing the profile of the reported cases, we found a higher number of notifications of violence against females, in addition to the fact that the main victims of VAE were between 60 and 69 years old. The findings of this study concerning the sex of VAE victims are similar to those obtained in most of the studies on the subject, both on the national and the local level, in the states of Paraná, Santa Catarina and Rio Grande do Sul, and in the cities of São Paulo and Recife.7,9,12,13,16,18
Over 20% of the reported cases were self-inflicted violence. Suicide attempts and suicide among the elderly are important public health problems in several parts of the world, including Brazil.24,25 When the Brazilian suicide mortality rates were analyzed for the period from 1980 to 2008, higher rates were found in the 70 or older age group. According to the authors, this indicator grew 29.5% in 26 years, although it is lower when compared to global estimates.
The difference between the most frequent types of VAE in the notifications we analyzed and those found in population-based studies. One study investigated the magnitude of VAE in the Ilha da Conceição neighborhood, located in Niterói, in 2006, and found psychological violence (43.2%) to be the most prevalent type of violence in the city, followed by physical violence (15.7%),26 differently from what we found in the present study. This difference reinforces the fact that notifications are “the tip of the iceberg”, since most of them refer to more serious, more visible and/or less socially tolerated situations of violence, such as, for example, physical and sexual violence. Physical violence is more frequently reported because the means of assault used is physical force, making it easier to identify when compared to other types of violence, such as psychological violence, financial violence and neglect/abandonment.27
Situations of violence can be aggravated in old age, due to increased dependence on care for carrying out daily activities and, in some cases, financial activities.19,28 In this sense, understanding intra-family dynamics favors identification of possible situations of intra-household violence. The present study found that the perpetrator of VAE is mainly an individual from the family environment who is close to the victim. This result is consistent with the literature, according to which most VAE is done by people close to them, such as children, spouses, ex-spouses, grandchildren and/or caregivers.8,29 As such, it is important to know the family dynamics,15 in which the Family Health Strategy can play a key role. Recognition of family members’ participation in these occurrences increases the potential for identifying these situations and, consequently, enables interventions to interrupt the cycle of violence, promoting the reduction/elimination of the recurrence of VAE.18 It is noteworthy that important variables for identifying and understanding the profile of aggressors had regular to poor completeness, which may hinder the drawing of a more detailed portrait of the possible perpetrator(s) of violence, reinforcing the importance of the training of health service professionals responsible for filling out notification forms.
In this study, referral of victims to other health sectors was recorded as not having taken place for most of the notifications (94.2%). This suggests a weakness of protection institutions in the municipality, since adequate referral of cases to reference sectors favors the formation of a network providing support and guaranteeing rights, thus contributing to the interruption of the cycle of violence.19 It is worth noting that the COVID-19 pandemic has further reduced governmental actions aimed at the well-being of the elderly and the social support network.19 It is important to point out that the number of referrals made in Niterói in 2020 was similar to that for 2019; however, these percentages are below what was expected (data not shown).
This study indicated an increasing trend in the number of reported cases of VAE in Niterói between 2011 and 2020. This growth may be related to both health service managers and health workers having greater access to information about the importance of identifying and notifying suspected cases, provided to them via booklets, documents and training courses held in the city. It is noteworthy that the results of this study are similar to those found in other national studies.9,12,13
Most of the types of violence analyzed increased in 2020. The opposite to that found by another study which focused on notifications of violence against children and adolescents in the state of Santa Catarina, also during the pandemic.30 One hypothesis for the continuing rising trend in notifications in Niterói, during the period covered here, may be related to the organization of the City Health Department, in particular the work of the city’s Violence Surveillance Committee. The Committee held periodic meetings with the purpose of reinforcing the importance of notifying suspected cases of violence during the social distancing period of the pandemic. According to Moraes et al.,19 the carrying out (i) of continuous monitoring by Family Health Strategy teams in their territories, through home visits, (ii) prioritization of care in services aimed at priority groups, even during lockdown, (iii) advertising campaigns to encourage the reporting of violence and (iv) intersectoral articulations, are initiatives that certainly contribute to cases of violence being notified.
This study should be analyzed in light of its limitations and strengths. The first limitation refers to the fact that it was carried out in a medium-sized municipality in the Rio de Janeiro metropolitan region, with high socioeconomic and quality of life indicators and, therefore, is not representative of most Brazilian municipalities, which limits the generalization of the findings to other places in the country. Another possible limitation, related to the use of secondary data derived from information systems, is possible underreporting and data recording errors, leading the study to underestimate this type of violence. Training and qualification of health professionals involved in the process of notifying suspected cases of VAE is fundamental in this sense, so as to minimize the problem in similar future situations.
Standing out among the strengths of this study is its analysis of notification form completeness, allowing identification of fields that are important for understanding cases of VAE, as well as those that need reinforcement and training regarding their completeness. Another strong point of the study refers to the inclusion of data for 2020, the year in which the COVID-19 pandemic began. Although publications are available dedicated to the topic of EAV in the context of the COVID-19 pandemic, this is the first study with empirical data that includes this period in Brazil.
Most notified suspected cases of VAE in the municipality of Niterói related to physical violence. When analyzing the time series, a rising trend in notifications can be seen, including in the initial period of the COVID-19 pandemic (2020), for most of the types of violence analyzed. The completeness of important fields for understanding the problem continues to be lower than expected, that is, the victim’s level of schooling, repeat violence and suspicion of alcohol use by the aggressor, which are fundamental for decision making for the protection of the elderly and prevention of VAE. Qualifying the surveillance process and valuing the quality of information are key elements for the formulation of public policies on prevention and control that are more in keeping with with Niterói's profile.
In conclusion, we highlight the importance of conducting population-based epidemiological studies in order to identify the real magnitude of the problem, at the local and the national level. Descriptive studies, focusing on gaining knowledge of the profile of violence against the elderly and the quality of its notification using data from the SINAN, both in other locations and for Brazil as a whole, are needed.

