











 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Similares en
SciELO
Similares en
SciELO 
 Permalink
PermalinkMansonelliasis is a disease caused by the accumulation of the Mansonella filaria genus in blood vessels. The first human report case of M. ozzardi in Brazil was made by Deane1 during an epidemiologic survey in the City of Manaus, Amazonas State, and since then has been reported in the States of Amazonas, Roraima, Mato Grosso and Acre2. During the 1950s, filaria were widely distributed throughout Amazonas, accompanied by high rates of filariasis in the Municipalities of the Solimões river, and more specifically in Codaiás (23.9%), Fonte Boa (17.8%), São Paulo de Olivença (12.6%) and Coari (10.0%)3. Since that time, more than 50 years passed without further researches being conducted in the Solimoes river; however, there are new studies on filaria vectors in the Municipality of Manacapuru4,5. Subsequently, an epidemiological study of M. ozzardi in the urban and rural areas of Coari6, and even more recently, in the Municipality of Tefé7 have been conducted, but there are no epidemiological surveys on mansonelliasis in Codajás.
The current study was carried out in the Municipalities of Codajas and Coari between 2011 and 2012, in the region of the Solimoes river, Amazonas State, which has experienced a large population that has increased because of the migratory flows due to installation of platforms used for petrol and gas extraction. It is known that mansonelliasis is endemic in these Municipalities3,6,8,9, where they have experienced a constant influx of people from several other regions of the country. Therefore, this study was designed to obtain updated information regarding the prevalence of M. ozzardi in the Municipalities of Codajás, and also in riverine communities of the Coari Municipality, which have not been previously studied.
The Municipalities of Codajás (3°50’S 62°3’W) and Coari (4°05’S 63°08’W) (Figure 1) are located approximately 297 and 363 km, respectively, from Manaus. The study was conducted in riverine communities: Codajás - Urucurizinho, Taracua, Massaranduba, Urucurizinho II, Vale de Benção, Murituba and Vila Nova, as well as other communities located in the Municipality of Coari bordering Codajás and Tefé - Tapiri, Miriti, Vila Camera, Camarazinho and Katua. In Codajás, a sample size was calculated using a prevalence of 18.9%6 design effect of 1.0 and a confidence interval of 95%. The target population of this study consisted of individuals aged ≥ 3 years old who were selected by convenience sampling methods, and were in their homes at the time when the field activities were performed. In this study, at least 30% of the population in each community was examined. A written informed consent was signed by each participant, and a parent to provide consent for children. The Ethics Committee of the Fundação de Medicina Tropical Doutor Heitor Vieira Dourado (protocol 1504/October 2010) approved the project.
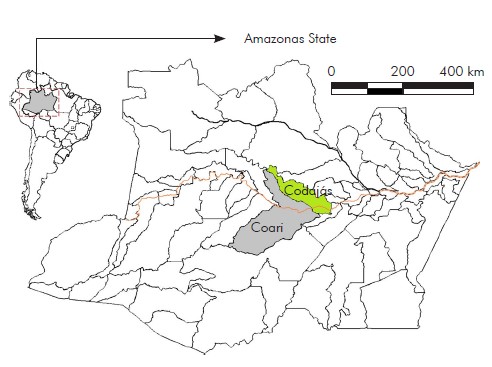
Figure 1 - Map of the studied area showing the Municipalities of Codajás and Coari, Amazonas State, Brazil
A total of 372 individuals, 245 in Codajas and 127 in Coari (average age = 27.7 ± 19.3 years old, range 3-86 years old) were examined for the presence of microfilariae by the thick blood smears using the following procedure. Two drops of blood (approximately 60 µ.L) were collected from each individual, they were dehemoglobinized, Giemsa stained and microscopically examined. In case of microfilaria (mf) it was found the morphological features that were compared with Post et al10, M. ozzardi mf were also identified using the polymerase chain reaction11.
All examined individuals were grouped by gender, age (3-10, 11-20, 21-30, 31-40, 41-50, 51-60, 61-70, 71-80 and ≥ 80 years) and occupation (farmer/fisherman, student, retired teacher, health agent, school manager, Eletrobrás’ technician and housewife). A factorial analysis of covariance (ANCOVA) adjusted to the binominal distribution of errors was performed to determine the prevalence of mansonelliasis in each occupational and age group. Thus, a full model was constructed in which the response variable was the prevalence of filariae, and the explanatory variables were group (two levels), occupation (six levels) and age (continuous variable). A step-down procedure based on Akaike information criterion values was used to determine the minimum adequate model. All analyses were performed using R statistical software, and p-values < 0.05 were regarded as statistically significant.
A total of 372 individuals were examined, and the unique mf specie found was identified as M. ozzardi. M. ozzardi mf was found in 23 (9.4%) and 28 (22.0%) individuals in Codajás and Coari, respectively. The highest prevalences of infection were found in the communities of Vila Nova (38.1%; 95% CI 19.5-59.8) and Katuá (72.7%; 95% CI 42.2-92.5) (Table 1). The prevalence of infection was significantly higher in men (17.1% - 27 microfilaraemic/158 examined) than in women (11.2% - 24/214) (ANOVA χ2 = -4.93; p = 0.02), and increased significantly according to age (ANOVA χ2 = -11.51; p < 0.001), with higher prevalences found in individuals aged ≥ 30 years old (Figure 2). A contrast analysis for infection prevalence based on occupation showed four different groups, with the rates of infection being highest among farmers/fishermen (29.2%) and retired (27.6%), others (15.0%) and students (1.8%) (ANOVA χ2 = -61.37; p < 0.001). It is noteworthy that no significant interaction among the different variables could be identified (Table 2).
Table 1 - Prevalence of M. ozzardi in riverine communities in the Municipalities of Codajás and Coari, Amazonas State, Brazil
| Communities | Total/Positive | Prevalence | 95% IC |
|---|---|---|---|
| Codajás | |||
| Urucurizinho | 49/5 | 10.2 | 3.8-21.2 |
| Taracua | 21/1 | 04.7 | 0.2-21.3 |
| Massaranduba | 28/0 | 00.0 | 0-10.1 |
| Urucurizinho II | 31/1 | 03.2 | 0.2-14.9 |
| Vale de Benção | 17/2 | 11.7 | 2.0-33.7 |
| Murituba | 80/6 | 07.5 | 3.1-14.9 |
| Vila Nova | 21/8 | 38.1 | 19.5-59.8 |
| Coari | |||
| Tapiri | 07/20 | 28.6 | 5.1-67.0 |
| Miriti | 27/30 | 11.1 | 2.9-27.3 |
| Vila Camera | 65/11 | 16.9 | 9.2-27.5 |
| Camarazinho | 17/40 | 23.5 | 7.9-47.5 |
| Katua | 11/80 | 72.7 | 42.2-92.5 |
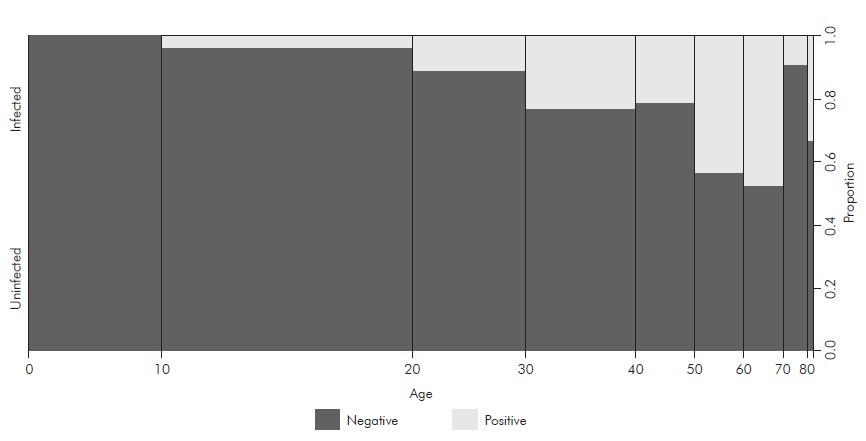
Figure 2 - Parasitized and non-parasitized individuals, according to age, in the Municipalities of Codajás and Coari, Amazonas State, Brazil
Table 2 - Factorial analysis of covariance for M. ozzardi prevalence in communities along the Solimões river in Codajás and Coari, Amazonas State, Brazil
| Variable | Level | ANOVA | ||
|---|---|---|---|---|
| χ2 | Contrast* | p-value | ||
| Gender | Male | -4.93 | - | 0.02† |
| Female | ||||
| Farmer/fishermen | a | |||
| Occupation | Retired | -61.37 | b | < 0.001† |
| Others | c | |||
| Student | d | |||
| Age | -11.51 | - | < 0.001† | |
| Gender: age | 0.13 | - | 0.71 | |
| Gender: occupation | -3.44 | - | 0.75 | |
| Age: occupation | -6.34 | - | 0.50 | |
*Different letters indicates statistical difference (p < 0.05); † Statistical difference (p < 0.05).
In Codajas, the general prevalence of mansonelliasis was 9.4% (23/245), and filaria-infected individuals were found in six of seven communities examined. The initial surveys for filariasis in Codajas had been conducted by Lacerda and Rachou3 and it was found microfilariae present in 23.9% of the examined individuals. Later surveys found filarial infection rates of 56.7%, 41.4%, and 45.9%, respectively, as determined by simultaneous diagnoses using thick blood smears and Knott methods12,13,14. Occasional cases of filariasis were reported by local health services during malaria surveys. The prevalence of filariasis in the Municipality of Coari was 22% (28/127), and microfilariae-infected individuals were also found in all the communities examined. M. ozzardt has been reported to be endemic in Coari since the first records3. Those records showed prevalences ranging from 10% to 17.8%; however, the most recent reports show microfilaremia prevalences of 18.9%, 18.2%, and 26.4%6,8,9. The infection prevalences which have persisted over the years in Codajas, and more clearly in Coari, are directly related to the lack of policies for treatment of mansonelliasis. This neglect has permitted circulation of the parasite by black flies, which are vectors for M. ozzardi in Brazil. These flies are highly anthropophilic, and routinely live along rivers in Amazonas5,6. Some Amazonas’ municipalities have shown a constant infection rate throughout the years, while the rate has increased in other areas. For example, along the river Purus, increasing rates of microfilariae infection have been reported in the Municipality of Lábrea (4.4%, and 20.7%)15,16.
The higher prevalence of infection in men is directly related to their greater levels of participation in daily activities such as agriculture and fishing, which increase their exposure to black flies6,12,15. Additionally, older individuals who have always worked outside will have a greater cumulative exposure to microfilariae vectors, which can lead to greater rates of infection6. This profile of M. ozzardi commonly occurred in Amazonas, and reflects the daily lives and activities of people in the riverine population who constantly expose themselves to vector stings. Furthermore, there is also the risk of developing multiple filaria infections involving both male and female macrofilariae. Such infections can serve to maintain circulating populations of microfilariae, and thus the disease transmission cycle.
Our current data confirm that over the years, mansonelliasis has been perpetuated in Codajás and Coari due to the non-implementation of public policies regarding treatment. Beyond the present damage caused to the public health by that infection in the current population, there is also the possibility that filaria may expand their range of infection into non-endemic areas. Such expansion might be facilitated by the large number of workers who temporarily live in these Municipalities, and then return to their regions of origin where there is the presence of vectors.

