










Servicios Personalizados
Revista

Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Curriculum ScienTI
Curriculum ScienTI Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO
Links relacionados
-
 Similares en
SciELO
Similares en
SciELO
Compartir

 Permalink
PermalinkRevista Pan-Amazônica de Saúde
versión impresa ISSN 2176-6215versión On-line ISSN 2176-6223
Rev Pan-Amaz Saude vol.11 Ananindeua 2020 Epub 24-Sep-2020
http://dx.doi.org/10.5123/s2176-6223202000378
ORIGINAL ARTICLE
Seroepidemiological study of measles in populations living in the metropolitan region of Belém, Pará State, Brazil, 2016 to 2018
1 Instituto Evandro Chagas/SVS/MS, Ananindeua, Pará, Brasil
OBJECTIVE:
To investigate the seroprevalence of antibodies against measles in young adults living in Belém and Ananindeua, Pará State, Brazil, in order to identify susceptible individuals.
MATERIALS AND METHODS:
Cross-sectional study by conglomerate, from 2,220 individuals (1,109 from Belém and 1,111 from Ananindeua), aged between 15 to 39 years old, being volunteers from schools, colleges, universities, research institutes, and barracks. Data were collected through an epidemiological questionnaire and entered using Epi-Info™ v7.0. The binomial test was used to analyze two proportions using BioEstat v5.3, significance level p < 0.05.
RESULTS:
The general susceptibility to measles was 17.2%, with 16.4% in Belém and 18.0% in Ananindeua, which was higher in males, with a wide geographical distribution. There was a significant difference in seropositivity in relation to the types of vaccine administered, with the triple viral vaccine (measles, mumps, rubella) reaching the highest percentages, as well as the comparison of information between self-reported and proven ones. Number of doses did not show significance in soropositivity when comparing individuals who referred one dose and the ones reporting three doses of measles vaccine. A decline in antibody levels over time (20 years) after the last vaccination was detected.
CONCLUSION:
There are groups of susceptible people forming pockets of vulnerable people in both municipalities, highlighting the need to strengthen epidemiological surveillance and vaccination strategies, in view of the reintroduction of the virus, in order to control the disease in Brazil.
Keywords: Measles; Vaccine; Disease Eradication; Seroepidemiological Studies
INTRODUCTION
Measles is a contagious exanthematic disease, caused by the measles virus, Measles morbillivirus (family Paramyxoviridae, genus Morbillivirus, mononegavirales order), with universal distribution. Transmission occurs directly, by means of nasophageous secretions expelled when coughing, sneezing, talking or breathing, by dispersion of aerosols with viral particles in the air in closed environments. It presents a clinical picture of hyperthermia, maculopapular rash usually associated with cough, coryza, conjunctivitis and Koplik spots in the oral mucosa, after prodromal symptoms of two to four days, and may evolve with severe complications. There is no specific treatment, vaccination is the best way of prevention1,2.
In Brazil, the measles virus stopped circulating in 2001, with records of imported cases from other countries in the Americas and other continents, mainly from Africa, and genotypes D4, D8 and B33 were identified.
The recommendation to maintain high levels of immunity in order to stop the chain of measles transmission is to maintain the homogeneity of vaccination coverage (VC) of 95%. The Brazilian Ministry of Health (MS) recommends the use of the triple viral vaccine (MMR: measles, mumps and rubella) at 12 months of age, first dose (D1) and between 15 months and 4 years of age, a dose of tetra viral (MMRV: measles mumps, rubella and chickenpox), which corresponds to the second dose (D2) of the vaccine. Sand the person did not receive the vaccine properly and is between 5 and 29 years of age, should perform two doses of MMR, with an interval of 30 days; and if you are between 30 and 49 years of age, only one dose of MMR4. Even with an appropriate immunization program, the accumulation of susceptible cases may occur after a few years, due to the vaccine shows no seroconversion or it may not be long-lasting, characterizing primary vaccine failures (PVF) and secondary vaccine failures (FVS), respectively5.
In 2010, there were three confirmed cases of measles in Belém, Pará State, in students aged between 18 and 26 years, with no immunization record, with identification of the viral genotype D46. From 2013 to 2015, Brazil faced an epidemic with laboratory-confirmed cases in several states, with greater frequency in the states of Pernambuco and Ceará. There were 220 cases recorded in eight states in 2013, 876 in four states in 2014 and 214 in three states in 20157 , due to the circulation of genotype D8, the same case detected in Latin America and the Caribbean (2010-2015)7. Those cases stopped due to the constant immunization and surveillance, and no case was recorded after 12 months. In September 2016, the World Health Organization (WHO) certified the measles elimination in Brazil8.
Global strategies for the measles elimination have avoided approximately 21.1 million deaths. In 2017, the WHO reported the occurrence of 6.7 million cases and 110,000 deaths worldwide9. However, due to the low VC, in 2018 there were cases in all of the world, with 328.689 cases confirmed in Europea, 84,468; Southeast Asia, 83,647; Africa, 55,394; Eastern Mediterranean, 57,960; Western Pacific, 30,531; and The Americas, 16,689 cases10.11.
In February 2018, Brazil recorded outbreaks that started in the state of Roraima, with 12 deaths reported. Four cases in Roraima, in children under 5 years of age (one Brazilian, two Venezuelan and one Korean); six cases in the state of Amazonas, four of them under 1 year of age, one in the age group of 40-49 years and one in over 50 years of age; and two reported in Pará, in the city of Belém, corresponding to Venezuelans/indigenous people under 1 year of age12. Venezuela had been facing a measles outbreak since July 2017, with the majority of cases coming from the state of Bolivar. Due to the sociopolitical economic situation that the country faced, there was an intense migratory movement that contributed to spread the virus to other geographical areas12.
Also in 2018, Brazil had measles outbreaks in 10 states and the Federal District, confirming a total of 10.326 cases, with higher occurrence in Amazonas and Roraima, with 9.803 and 361 cases, respectively. They also confirmed cases in the states of Pará (79), Rio Grande do Sul (46), Rio de Janeiro (20), Sergipe (four), Pernambuco (four), São Paulo (three), Bahia (three), Rondônia (two); and the Federal District (one). The genotypes detected were D8 from Venezuela and Lebanon and B3 from Europe12,13.
The incidence rate of confirmed cases in the Amazon region from 2018 to 2019, was 273.1/100,000 inhabitants with those under 1 year of age, and those aged 20-29 years with the highest incidences, 2,191.8 and 358.6, respectively. In Roraima the rate was 81.3/100.00 inhabitants, with a higher incidence in children under 1 year of age, with 841.8/100.00 inhabitants, and in children aged 1 to 4 years, with 255.8/100,000 inhabitants. Pará had a general incidence of 1.3/100.000 inhabitants, higher incidence in children under 1 year of age, with 15.0/100.000 inhabitants. Vaccination campaigns were carried out to increase VC, the goal was to vaccinate at least 95% of children at the age of 1 to 5 years13.
WHO warned Brazil of the necessity to contain cases in less than 12 months; however, Amazonas and Pará continued to confirm cases, which caused Brazil to lose the status of measles-free country in 201913.
In 2019, Brazil reported 64,765 suspected cases of measles, of which 18,203 (28.1%) confirmed in 23 Federation Units. The majority occurred in the state of São Paulo, which recorded 16,090 (88.4%) confirmed cases in 259 municipalities, followed by the states of Paraná (760; 4.2%), Rio de Janeiro (333; 1.8%), Pernambuco (268; 1.5%), Santa Catarina (251; 1.4%), Minas Gerais (135; 0.7%) and Pará (118; 0.6%). In the same year, 15 deaths were confirmed, six (40.0%) occurred in children under 1 year of age; two (13.3%) in children aged one 1; and seven (46.7%) in adults over 20 years of age. Of the 15 deaths, two people were vaccinated against measles14.
The study by Pacheco et al.15, 2019, described the risk of restoring endemic transmission of measles in Brazil and found that, at national level, the VC of D1 of the MMR vaccine has decreased since 2014, not reaching the goal established by the MH; and the same occurred with the D2 of MMR, which has not reached the its target since 2013. At the regional level, reductions were also found, and the lowest VC for D1 and D2 was also observed in the Northern Region. According to the Brazilian Health Informatics Department (DATASUS) of the MH, Belém and Ananindeua presented VC below that recommended for both D1 and D2. In 2016, Belém showed D1 of 77.0% and D2 of 72.0%; in 2017, D1 of 65.8% and D2 of 42.4%; and, in 2018, D1 of 75.1% and D2 of 55.2%. In 2016, Ananindeua showed D1 of 34.0% and D2 of 29.8%; in 2017, D1 of 52.6% and D2 of 57.9%; and, in 2018, D1 of 56.7% and D2 of 42.1%16 Measles continues to spread in global outbreaks, with 568,573 confirmed cases recorded in 2019; and, in August 2020, 77,673 casos were confirmed in all WHO regions17. The currently circulating genotypes of the measles virus are B3 and D818.
Seroprevalence studies guide epidemiological surveillance in the application of prophylactic and control measures in the susceptible population, thus contributing to public health in to regain the certification for measles elimination in Brazil.
In this context, the panorama of susceptibility to measles virus in populations of two municipalities in the metropolitan area of Belém was investigated in a population of individuals born from 1978 to 2002.
MATERIALS AND METHODS
This is a cross-sectional study in individuals aged from 15 to 39 years, both genders, apparently healthy, randomly selected and by groups in schools, colleges, universities, barracks and research institute of two municipalities in the Metropolitan Region of Belém. They had been selected because they are the most populous place in Pará with VC below that recommended by the MH16.
The sample size was calculated considering it was a stratified sampling by age. The StatCalc software was used in the Epi Info program™ v7.0, and maximum number of estimable parameters (80%), confidence limit (5%), confidence level (95%) and adjustment by design effect (deff = 1.5), in order to control confounding variables, as well as loss of power of the statistical test used. For the calculation the following formula was used n = [EDFF*Np(1-p)] / [(d2/Z21-α/2*(N-1)+p*(1-p)], and the total result was 2,210, 1,107 for Belém and 1,103 for Ananindeua. This sampling was calculated to detect the statistically significant differences considered from the α level of 5% and CI of 95%, considering possible losses in the selection process.
A total of 2,220 participants were selected for the study, 1,109 from Belém and 1,111 from Ananindeua, with samples collected from April 2016 to September 2018. The following inclusion criteria were: belonging to the age group from 15 to 39 years and living in the selected municipalities, regardless of the immunization record or natural history of disease.
The studied places in Belém were: Public Middle and High School (EEEFM) Professor Jorge Lopes Raposo (Icoaraci), EEEFM do Outeiro (Outeiro), EEEFM Abelardo Leão Condurú (Mosqueiro), Instituto Federal do Pará, Faculdades Integradas da Amazônia, Faculdade Maurício de Nassau, Universidade Estadual do Pará, Escola Superior da Amazônia, Comando Militar do Norte, Corpo de Bombeiros de Belém and Instituto Evandro Chagas (campi Belém and Ananindeua). In Ananindeua: EEEFM Antônio Goldim Lins, EEEFM Antônio Teixeira Gueiros, EEEFM Erotides Frota Aguiar, Faculdade da Amazônia, Instituto Federal do Pará campus Ananindeua, Sistema de Ensino da Amazônia, Universidade Federal do Pará campus Ananindeua and Corpo de Bombeiros de Ananindeua.
Those who agreed to participate had to sign the Informed Consent Form; and, in the cases of minors under 18 years of age, an Informed Consent Form was signed by both participant and guardian. The participants answered a questionnaire applied by eight trained field researchers, aiming at greater familiarity and uniformity in the information. The questionnaires were typed using Epi Info™ v7.0.
Data were collected such as: name; age; gender; municipality of origin; address immunization record (vaccination status, types of vaccine and number of doses) based on the vaccination card or, if it is lost, based on reports of the participant or her/his mother/guardian; in case of an unvaccinated person, the justification; records of disease occurrence; and two questions to verify whether they knew the mode of transmission and the mode of measles prevention. The patient's knowledge was computed as "partially" in case they knew how to answer only one question.
According to their address, it was decided to map the distribution of participants by administrative districts of Belém and Ananindeua districts. Belém has eight administrative districts19 and Ananindeua has 22 urban and nine rural districts20.
The qualitative research of IgG antibodies was carried out by the ELISA method (Enzygnost Anti-Measles Virus/IgG), using commercial kits (SIEMENS®,Marburg, Germany), according to the manufacturer's instructions. The quantification of IgG antibodies was expressed in international units (mIU/mL) by calculating the α, according to the manufacturer's instructions. Those values considered reactive values were IgG titers > 350 mIU/mL, non-reactive values were titers < 150 mIU/mL and inconclusive levels between 150-350 mIU/mL. Non-reactive (IgG-) and inconclusive were considered susceptible, and those with reactivity (IgG+) were considered immune. Serum samples with inconclusive results were submitted to a new test in order to confirm the result.
For statistical analysis, the binomial test was used for a proportion of the BioEstat v5.3 program, establishing a significance level with p< 0.05, as well as the Microsoft Excel 2013 program for graphical representation, and Arc GIS v10.2 software for map generation.
The study was approved by the Research Ethics Committee of the IEC, under approval opinion No. 2556024 CAAE 46849515800000019, ensuring the privacy of information and the anonymity of the participants in the study, as established by Ordinance No. 466/2012, of the National Research Council21.
RESULTS
Among the 2,220 participants, 49.9% (1,109/2,220) lived in Belém and 50.1% (1,111/2,220) in Ananindeua. The average age was 21 years, median 23 years and standard deviation was 1.3. The frequency of female participants was 66.8% (1,482/2,220). In Belém, 49.1% (545/1,109) of the participants were between 20 and 29 years old and, in Ananindeua, 52.4% (582/1,111) were between 15 and 19 years of age (Table 1).
Table 1 - Profile of participants, according to gender, age group, immunization record, occurrence of disease and participant's knowledge about measles, Belém and Ananindeua, Pará State, Brazil, 2016 to 2018
| Variables | Total | Locations | p-value* | ||||
|---|---|---|---|---|---|---|---|
| Belém | Ananindeua | ||||||
| N | % | N | % | N | % | ||
| Sex | |||||||
| Male | 738 | 33,2 | 363 | 32,7 | 375 | 33,8 | 0,6415 |
| Female | 1.482 | 66,8 | 746 | 67,3 | 736 | 66,2 | |
| Age group (years) | |||||||
| 15-19 | 908 | 40,9 | 326 | 29,4 | 582 | 52,4 | <0,0001 |
| 20-29 | 884 | 39,8 | 545 | 49,1 | 339 | 30,5 | |
| 30-39 | 428 | 19,3 | 238 | 21,5 | 190 | 17,1 | |
| Vaccination status | |||||||
| Vaccinated | 1.615 | 72,7 | 795 | 71,7 | 820 | 73,8 | 0,5136 |
| Not vaccinated | 37 | 1,7 | 20 | 1,8 | 17 | 1,5 | |
| Unable to give further information | 568 | 25,6 | 294 | 26,5 | 274 | 24,7 | |
| Vaccination card | |||||||
| Yes | 695 | 31,3 | 329 | 29,7 | 366 | 32,9 | 0,1055 |
| No | 1.525 | 68,7 | 780 | 70,3 | 745 | 67,1 | |
| Types of vaccine and their administration | |||||||
| Measles Vaccine (M-Vac) | 132 | 8,2 | 67 | 8,4 | 65 | 7,9 | <0,0001 |
| Double viral vaccine (MR) | 65 | 4,0 | 22 | 2,8 | 43 | 5,2 | |
| Triple viral vaccine (MMR) | 163 | 10,1 | 44 | 5,5 | 119 | 14,5 | |
| M-Vac +MR | 413 | 25,5 | 257 | 32,3 | 156 | 19,0 | |
| M-Vac +MMR | 58 | 3,6 | 38 | 4,8 | 20 | 2,5 | |
| MR+MMR | 90 | 5,6 | 33 | 4,2 | 57 | 7,0 | |
| M-Vac +MR+MMR | 68 | 4,2 | 49 | 6,2 | 19 | 2,3 | |
| Unable to give further information | 626 | 38,8 | 285 | 35,8 | 341 | 41,6 | |
| Number of doses | |||||||
| One | 158 | 9,8 | 75 | 9,4 | 83 | 10,1 | 0,0004 |
| Two | 415 | 25,7 | 205 | 25,8 | 210 | 25,6 | |
| Three or more | 424 | 26,2 | 243 | 30,6 | 181 | 22,1 | |
| Unable to give further information | 618 | 38,3 | 272 | 34,2 | 346 | 42,2 | |
| Justification for not vaccinating | |||||||
| Lack of vaccines | 2 | 5,4 | 1 | 5,0 | 1 | 5,9 | 0,2799 |
| Ignorance about vaccines | 12 | 32,4 | 6 | 30,0 | 6 | 35,3 | |
| Other reasons | 19 | 51,4 | 9 | 45,0 | 10 | 58,8 | |
| Unable to give further information | 4 | 10,8 | 4 | 20,0 | - | - | |
| Occurrence of measles | |||||||
| Yes | 145 | 6,5 | 91 | 8,2 | 54 | 4,9 | 0,0004 |
| No | 1.758 | 79,2 | 843 | 76,0 | 915 | 82,3 | |
| Unable to give further information | 317 | 14,3 | 175 | 15,8 | 142 | 12,8 | |
| Knowledge about measles | |||||||
| Yes | 851 | 38,3 | 486 | 43,8 | 365 | 32,8 | <0,0001 |
| No | 868 | 39,1 | 355 | 32,0 | 513 | 46,2 | |
| Partially | 501 | 22,6 | 268 | 24,2 | 233 | 21,0 | |
* Binomial test for a proportion; Conventional signal used: - Numerical data equal to zero, not resulting from rounding.
Regarding the immunization records for measles, 72.7% (1,615/2,220) of participants reported having received the vaccine; however, only 31.3% (695/2,220) had the vaccination card. Of the total number of self-reported vaccination, 38.8% (626/1,615) and 38.3% (618/1,615) did not know the type of vaccine and the number of doses, respectively (Table 1). The lack of the vaccination card due to its loss, to prove the vaccination status of the participants, represents a limiting factor in seroepidemiological studies of vaccine-preventable diseases.
Among the justifications declared by unvaccinated individuals, 32.4% (12/37) stated ignorance of the vaccine, 5.4% (2/37) lack of vaccines and 51.4% (19/37) other reasons, such as living in an area of difficult access, the guardian forgot about the immunization day, vaccine hesitancy, lack of knowledge about the benefits of the vaccines and fear of adverse reactions. Of the total number of participants, 39.1% (868/2,220) reported not knowing the mode of transmission and prevention of measles; and 6.5% (145/2,220) reported having already contracted measles (Table 1), of which 58.6% (85/145) were aged 30 to 39 years.
The overall frequency of immune (reactive) individuals for measles in the IgG ELISA test was 82.8% (1,838/2,220) and 17.2% (382/2,220) susceptible, and 10.2% were non-reactive and 7.0% inconclusive (Table 2). Seropositivity was 83.6% in Belém and 82% in Ananindeua, both municipalities showed statistically significant differences (p < 0.05) in relation to the percentage of VC recommended by the MH. In the age stratification, the proportion of susceptible adolescents aged 15 to 19 years was 22.4% and 21.0% in Belém and Ananindeua, respectively (Table 2).
Table 2 - Frequencies of immune and susceptible individuals to measles in the population studied by the research of specific IgG antibodies, by age group, in the municipalities of Belém and Ananindeua, Pará State, Brazil, 2016 to 2018
| BELÉM | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age group (years) | Total | % | Immune | % | IC 95% | Susceptible* | % | IC 95% | p-† |
| 15-19 | 326 | 29,4 | 253 | 77,6 | 75,2-79,6 | 73 | 22,4 | 20,0-24,4 | p < 0,05 |
| 20-29 | 545 | 49,1 | 457 | 83,9 | 81,6-85,7 | 88 | 16,1 | 14,1-18,0 | p < 0,05 |
| 30-39 | 238 | 21,5 | 217 | 91,2 | 89,5-92,5 | 21 | 8,8 | 7,2-10,2 | p < 0,05 |
| Total | 1.109 | 100,0 | 927 | 83,6 | 81,4-85,4 | 182 | 16,4 | 14,3-18,2 | p < 0,05 |
| ANANINDEUA | |||||||||
| Age group (years) | Total | % | Immune | % | IC 95% | Susceptible* | % | IC 95% | p-† |
| 15-19 | 582 | 52,4 | 460 | 79,0 | 76,5-80,9 | 122 | 21,0 | 18,6-23,0 | p < 0,05 |
| 20-29 | 339 | 30,5 | 279 | 82,3 | 80,0-84,2 | 60 | 17,7 | 15,1-19,2 | p < 0,05 |
| 30-39 | 190 | 17,1 | 172 | 90,5 | 88,8-91,9 | 18 | 9,5 | 7,8-11,0 | p < 0,05 |
| Total | 1.111 | 100,0 | 911 | 82,0 | 79,7-83,9 | 200 | 18,0 | 15,8-19,9 | p < 0,05 |
| Overall total | 2.220 | 100,0 | 1.838 | 82,8 | 81,3-84,1 | 382 | 17,2 | 15,6-18,5 | p < 0,05 |
* Sum of negatives and inconclusive cases in the ELISA test; † Binomial test for proportion.
Female participants presented 84.2% reactivity and males 80.0%, with statistically significant difference (binominal test, z = 0.51, p = 0.0061) (Figure 1). The participants from Belém came from eight administrative districts of Mosqueiro Administrative District (DAMOS), Outeiro Administrative District (DAOUT), Icoaraci Administrative District (DAICO), Benguí Administrative District (DABEN), Entroncamento Administrative District (DAENT), Sacramenta Administrative District (DASAC), Belém Administrative District (DABEL) and Guamá Administrative District (DAGUA). From Ananindeua, the participants belonged to 15 districts: Centro, Águas Brancas, Águas Lindas, Coqueiro, Distrito Industrial, Maguari, 40 Horas, Atalaia, Conjunto Guajará I, Guanabara, Icuí-Guajará, Jaderlândia, Heliolândia, Curuçamba and PAAR.
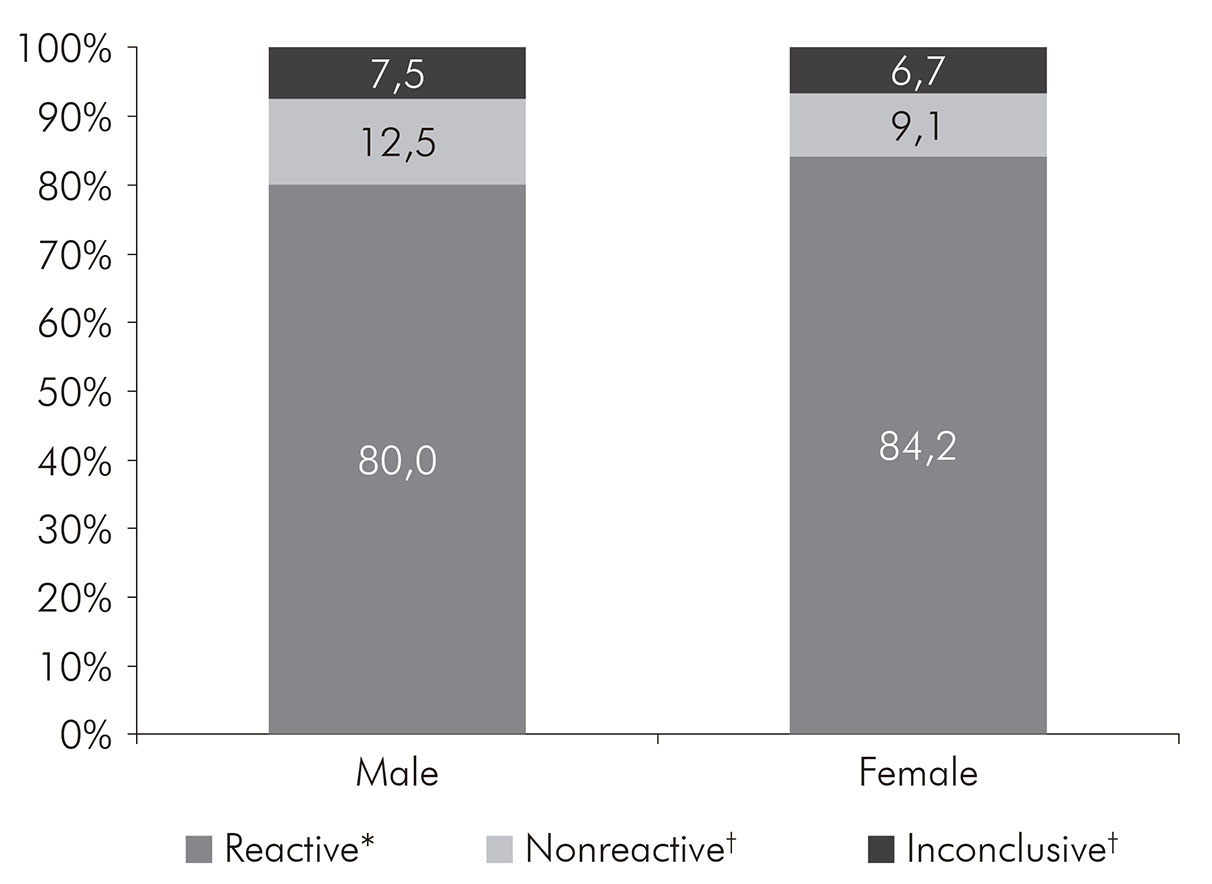
z = 0.51, p = 0.0061; * Immune; † Susceptible.
Figure 1 - Prevalence of IgG antimeasles antibodies, according to gender in the population studied in the municipalities of Belém and Ananindeua, Pará State, Brazil, 2016 to 2018
The mapping of individuals susceptible to measles, among the eight administrative districts of Belém, revealed that six (75.0%) districts had statistically significant frequencies (p > 0.0001): DAGUA (20.0%), DABEL (19.0%), DAICO (14.0%), DABEN (13.0%), DASAC (12.0%) and DAENT (16.0%). In Ananindeua, seven (46.7%) districts presented significant susceptible percentages (p > 0.0001) in relation to the measles virus: Coqueiro (22.0%); Distrito (16.0%); Águas Lindas (15.0%); Maguari (12.0%); Águas Brancas (12.0%); Centro (9.0%) and Icuí-Guajará (6.0%) (Figure 2).
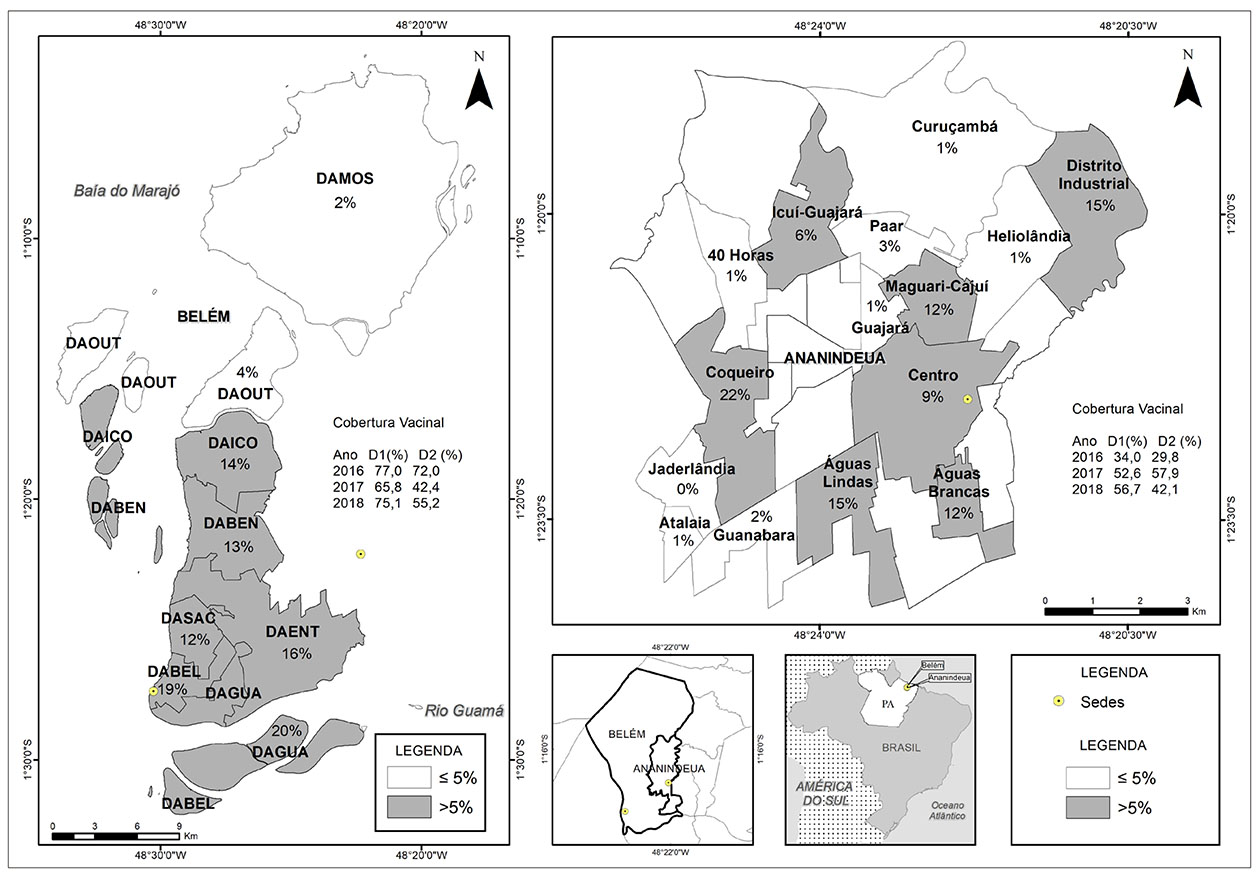
Font: LABGEO/IEC/SVS/MS.
DAMOS: Mosqueiro Administrative District; DAOUT: Outeiro Administrative District; DAICO: Icoaraci Administrative District; DABEN: Benguí Administrative District; DAENT: Entroncamento Administrative District ; DASAC: Sacramenta Administrative District; DABEL: Belém Administrative District; DAGUA: Guamá Administrative District; D1: First dose of measles vaccine; D2: Second dose of measles vaccine.
Figure 2 - Mapping of measles-susceptible participants distributed in administrative districts of Belém and Ananindeua, Pará State, Brazil, 2016 to 2018
The frequencies of immune and susceptible individuals, according to the immunization record related to the type of vaccine and its combinations can be seen in Figure 3. To evaluate the impact of possible lapses in self-reported vaccination, the frequencies of immune and susceptible individuals were analyzed according to self-reference (Figure 3A) and also according to the vaccination card (Figure 3B). In the analyses, part of the self-reported vaccinated patients was considered, as well as part of the vaccinated patients with vaccination card, since not every self-reference of vaccination knew about the type of vaccine, and not every vaccination card had this legible information. The difference of immune individuals who received single and combined M-Vac with two (double viral - MR) and three components (MMR) presented test G = 6.1677, p = 0.4491, for self-reported vaccinated patients and x2 = 27.666, p = 0.001, for those with vaccination card. Comparing the two analyses, test G = 2.4443, p < 0.0001 was found.

A: Information based on self-references; B: Vaccine information from the vaccination card. M-Vac: Measles vaccine - monovalent; MR: Measles and rubella - double viral; MMR: Measles, mumps and rubella - triple viral. G = 244.43, p < 0.0001.
Figure 3 - Frequency of immune and susceptible to measles, according to the types of vaccines received by participants, in Belém and Ananindeua, Pará State, Brazil, 2016 to 2018
In relation to the number of doses of vaccine received, the levels of measles-specific IgG antibodies were analyzed only in the participants who showed the vaccination card, excluding those who reported having contracted the disease. Of the 521 analyzed people, 14.0% (73/521) had received only one dose of M-Vac; 32.8% (171/521), two doses; and 53.2% (277/521), three doses or more. The proportion test for two independent samples showed that the odds ratio (OR) for the antibody reagent titer was similar among participants who received a dose of the vaccine vs. three doses, OR = 1.70 (95% CI 0.70-3.78); p = 0.2538) and also for those who received two doses of the vaccine vs. three doses, OR = 0.79 (95% CI 0.48-1.27; p = 0.3917), as well as for those who received a dose vs. two doses, OR = 2.17 (95% CI 0.95-4.92; p = 0.0899) (Table 3).
Table 3 - IgG antibody title by ELISA/Enzygnost Anti-Measles Virus/IgG, according to the number of doses of measles vaccine and the comparative analysis between the number of doses, among participants from Belém and Ananindeua, Pará State, Brazil, 2016 to 2018
| Measles as component of vaccine | Titles (mIU/mL) | ||
|---|---|---|---|
| Number of doses | > 350* | 150-350† | < 150‡ |
| One (73) | 65 (89,0%) | 4 (5,5%) | 4 (5,5%) |
| Two (171) | 135 (78,9%) | 15 (8,8%) | 21 (12,3%) |
| Three or more (277) | 229 (82,7%) | 21 (7,6%) | 27 (9,7%) |
| Total (521) | 429 (82,3%) | 40 (7,7%) | 52 (10,0%) |
| Comparison between number of doses | Odds ratio | IC 95% | p-value |
| One dose x three doses | 1,70 | 0,70-3,78 | 0,2538 |
| Two doses x three doses | 0,79 | 0,48-1,27 | 0,3917 |
| One dose x two doses | 2,17 | 0,95-4,92 | 0,0899 |
* Reactive; † Indeterminate; ‡ Nonreactive.
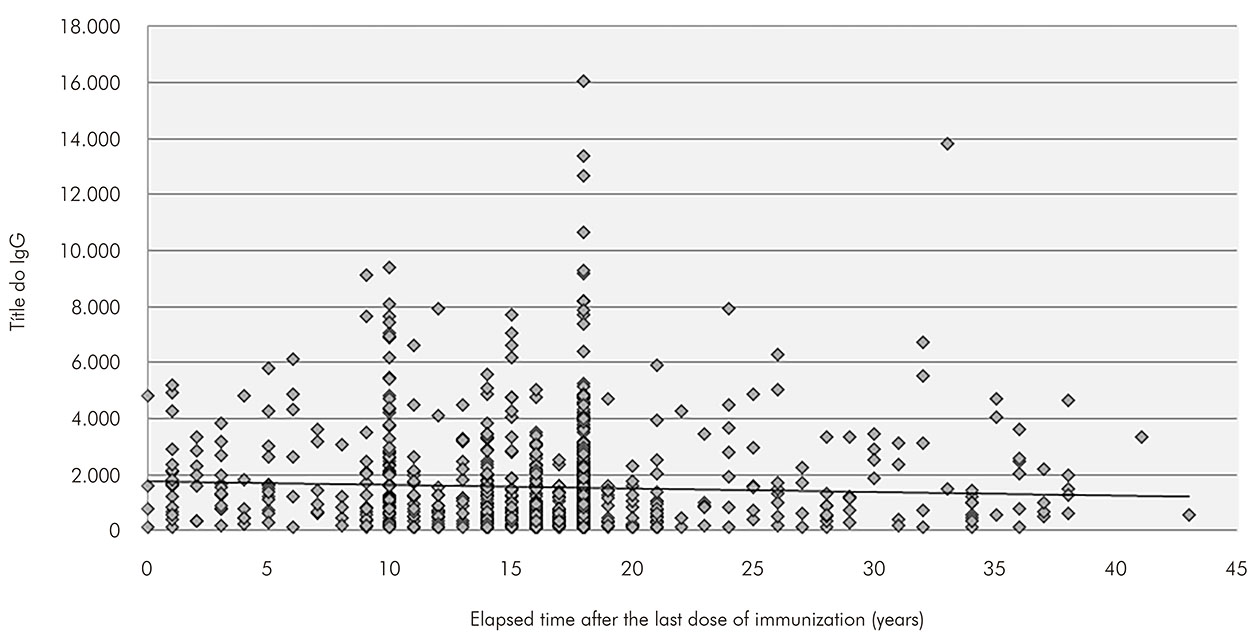
In order to verify a possible association between antibody titers for measles and post-vaccination time, Spearman correlation analysis was used, considering the time in years elapsed after the last dose of the vaccine self-reported and proven by vaccination by each participant, resulting in rs = -0.0897; t = -28721; p = 0.004 (Figure 4).
DISCUSSION
This is a pioneer article in the Pará State, with a seroepidemiological analysis of measles reporting the seroprevalence and epidemiological profile of a population that experienced the epidemic period and the process of changes in the immunization program, aiming at the elimination of measles, with the implementation of MR and MMR vaccines from the year 2000.
The general frequency of immune individuals, as well as in all age groups of the current study, was below 95% recommended by the MS of Brazil. This fact demonstrates that part of the population may not have received reinforcement, according to the guidance of MH. Estofolete et al.22, when describing the seroprevalence for measles in individuals over 10 years of age in São José de Rio Preto, in the state of São Paulo, they had found similar percentages (84.2%) in the population aged 10 to 40 years.
The overall susceptibility was 17.2% for the measles virus in Belém and Ananindeua; the highest frequencies of susceptibility were detected among participants aged from 15 to 29 years, a fact that occurs due to the absence of the second dose of the vaccine, PFV or SVF. All age groups in the current study, in both municipalities, showed statistically significant differences in relation to the percentage of susceptible individuals admitted by the MH, demonstrating that there is a risk of measles outbreaks, due to the concentration of susceptible patients over the years with the virus importation that started circulating in the country. These results were higher than that found by Sampaio et al. 23, when they studied the prevalence of antibodies against measles among vaccinated students from schools and universities in the city of São Paulo, with 3.2%.
According to information from the National Immunization Program, the VC for measles in Pará was 79.5% from 1998 to 2018, After the implementation of MR and MMR vaccines between 2000 and 2003, a VC of 118.6% was recorded (according to values published by the DATASUS system), declining to 62.1% in 2003; from 2004 , reached the goal set by the MS (95%) by the year 2012. From 2013 to 2018, VC declined again reaching 53.2% in 201816.
After declaration of the measles elimination, there was a lack of MR and MMR vaccines in health centers, in addition to reducing vaccination campaigns, with little dissemination. Anti-vaccine movements have grown worldwide, including in Brazil, which has always been an international example of immunization programs, causing a decrease in vaccination and end up increasing outbreaks and epidemics of vaccine-preventable diseases, such as measles24.
Males were more susceptible to measles than females, results similar to the findings of Poethko-Müller and Mankertz25 in Germany. This may have occurred due to vaccination campaigns, which happened during the implementation of MR and MMR, initially contemplated by women of childbearing age, with the objective of avoiding rubella among pregnant women26. It was also observed a lower percentage of male participants in the study, both in Belém and Ananindeua, a different result to the study conducted by Tafuri et al.27, when analyzing the monitoring of the measles elimination process in Apulian, Italy. According to the authors, lower support may have been influenced by the aversion to invasive procedures manifested by men during the blood tests27.
The geographic distribution of susceptible individuals was revealed by the evidence of these individuals in six administrative districts of Belém and in seven districts of Ananindeua, including with significant susceptibility frequencies in many of them. When verifying the VC of 2018, Belém recorded 65.2% and Ananindeua 49.4%, demonstrating a low percentage, thus creating pockets of susceptibles at risk of contracting the disease, mainly due to population migration to the north of the country16.
Analyzing the frequencies of immune and susceptible to measles among the types of vaccines administered (M-Vac, MR and MMR) in information based on self-references, no significant difference was found; however, among those who presented the vaccination card, this difference was found. Regarding the type of vaccine administered, when comparing the information of the vaccinated patients proven by the vaccination card with the information based on self-references, a significant difference was detected, suggesting that any lapses in the reports about the type of vaccine were impacting. The M-Vac vaccine showed a higher frequency of positivity, then it is the most used since its implantation. Santos et al.28 showed that the immunogenicity and reactogenicity of the combined vaccine are similar to the single measles antigen vaccine. Rivière et al.29, when assessing the economic benefits of a combined vaccine vaccination program in Canada, concluded a considerable cost savings.
The presence of susceptible individuals in those mentioned groups, especially among those vaccinated with vaccination card, evidences the occurrence of vaccine failure. The accumulation of susceptible cases causes the emergence of outbreaks, which is the reason why the appropriate conditions of the cold chain, the correct handling and the vaccine administration are important in order to mitigate PFV and SVF30.
Comparing the titers of antibodies against measles of those confirmed by the vaccination card, it was observed that the inconclusive and nonreactive groups that received D2 is a worrying situation which can be explained by the occurrence of PFV and SVF in the administration of this dose or by the rapid loss of antibodies. Similar findings have been reported by Kang al.31 when studying a vaccinated population in Korea.
Measles immunoglobulin G (IgG) antibodies levels in relation to the number of vaccine doses received showed that the odds ratio (OR) for positive antibody titer was not significant among participants who received single doses, compared to two or three doses. These results show that to achieve immunity, a dose of the vaccine may be sufficient; however, according to the Centers for Disease Control and Prevention (CDC) report32, a dose of the MMR vaccine has about 93.0% effectiveness for measles, and two doses or more, 97.0%. By comparing the data of this study with those of the CDC report and those of the study by Ogawa et al.33, which evaluated the immunization record in medical and nursing students, this study was low level of immunity; however, the results among the number of doses were similar. Lievano et al.34 detected 8% of people without classic symptoms with serological evidence of measles infection. Part of the population of the present study experienced the epidemic period of measles before elimination.
The correlation between the titer of IgG antibodies against measles and the time elapsed after the last vaccination showed a weak negative association, revealing a reduction in antibody levels over time, about 20 years after the last vaccination, confirming the decrease in vaccine-induced immunity. Similar findings have been reported by Smetana et al.35 in the Czech Republic, with a reduction in antibodies around 30 to 39 years after the last vaccination. These results demonstrate that individuals who have been immunized in childhood or adolescence may become susceptible as adults and, in the case of women, may transfer low levels of maternal antibodies to their children, proving the need to comply with the recommendations of the MH about D2 in order to correct possible vaccine failures36.
The diverse profile of vaccine types and measles vaccine regimens shows that this population has undergone changes during strategies in the MH vaccination program, with the implementation of the measles and rubella elimination plan. In Pará, in 2000, the first vaccination campaign with MR was carried out for the ages of 1 to 4 years and for women of childbearing age; and, in 2003, M-Vac was replaced by MMR, being administered at 12 months of age, as recommended by the MH37.
CONCLUSION
The study reveals significant susceptibility in the age group from 15 to 39 years, forming pockets of vulnerable, detecting a gap in protection against measles in adults after 20 years of the last vaccination. It may have been the cause of measles outbreaks in Belém and Ananindeua since 2018. It is clear the necessity to strengthen vaccination strategies and decision conducted by the State facing the virus reintroduction in order to control the disease in Brazil, regain the certification of the measles elimination in the country and the scope of its eradication. Serological surveillance is used to identify susceptible cases and revaccination when the absence of protective antibodies may be detected.
ACKNOWLEDGMENT
To the Evandro Chagas Institute and the technicians involved; Antônio Carlos Fernandes do Nascimento and Patrícia Sousa Moraes de Almeida, responsible for serological tests; Vanda do Socorro da Costa Siqueira and Aline Colares, for the application of the questionnaires; Clistenes Catete and Marcos Vulcão, for the elaboration of graphs and maps, Ângela Pereira, for linguistic correction; Emilene Monteiro Furtado Serra, Aurélia Maria Mendes Oliveira, Leda Mani França de Arruda, Raimunda do Socorro Pimentel, Idebê Caldas da Cruz and Rita Maria Felix de Oliveira, who worked in the collection of biological species.
REFERENCES
1 Laksono BM, Vries RD, McQuaid S, Duprex WP, Swart RL. Measles virus host invasion and pathogenesis. Viruses. 2016;8(8):210. Doi: 10.3390/v8080210 [Link] [ Links ]
2 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Coordenação-Geral de Desenvolvimento da Epidemiologia em Serviços. Guia de vigilância em saúde. Vol. 1. Brasília: Ministério da Saúde; 2017. p. 119-34. [Link] [ Links ]
3 Prevots DR, Parise MS, Segatto TCV, Siqueira MM, Santos ED, Ganter B, et al. Interruption of measles transmission in Brazil, 2000-2001. J Infect Dis. 2003 May;187 Suppl 1:S111-20. Doi: 10.1086/368030 [Link] [ Links ]
4 Ministério da Saúde (BR). Calendário nacional de vacinação [Internet]. Brasília: Ministério da Saúde ; 2013 [citado 2018 dez 12]. Disponível em: Disponível em: https://www.saude.gov.br/saude-de-a-z/vacinacao/calendario-vacinacao . [ Links ]
5 Mello JN, Haddad DAR, Câmara GNP, Carvalho MS, Abrahão NM, Procaci VR. Panorama atual do sarampo no mundo: risco de surtos nos grandes eventos no Brasil. J Bras Med. 2014 jan-fev;102(1):33-40. [Link] [ Links ]
6 Jesus HS, Nascimento GL, Rosa FM, Santos DA. Investigação de surto de sarampo no Estado do Pará na era da eliminação da doença no Brasil. Cad Saude Publica. 2015;31(10):2241-6. Doi: 10.1590/0102-311X00017515 [Link] [ Links ]
7 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Plano de contingência para resposta às emergências de saúde pública: sarampo. Brasília: Ministério da Saúde ; 2016. [Link] [ Links ]
8 Pan American Health Organization, World Health Organization. Region of the Americas is declared free or measles [Internet]. Washington: PAHO, WHO; 2016 [cited 2019 Sep 3]. Available from: Available from: https://www.paho.org/hq/index.php?option=com_content&view=article&id=12528:region-americas-declared-free-measles&Itemid=1926&lang=en . [ Links ]
9 World Health Organization. New measles surveillance data from WHO [Internet]. Geneva: World Health Organization; 2019 [cited 2019 Sep 11]. Available from: Available from: https://www.who.int/immunization/newsroom/new-measles-data-august-2019/en/ . [ Links ]
10 Centers for Disease Control and Prevention. Nationwide rubella epidemic - Japan, 2013. MMWR Morb Mortal Wkly Rep. 2013 Jun 14;62(23):457-86. [Link] [ Links ]
11 World Health Organization. Measles and rubella surveillance data. Reported measles and rubella cases and incidence rates by member states [Internet]. Geneva: World Health Organization ; 2020 [cited 2019 Sep 3]. Available from: Available from: who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/active/measles_monthlydata/en/ . [ Links ]
12 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Situação do sarampo no Brasil - 2018. Informe. 2018 nov;(32):1-9. [Link] [ Links ]
13 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Situação do sarampo no Brasil - 2018-2019. Informe. 2019 mar;(37):1-11. [Link] [ Links ]
14 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Vigilância epidemiológica do sarampo no Brasil 2019: janeiro a dezembro. Bol Epidemiol. 2020 mar;51(6). [Link] [ Links ]
15 Pacheco FC, França GVA, Elidio GA, Leal MB, Oliveira C, Guilhem DB. Measles-containing vaccines in Brazil: coverage, homogeneity of coverage and associations with contextual factors at municipal level. Vaccine. 2020 Feb;38(8):1881-7. Doi: 10.1016/j.vaccine.2020.01.030 [Link] [ Links ]
16 Ministério da Saúde (BR). Departamento de Informática do SUS. Imunizações - cobertura - Pará [Internet]. Brasília: Ministério da Saúde ; 2019 [citado 2018 dez 10]. Disponível em: Disponível em: http://tabnet.datasus. gov.br/cgi/deftohtm.exe?pni/CNV/CPNIPA.def . [ Links ]
17 Word Health Organization. Measles - global situation [Internet]. Geneva: World Health Organization ; 2019 [cited 2020 May 7]. Available from: Available from: https://www.who.int/csr/don/26-november-2019-measles-global_situation/en/ . [ Links ]
18 Fraser-bell CJ. Global re-emergence of measles - 2019 update. Glob Biosecur. 2019;1(3). Doi: 10.31646/gbio.43 [Link] [ Links ]
19 Prefeitura Municipal de Belém (PA). Anuário estatístico do município de Belém 2011. 16. ed. Belém: Secretaria Municipal de Coordenação Geral do Planejamento e Gestão; 2012. [Link] [ Links ]
20 Gusmão LHA. Mapas dos bairros de Ananindeua (serviço) [Internet]. 2017 dez [citado 2019 set 7]. Disponível em: Disponível em: http://geocartografiadigital.blogspot.com/2017/12/ . [ Links ]
21 Brasil. Ministério da Saúde. Comissão Nacional de Ética em Pesquisa. Resolução nº 466, de 12 de dezembro de 2012. Aprova diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos [Internet]. [Diário Oficial da União], Brasília (DF); 2012 [citado 2013 jun 3]. Disponível em: Disponível em: http://conselho.saude.gov.br/resolucoes/2012/Reso466.pdf . [ Links ]
22 Estofolete CF, Milhim BHGA, França CG, Silva GCD, Augusto MT, Terzian ACB, et al. Prevalence of measles antibodies in São José do Rio Preto, São Paulo, Brazil: a serological survey model. Sci Rep. 2020 Mar;10:5179. Doi: 10.1038/s41598-020-62151-3 [Link] [ Links ]
23 Sampaio BCF, Rodrigues JP, Meireles LR, Andrade Jr HF. Measles, rubella, mumps and Toxoplasma gondii antibodies in saliva of vaccinated students of schools and universities in São Paulo city, Brazil. Braz J Infect Dis. 2020 Feb;24(1):51-7. Doi: 10.1016/j.bjid.2019.11.005 [Link] [ Links ]
24 Sato APS. Qual a importância da hesitação vacinal na queda das coberturas vacinais no Brasil? Rev Saude Publica. 2018;52:96. Doi: 10.11606/S1518-8787.20180520011991 [Link] [ Links ]
25 Poethko-Müller C, Mankertz A. Seroprevalence of measles-, mumps- and rubella-specific IgG antibodies in German children and adolescents and predictors for seronegativity. PLoS One. 2012;7(8):e42867. Doi: 10.1371/journal.pone.0042867 [Link] [ Links ]
26 Moraes MM, Cruz ACR, Silva DFL, Sagica FES, Santos ECO. Trajetória da rubéola no Estado do Pará, Brasil: rumo à erradicação. Rev Pan-Amaz Saude. 2015;6(1):19-28. Doi: 10.5123/S2176-62232015000100003 [Link] [ Links ]
27 Tafuri S, Gallone MS, Gallone MF, Pappagallo MT, Larocca A, Germinario C. Monitoring the process of measles elimination by serosurveillance data: the apulian 2012 study. Vaccine. 2016 Apr;34(18):2092-5. Doi: 10.1016/j.vaccine.2016.03.011 [Link] [ Links ]
28 Santos EM, Martins R, Noronha T, Cruz R, Siqueira M, Pavão AL, et al. Estudo comparativo da imunogenicidade da vacina tríplice viral (sarampo, caxumba e rubéola) nas apresentações monodose e multidose, em lactentes. In: 6º Seminário Anual Científico e Tecnológico de Bio-Manguinhos; 2018; Rio de Janeiro, RJ. Anais... Rio de Janeiro: Bio-Manguinhos; 2018. p. 24-5. [Link] [ Links ]
29 Rivière M, Tretiak R, Levinton C, Fitzsimon C, Leclerc C. Economic benefits of a routine second dose of combined measles, mumps and rubella vaccine in Canada. Can J Infect Dis. 1997 Sep-Oct;8(5):257-64. Doi: 10.1155/1997/215175 [Link] [ Links ]
30 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Departamento de Vigilância das Doenças Transmissíveis. Manual de normas e procedimentos para vacinação. Brasília: Ministério da Saúde ; 2014. 176 p. [Link] [ Links ]
31 Kang HJ, Han YW, Kim SJ, Kim YJ, Kim AR, Kim JA, et al. An increasing, potentially measles-susceptible population over time after vaccination in Korea. Vaccine. 2017 Jul;35(33):4126-32. Doi: 10.1016/j.vaccine.2017.06.058 [Link] [ Links ]
32 Centers for Disease Control and Prevention. Plan for travel [Internet]. Atlanta (GA): Centers for Disease Control and Prevention; 2019 [cited 2020 Feb 19]. Available from: Available from: https://www.cdc.gov/measles/plan-for-travel.html . [ Links ]
33 Ogawa M, Ae R, Sasahara T. Relationship between self-reported vaccination history and measles and rubella antibody titers in medical and nursing students. Adv Infect Dis. 2017 May;7(2):27-36. Doi: 10.4236/aid.2017.72004 [Link] [ Links ]
34 Lievano FA, Helfand RF, Harpaz R, Walls L, Katz RS, Williams I, et al. Lack of evidence of measles virus shedding in people with inapparent measles virus infections. J Infect Dis. 2004 May;189 Suppl 1:S165-70. Doi: 10.1086/377715 [Link] [ Links ]
35 Smetana J, Chlibek R, Hanovcova I, Sosovickova R, Smetanova L, Gal P, et al. Decreasing seroprevalence of measles antibodies after vaccination - possible gap in measles protection in adults in the Czech Republic. PLoS One. 2017 Jan;12(1):e0170257. Doi: 10.1371/journal.pone.0170257 [Link] [ Links ]
36 Wiedermann U, Garner-Spitzer E, Wagner A. Primary vaccine failure to routine vaccines: why and what to do? Hum Vaccin Immunother. 2016 Jan;12(1):239-43. Doi: 10.1080/21645515.2015.1093263 [Link] [ Links ]
37 Ministério da Saúde (BR). Secretaria de Vigilância em Saúde. Secretaria de Atenção à Saúde. Relatório da verificação dos critérios de eliminação da transmissão dos vírus endêmicos do sarampo e rubéola e da síndrome da rubéola congênita (SRC) no Brasil. Brasília: Ministério da Saúde ; 2010. [Link] [ Links ]
How to cite this article / Como citar este artigo: Moraes MM, Sagica FES, Jesus MI, Medeiros RLF, Silva DFL, Matos HJ, et al. Seroepidemiological study of measles in populations living in the metropolitan region of Belém, Pará State, Brazil, 2016 to 2018. Rev Pan Amaz Saude. 2020;11:e202000378. Doi: http://dx.doi.org/10.5123/S2176-6223202000378
Received: June 24, 2019; Accepted: July 09, 2020
 Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
Este é um artigo publicado em acesso aberto sob uma licença Creative Commons
